 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Article
- Postoperative sagittal alignment and reoperation predict late outcomes after plate fixation of AO/OTA 33C distal femur fractures: a retrospective cohort study
- Hee Gon Park
- J Musculoskelet Trauma 2026;39(3):216-226. Published online July 24, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00073
-
 Abstract
Abstract
 PDF
PDF - Background
Intra-articular distal femoral fractures are associated with high complication rates and variable late outcomes. Although the AO Foundation/Orthopaedic Trauma Association (AO/OTA) classification system is useful for describing injury severity and anticipating complications, whether fracture subtype alone determines clinically relevant late outcomes remains unclear. This study aimed to evaluate postoperative complications and late outcomes following plate fixation of intra-articular distal femoral fractures and to identify factors independently associated with final clinical outcomes.
Methods
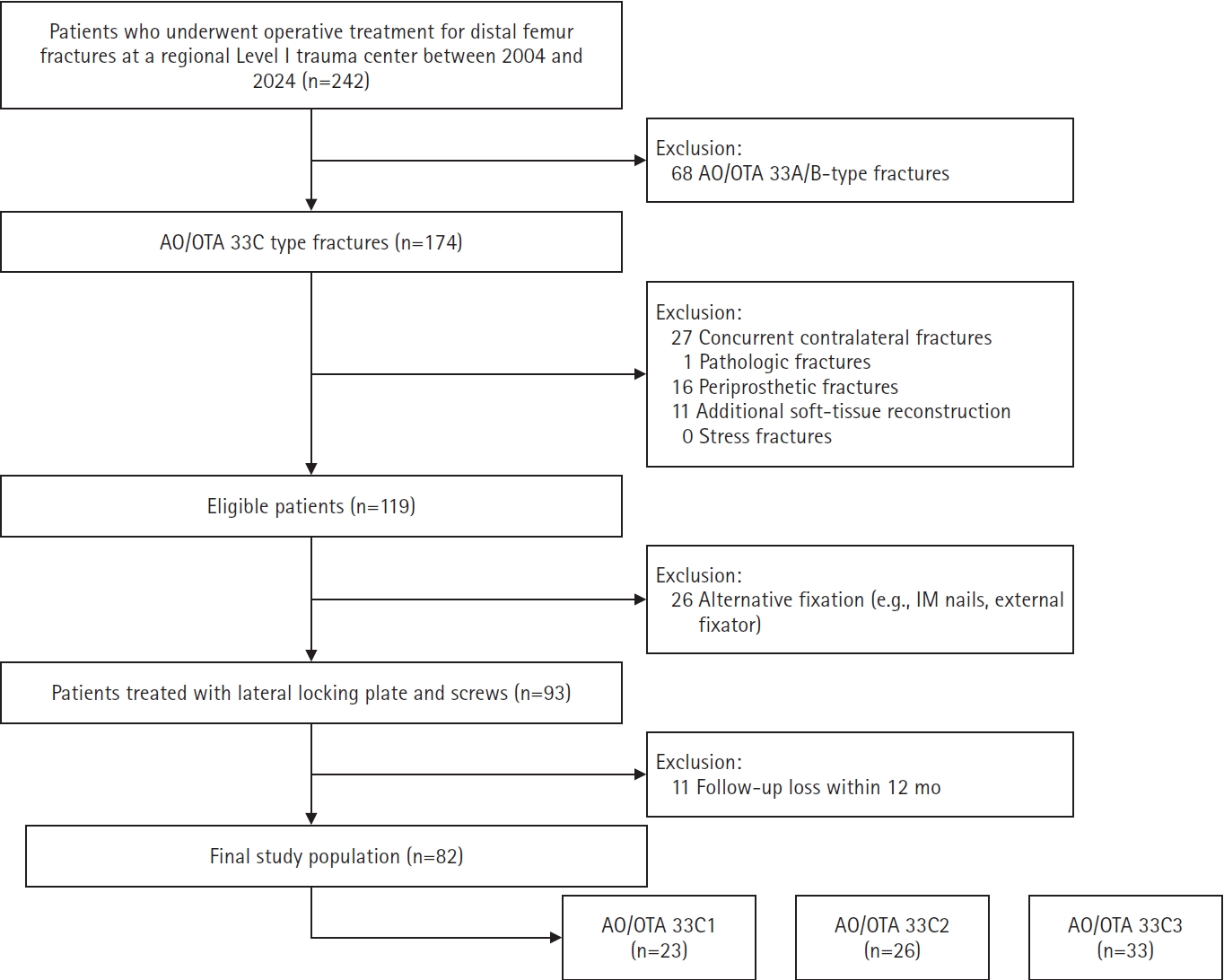
This retrospective cohort study was conducted at a regional Level I trauma center. Patients with AO/OTA 33C intra-articular distal femoral fractures who underwent plate fixation and were followed for at least 12 months were included. Radiographic parameters reflecting coronal and sagittal alignment were assessed using standardized measurement methods. Postoperative complications and reoperation were recorded as intermediate events. Clinically relevant late outcomes included final knee range of motion (ROM), leg length discrepancy, and radiographic osteoarthritis severity, assessed as the difference in Kellgren-Lawrence grade. Multivariable linear regression analyses were performed to identify factors independently associated with late outcomes.
Results
The 33C3 group (n=33) had significantly higher rates of open fracture (54.5%), nonunion (39.4%), and reoperation (45.5%) than the 33C1–2 group (n=49). At the final follow-up, 33C3 fractures were associated with lower mean ROM (P<0.001) and greater osteoarthritis progression (P<0.001). However, multivariable analysis showed that sagittal malalignment (Δ anatomical posterior distal femoral angle: β=−2.35, P=0.001) and reoperation (β=−17.5, P=0.001), rather than AO/OTA subtype itself, were independent predictors of final ROM.
Conclusions
Although fracture subtype according to the AO/OTA classification was associated with predictable complication patterns, clinically relevant late outcomes following intra-articular distal femoral fractures were more closely associated with postoperative alignment quality and the treatment course than with fracture classification alone. These findings highlight the importance of optimizing radiographic alignment and preventing complications that lead to reoperation to improve long-term outcomes after plate fixation. Level of evidence: III.
- 82 View
- 6 Download

Case Report
- Open distal radius fracture with ulnar neurovascular injury treated with dorsal spanning plate fixation and vein interposition grafting: a case report
- Kyeong-Eon Kim, Ho-Yong Lee, Shin-Woo Lee, Ji-Sup Kim
- J Musculoskelet Trauma 2026;39(3):262-268. Published online July 20, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00164

-
Abstract
PDF
- Open comminuted intra-articular distal radius fractures with associated ulnar neurovascular injury are rare; furthermore, these injuries are challenging because skeletal stabilization, arterial reconstruction, nerve assessment, and soft-tissue coverage must be coordinated. We report the case of an 80-year-old female patient who presented after a fall from stairway with a severe open distal radius fracture and a volar-ulnar distal forearm wound. She reported numbness and tingling in the ring and small fingers, with a cold sensation and delayed capillary refill. Imaging showed a severely comminuted intra-articular distal radius fracture (AO/OTA type 23-C3). Emergency surgery was performed within 6 hours. First, a dorsal spanning plate was applied, and the small volar lunate facet fragment was fixed with a volar lunate facet plate. After debridement of the injured ulnar artery, a segmental defect remained and was reconstructed using a reversed basilic vein interposition graft harvested from the ipsilateral proximal forearm. The contused but continuous ulnar nerve was treated with neurolysis. The soft-tissue defect was managed with an acellular dermal matrix and negative-pressure wound therapy, followed by staged full-thickness skin grafting 1 week later. At 1 year postoperatively, bony union was achieved, and the functional outcomes were satisfactory. Level of evidence: V.
- 96 View
- 7 Download
Original Article
- Open reduction and internal fixation for distal humerus fractures in older adults: a retrospective comparative study by osteoporosis status
- Tong Joo Lee, Hee Beom Shin, Yongseok Lee
- J Musculoskelet Trauma 2026;39(3):227-235. Published online July 15, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00101
-
Abstract
PDF
- Background
Distal humerus fractures in older patients, particularly those with osteoporosis, pose substantial treatment challenges because of increased fracture complexity and compromised bone stock. Open reduction and internal fixation (ORIF) is the preferred treatment but may be complicated by fixation failure. This study investigated the outcomes of ORIF in older osteoporotic and nonosteoporotic patients with complete articular distal humerus fractures.
Methods
This retrospective study included 19 patients with Arbeitsgemeinschaft für Osteosynthesefragen/ Orthopaedic Trauma Association (AO/OTA) 13C distal humerus fractures who underwent surgical treatment between 2012 and 2024. The mean patient age was 79.1 years. Patients were divided into osteoporotic (n=11) and nonosteoporotic (n=8) groups based on the lowest recorded dual-energy X-ray absorptiometry T-score at the femoral neck or lumbar spine. Osteoporosis was defined as a T-score of −2.5 or lower, and the nonosteoporotic group included patients with osteopenia. All fractures were treated with ORIF using bicolumnar plating. All included patients completed 12 months of clinical follow-up for visual analog scale (VAS) and Mayo Elbow Performance Score (MEPS) assessments. Radiographic follow-up was recorded separately and continued until union was confirmed; imaging follow-up extended to 12 months or longer in 14 patients and was limited to 6 months in five asymptomatic patients after confirmed union.
Results
Both groups showed significant within-group improvement in pain, as assessed using the VAS, and function, as assessed using the MEPS, over time. Between-group comparisons at each follow-up time point showed no statistically significant differences in VAS or MEPS. No radiographic nonunion was observed during the available imaging follow- up, and complications were limited to one case of screw pullout/loosening and one case of postoperative stiffness.
Conclusions
ORIF provides reliable outcomes for older patients with complex distal humerus fractures, regardless of osteoporosis status, when stable reconstruction is achievable. These findings suggest that ORIF remains a viable treatment option, with satisfactory functional recovery and low complication rates in this population. Level of evidence: III.
- 164 View
- 7 Download
Case Reports
- Fixation with two headless compression screws and a distal-radius bone graft for proximal scaphoid nonunion with dorsal intercalated segment instability deformity: a report of three cases
- Seonjeong Lee, Won Sun Lee, Jae Kwang Kim
- J Musculoskelet Trauma 2026;39(3):252-261. Published online July 7, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00136
-
Abstract
PDF
- Proximal scaphoid nonunion is difficult to treat because the proximal fragment is small and biologically compromised. Secure fixation can be especially challenging when dorsal intercalated segment instability (DISI) is present and requires correction. We report three male patients with proximal scaphoid nonunion and DISI deformity who underwent volar fixation with two 2.4-mm headless compression screws and cancellous bone graft harvested from the distal radius at the Lister tubercle. Preoperative computed tomography confirmed a proximal nonunion line and proximal fragment dimensions considered sufficient for dual-screw fixation, and magnetic resonance imaging showed no definite avascular necrosis. Early postoperative computed tomography showed maintained fixation and alignment in all three patients. Although CT-confirmed union at final follow-up was not uniformly available, radiographic union defined on plain radiographs was achieved in all cases without loss of alignment or carpal collapse. Carpal alignment improved in two patients, but DISI persisted in one. One patient underwent secondary removal of a preexisting loose body and one screw. This small case series suggests that dual-screw fixation with cancellous grafting may be technically feasible in selected proximal scaphoid nonunions with concomitant DISI. Level of evidence: V.
- 175 View
- 6 Download
- Radiocarpal subluxation after volar plating due to an insufficiently supported dorsal key fragment: a case report
- Yeongyoon Koh, Kanghun Yu, Jong Woong Park, In Cheul Choi
- J Musculoskelet Trauma 2026;39(3):269-274. Published online July 3, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00185

-
Abstract
PDF
- Distal radius fractures are commonly managed using volar locking plate fixation, which provides stable fixation in most cases. However, certain fracture patterns involving dorsal key fragments may not be adequately stabilized with a volar approach alone, even when intraoperative reduction appears satisfactory. We report the case of a 58-year-old male patient with a complex intra-articular distal radius fracture involving a dorsoulnar corner (DUC) fragment. Preoperative computed tomography revealed a dorsal fragment associated with subtle dorsal radiocarpal subluxation. Despite this finding, the fragment was considered amenable to fixation through a volar approach because it was relatively large. Although satisfactory reduction was achieved intraoperatively, early postoperative imaging demonstrated progressive dorsal radiocarpal subluxation due to displacement of the DUC fragment, while overall alignment parameters remained preserved. Revision surgery with additional dorsal buttress fixation successfully restored stability. This case highlights the critical importance of recognizing dorsal key fragments and achieving adequate dorsal support during fixation, as failure to provide sufficient support may result in delayed instability despite acceptable initial reduction. Level of evidence: V.
- 210 View
- 7 Download
Review Article
- Current concepts and applications of internal fixation for forearm diaphyseal fractures
- Sung Yoon Jung, Min Kyun Cho, Dong-hee Kim, Sang Hyun Lee
- J Musculoskelet Trauma 2026;39(3):205-215. Published online July 3, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00087
-
Abstract
PDF
- Adult diaphyseal fractures of the forearm functionally behave as intra-articular injuries because forearm rotation depends on accurate restoration of length, axial alignment, rotation, and the native radial bow. This narrative review summarizes contemporary surgical options for adult forearm shaft fractures, including 3.5-mm plate osteosynthesis, dual mini-plate fixation, interlocking intramedullary nailing, and minimally invasive plate osteosynthesis (MIPO). Compression plating with 3.5-mm plates remains the reference standard for most fracture patterns, whereas other techniques should be regarded as selective, emerging, or salvage options according to their indication spectrum and evidence base. Mini-fragment dual plating may be useful for short segments or thin soft-tissue envelopes, although the supporting clinical evidence remains limited and meticulous biomechanical execution is essential. Interlocking intramedullary nailing is a viable alternative for carefully selected simple fracture patterns or soft-tissue-compromised situations, offering less invasive exposure but a narrower indication spectrum. MIPO may be considered for selected comminuted or soft-tissue-compromised diaphyseal fractures; however, its use in adult forearm fractures remains constrained by the high functional requirement for precise restoration of length, rotation, and the radial bow. To improve transparency, this review explicitly distinguishes established, evidence-supported methods from techniques supported mainly by limited retrospective data or institutional experience. A pattern-based pragmatic algorithm and expanded comparison table are provided to guide fixation selection according to the bone involved, fracture location, fracture morphology, soft-tissue condition, and evidence tier while minimizing complications such as nonunion, infection, nerve injury, refracture after plate removal, and radioulnar synostosis.
- 230 View
- 6 Download
Case Report
- Paradoxical hypertrophy as a cause of femoral insufficiency fractures analyzed through differences in force application in Korea: three case reports
- Yong-Uk Kwon, Dae-Hyun Park, Hyoung-Gu Kang
- J Musculoskelet Trauma 2026;39(2):174-180. Published online April 23, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00388
-
Abstract
PDF
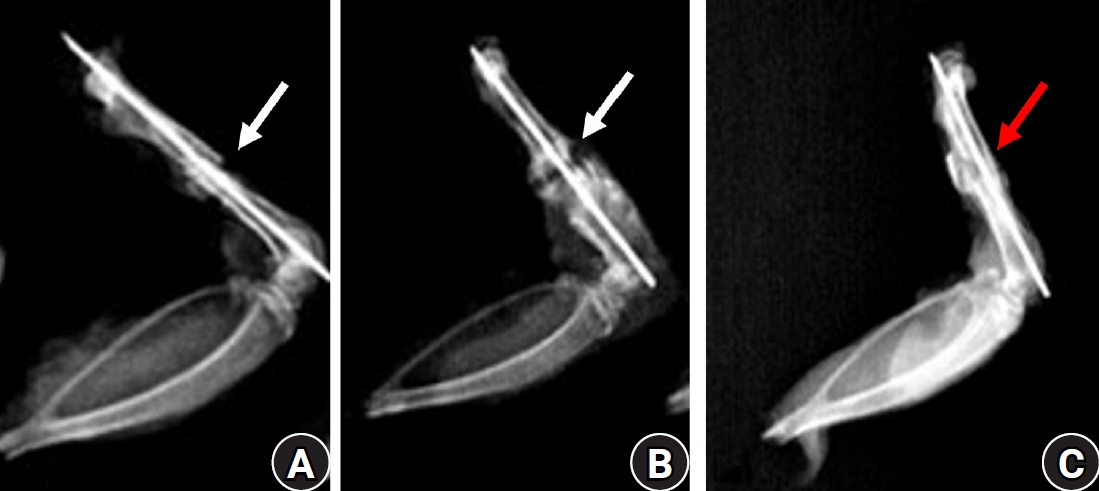
- Previous studies have extensively examined the association between femoral insufficiency fractures and prolonged bisphosphonate therapy. However, alternative etiologies remain insufficiently characterized. This study aimed to analyze nonpharmacologic factors associated with femoral insufficiency fractures, with particular emphasis on paradoxical cortical hypertrophy and altered biomechanical load distribution. We reviewed three cases of femoral insufficiency fracture that were surgically treated at our institution between January 2018 and January 2022. None of the patients had a history of bisphosphonate use. Clinical histories—including underlying comorbidities, prior surgical procedures, and radiographic findings—were evaluated. Serial radiographs obtained before and after fracture occurrence were analyzed to characterize fracture morphology and associated cortical changes. Case 1 involved a patient with posttraumatic hip synostosis; case 2 involved a patient with osteogenesis imperfecta; and case 3 involved a patient who had previously undergone intramedullary nailing for an intertrochanteric fracture. Lateral femoral bowing and cortical hypertrophy preceded fracture development in two cases, whereas focal cortical hypertrophy at the distal locking screw site was observed in the third case. No history of bisphosphonate therapy was identified in any patient. Fractures developed at sites characterized by increased cortical remodeling and abnormal load concentration. Femoral insufficiency fractures can occur in the absence of bisphosphonate therapy. Paradoxical cortical hypertrophy and altered biomechanical force distribution appear to be important contributing factors. Level of evidence: IV.
- 351 View
- 15 Download
Original Article
-
NSAID-induced suppression of type X collagen and VEGF expression in the early phase of rat femoral fracture healing

- Maria Zafar, Rana Mohammad Zeeshan, Safia Tasawar, Muhammad Saad Ilyas, Amer Aziz, Uruj Zehra
- J Musculoskelet Trauma 2026;39(2):162-173. Published online April 10, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00367
-
Abstract
PDF
 Supplementary Material
Supplementary Material - Background
The current literature presents conflicting evidence regarding the effects of nonsteroidal anti-inflammatory drugs (NSAIDs) on fracture healing. This experimental study aimed to evaluate and compare the histological and immunohistochemical changes during femoral fracture healing in rats treated with a nonselective cyclooxygenase (COX) inhibitor (diclofenac sodium) and a selective COX-2 inhibitor (celecoxib).
Methods
Thirty-six male Wistar (standard outbred) albino rats weighing 200–400 g underwent standardized mid-diaphyseal femoral fracture surgery. The animals were randomized into three groups (n=12 per group): group 1 received diclofenac sodium, group 2 received celecoxib, and group 3 served as the control group and received 1 mL of distilled water orally once daily. Six rats from each group were euthanized at the end of the 2nd and 7th weeks after fracture for sample collection. Histological examination was complemented by immunohistochemical analysis, and the expression of type X collagen and vascular endothelial growth factor (VEGF) was assessed using the immunoreactive score (IRS) method.
Results
Healing scores were significantly higher in the control group at both time points (2nd week, P=0.01; 7th week, P=0.03). At the 2nd week, rats treated with diclofenac sodium demonstrated significantly greater fibrosis (P=0.01), and by the 7th week, they exhibited impaired bone formation (P=0.003) along with increased bone defects (P=0.01). IRS values for type X collagen and VEGF were significantly higher in the control group than in both treatment groups during the 2nd week (P=0.01 and P=0.005, respectively).
Conclusions
These findings suggest that, in this rat model, NSAIDs, particularly nonselective COX inhibitors, may disrupt the early phases of bone repair by affecting hypertrophic chondrocyte differentiation and reducing angiogenic activity. Although these results indicate a potential risk to optimal healing, they are preclinical observations, and their relevance to clinical fracture management should be interpreted with caution. Level of evidence: V.
- 889 View
- 19 Download
Review Article
- Combined acetabular and pelvic ring injuries: a reference-frame algorithm for definitive fixation sequencing
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(2):83-92. Published online April 9, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00031
-
Abstract
PDF
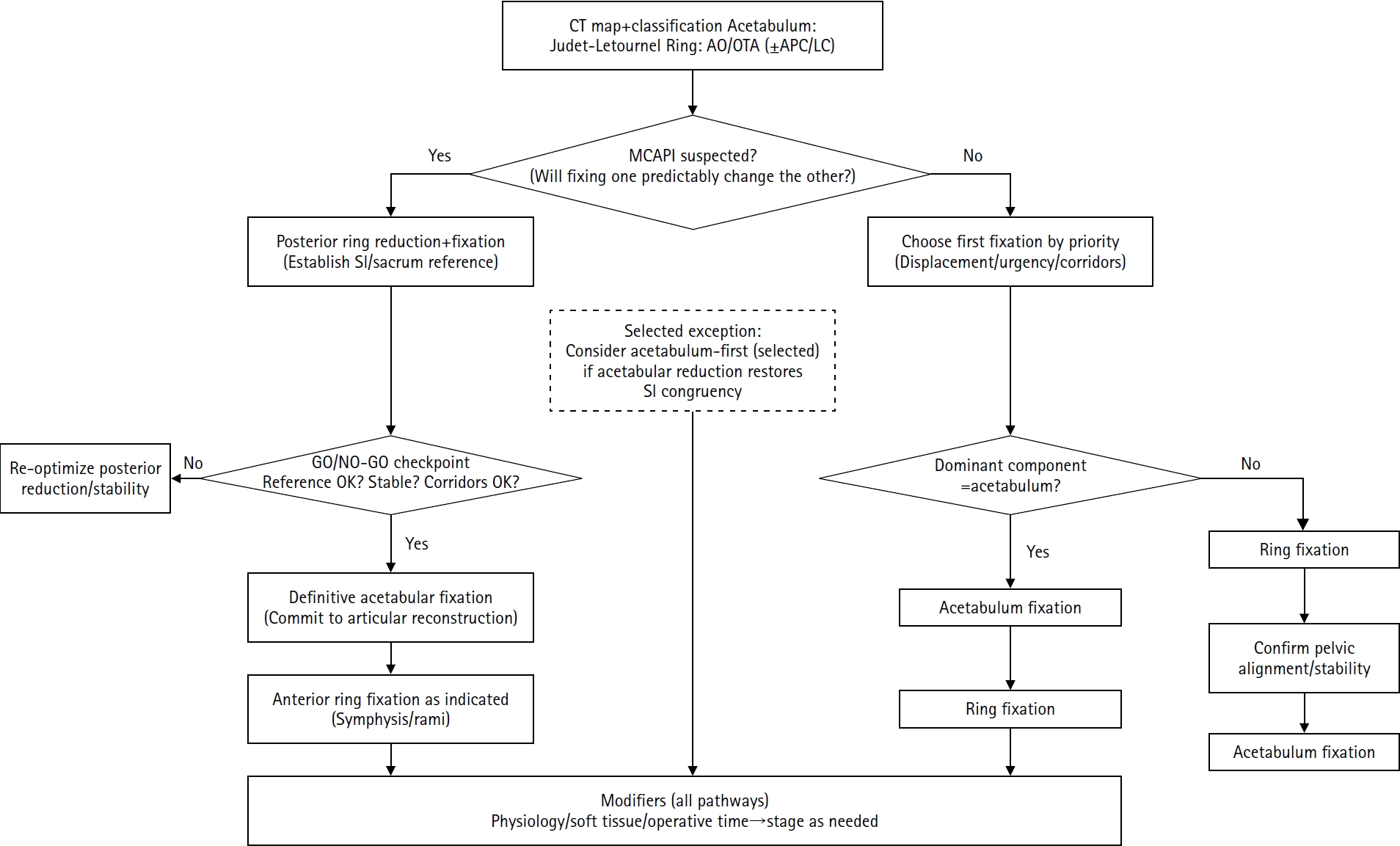
- Combined acetabular and pelvic ring injuries are not simply “two fractures in one patient.” Reduction and fixation of one component can alter the alignment and reducibility of the other, rendering operative sequencing a primary decision variable rather than a secondary consideration. These injuries typically result from high-energy trauma, frequently occur in patients with polytrauma, and are further influenced by physiological tolerance and the feasibility of available operative corridors. The existing evidence base remains constrained by retrospective study designs, inconsistent definitions, variable classification systems, and heterogeneous outcome reporting, all of which limit the strength of comparative recommendations. This state-of-the-art review presents a surgeon-facing, algorithmic approach grounded in a reference-frame mindset. We emphasize computed tomography (CT)-based mapping and the use of consistent terminology to characterize acetabular morphology, pelvic ring instability, deformity vectors, suspicion of mechanical coupling, and feasible operative corridors. Mechanically connected acetabular and pelvic ring injuries (MCAPI) are introduced as a working framework for identifying patterns in which reduction or fixation of one injury predictably influences the other. In cases of suspected MCAPI, a posterior ring-based sequence is generally preferred, typically consisting of posterior ring reduction and fixation, definitive acetabular reconstruction, and subsequent anterior ring fixation. We propose an explicit intraoperative “GO/NO-GO” checkpoint (reference acceptable, stable, corridors feasible) to prevent acetabular reconstruction on a moving target. Acetabulum-first strategies may be appropriate only in selected anteroposterior compression- type configurations in which acetabular fixation plausibly restores sacroiliac congruency and posterior stabilization remains technically feasible. We summarize key outcome domains and complication patterns, highlighting hip dislocation as an important risk factor associated with both neurologic deficits and overall complications. Standardized CTbased definitions and outcome instruments, together with multicenter cohorts employing predefined decision pathways, are required to test sequencing strategies and to determine whether improved radiographic reduction translates into durable functional benefit.
- 2,574 View
- 34 Download
Case Report
- Successful reconstruction and functional recovery of a pediatric medial malleolus defect in an 8-year-old girl using autologous iliac crest bone grafting in Korea: a case report
- Sung Yoon Jung, Dong-hee Kim, Sang Hyun Lee, Ki-Hun Kim
- J Musculoskelet Trauma 2026;39(3):245-251. Published online April 8, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00059

-
Abstract
PDF
- An 8-year-old girl presented after a traffic accident with a severe crush and degloving injury of the medial right ankle and foot, a distal tibiofibular fracture, and medial midfoot bone defects. After staged irrigation and debridement with temporary external fixation, definitive reconstruction was performed on August 6, 2016. The medial malleolar defect (2.5×2.0 cm) was reconstructed using a contoured autologous iliac crest bone graft secured with internal fixation, and medial stability was augmented using harvested gluteal fascia as a deltoid ligament substitute fixed with suture anchors. A bone-cement spacer was placed adjacent to the injured physis to mitigate physeal bridging, and the extensive soft-tissue defect was covered with a free anterolateral thigh flap and skin graft. During follow-up, progressive varus deformity and contracture were managed with corrective osteotomy and plating, Achilles tendon lengthening, Z-plasty, and Ilizarov fixation. At the final follow-up (March 6, 2025), the limb-length discrepancy was 5 mm, active ankle dorsiflexion was 0° (passive dorsiflexion 5°), and the patient was pain-free with full participation in daily activities, including hiking and dancing. This case emphasizes the value of an integrated staged strategy that combines bony reconstruction, medial stabilization, physeal management, and durable soft-tissue coverage during skeletal growth. Level of evidence: V.
- 769 View
- 12 Download
Original Articles
- Biomechanical comparison of anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating in patellar fractures using a synthetic bone model
- Abdullah M. Aljeaid, Wonseok Choi, Jeong-Seok Choi, Youngsig Choi, Jiyeon Bae, Jong-Keon Oh, Jae-Woo Cho
- J Musculoskelet Trauma 2026;39(2):130-139. Published online April 7, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00353
-
Abstract
PDF
- Background
Patellar fractures are common injuries that require stable fixation to achieve optimal healing and restoration of knee function. This study aimed to analyze the mechanical properties of an anatomically precontoured patellar plate and to compare its maximum tensile load-bearing capacity with that of anterior tension wiring through cannulated screws and double-sided plating for the fixation of patellar fractures.
Methods
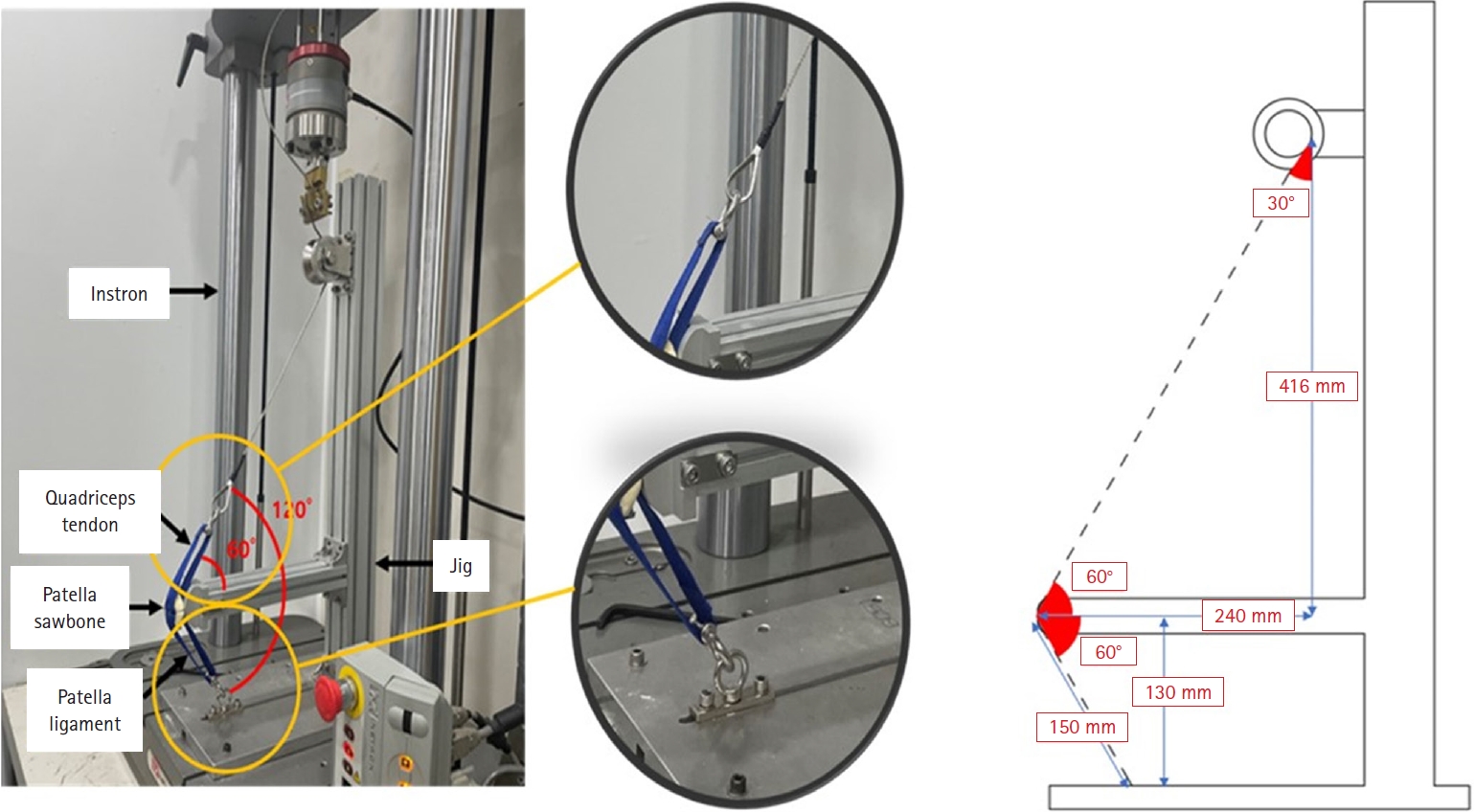
Artificial Sawbones with a standardized transverse fracture line were used to simulate patellar fractures. Each sawbone was attached to polyester bands, and this fracture model was applied consistently across all test samples. To evaluate mechanical properties of the anatomically precontoured patellar plate (model code 25-ANPA-209) made of ASTM F67 titanium, static tensile strength testing and dynamic tensile strength testing were performed, with seven samples prepared for each test. For comparison of maximum tensile load capacity among the anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating, five samples were prepared for each fixation group. All specimens were tested using a tension/compression testing machine.
Results
In the static tensile strength test, all seven samples exhibited a maximum tensile load capacity above 844 N without any fractures or failure points. The dynamic tensile strength test showed that all seven samples completed 10,000 cycles without deformation or damage to the anatomically precontoured patellar plate. When comparing maximum tensile load capacity, the anatomically precontoured patellar plate exhibited a significantly higher maximum tensile load-bearing capacity than anterior tension wiring through cannulated screws and double-sided plating.
Conclusions
The anatomically precontoured patellar plate demonstrated satisfactory mechanical performance, successfully meeting the criteria of both static and dynamic tensile strength testing, and showed superior maximum tensile load-bearing capacity compared with the other fixation methods evaluated. These findings suggest that the anatomically precontoured patellar plate may represent a reliable fixation option for the management of patellar fractures. Level of evidence: V.
- 999 View
- 24 Download
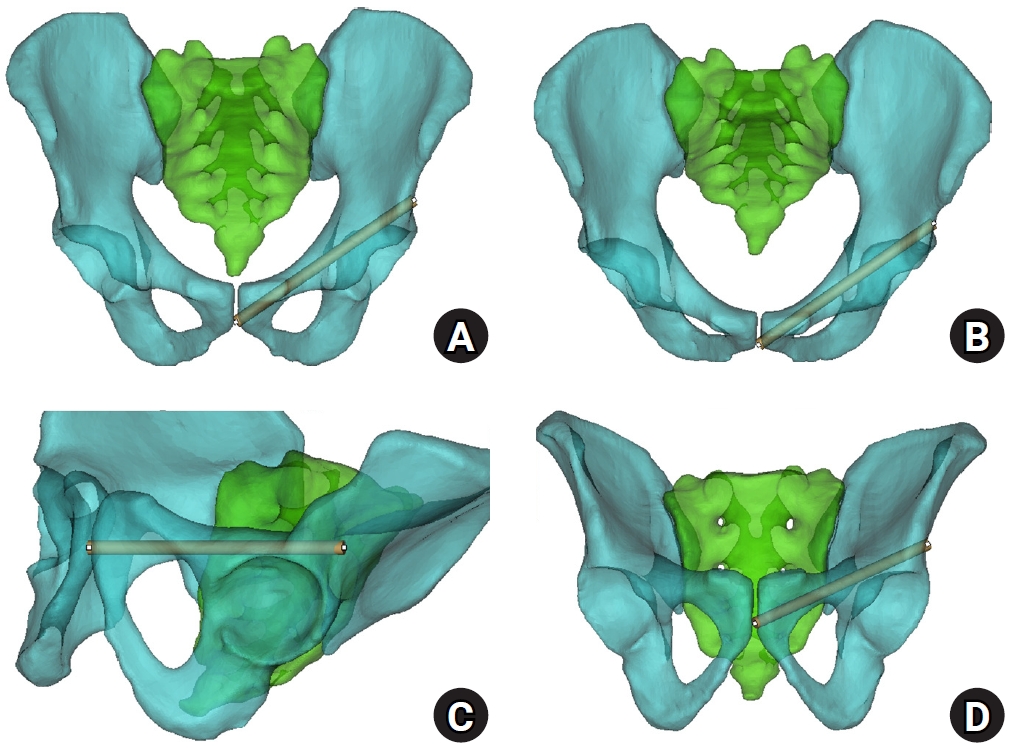
- Sex-specific bottlenecks and risk zones in the retrograde superior pubic ramus screw corridor: a 3D CT-based morphometric cadaver study
- Ji Won Jeong, Jung Tae Ahn, Gu Hee Jung, Kun Tae Kim
- J Musculoskelet Trauma 2026;39(2):103-116. Published online March 26, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00066
-
Abstract
PDFSupplementary Material
- Background
Superior ramus screw fixation is commonly used to stabilize anterior pelvic ring injuries but is constrained by a narrow, irregular, and curved intraosseous corridor. Trajectory-based morphometric analysis may assist in screw diameter selection and enable identification of reproducible anatomic constriction zones.
Methods
We conducted a cross-sectional computed tomography (CT)-based morphometric study of 82 cadaveric pelvises (42 males, 40 females). Bottleneck diameter was defined as the diameter of the largest fully contained virtual cylinder along the planned trajectory, and cylinder length was recorded. Orthogonal cross-sections at 9.5-mm intervals (up to 12 segments) were generated to measure segment-wise effective diameter (defined as twice the minimum centerline-to-cortex distance) and cortical clearance, which was used as a diameter-based safety margin. Segments were realigned to the acetabular start segment to define relative segment positions (Δ seg). Feasibility was assessed for prespecified screw diameters ranging from 3.5 to 7.3 mm.
Results
Mean bottleneck diameter was larger in males than in females (7.34±1.10 vs. 5.93±0.98 mm), whereas trajectory length was similar between sexes (127.85±8.54 vs. 128.85±8.20 mm). Δ seg realignment localized corridor constriction to two discrete zones: a preacetabular zone (Δ seg −6 to −4) and a periacetabular zone (Δ seg 1 to 2), where effective diameter and cortical clearance were most limited. Feasibility rates were 100% at 3.5–4.5 mm, 95.2% vs. 82.5% at 5.0 mm, 81.0% vs. 27.5% at 6.5 mm, and 59.5% vs. 10.0% at 7.3 mm in males and females, respectively.
Conclusions
Female models demonstrated smaller trajectory-wide bottleneck diameters and segment-wise effective diameters than male models. Acetabular-referenced Δ seg realignment identified two reproducible anatomic risk zones: a preacetabular zone adjacent to the obturator neurovascular bundle and a periacetabular zone near the external iliac vessels. At diameters ≥6.5 mm, cortical proximity increased more prominently in females than in males. Level of evidence: III.
- 1,066 View
- 28 Download
Review Article
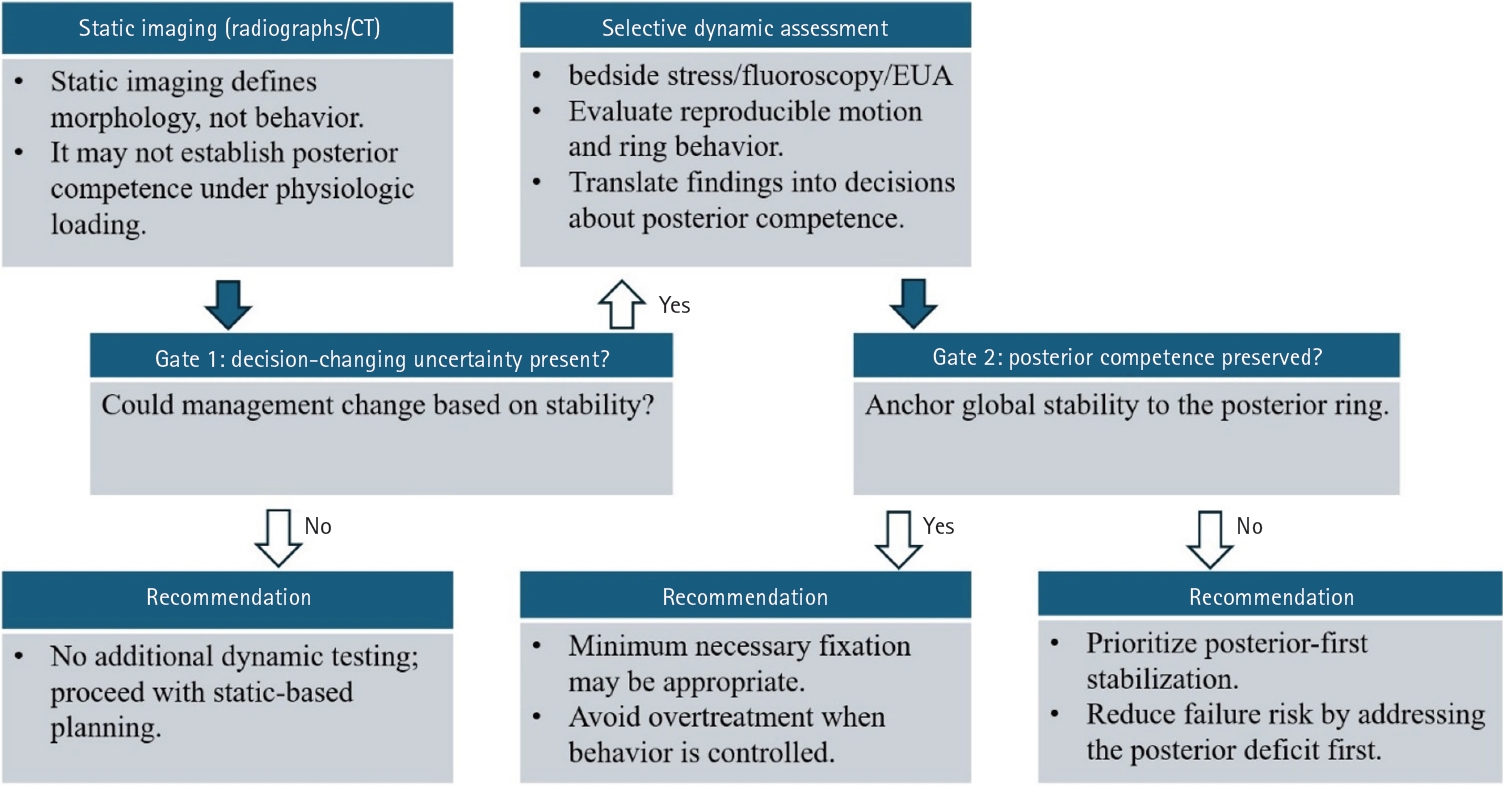
- Definitive fixation for traumatic pelvic ring injuries: a dynamically informed, posterior-referenced framework
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(2):73-82. Published online March 24, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00045
-
Abstract
PDF
- Optimal definitive fixation for traumatic pelvic ring injuries remains challenging because static radiographs and computed tomography, although essential for defining morphology, do not consistently predict load-dependent behavior during early mobilization. This uncertainty contributes to substantial practice variation and continued reliance on simplified displacement thresholds, such as the 2.5 cm rule. Such rules can misclassify instability by underrepresenting posterior competence and by privileging static measurements over functional behavior. In this narrative review, we propose a dynamically informed, posterior- referenced framework composed of three linked elements: (1) decision-linked terminology that explicitly distinguishes dynamic instability, radiographic change, and clinical failure; (2) selective stress-based assessment when uncertainty is likely to alter management; and (3) escalation along a fixation continuum that weighs incremental stability against operative burden. When static imaging cannot establish posterior competence with confidence, we outline selective stress-based approaches to assess pelvic ring behavior and to translate demonstrated instability into fixation selection along a defined continuum. Across all steps, the framework emphasizes minimum necessary fixation and explicitly incorporates the cost of selection as a primary decision variable. The operative question, therefore, shifts from gap width alone to clinically relevant motion and preservation of posterior competence. In doing so, this approach aims to reduce both undertreatment and overtreatment and to improve the consistency and defensibility of definitive fixation strategies across diverse practice environments.
- 1,643 View
- 36 Download
Original Articles
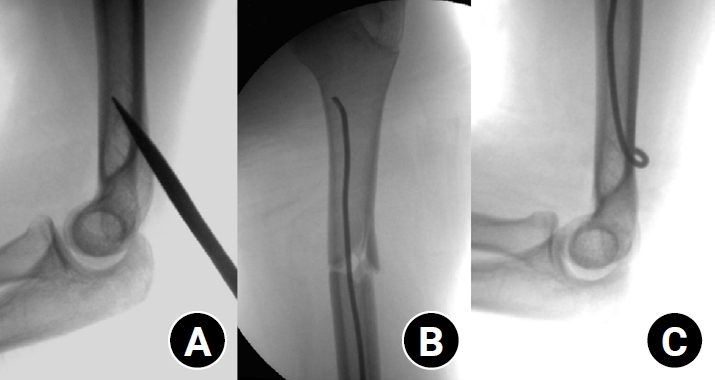
- Clinical and radiographic outcomes of elastic stable intramedullary nailing for pediatric humeral shaft fractures: a retrospective case series
- Kang-San Lee, Dongju Shin, Sang Hee Kim, Il Seo, Tae-Hoon Kim, Sung Jung Kim
- J Musculoskelet Trauma 2026;39(2):156-161. Published online March 10, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00381
-
Abstract
PDF
- Background
Pediatric humeral shaft fractures are uncommon and are generally treated conservatively, with satisfactory clinical outcomes reported in most cases. However, conservative management often necessitates prolonged immobilization and frequent outpatient follow-up visits, and it carries an inherent risk of residual angular or translational deformity. Elastic stable intramedullary nailing (ESIN) provides a simple and minimally invasive method of fracture fixation that offers adequate stability without disrupting the periosteal blood supply, thereby permitting early mobilization and promoting rapid bone union. The purpose of this study was to evaluate the clinical and radiological outcomes of ESIN fixation in pediatric patients with humeral shaft fractures.
Methods
The medical records of pediatric patients with humeral shaft fractures who underwent ESIN fixation between January 2015 and November 2025 were retrospectively reviewed. Data collected included patient demographics, mechanism of injury, fracture location, number of elastic nails used, time to union, degree of residual angulation, range of motion (ROM), and postoperative complications.
Results
The mean age of the patients was 10.0 years (range, 7 to 15 years). The mean time to radiographic union was 5.4 weeks (range, 2.4 to 10.4 weeks). The mean coronal angulation was 0.2° (range, −9.1° to 5.8°), while the mean sagittal angulation was −1.3° (range, −6.9° to 5.3°). No cases of infection, nerve injury, or nail migration were observed during the follow-up period. At the final follow-up assessment, all patients demonstrated full shoulder and elbow ROM, with no residual deformity or pain reported.
Conclusions
In this small retrospective case series, ESIN fixation resulted in favorable union rates and excellent functional outcomes in pediatric humeral shaft fractures. Level of evidence: IV.
- 634 View
- 21 Download
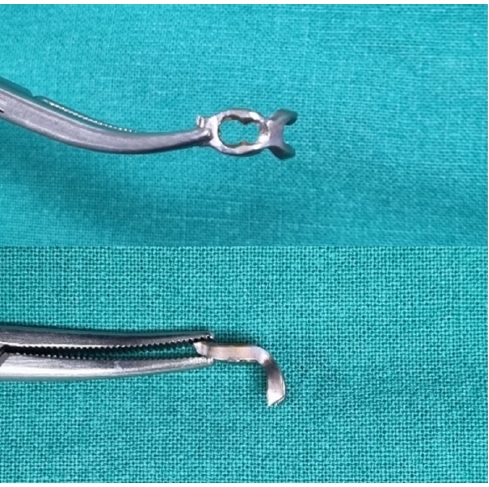
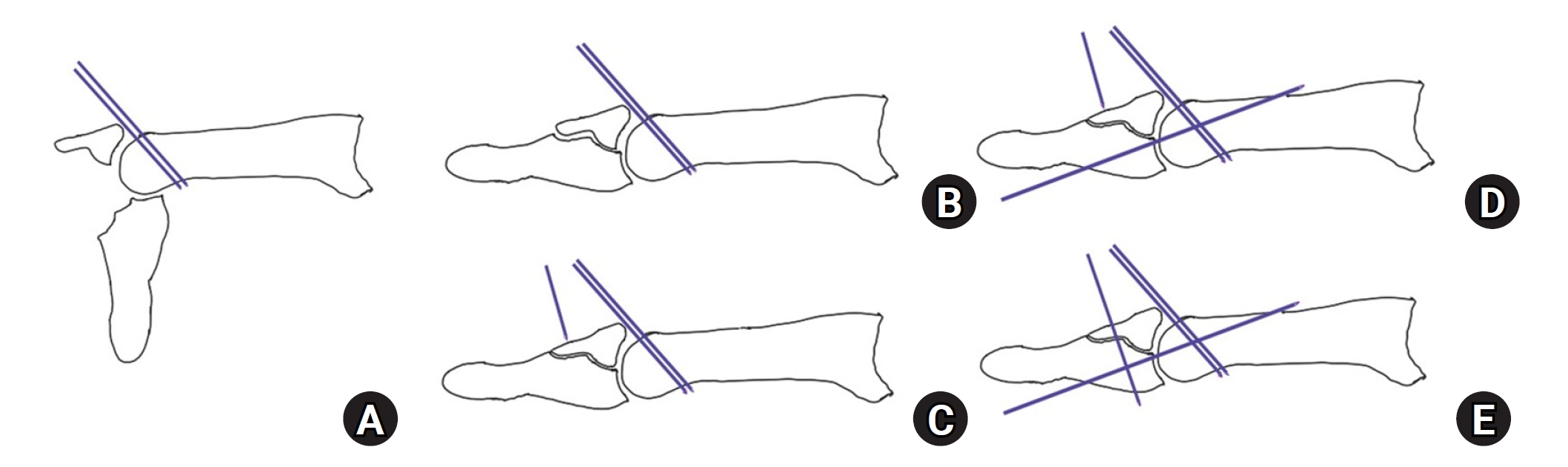
- Hook plate fixation for volar plate avulsion fractures of the middle phalanges in Korea: a case series
- Kang-San Lee, Sang-Woo Son, Hee-June Kim, Hyun-Joo Lee, Dong Hee Kim
- J Musculoskelet Trauma 2026;39(1):48-53. Published online January 25, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00339
-
Abstract
PDF
- Background
Volar plate avulsion fractures in phalanges are relatively common injuries. While surgical treatment can help reduce limitations in motion after injury, the small size of the fracture fragment can make the procedure challenging. In this study, we used hook plate fixation as a surgical technique for treating volar avulsion fractures in phalanges and evaluated its radiological and clinical outcomes.
Methods
The medical records of eight patients (nine digits) with volar plate avulsion fractures of the middle phalanx were retrospectively reviewed. All fractures were treated with a 1.5-mm hook plate after open reduction. Radiologic evaluations were performed using simple radiographs, and clinical outcomes were assessed through range of motion, instability, and pain.
Results
The mean follow-up period was 4.89 months (range, 1–9 months). All nine digits achieved bone union at the final follow-up. The mean union time was 2.2 months (range, 1–4 months). In all patients, the range of motion in the proximal interphalangeal joint was 85° (range, 70°–100°) before implant removal and 89.4° (range, 80°–100°) after implant removal. All patients demonstrated no joint instability and no residual pain.
Conclusion
Using a hook plate for volar plate avulsion fractures presents a promising alternative to existing fixation methods. Its biomechanical advantages and ease of fabrication make it a valuable tool in hand surgery. Level of evidence: IV.
- 1,458 View
- 40 Download
- Association between decreased bone mineral density and Pauwels angle in femoral neck fractures: a cross-sectional study
- Soo-Hwan Jung, Yong-Uk Kwon, Ji-Hun Park
- J Musculoskelet Trauma 2026;39(1):20-29. Published online January 25, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00269
-
Abstract
PDFSupplementary Material
- Background
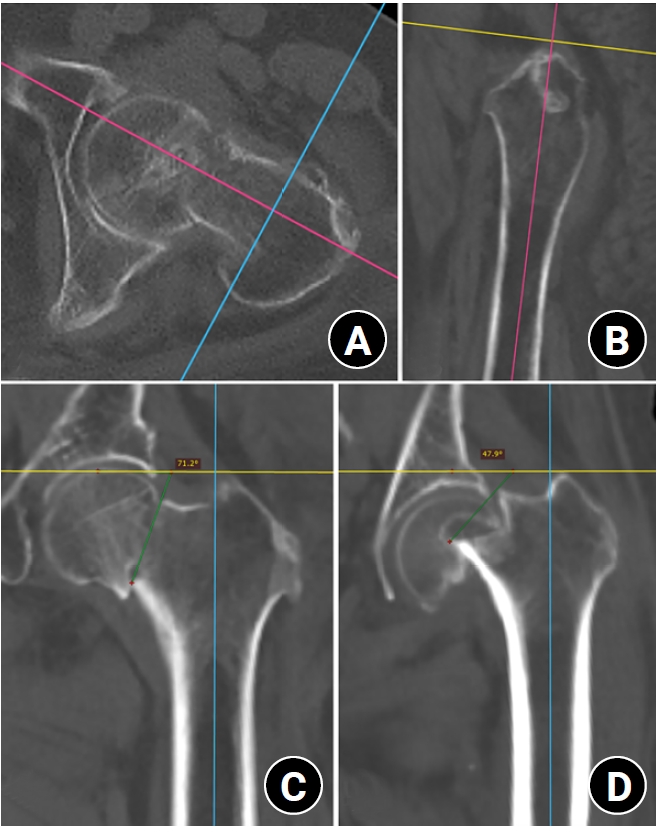
Progressive osteoporosis reduces the trabecular structures of the proximal femur, whereas the primary compression trabeculae (PCTs) are relatively preserved. We hypothesize that the loss of the vertically oriented PCTs in osteoporosis, which act as a mechanical barrier, affects fracture line propagation and influences the Pauwels angle. This study investigated the association between bone mineral density (BMD) and Pauwels angles in low-energy femoral neck fractures (FNFs).
Methods
This cross-sectional study included 150 patients (mean age, 75.3 years; range, 50–94 years) diagnosed with intracapsular FNFs between May 2019 and May 2023. BMD was measured within 1 month of the injury date using dual-energy X-ray absorptiometry, and modified Pauwels angles were assessed using a computed tomography-based multiplanar reconstruction program. Multiple linear regression analysis was performed to evaluate the factors influencing the Pauwels angles. The dependent variable was the Pauwels angle, while the independent variables included sex, age, height, body weight, body mass index, American Society of Anesthesiologists score, Charlson comorbidity index score, smoking status, alcohol use, preinjury walking ability, and femoral neck BMD T-scores.
Results
Higher femoral neck BMD T-scores were significantly associated with increased Pauwels angles (β=3.449, P<0.001). Greater body weight was independently associated with increased Pauwels angles (β=0.213, P=0.007).
Conclusions
The Pauwels angle demonstrated a significant association with BMD, with lower BMD associated with less steep Pauwels angles. In the absence of BMD measurement, the Pauwels angle may indicate osteoporosis severity in patients with low-energy FNFs. Level of evidence: III.
- 1,221 View
- 26 Download
Technical Note
- Rim plate-assisted intramedullary nail and plate combination technique for complex tibial plateau-to-diaphysis fractures: a technical note and case series
- Whee Sung Son
- J Musculoskelet Trauma 2026;39(1):62-71. Published online December 4, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00290

-
Abstract
PDF
- Complex tibial plateau-to-diaphysis fractures present a significant surgical challenge due to their intricate fracture patterns and frequent association with severe soft tissue damage and concomitant injuries. This technical note introduces a novel fixation strategy: the rim plate-assisted intramedullary nail-plate combination (NPC) technique. In this approach, a rim plate simplifies the conventional NPC procedure by unifying the tibial plateau fracture into a single structural segment. This modification eliminates the need to address the articular and diaphyseal components simultaneously while enhancing articular stability. Furthermore, the technique preserves soft tissue integrity and promotes early rehabilitation. Clinical case examples demonstrate its successful application in managing complex tibial plateau-to-diaphysis injuries. Level of evidence: V.
- 1,564 View
- 63 Download
Review Article
- Current concepts and applications of bone graft substitutes in orthopedic surgery
- Jae Ho Cho, Hyung Keun Song
- J Musculoskelet Trauma 2025;38(4):169-177. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00248

-
Abstract
PDF
- Bone defects, which often arise from high-energy injuries, infections, tumor resections, or nonunions, represent a persistent challenge in orthopedic trauma surgery. Autologous bone grafting remains the gold standard due to its unique combination of osteogenic, osteoinductive, and osteoconductive properties. However, issues such as donor site morbidity, limited graft volume, and increased surgical time have driven the development of bone graft substitutes. These substitutes vary widely in origin, composition, biological activity, and mechanical characteristics, encompassing allografts, xenografts, synthetic materials, and biologically enhanced constructs. This review outlines the fundamental biological principles underlying bone regeneration—including osteogenesis, osteoinduction, and osteoconduction—and addresses additional key factors such as biocompatibility, biodegradability, and mechanical strength. Current bone graft materials are classified by biological origin and functional characteristics, with an emphasis on their use in trauma surgery. Particular attention is given to the clinical applications, indications, and limitations of allograft-based solutions (such as structural allografts and demineralized bone matrix), synthetic ceramics (including calcium phosphate and bioactive glass), and biologically enhanced options, such as recombinant growth factors and stem cell therapies. In trauma settings, graft selection must be tailored to the characteristics of the defect, mechanical demands, the biological environment, and patient-specific factors. Integration with surgical technique and fixation is crucial for optimizing outcomes. Although modern substitutes show promise, none fully replicate the complex biology of autografts. Looking ahead, emerging technologies such as 3D printing, nanotechnology, and smart biomaterials offer exciting possibilities but face translational challenges. This review aims to provide practicing orthopedic surgeons with a concise, evidence-based overview of bone substitute options and their roles in trauma care. By applying core biological principles and clinical judgment, surgeons can better navigate the expanding array of graft materials to improve outcomes for patients with complex skeletal defects.
-
Citations
Citations to this article as recorded by
- Safety and Efficacy of rhBMP-2 for Treating Acute Traumatic Fractures of the Upper and Lower Extremities: A Multicenter Prospective Study
Seungyeob Sakong, Seokjun Hong, Wonseok Choi, Seonghyun Kang, Jae-Woo Cho, Whee Sung Son, Jeong-Seok Choi, Chang-Jin Yon, Won-Tae Cho, Jong-Keon Oh
Journal of Clinical Medicine.2026; 15(3): 1176. CrossRef - Plasma‐Assisted KR‐12 Conjugated PLGA Nanofibers With Dual Osteogenic and Biofilm‐Inhibitory Activity
Günnur Pulat, Eda Bilgiç, Buse Sezer
Journal of Biomedical Materials Research Part A.2026;[Epub] CrossRef - Histological Study of a Novel 3D-Printed Hydroxyapatite/PLGA Bone Graft in the Regeneration of Critical-Sized Long Bone Defects
Marijana Popović Bajić, Smiljana Paraš, Milutin Mićić, Božana Petrović, Vladimir Biočanin, Slavoljub Živković, Marija Živković, Damjana Drobne, Vukoman Jokanović
Bioengineering.2026; 13(4): 394. CrossRef - The Use of Osteo-Inductive 3D-Printed Scaffolds Covered with a Pleiotrophin Peptide for Bone Defects: An In Vivo Experimental Study
Dimitrios Tsoumanis, Emilios E. Pakos, Ioannis Gkiatas, Ioannis Gelalis, Anna Batistatou, Evangelia Lampri, Despoina Deligianni, Evangelia Papadimitriou, Dimitrios Fotiadis, Anastasios Korompilias
Bioengineering.2026; 13(6): 608. CrossRef - Research advances in bioactive bone graft materials and bone marrow enrichment techniques for bone defect treatment
Zhezheng Shen, Xueyuan Li, Zijun Ye, Yuhao Zhou, Di Tu, Zongying Tian, Wei Qian
Cell Transplantation.2026;[Epub] CrossRef - A Novel Technique of Overlapping Distal Stump Within Femoral Allograft-Prosthesis Composite for Extensive Humeral Bone Loss in Revision Total Elbow Arthroplasty
Chul-Hyun Cho, Bum-Soon Park, Eun-Seok Son, Du-Han Kim
Techniques in Orthopaedics.2026;[Epub] CrossRef - Enhancing Bone Healing with a Priming Stimulus
Michael Tanzer, Misghana Kassa, Nitin Chandra Teja Dadi, Tarek Klaylat, Rahul Gawri, Paul Martineau, Adam Hart
Life.2026; 16(7): 1111. CrossRef
- Safety and Efficacy of rhBMP-2 for Treating Acute Traumatic Fractures of the Upper and Lower Extremities: A Multicenter Prospective Study
- 10,848 View
- 285 Download
- 7 Crossref
Original Articles
- Hook plate versus periarticular-type volar locking plate for distal radius fractures involving the volar lunate facet in Korea: a retrospective cohort study
- Hyun-Jae Park, Joo-Hak Kim
- J Musculoskelet Trauma 2025;38(4):221-228. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00241
-
Abstract
PDF
- Background
This study investigated the clinical and radiographic outcomes of hook plate (HP) fixation for volar lunate facet fractures, comparing them with periarticular-type volar locking plates (PVLPs).
Methods
A retrospective review was conducted on 24 patients with distal radius fractures involving volar lunate facet fragments who underwent surgery between January 2016 and April 2021. Patients were divided into two groups: HP (n=12) and PVLP (n=12). Radiographic union, wrist range of motion, Disabilities of the Arm, Shoulder and Hand (DASH) scores, and implant-related complications were compared. Statistical analyses included the Mann-Whitney U test and Fisher exact test.
Results
Radiographic union was achieved in all patients (100%), without secondary displacement or hardware failure. No significant differences were observed between the two groups in wrist flexion (P=0.152), extension (P=0.832), pronation (P=0.792), or supination (P=0.328). The mean DASH scores were 12.8±5.5 in the HP group and 14.6±6.0 in the volar plate group (P=0.449). One patient in the HP group experienced mild flexor tendinopathy that resolved with conservative management. No cases of tendon rupture or early reoperation were reported.
Conclusions
Fixation of volar lunate facet fractures using a HP yielded clinical and radiographic outcomes comparable to those of PVLPs, with a low rate of complications and reliable bony union. Due to its mechanical stability, compatibility with standard surgical approaches, and low risk of flexor tendon irritation, the HP may serve as a valuable alternative for managing volar lunate facet fractures. Level of evidence: IV. -
Citations
Citations to this article as recorded by- Open distal radius fracture with ulnar neurovascular injury treated with dorsal spanning plate fixation and vein interposition grafting: a case report
Kyeong-Eon Kim, Ho-Yong Lee, Shin-Woo Lee, Ji-Sup Kim
Journal of Musculoskeletal Trauma.2026; 39(3): 262. CrossRef
- Open distal radius fracture with ulnar neurovascular injury treated with dorsal spanning plate fixation and vein interposition grafting: a case report
- 1,236 View
- 32 Download
- 1 Crossref
- Correlation of bone mineral density with ankle fractures in older adults in Korea: a retrospective cohort study
- Seung Hyun Lee, Chae Hun Lee, Seo Jin Park, Jun Young Lee
- J Musculoskelet Trauma 2025;38(4):186-192. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00150
-
Abstract
PDF
- Background
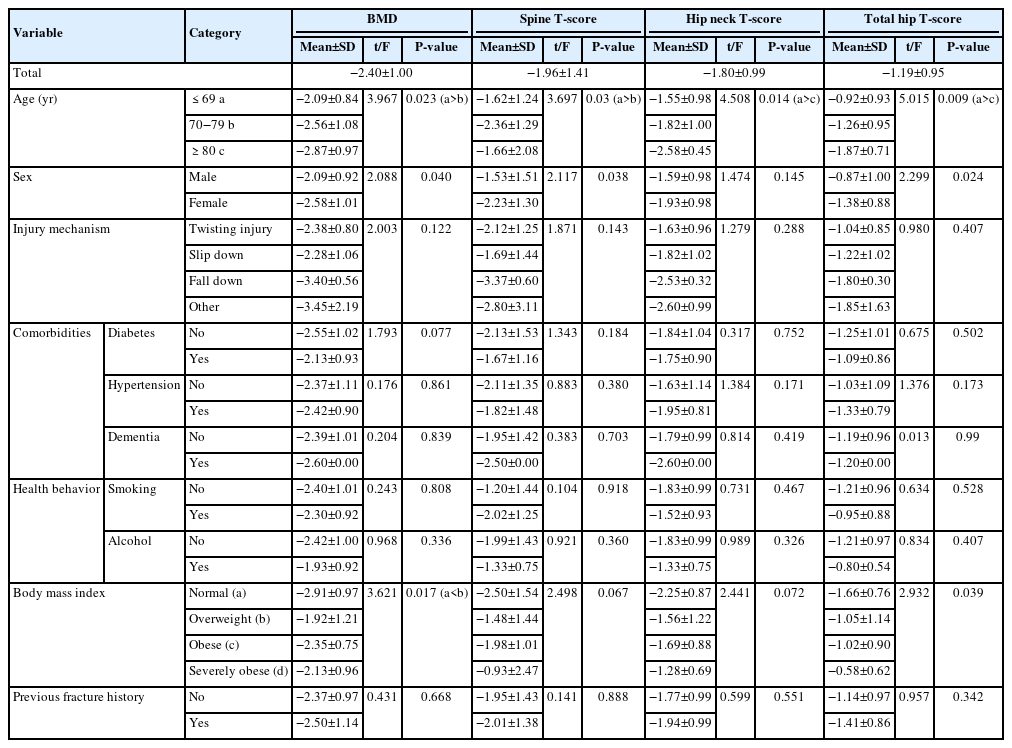
Bone mineral density (BMD) is well-documented in relation to fractures of the spine, hip, distal radius, and proximal humerus; however, its correlations with other fracture types are less established. This study aimed to analyze BMD and associated risk factors in older adults (≥65 years of age) with osteoporotic ankle fractures. These fractures involve low-energy trauma, resulting from falls from a standing height or lower, and occur from impacts which typically do not cause fractures in individuals with normal bone.
Methods
This retrospective study analyzed data from 1,411 patients diagnosed with ankle fractures admitted to Chosun University Hospital between February 2012 and April 2023. After applying inclusion criteria (age ≥65 years; low energy ankle fracture) and exclusion criteria (high energy trauma, open/multiple fractures, missing dual X-ray absorptiometry [DXA]), 73 of 1,411 patients were analyzed. Lumbar spine, femoral neck, and total hip T scores were obtained with a Horizon Wi DXA scanner, and associations with age, sex, mechanism of injury, comorbidities, smoking status, alcohol consumption, body mass index (BMI), and history of fractures were tested by ANOVA with Scheffe post hoc and Fisher exact tests.
Results
Lower BMD correlated significantly with older age, female sex, and lower BMI (P<0.05) in older adults with ankle fractures. No significant associations were observed for comorbidities (diabetes, hypertension, dementia), smoking, alcohol consumption, injury mechanism, or prior fractures.
Conclusion
These results indicate that older age, female, and lower BMI are linked to reduced BMD in ankle fracture patients over 65 years of age. Focused osteoporosis screening and management may therefore be most beneficial for older, low BMI women presenting with ankle fractures. Level of evidence: IV.
- 1,486 View
- 40 Download
Review Articles
- Atypical ulnar fractures: a narrative review of current concepts and a case of bilateral surgical management
- Chi-Hoon Oh, Hyun Tak Kang, Jun-Ku Lee
- J Musculoskelet Trauma 2025;38(3):124-132. Published online July 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00227
-
Abstract
PDF
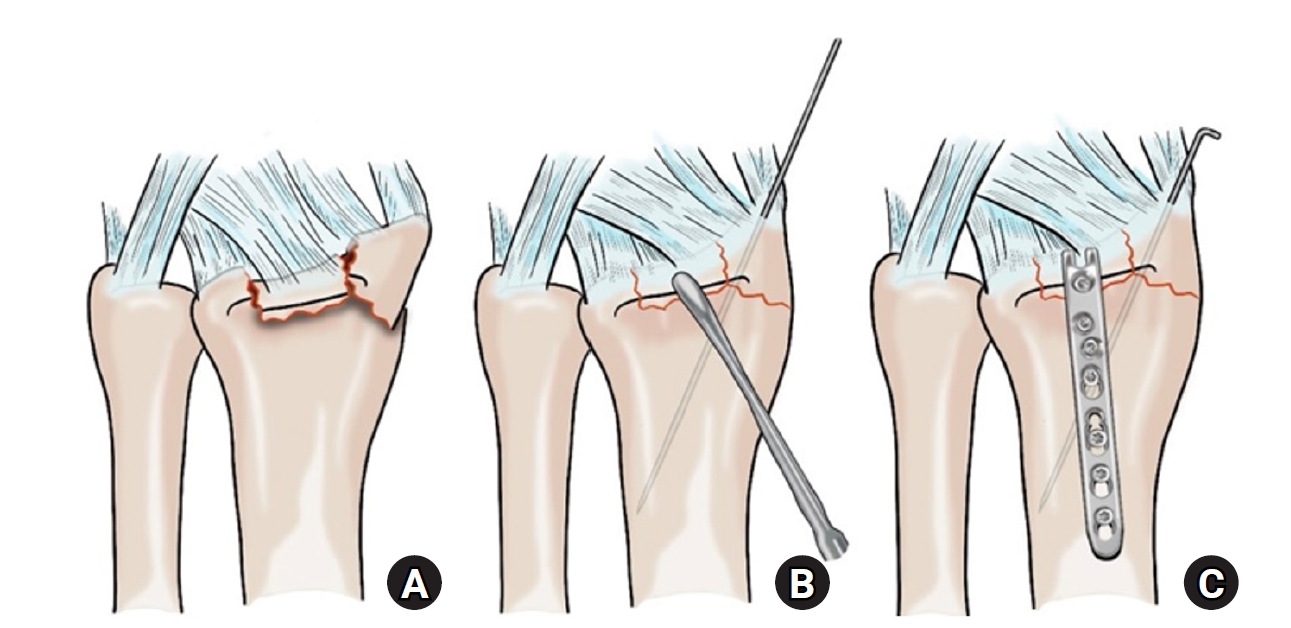
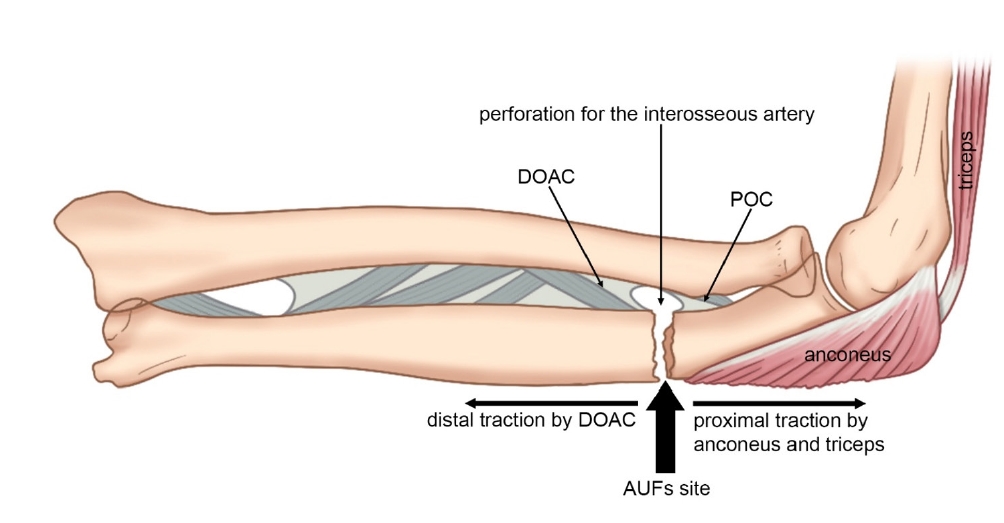
- Atypical ulnar fractures (AUFs) are rare complications that are often linked to long-term antiresorptive therapy. Although atypical femoral fractures are well-studied, AUFs lack standardized diagnostic and treatment protocols. This review summarizes current knowledge on AUFs, including their pathophysiology, diagnostic criteria, and management. A case of bilateral AUFs treated with two distinct osteosynthesis methods is presented, emphasizing the principles of biological healing and mechanical stabilization.
- 2,732 View
- 66 Download
- Current concepts in the management of phalangeal fractures in the hand
- Hyun Tak Kang, Jun-Ku Lee
- J Musculoskelet Trauma 2025;38(3):109-123. Published online July 22, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00136
-
Abstract
PDF
- This review focuses on the treatment of hand fractures based on the anatomical location of the fractured phalanx, excluding the thumb, and examines recent studies on the topic. The main points are as follows: in most cases of hand fractures, conservative treatment should be prioritized over surgical intervention. The three key factors in determining whether surgical treatment is necessary are (1) whether the fracture is intraarticular, (2) the stability of the fracture itself, and (3) the extent of damage to surrounding soft tissues. The primary surgical treatment is closed reduction and Kirschner-wire fixation. The risk of rotational deformity increases with fractures closer to the proximal region. Intra- articular fractures may lead to subsequent stiffness and arthritis; thus, computed tomography is recommended to assess the fracture pattern. Anatomic reduction of intraarticular fragments is required, along with correction of the inherent joint instability. No surgical method has proven to be superior; it is advantageous for the surgeon to choose a surgical approach they are familiar with and confident in, based on the specific fracture and patient factors. Complications in hand fractures are various; the most frequent is stiffness, and nonunion is uncommon. Early joint motion is crucial in minimizing the risk of stiffness.
-
Citations
Citations to this article as recorded by- Imaging of hand and wrist injuries in alpine skiing: common injury mechanisms, imaging findings, and treatment
Andreas Josef Walch, Andreas Schweizer, Reto Sutter
Skeletal Radiology.2026;[Epub] CrossRef
- Imaging of hand and wrist injuries in alpine skiing: common injury mechanisms, imaging findings, and treatment
- 60,584 View
- 768 Download
- 1 Crossref
Original Article
- Computational simulation of coracoclavicular screw insertion through the superior distal clavicular plate for clinical applications in Korean cadavers
- Hyung-Lae Cho, Ji Han Choi, Se-Lin Jeong, Gu-Hee Jung
- J Musculoskelet Trauma 2025;38(3):143-151. Published online July 22, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00122

-
Abstract
PDF
- Background
The study was conducted to determine the practical area for inserting the coracoclavicular (CC) screw through the plate by analyzing three-dimensional (3D) shoulder models featuring virtually implanted, actual-size plates and screws.
Methods
Ninety cadaveric shoulders (41 males and 49 females) underwent continuous 1.0-mm slice computed tomography scans. The data were imported into image-processing software to generate a 3D shoulder model, including the scapula and clavicle. The overlapping area between the clavicle and the horizontal portion of the coracoid process (horizontal portion_CP) was analyzed in the cranial view. A curved pelvic recon plate was virtually placed on the upper surface of the distal clavicle, and an actual-size (3.5 mm) CC screw was inserted through the plate.
Results
The distal clavicle directly overlapped with the horizontal portion_CP in the vertical direction. The overlapping area was sufficient to place the 3.5 mm and 4.5 mm-sized screws. In all shoulder models, the CC screw could be inserted through the plate into the vertical direction, with an average length of 35.5 mm (range, 26.2–62.5 mm; standard deviation, 1.2 mm). In 87 models, the CC screw was inserted through the third hole from the lateral end of the plate. Two models were inserted through the second hole, and one model through the fourth hole.
Conclusions
The upper surface of the clavicle has sufficient overlapping area to place CC screws through the plate in the vertical direction in the corresponding hole. Supplemental CC screw fixation through the plate can be performed without additional or special equipment. Level of evidence: IV
- 1,254 View
- 26 Download
Review Articles
- How to obtain the desired results from distal tibial nailing based on anatomy, biomechanics, and reduction techniques
- Jungtae Ahn, Se-Lin Jeong, Gu-Hee Jung
- J Musculoskelet Trauma 2025;38(2):74-85. Published online March 31, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00024

-
Abstract
PDF
- Distal tibial metaphyseal fractures are commonly caused by high-energy injuries in young men and osteoporosis in older women. These fractures should be clearly distinguished from high-energy pilon fractures. Although the optimal surgical intervention methods for distal tibial metaphyseal fractures remain uncertain and challenging, surgical treatments for nonarticular distal tibia fractures can be broadly divided into two types: plate fixation and intramedullary nail (IMN) fixation. Once functional reduction is achieved using an appropriate technique, distal tibial nailing might be slightly superior to plate fixation in reducing postoperative complications. Thus, the surgical strategy should focus on functional realignment and proceed in the following sequence: (1) restoring the original tibial length, regardless of whether fibular fixation is to be done; (2) making the optimal entry point through an anteroposterior (AP) projection based on the overlapping point between the fibular tip and lateral plateau margin; (3) placing Kirschner wires (Ø2.4 mm) as blocking pins (in the AP orientation for coronal control and in the mediolateral [ML] orientation for sagittal control) as close to the upper locking hole as possible without causing further comminution on the concave aspect of the short fragment; and (4) making the the distal fixation construct with at least two ML and one AP interlocking screw or two ML interlocking screws and blocking screws. After the IMN is adequately locked, blocking pins (Ø2.4 mm) need to be replaced by a 3.5 mm screw.
-
Citations
Citations to this article as recorded by- Rigid intramedullary nailing with suprapatellar approach for tibial shaft fractures in adolescents with open physes
Jong Wha Lee, Jae Ho Cho, Tae Hun Kim, Hyung Keun Song, Won-Tae Cho, Seungyeob Sakong, Hyun Il Choi, Sumin Lim
Injury.2026; 57(4): 113130. CrossRef - Impact of Foot Width on Patient-Reported Outcomes Assessed by 3-Dimensional Foot Morphometry in Hallux Valgus
Jungtae Ahn, Dae-Cheol Nam, Gu-Hee Jung
Clinics in Orthopedic Surgery.2025; 17(6): 1062. CrossRef
- Rigid intramedullary nailing with suprapatellar approach for tibial shaft fractures in adolescents with open physes
- 5,599 View
- 119 Download
- 2 Crossref
- Atypical femoral fractures: an update
- Won-Tae Cho, Jeong-Hyun Koh, Seungyeob Sakong, Jung-Taek Kim
- J Musculoskelet Trauma 2025;38(2):41-52. Published online March 28, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00031
-
Abstract
PDF
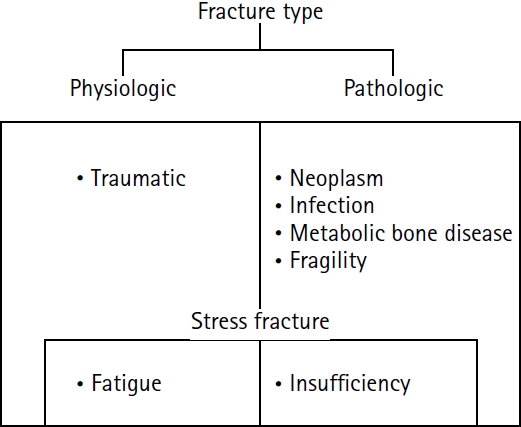
- This narrative review provides an up-to-date overview of atypical femoral fractures (AFFs), emphasizing diagnostic criteria, epidemiology, pathophysiology, risk factors, and evaluation with screening strategies. AFFs are rare but significant complications associated with prolonged bisphosphonate (BP) therapy for osteoporosis. Although the pathogenesis of AFFs has not been fully elucidated, its primary mechanism is thought to involve impaired bone remodeling, leading to unhealed microfractures that progress to stress fractures under repetitive loading. AFFs can occur in various regions of the femur, influenced by femoral geometry and the lower limb axis. Other risk factors include prolonged steroid use, arthroplasty, genetic predispositions, and metabolic bone disorders. The diagnosis of AFFs is based on criteria established by the American Society for Bone and Mineral Research. Key radiographic features include lateral cortical transverse fracture lines and localized cortical thickening, typically with minimal or no comminution on the medial cortex. Dual-energy X-ray absorptiometry for screening tests and magnetic resonance imaging as an advanced imaging modality enable the early detection of incomplete fractures. This multi-modal approach facilitates the prompt identification of prodromal cortical changes, reducing the risk of complete fractures in high-risk populations, particularly patients undergoing prolonged BP therapy. Level of Evidence: V
-
Citations
Citations to this article as recorded by- Clinical Images: Bisphosphonate‐associated atypical femoral fracture with contralateral cortical beaking
Andreina Martinez Paulino, Valentin Marian
ACR Open Rheumatology.2026;[Epub] CrossRef - Atypical femoral fracture: The periprosthetic variant about two cases without bisphosphonate use
Guillaume Auberger, Thomas Aubert, Younes Kerroumi, Philippe Leclerc, Simon Marmor
SICOT-J.2026; 12: 41. CrossRef - Atypical Femur Fractures Without Bisphosphonate Exposure (AFFwB): A Retrospective Report of 21 Cases
Lorenzo Lucchetta, Carmelinda Ruggiero, Samuele Berardi, Alice Franceschi, Michele Bisaccia, Giuseppe Rinonapoli
Journal of Clinical Medicine.2025; 15(1): 25. CrossRef
- Clinical Images: Bisphosphonate‐associated atypical femoral fracture with contralateral cortical beaking
- 65,535 View
- 697 Download
- 3 Crossref
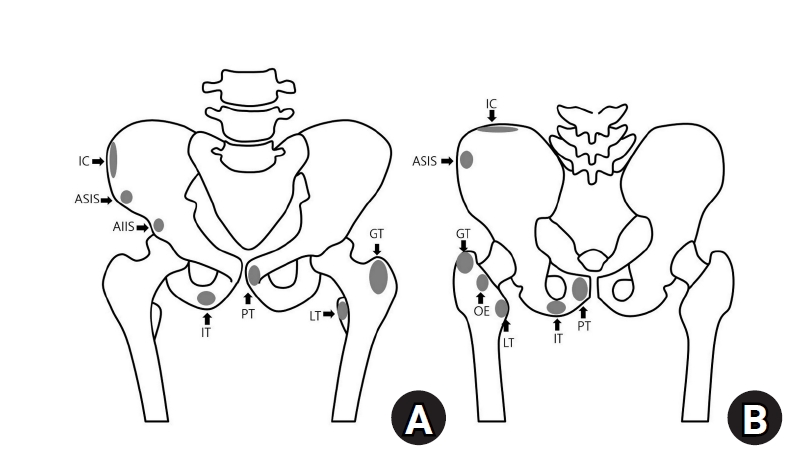
- Avulsion fractures around the hip joint and pelvis
- Won-Sik Choy, Yonghan Cha, Jung-Taek Kim, Jun-Il Yoo, Jin-Woo Kim
- J Musculoskelet Trauma 2025;38(2):53-62. Published online March 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00010
-
Abstract
PDF
- Avulsion fractures occur when tendons or ligaments are subjected to forces greater than they can withstand at the apophysis or enthesis, regardless of fusion status. The pelvis and hip joint are vulnerable to these injuries due to the diverse muscular structures in these structures, which serve as origins for multiple muscles leading to the lower extremities. Pelvic avulsion fractures commonly affect young athletes, but can also occur in adults. The diagnosis typically involves assessing trauma history, a clinical examination, and radiographic imaging. If the diagnosis is unclear, additional tests such as computed tomography and magnetic resonance imaging may assist in the diagnosis and provide useful information for treatment decisions. While most avulsion fractures respond well to conservative treatment, surgical intervention may be preferred in severe displacements, cases of significant retraction in active athletes, or when a faster recovery is necessary. Chronic or neglected injuries may lead to excessive osseous formation around the pelvis, causing impingement syndromes. Recognizing characteristic radiological findings based on pelvic anatomy helps to make an accurate diagnosis, as chronic injuries can mimic tumors or infectious conditions, necessitating a careful differential diagnosis.
-
Citations
Citations to this article as recorded by- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
Dawid Bartosik, Bartlomiej Cwikla, Anna Kowalczyk, Michalina Loson-Kawalec, Anna Palka-Szymaniec, Bartosz Starzynski, Alina Keska, Jakub Szkuta, Klaudia Wojcik
Cureus.2026;[Epub] CrossRef - Outcomes of Conservative Versus Surgical Treatment of Adolescent Pelvic and Hip Avulsion Fractures: A Systematic Review and Meta-Analysis
Lindsey L. Molina, Andrew M. Block, Sasha Carsen, Allison E. Crepeau, Tyler J. Stavinoha, Michael M. Chau, Jeffrey J. Nepple
Journal of Pediatric Orthopaedics.2026;[Epub] CrossRef - Diagnostic Accuracy of Ultrasound for Adolescent Pelvic Avulsion Fractures: A Blinded Multirater Study
Meena Meiyyappan, Robert Van Pelt, Kate Lampe, Jane Chung, Matthew Ditzler, Shane Miller, Henry Ellis, Hamza Alizai, Matthew Hammer, Ben Johnson, Charles Wyatt, Jacob Jones
Journal of Clinical Ultrasound.2026;[Epub] CrossRef
- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
- 19,932 View
- 209 Download
- 3 Crossref
Original Article
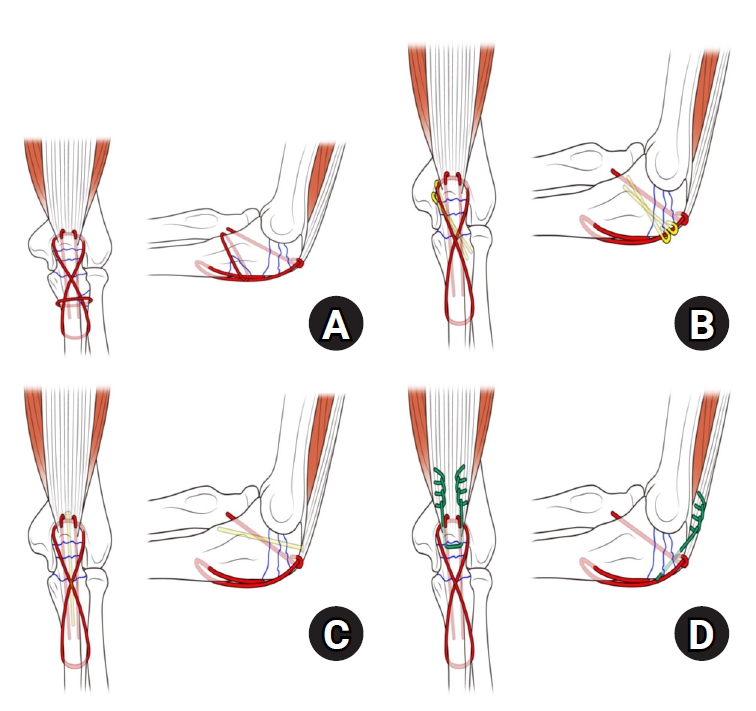
- Comparison of outcomes of reinforced tension band wiring and precontoured plate and screw fixation in the management of Mayo type IIIB olecranon fractures
- Hyun Goo Kang, Tong Joo Lee, Samuel Jaeyoon Won
- J Musculoskelet Trauma 2025;38(2):96-101. Published online February 28, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00059
- Correction in: J Musculoskelet Trauma 2025;38(3):168
-
Abstract
PDF
- Background
Mayo type IIIB olecranon fractures are characterized by significant displacement and comminution, presenting a challenge in selecting the appropriate fixation technique. This study compared the clinical and radiographic outcomes, complications, and reoperation rates of reinforced tension band wiring (TBW) and precontoured plate and screw fixation (PF) in the surgical treatment of Mayo type IIIB olecranon fractures.
Methods
This retrospective review analyzed 24 patients diagnosed with Mayo type IIIB olecranon fractures, who were treated between 2005 and 2023. Of these, 11 patients underwent reinforced TBW, and 13 received precontoured PF. Clinical outcomes were assessed using Disabilities of the Arm, Shoulder, and Hand (DASH) scores and the Mayo Elbow Performance Score (MEPS). Radiographic outcomes focused on fracture union. Operative times, complication rates, and reoperation rates were compared between the groups.
Results
Both the reinforced TBW and PF groups achieved satisfactory clinical outcomes, with no significant between-group differences in DASH and MEPS scores (P>0.05). Radiographic union was achieved in all patients. The reinforced TBW group demonstrated a significantly shorter operative time than the PF group (93.6±7.4 min vs. 132.3±13.7 min; P<0.001). Complication rates were similar between the two groups (reinforced TBW, 38.4%; PF, 36.3%), but hardware-related irritation occurred more frequently in the reinforced TBW group. Reoperations were required in 15.8% of the reinforced TBW group due to hardware irritation, whereas no reoperations were necessary in the PF group.
Conclusions
Reinforced TBW and PF are both effective surgical options for managing Mayo type IIIB olecranon fractures, yielding comparable clinical and radiographic outcomes. While reinforced TBW offers shorter operative times and lower costs, PF is associated with fewer hardware-related complications. Further prospective studies are needed to optimize treatment strategies for these complex fractures. Level of Evidence: Level III. -
Citations
Citations to this article as recorded by- Suture tension band fixation of olecranon fractures: description and early outcomes of a novel technique
Joseph G. Monir, Frank L. Vazquez, Musab Gulzar, Kevin Cuneo, Thomas McQuillan, Michael B. Gottschalk, Eric R. Wagner
JSES Reviews, Reports, and Techniques.2026; 6(2): 100707. CrossRef - Comparative Efficacy and Safety of Tension Band Wiring versus Plate Fixation for Olecranon Fractures: A Meta-Analysis and Trial Sequential Analysis of Randomized Clinical Trials
Malik A. Alshayban, Amr Khaleel Ibraheem, Abdulrahman Ali Aloudah, Turki S. Alqahtani, Mohamed Nabawy Elseaidy, Mohammed Abdelmalek, Mohamed Abdelhady Mourad
JSES Reviews, Reports, and Techniques.2026; : 100817. CrossRef - Are posterior olecranon locking plates a problem for patients after fracture healing because of prominence?
Reva Qiu, Mallika Makkar, Richard Buckley
Injury.2025; 56(11): 112769. CrossRef
- Suture tension band fixation of olecranon fractures: description and early outcomes of a novel technique
- 3,829 View
- 62 Download
- 3 Crossref
Review Article
- Easily missed nondisplaced fractures accompanying complete fractures in the lower extremity and pelvis: a narrative review
- Young-Chang Park
- J Musculoskelet Trauma 2025;38(1):5-12. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00017

-
Abstract
PDF
- Nondisplaced fractures accompanying complete fractures are often difficult to detect on plain radiographs or computed tomography scans, posing a diagnostic challenge. The diagnosis of these frequently overlooked injuries can be delayed, potentially leading to suboptimal patient outcomes. This review discusses four commonly missed fracture patterns in the lower extremity and pelvis, including posterior involvement in fragility fractures of the pelvis, intertrochanteric extensions in isolated greater trochanter fractures, ipsilateral femoral neck fractures in high energy femoral shaft fractures, and posterior malleolar fractures in distal spiral tibial shaft fractures. An accurate diagnosis of these accompanying nondisplaced fractures is critical for optimizing surgical outcomes. Surgeons should incorporate thorough preoperative evaluations into their clinical practice to facilitate early detection and appropriate treatment strategies. Prompt identification and comprehensive management remain essential for improving patient outcomes.
-
Citations
Citations to this article as recorded by- Selective Anterior Fixation for Rami Fractures in Anteroposterior Compression-Type Pelvic Ring Injuries: Impact of Posterior Stability
Jeong-Hyun Koh, Sumin Lim, Won-Tae Cho, Seungyeob Sakong, Wan-Sun Choi, Daehyun Han, Hyung Keun Song
Journal of Clinical Medicine.2026; 15(10): 3773. CrossRef - Initial lateral stress radiographs predict instability in fragility fractures of the pelvis type I and II: a prospective observational study
Kyu-Hyun Yang, Jun-Young An, Young-Chang Park
Scientific Reports.2026;[Epub] CrossRef
- Selective Anterior Fixation for Rami Fractures in Anteroposterior Compression-Type Pelvic Ring Injuries: Impact of Posterior Stability
- 4,180 View
- 65 Download
- 2 Crossref
Original Articles
- Outcomes of open reduction and internal fixation using 2.0/2.4 mm locking compression plate in isolated greater tuberosity fractures of humerus
- Sung Choi, Dongju Shin, Sangwoo Kim, Byung Hoon Kwack
- J Musculoskelet Trauma 2025;38(1):32-39. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00005

-
Abstract
PDF
- Background
The purpose of this study was to retrospectively evaluate the radiographic and clinical results of a small single or double low-profile plate fixation of 2.0/2.4 mm locking compression plate (LCP) in treating isolated greater tuberosity (GT) fractures of the humerus. Methods: From June 2015 to October 2022, patients who underwent LCP in treating isolated GT fractures of the humerus were included in this study. The radiological and clinical results were analyzed in 15 patients who underwent open reduction and internal fixation used 2.0/2.4 mm LCP. Results: Bone union was achieved in 14 patients (93.3%) and one failed case was treated with a 2.4 mm single LCP fixation. Radiological union was achieved within 10–20 weeks. Complications occurred in two patients (13.3%), including the reduction failure and shoulder stiffness. At the final follow-up, the average clinical scores were as follows: a visual analog scale for pain of 2.1 (range, 0–5) and a University of California, Los Angeles score of 27.2 (range, 18–31). Regarding range of motion (ROM), the average active ROMs were 142° for forward flexion (range, 120°–150°), 147.1° for abduction (range, 120°– 180°), and 59.3° for external rotation (range, 45°–80°). For internal rotation, the average was observed to reach the 10th thoracic vertebra (range, 1st lumbar vertebra–7th thoracic vertebra). Conclusions: The clinical and radiologic outcomes of treating isolated GT fracture using 2.0/2.4 mm LCP were favorable, and double low-profile plate fixation may be beneficial for sufficient fracture stability if possible. Level of evidence: Level IV, case series.
- 3,563 View
- 76 Download
- Interpositional tricortical iliac bone graft in nonunion of midshaft clavicular fractures
- Eun-Seok Son, Bum-Soon Park, Chang-Jin Yon, Chul-Hyun Cho
- J Musculoskelet Trauma 2025;38(1):23-31. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00004

-
Abstract
PDF
- Background
The purpose of this study was to investigate the radiological and clinical outcomes after interpositional tricortical iliac bone graft with plate fixation for the nonunion of clavicle midshaft fractures. Methods: Between 2007 and 2020, 17 cases who were treated by interpositional tricortical iliac bone graft with plate fixation for the clavicle midshaft nonunion combined with bone defect were investigated. The mean age was 53 years (range, 22–70 years). The mean follow-up period was 102.2 months (range, 18–193 months). Serial plain radiographs were used to evaluate radiological outcomes. The University of California, Los Angeles (UCLA) score, American Shoulder and Elbow Surgeons (ASES) score, and Quick-disabilities of the arm, shoulder, and hand (DASH) score were used to evaluate clinical outcomes. Complications were also evaluated. Results: All cases achieved complete bony union with mean healing time of 17.6 weeks (range, 14–22 weeks). The mean clavicle length difference was significantly decreased from 9.1 mm preoperatively to 2.6 mm postoperatively (P<0.001). The mean UCLA and ASES scores were significantly improved from 18.1 and 52.2 before surgery to 30.6 and 88.6 after surgery (both P<0.001), respectively. The mean final Quick-DASH score was 18.0. Three cases (17.6%) developed postoperative complications including two cases of shoulder stiffness and one case of screw irritation. Conclusions: Interpositional tricortical iliac bone graft with plate fixation for the clavicle midshaft nonunion demonstrated excellent radiological and clinical outcomes. In cases of atrophic nonunion combined with bone defect, this technique is an effective option that can provide structural support and restore clavicle length. Level of evidence: Level IV, case series.
- 3,747 View
- 60 Download
Review Article
- Avulsion Fractures in the Ankle and Foot
- Gyeong Hoon Lim, Jae Won Kim, Sung Hyun Lee
- J Korean Fract Soc 2024;37(2):102-116. Published online April 30, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.2.102
-
Abstract
PDF
- An avulsion fracture occurs when a muscle-tendon unit attached to a bone produces sufficient force to tear a fragment of the bone. If not treated properly, this injury can lead to deformity, nonunion, malunion, pain, and disability. Although avulsion fractures around the foot and ankle can occur anywhere there are tendon and ligament attachments, they are common in the anterior talofibular ligament, anterior-inferior tibiotalar ligament, calcaneal tuberosity, the base of the fifth metatarsal, and navicular bone. The optimal treatment for each fracture depends on the location and severity of the fracture. Conservative treatment involves limiting weight bearing for a period, splint immobilization, and using various orthoses. Surgical treatment is usually reserved for cases of severe displacement or when nonsurgical treatment has failed. The goals of surgery include reduction of the fracture fragment, prevention of nonunion or malunion and soft tissue injury, and early return to function. The decision for each treatment modality may depend on the patient demographics or preferences and the surgeon experience. This review summarizes previous and current views on the pathogenesis, diagnosis, and treatment of common avulsion fractures to guide the treatment and diagnosis.
- 5,111 View
- 73 Download
Original Article
- Effect of Additional Medial Locking Plate Fixation and Autogenous Bone Graft for Distal Femur Nonunion after Lateral Locking Plate Fixation
- Ho Min Lee, Jong Pil Kim, In Hwa Baek, Han Sol Moon, Sun Kyo Nam
- J Korean Fract Soc 2024;37(1):30-38. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.30
-
Abstract
PDF
- Purpose
This study examined the outcomes of additional medial locking plate fixation and autogenous bone grafting in the treatment of nonunions that occurred after initial fixation for distal femoral fractures using lateral locking plates.
Materials and Methods
The study involved eleven patients who initially underwent minimally invasive lateral locking plate fixation for distal femoral fractures between January 2008 and December 2020. The initial procedure was followed by additional medial locking plate fixation and autogenous bone grafting for clinically and radiographically confirmed nonunions, while leaving the stable lateral locking plate in situ. A clinical evaluation of the bone union time, knee joint range of motion, visual analog scale (VAS) pain scores, presence of postoperative complications, and functional evaluations using the lower extremity functional scale (LEFS) were performed.
Results
In all cases, bone union was achieved in an average of 6.1 months after the secondary surgery. The range of knee joint motion, weight-bearing ability, and VAS and LEFS scores improved at the final follow-up compared to the preoperative conditions. All patients could walk without walking assistive devices and did not experience pain at the fracture site. On the other hand, three patients complained of pain in the lateral knee joint caused by irritation by the lateral locking plate; hence, lateral hardware removal was performed. One patient complained of mild paresthesia at the anteromedial incision site. Severe complications, such as deep infection or metal failure, were not observed.
Conclusion
For nonunion with stable lateral locking plates after minimally invasive lateral locking plate fixation of distal femur fractures, additional medial locking plate fixation and autogenous bone grafting, while leaving the lateral locking plate intact, can achieve successful bone union.
- 803 View
- 9 Download
Review Articles
- Fracture-Related Complication: Fat Embolism Syndrome
- Beom-Soo Kim
- J Korean Fract Soc 2023;36(3):95-102. Published online July 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.3.95
-
Abstract
PDF
- Fat embolization is a common occurrence after trauma or during orthopedic procedures involving intramedullary manipulation. Although uncommon, fat embolism syndrome (FES) with respiratory failure, neurologic dysfunction, and petechial rash can be fatal to patients. Two theories are proposed for the manifestation of FES: in the mechanical theory, FES occurs when fat tissue in the bone marrow enters the bloodstream and mechanically blocks it; the biochemical theory proposes that FES occurs due to an inflammatory reaction caused by free fatty acids. There are currently no clear diagnostic criteria for FES, and symptoms and signs are typically nonspecific. For the treatment of FES, conservative and supportive management is performed for the specific symptoms, and close monitoring of the respiratory and neurologic systems is required in high-risk groups. Early fracture fixation of long bones helps prevent and reduce the severity of fat embolism.
- 2,064 View
- 17 Download
- Treatment of Scaphoid Fractures and Nonunions
- Wan-Sun Choi
- J Korean Fract Soc 2022;35(4):182-189. Published online October 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.4.182
-
Abstract
PDF
- A scaphoid fracture is one of the most common types of wrist fractures, and if treatment is delayed, there is a high possibility of nonunion due to anatomical factors such as limited blood supply to the injured bone. Therefore, it is important to suspect a scaphoid fracture based on the mechanism of wrist injury and physical examination of the patient. A computed tomography scan or magnetic resonance imaging can also aid early diagnosis of the fracture. Stable acute fractures can be treated conservatively, but unstable fractures require surgical treatment, and percutaneous screw fixation is usually performed. Nonunions require bone grafts and are treated with non-vascularized bone grafts and screw fixation. However, if the nonunion is located at the proximal pole, a vascularized bone graft may be considered because there is a possibility of avascular necrosis. Pedicled vascularized and free vascularized medial femoral condyle bone grafts are mainly used in such cases. The treatment of a proximal pole nonunion with impaired blood flow remains controversial. There are conflicting opinions on whether a nonvascularized bone graft is sufficient or whether a vascularized bone graft is necessary.
- 1,595 View
- 13 Download
Original Article
- Benefits of a Demineralized Bone Matrix in Osteoporotic Intertrochanteric Femoral Fracture Patients
- Se Jin Kim, Hong-Man Cho, Myung Cheol Jung
- J Korean Fract Soc 2022;35(4):151-161. Published online October 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.4.151
-
Abstract
PDF
- Purpose
Osteoporosis causes various fixation failures in patients with intertrochanteric fractures. This study aimed to investigate the effect of a demineralized bone matrix (DBM) for cancellous or cortical bone defects on internal fixation in older osteoporotic patients with intertrochanteric fractures.
Materials and Methods
Among patients with intertrochanteric fractures who underwent surgical treatment from January 2016 to December 2021 at a facility, 171 patients were AO/OTA type 31-A1 and type 2 fractures which are considered relatively stable. The patients were grouped based on DBM use (Group A: DBM use, Group B: DBM non-use), and their clinical and radiology results were analyzed retrospectively. The patients were then subdivided into Group A-a and -b after removing factors that could cause treatment failures, such as the reduction status and location of the helical blade, and then further subdivided (Group A-a-1/2/3/4 and Group B-b-1/2/3/4) according to cancellous or cortical bone defects that could accompany intertrochanteric fractures. The time to full weight-bearing (FWB) and Harris hip score (HSS) 3 months after surgery in these subgroups were investigated.
Results
There was no significant difference in the clinical radiology results and complications between Group A and Group B. However, the time to FWB (p<0.001) and HSS (p=0.029) were significantly superior in Group A. In Group A-a with DBM use, after removing the risk factors for intertrochanteric fracture failure, the time to FWB (p=0.055) was close to the significance level, and HSS (p=0.036) was significantly superior. In Group A-a-1 (cancellous defect only) and Group A-a-3 (cancellous and cortical defect), the time to FWB (p=0.088, 0.052) was close to the significance level, and the HSS (p=0.039, 0.018) was significantly superior when DBM was used.
Conclusion
In patients with intertrochanteric fractures of AO/OTA type 31-A2.3 or less, if stable reduction and firm fixation are achieved, selective DBM use may help early recovery after surgery.
- 953 View
- 6 Download
Review Articles
- Perilunate Dislocation and Perilunate Fracture-Dislocation
- Jung Il Lee
- J Korean Fract Soc 2022;35(3):114-119. Published online July 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.3.114
-
Abstract
PDF
- Perilunate dislocations and perilunate fracture-dislocations are one of the most severe forms of wrist injuries and are generally caused by high-energy trauma such as falls from a height or traffic accidents. Prompt recognition and immediate, gentle closed reduction are critical, but diagnosis can often be missed at the initial presentation. The current standard management is open reduction, ligamentous and bony repair, and supplemental fixation for the protection of the repair. The pathomechanics of the injury, diagnosis by plain wrist radiographs, closed reduction techniques, current surgical treatments, and complications are presented in this review.
- 1,155 View
- 10 Download
- Lisfranc Joint Injury
- Bi O Jeong, Jungtae Ahn
- J Korean Fract Soc 2022;35(2):83-89. Published online April 30, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.2.83
-
Abstract
PDF
- The Lisfranc joint complex is composed of complex bony structures, ligaments, and soft tissues and has a systematic interrelationship. Sufficient radiologic modalities should be considered for an accurate initial diagnosis. Based on an accurate understanding of normal anatomy and restoration of anatomical relationships, the diagnosis should be obtained, and more discussion is needed on detailed treatment strategies.
- 2,193 View
- 16 Download
Original Articles
- Minimal Invasive Fixation Methods for the Metacarpal Fracture
- Ki Youn Kwon, Jin Rok Oh, Ji Woong Kwak
- J Korean Fract Soc 2022;35(1):9-15. Published online January 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.1.9
-
Abstract
PDF
- Purpose
This study compared the radiologic and clinical outcomes of metacarpal fractures treated with two minimally invasive surgical techniques: Kirschner wire (K-wire) fixation and headless screw fixation.
Materials and Methods
This study included 52 patients (46 males and 6 females; age 18-55 years) with distal metacarpal fractures (middle and distal shaft, including the neck) who had undergone K-wire fixation or headless screw fixation. All subjects were followed up for at least six months. The radiologic assessments were performed to evaluate the angular deformity and shortenings. The total active motion (TAM), grip strength, and patients’ subjective functional assessment were measured to evaluate the hand function. The time taken to return to work (RTW) and adverse events were analyzed.
Results
Of the 52 cases, metacarpal fractures treated with headless screw fixation and K-wire fixation showed a significant difference associated with early RTW (p<0.05). There were no significant differences between the subjects treated with K-wire fixation and those with headless screw fixation in terms of the radiologic measurement, hand function examinations, complications, and adverse events (p>0.05).
Conclusion
After a six-month follow-up, minimally invasive K-wire fixation and headless screw fixation produced similar clinical and radiologic outcomes in subjects with metacarpal fractures. Compared to K-wire fixation, however, headless screw fixation led to earlier functional recovery and might be a better option for treating metacarpal fractures in this regard.
- 902 View
- 6 Download
- Comparing Outcomes of Retrograde Intramedullary Nail and Locking Plate Fixation in Distal Femoral Fractures
- Byung-Ho Yoon, Bo Kwon Hwang, Hyoung-Keun Oh, Suk Kyu Choo, Jong Min Sohn, Yerl-Bo Sung
- J Korean Fract Soc 2021;34(4):131-136. Published online October 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.4.131
-
Abstract
PDF
- Purpose
We compared the radiological and clinical results of fixation for distal femoral fracture (DFF) using a locking compression plate (LCP) or a retrograde intramedullary nail (RIN).
Materials and Methods
From October 2003 to February 2020, 52 cases of DFF with a minimum 1-year follow-up (with a mean follow-up of 19.1 months) were included: 31 were treated with LCP and 21 with RIN. The operation time, blood loss, and hospitalization period were compared, and the incidence of postoperative nonunion, malunion, delayed union and metal failure and other post-operative complications were evaluated and compared.
Results
There was no significant difference in the operating time between the two groups, but the mean blood loss was significantly higher in the LCP group (LCP 683.5 ml vs RIN; 134.9 ml; p=0.015). In 49 out of 52 cases, bone union was achieved without additional surgery in an average of 6.8 months, and a complete union was achieved after additional surgery in three cases of nonunion (LCP 2 cases vs RIN 1 case; p=0.065). One case of malunion and superficial infection was confirmed in each group.
Conclusion
Internal fixation using LCP and RIN give good outcomes with a low complication rate and can therefore be considered useful surgical treatments for DFF.
- 858 View
- 7 Download
Review Articles
- Bone Substitutes: From Basic to Current Update
- Jong Seong Han, Hyung Keun Song
- J Korean Fract Soc 2020;33(4):238-244. Published online October 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.4.238
-
Abstract
PDF
- Bone substitutes are being used increasingly in bony surgery as more than two million bone grafts are performed worldwide per year. Autobone grafts represent the gold standard for bone grafting, but morbidity and limited availability are the main problems. Allobone grafts are osteoconductive, but there are still concerns regarding the infection risks, costs, and donor availability issues. As an alternative, widely used ceramic-based synthetic bone substitutes are based alternatively on calcium (hydroxyapatite, tricalcium phosphate, calcium sulfate, calcium phosphate). Ceramic-based bone substitutes are osteoconductive, but they are weaker than cortical bone and are not osteoinductive. Bone morphogenic protein, demineralized bone matrix, and platelet-rich plasma are used to obtain an osteoinductive function. Recently, cell-based and gen-based bone substitutes were developed and studied. This paper reviews the basic information and the latest concepts on bone grafts and bone substitutes.
-
Citations
Citations to this article as recorded by- Tannic acid-modified magnesium oxychloride bone cement with high water resistance and osteogenic properties
Junying Chen, Yijia Guan, Yue Yang, Tingting Ma, Jinlun Feng, Wenjie Guo, Qifang Wang, Yanru Zhang, Jianguo Liao
Ceramics International.2024; 50(24): 53407. CrossRef - Surface modification of magnesium with a novel composite coating for application in bone tissue engineering
Jorgimara de O. Braga, Diogo M.M. dos Santos, Fernando Cotting, Vanessa F.C. Lins, Nádia M. Leão, Daniel C.F. Soares, Eric M. Mazzer, Manuel Houmard, Roberto B. Figueiredo, Eduardo H.M. Nunes
Surface and Coatings Technology.2022; 433: 128078. CrossRef
- Tannic acid-modified magnesium oxychloride bone cement with high water resistance and osteogenic properties
- 1,909 View
- 16 Download
- 2 Crossref
- Current Concepts of Bone Healing
- Dong Hun Suh, Bong Mo Koo, Jong Woo Kang
- J Korean Fract Soc 2020;33(3):171-177. Published online July 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.3.171
-
Abstract
PDF
- Bone injuries induce an inflammatory response that promotes bone healing. On the other hand, an aberrant process, where inflammation becomes chronic, can inhibit the healing of injured bone. At the first stage of the bone healing process, inflammatory cells, such as neutrophils and macrophages, are assembled and secrete various cytokines, chemokines, and growth factors. During callus formation, cells differentiated from mesenchymal stem cells, such as osteoblasts and chondrocytes, play leading roles in bone healing. Currently, various treatment modalities have been developed through the known mechanism of bone healing, and the clinical outcomes of bone defect and fracture nonunion have been good.
- 3,181 View
- 138 Download
Case Report
- Treatment of Atypical Ulnar Fracture Associated with Bisphosphonate Therapy - A Case Report -
- Dong-Soo Kim, Ji-Kang Park, Eui-Sung Choi, Ho-Seung Jeong, Seok-Hyun Hong, Byung-Hyun Ahn
- J Korean Fract Soc 2020;33(2):101-104. Published online April 30, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.2.101
-
Abstract
PDF
- Bisphosphonates can cause atypical fractures when taken for a long time. Atypical fractures appear mainly as femoral subtrochanteric or shaft fractures. On the other hand, reports of atypical fractures in the proximal ulna are relatively rare, with a high proportion of nonunion cases. This paper reports a case of nonunion after fixation for atypical fractures of the proximal ulna.
- 832 View
- 3 Download
Original Articles
- Failure of Intramedullary Nailing for Subtrochanteric Atypical Femoral Fractures Caused by Endosteal Cortical Thickening
- Young Ho Roh, Kimoon Kang, Hee Joong Kim, Kwang Woo Nam
- J Korean Fract Soc 2019;32(4):211-221. Published online October 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.4.211
- Correction in: J Musculoskelet Trauma 2020;33(1):63
-
Abstract
PDF
- PURPOSE
Recent literature has noted incidences of subtrochanteric atypical femoral fractures (AFFs) in patients who have taken long-term bisphosphonates (BPs). Most cases of subtrochanteric AFFs have been treated with intramedullary nailing and cases of delayed union have been reported. On the other hand, there is no data available on the complications associated with endosteal thickening or cortical thickening. This study evaluated the results of surgical treatment according to the endosteal thickening of the lateral cortex in subtrochanteric AFFs.
MATERIALS AND METHODS
Investigation was performed at the Department of Orthopaedic Surgery, Jeju National University Hospital. The study consisted of patients with subtrochanteric AFFs, defined by the American Society for Bone and Mineral Research (ASBMR) major criteria, who underwent intramedullary nailing from March 2012 to October 2014. The cases were categorized into two groups based on the presence of endosteal thickening. The evaluation included the demographic data, radiographic data of initial reduction state, and duration of BPs.
RESULTS
The demographic data and duration of BPs were similar in the two groups. On the other hand, varus reduction (Group I: 12.5% vs. Group II: 78.9%; p=0.001), delayed union (Group I: 0% vs. Group II: 70.0%; p=0.003), nonunion (Group I: 0% vs. Group II: 47.4%; p=0.017), and union time (Group I: 5.5 months vs. Group II: 8.3 months; p<0.001) were significantly different in the two groups.
CONCLUSION
Endosteal thickening of the lateral cortex in subtrochanteric AFFs was identified as an independent factor that decides the reduction of the fracture and nonunion. The endosteal thickening should be removed to obtain anatomical alignment for successful surgical results. -
Citations
Citations to this article as recorded by- Controlled bending of proximal femoral nails used in fractures of bowed femurs: biomechanical study with clinical application
Hong Moon Sohn, Suenghwan Jo
Medical Biological Science and Engineering.2022; 5(2): 63. CrossRef
- Controlled bending of proximal femoral nails used in fractures of bowed femurs: biomechanical study with clinical application
- 2,111 View
- 19 Download
- 1 Crossref
- Simulation for Reduction of Transverse Acetabular Fractures in Sawbones Models
- Seongeun Byun, Cyril Mauffrey, Jehyun Yoo, Changwon Park, Jihyo Hwang
- J Korean Fract Soc 2019;32(4):196-203. Published online October 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.4.196
-
Abstract
PDF
- PURPOSE
The transversely oriented fracture lines are very difficult to reduce during operations, even after clear exposure of the fracture site, in acetabular fractures. The purpose of this study is to verify the quality of reduction between the different subtypes (transtectal, juxtatectal, and infratectal) of transverse fractures. This study also determined the proper type of clamps to use and the proper zone for achieving accurate reductions in Sawbones models.
MATERIALS AND METHODS
Six fractures in 3 different subtypes of transverse fractures were artificially created. Ten different reduction clamps were applied for reduction of the fractures. Twelve holes around the fracture were drilled for the maintenance of the clamps. The fracture displacements were measured at the extra-articular area and the intra-articular joint portion. The pictures of the intra-articular fracture displacements were taken by a camera and these were uploaded and analyzed by the TraumaCad® computer program (Brainlab).
RESULTS
The reduction quality was poor in order of transtectal, juxtatectal and infratectal. The intraarticular opening was more prominent in the transtectal subtype. The safe zone, when giving consideration of the neurovascular bundles, was a quadrilateral surface of the ilium. Drill holes are useful for maintenance of the reduction clamps. Reduction clamps with points (Weber clamp) were the best for maintenance and accurate reduction. Regarding the concerns of placement of clamps, the middle to posterior combination was the best. The upper hole among the posterior holes in the ilium was the most likely to well reduce the intra-articular opening.
CONCLUSION
Transtectal was the more complicated subtype in the aspect of reduction quality. The Weber type reduction clamp was the best for reduction by centrally located holes in the quadrilateral surface and posteriorly located iliac holes in transverse acetabular fractures. The upper hole, among the posterior holes in the ilium, was the best for reduction of the fracture displacements in the intraarticular portion of acetabulum. -
Citations
Citations to this article as recorded by- Surgical outcomes of transverse acetabular fractures and risk factors for poor outcomes
Jae Hoon Jang, Nam Hoon Moon, Seung Joon Rhee, Seok Jin Jung, Tae Young Ahn
BMC Musculoskeletal Disorders.2021;[Epub] CrossRef
- Surgical outcomes of transverse acetabular fractures and risk factors for poor outcomes
- 2,174 View
- 16 Download
- 1 Crossref
- Percutaneous Iliosacral Screw Fixation with Cement Augmentation in Osteoporotic Sacral Fracture
- Cheol hwan Kim, Young yool Chung, Seung woo Shim, Sung nyun Baek, Choong young Kim
- J Korean Fract Soc 2019;32(4):165-172. Published online October 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.4.165
-
Abstract
PDF
- PURPOSE
The prevalence of osteoporotic sacral fractures is increasing. Traditionally, conservative treatment is the 1st option, but it can increase the risk of comorbidity in the elderly. To reduce the complications and allow early mobility, iliosacral screw fixation with cement augmentation will be one of the treatment options for patients with osteoporotic sacral fractures.
MATERIALS AND METHODS
This study reviewed 25 patients (30 cases) who had undergone percutaneous iliosacral screw fixation with cement augmentation for osteoporotic sacral fractures from July 2012 to December 2018 with a minimum follow up of six months. The clinical outcomes were assessed using the measures of pain (visual analogue scale [VAS] score), hospital stay and the date when weight-bearing started. All patients were evaluated radiologically for pull-out of screw, bone-union, and cement-leakage.
RESULTS
Bone union was achieved in 30 cases (100%). The mean duration of the hospital stay was 24 days (4–66 days); weight-bearing was performed on an average nine days after surgery. The VAS scores immediately (3.16) and three months after surgery (2.63) were lower than that of the preoperative VAS score (8.3) (p<0.05). No cases of cement-leakage or neurologic symptoms were encountered. Two patients (6.7%) experienced a pulling-out of the screw, but bone-union was accomplished without any additional procedures.
CONCLUSION
Percutaneous iliosacral fixation with cement augmentation will be an appropriate and safe surgical option for osteoporotic sacral fractures in the elderly in terms of early weight-bearing, pain reduction, and bone-union. -
Citations
Citations to this article as recorded by- Role of Augmentation in the Fixation of Osteoporotic Fractures
Chinmoy Das, Partha Pratim Das
Indian Journal of Orthopaedics.2025; 59(3): 294. CrossRef
- Role of Augmentation in the Fixation of Osteoporotic Fractures
- 1,843 View
- 4 Download
- 1 Crossref
- Safety and Effectiveness of the Anchor Augmentation with Bone Cement on Osteoporotic Femoral Fracture: A Systematic Reviews
- So Young Kim
- J Korean Fract Soc 2019;32(2):89-96. Published online April 30, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.2.89
-
Abstract
PDF
- PURPOSE
This paper reviewed the safety and effectiveness of anchor augmentation with bone cement in osteoporotic femoral fractures.
MATERIALS AND METHODS
A systematic review was conducted by searching multiple databases including five Korean databases, Ovid-MEDLINE, Ovid-EMBASE, and Cochrane Library. Safety was assessed through the incidence of complication. The effectiveness was assessed through the failure rate of anchor fixation, improvement of function and radiological assessment (sliding distance of lag screw and cutout). The safety and effectiveness of anchor augmentation with bone cement were assessed by reviewing all articles reporting on the treatment. Two researchers carried out independently each stage from the literature search to data extraction. The tools of Scottish Intercollegiate Guidelines Networks were used to assess the quality of studies.
RESULTS
Six studies were considered eligible. The safety results revealed a small amount of cement leakage (1 case), but no other severe complications were encountered. Regarding the effectiveness, the failure rate of anchor fixation was 16.7% and the Harris's hip score showed no significant improvement. The sliding distance of the anchor was similar in the cement augmentation group and non-cement group but there was no cutout.
CONCLUSION
The results of the assessment suggest that the safety is acceptable, but further research will be needed to verify the effectiveness of the treatment.
- 1,204 View
- 5 Download
Case Report
- Cortical Perforation Misidentified with Medial Condylar Fracture of Femur in Total Knee Arthroplasty: Case Report
- Seung Suk Seo, Sang Won Moon
- J Korean Fract Soc 2019;32(1):52-55. Published online January 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.1.52
-
Abstract
PDF
- Intraoperative fracture in total knee arthroplasty (TKA) is a rare complication. However, when it happens, additional surgery to fix the fracture site is needed. Therefore, it is important to diagnose intraoperative fractures in TKA exactly. The authors experienced two cases of cortical perforation of medial femoral condyle misidentified as the fracture in TKA. Cortical perforation could be misdiagnosed as the fracture, which could lead to unnecessary surgery. This is the first report about cortical perforation in TKA. We report two cases of intraoperative cortical perforations and describe the radiological characteristics.
- 1,560 View
- 3 Download
Original Article
- Risk Factors for Knee Stiffness in Distal Femoral Fractures
- Dong Wook Son, Hyoung Soo Kim, Woo Young Choi
- J Korean Fract Soc 2018;31(4):123-131. Published online October 31, 2018
- DOI: https://doi.org/10.12671/jkfs.2018.31.4.123
-
Abstract
PDF
- PURPOSE
The aims of this study were to evaluate risk factors for knee stiffness after the fixation of distal femoral fractures, and to analyze the clinical and radiologic outcomes.
MATERIALS AND METHODS
This is a retrospective case control study of 104 consecutive patients who have a distal femoral fracture and were treated with a submuscular locking plate. The case group comprised of patients with 12-month postoperative range of motion (ROM) ≤90° or a history of manipulation under anesthesia. The case group was compared with the control group of patients with a 12-month postoperative ROM >90°. The possible risk factors were evaluated by univariate and logistic regression analysis. The postoperative ROM and Knee Society clinical rating system was evaluated for the clinical assessment and the distal femoral angle on a whole-extremity scanogram was measured for radiologic assessments.
RESULTS
Fifty-four patients were included in the study (14 in the case group, 40 in the control group). Univariate analysis showed that comminuted fracture, intra-articular fracture, open fracture, temporary external fixation, severe osteoarthritis, and prolonged immobilization placed patients at an increased risk for knee stiffness. On the other hand, multivariate logistic regression showed that an extensor mechanism injury was the only significant predictor (p=0.001; odds ratio, 42.0; 95% confidence interval, 5.0–350.7). The ROM and Knee Society score were significantly lower in the case group; however, the coronal alignment was similar in the case and control group.
CONCLUSION
Various factors that delay postoperative knee motion place patients at increased risk of knee stiffness. Understanding these risk factors may help surgeons prevent postoperative knee stiffness after distal femoral fractures. In particular, extensor mechanism injury, such as patella fracture or open quadriceps injury, was found to be an independent predictable factor associated with knee stiffness. -
Citations
Citations to this article as recorded by- Post operative knee stiffness after surgical fixation of knee osseous injuries
Oitangor Arthur, Sekamatte Yasin, Mulepo Phillip
Adesh University Journal of Medical Sciences & Research.2026; 8: 56. CrossRef - The outcomes of patients with segmental long bone fractures treated with SIGN nail at Addis Ababa Burn, Emergency and Trauma Hospital
Cheru B. Tesso, Lelisa Merga, Samuel Kebede
OTA International.2026;[Epub] CrossRef - A Comprehensive Approach to Stiffness in Total Knee Arthroplasty
Brian P. Chalmers, Linda I. Suleiman, Peter K. Sculco, Matthew P. Abdel
The Journal of Arthroplasty.2025; 40(9): S59. CrossRef - Staged Management for Distal Femur Fractures: Impacts on Reoperation, Stiffness, and Overall Outcomes
Matthew T. Yeager, Robert W. Rutz, Alex Roszman, Gerald McGwin, James E. Darnley, Joseph P. Johnson, Clay A. Spitler
Journal of Orthopaedic Trauma.2024; 38(11): 577. CrossRef - Outcome of the Masquelet Technique for Complex Bilateral Distal Femoral Bone Defects
Ziad A Aljaafri, Abdullah Alzahrani, Ali Alshehri, Ahmed AlHussain, Faisal Alzahrani, Khalid Alsheikh
Cureus.2023;[Epub] CrossRef - Efficacy of non-operative treatment of patients with knee arthrofibrosis using high-intensity home mechanical therapy: a retrospective review of 11,000+ patients
Shaun K. Stinton, Samantha J. Beckley, Thomas P. Branch
Journal of Orthopaedic Surgery and Research.2022;[Epub] CrossRef - Distal Femoral Replacement and Extensor Mechanism Repair Reinforced With Synthetic Mesh for Distal Femur Fracture With Patellar Ligament Avulsion
Charles Powell, Kristopher Sanders, Neal Huang, Luis Felipe Colón, Colton Norton
Arthroplasty Today.2022; 16: 31. CrossRef - The fragility of statistical significance in distal femur fractures: systematic review of randomized controlled trials
Michael Megafu, Hassan Mian, Emmanuel Megafu, Sulabh Singhal, Alexander Lee, Richawna Cassie, Paul Tornetta, Robert Parisien
European Journal of Orthopaedic Surgery & Traumatology.2022; 33(6): 2411. CrossRef - Association Between Femoral “Spike” Size After Intramedullary Nailing and Subsequent Knee Motion Surgery
Michael G. Schloss, Nathan N. O'Hara, Syed M. R. Zaidi, Zachary D. Hannan, Dimitrius Marinos, Jared Atchison, Alexandra Mulliken, Jason W. Nascone, Robert V. O'Toole
Journal of Orthopaedic Trauma.2021; 35(2): 100. CrossRef - Distal Femur Replacement Versus Surgical Fixation for the Treatment of Geriatric Distal Femur Fractures: A Systematic Review
Brett P. Salazar, Aaron R. Babian, Malcolm R. DeBaun, Michael F. Githens, Gustavo A. Chavez, L. Henry Goodnough, Michael J. Gardner, Julius A. Bishop
Journal of Orthopaedic Trauma.2021; 35(1): 2. CrossRef
- Post operative knee stiffness after surgical fixation of knee osseous injuries
- 1,168 View
- 20 Download
- 10 Crossref
Review Articles
- Hand Fractures
- Seokwon Yang, Jong Pil Kim
- J Korean Fract Soc 2018;31(2):61-70. Published online April 30, 2018
- DOI: https://doi.org/10.12671/jkfs.2018.31.2.61
-
Abstract
PDF
- Hand fractures are the second most common fracture in the upper extremities after the distal radius, and patients with these injuries may be experienced in hand surgery clinics. On the other hand, during the treatment of hand fractures, complications can occur due to complex functions of the hand and small-sized injuries to the bone and soft tissues. This review focused on the principles of management of these fractures, including injury mechanism, evaluations and recent treatment options. Minimally invasive surgery in various types of hand fractures, including the phalanx and metacarpal bone, is preferred because early mobilization after surgery has been emphasized to reduce complications, such as stiffness.
-
Citations
Citations to this article as recorded by- A novel finger brace for preventing finger stiffness after trauma or surgery: a preliminary report with a case series
Dae-Geun Kim, Hyo Jun Park
Archives of Hand and Microsurgery.2023; 28(4): 239. CrossRef
- A novel finger brace for preventing finger stiffness after trauma or surgery: a preliminary report with a case series
- 1,030 View
- 4 Download
- 1 Crossref
- Treatment Options for the Nonunions with Critical Sized Bone Loss
- Jin Kak Kim, Soo Hyun Kim, Jae Woo Cho, Jong Keon Oh
- J Korean Fract Soc 2017;30(2):89-101. Published online April 30, 2017
- DOI: https://doi.org/10.12671/jkfs.2017.30.2.89
-
Abstract
PDF
- The management of nonunion with severe bone loss is a challenging task to both surgeons and patients. It often requires prolonged and potentially painful treatments. Moreover, it also represents serious socioeconomic issues for patients. Inadequate fracture stability, disrupted biology, such as blood supply and soft tissue, as well as severe bone loss or presence of infection are possible reasons for nonunion. Several different treatment modalities are available, including nail dynamization, plate osteosynthesis, exchange nailing, and adjuvant alternatives, such as electrical or ultrasound stimulation. Autogenous bone graft remains the standard method to reconstruct small defects. Distraction osteogenesis and induced membrane techniques are contemporary strategies of choice for the reconstruction of larger bony defects. Herein, we attempt to describe the key techniques that may be employed in treating nonunion with severe bone loss.
-
Citations
Citations to this article as recorded by- Individualized herbal prescriptions for delayed union: A case series
Jiyoon Won, Youngjin Choi, Lyang Sook Yoon, Jun-Hwan Lee, Keunsun Choi, Hyangsook Lee
EXPLORE.2023; 19(2): 260. CrossRef
- Individualized herbal prescriptions for delayed union: A case series
- 1,107 View
- 6 Download
- 1 Crossref
 First
First Prev
Prev

