 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 30(1); 2017 > Article
-
Case Report
- Decompressive Sacral Foraminotomy for Nerve Root Injury during Conservative Treatment of Sacral Fracture: A Case Report
- Jung-Gil Lee, M.D., Jae-Hyuk Shin, M.D., Kwon Kim, M.D., Sang-Min Choi, M.D., Moon Soo Park, M.D., Ho-Guen Chang, M.D.
-
Journal of the Korean Fracture Society 2017;30(1):24-28.
DOI: https://doi.org/10.12671/jkfs.2017.30.1.24
Published online: January 20, 2017
Department of Orthopedic Surgery, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea.
*Department of Orthopaedic Surgery, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- Correspondence to: Jae-Hyuk Shin, M.D. Department of Orthopedic Surgery, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, 150 Seongan-ro, Gangdong-gu, Seoul 05355, Korea. Tel: +82-2-2224-2230, Fax: +82-2-2224-2231, jshin2100@gmail.com
• Received: July 26, 2016 • Revised: September 23, 2016 • Accepted: October 26, 2016
Copyright © 2017 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,007 Views
- 9 Download
Abstract
- A 35-year-old woman visited the emergency department for a pedestrian traffic accident. Severe tenderness was noted at the posterior sacrum area, without open wound or initial neurologic deficit. Fracture of the left sacral ala extended to the S1 foramen, anterior acetabulum, and pubic ramus. Two weeks after the injury, she presented aggravating radiculopathy with the weakness of the left great toe plantar flexion. The S1 nerve root was compressed by the fracture fragments in the left S1 foramen. Decompressive S1 foraminotomy was performed. The postoperative follow-up computed tomography scan showed successful decompression of the encroachment, and the patient recovered well from the radiculopathy with motor weakness. She was able to resume her daily routine activity. We suggest that early decompressive sacral foraminotomy could be a useful additional procedure in selective sacral zone II fractures that are accompanied by radiculopathy with a motor deficit.
- 1. Denis F, Davis S, Comfort T. Sacral fractures: an important problem Retrospective analysis of 236 cases. Clin Orthop Relat Res, 1988;227:67-81.
- 2. Young JW, Burgess AR, Brumback RJ, Poka A. Lateral compression fractures of the pelvis: the importance of plain radiographs in the diagnosis and surgical management. Skeletal Radiol, 1986;15:103-109.ArticlePDF
- 3. Kim MY, Reidy DP, Nolan PC, Finkelstein JA. Transverse sacral fractures: case series and literature review. Can J Surg, 2001;44:359-363.
- 4. Hersche O, Isler B, Aebi M. Follow-up and prognosis of neurologic sequelae of pelvic ring fractures with involvement of the sacrum and/or the iliosacral joint. Unfallchirurg, 1993;96:311-318.
- 5. Roy-Camille R, Saillant G, Gagna G, Mazel C. Transverse fracture of the upper sacrum. Suicidal jumpers fracture. Spine (Phila Pa 1976), 1985;10:838-845.
- 6. Schnaid E, Eisenstein SM, Drummond-Webb J. Delayed posttraumatic cauda equina compression syndrome. J Trauma, 1985;25:1099-1101.
- 7. Schmidek HH, Smith DA, Kristiansen TK. Sacral fractures. Neurosurgery, 1984;15:735-746.ArticlePDF
- 8. Fountain SS, Hamilton RD, Jameson RM. Transverse fractures of the sacrum A report of six cases. J Bone Joint Surg Am, 1977;59:486-489.Article
- 9. Phelan ST, Jones DA, Bishay M. Conservative management of transverse fractures of the sacrum with neurological features A report of four cases. J Bone Joint Surg Br, 1991;73:969-971.ArticlePDF
- 10. Zelle BA, Gruen GS, Hunt T, Speth SR. Sacral fractures with neurological injury: is early decompression beneficial? Int Orthop, 2004;28:244-251.ArticlePDF
REFERENCES
Fig. 1
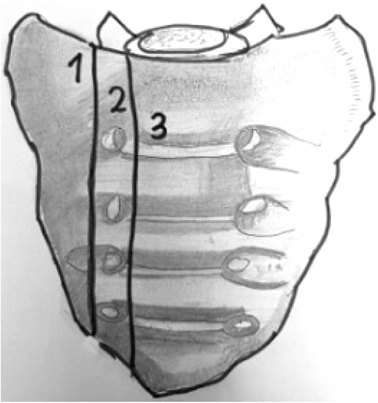
This schematic drawing of the sacrum shows a classification of sacral fractures according to Denis et al.1) 1: Zone I-ala region; 2: Zone II-foramina region; 3: Zone III-central sacral canal region.
Fig. 2

A, B) Anteroposterior pelvic radiograph and 3-dimensional computed tomography (CT) shows a fracture at the left sacral ala, sacral foramina (white arrows) anterior acetabulum, and pubic ramus. Coronal (C), and axial (D) view of the CT image show S1 left foraminal encroachment by the fracture fragment (arrows).
Fig. 3
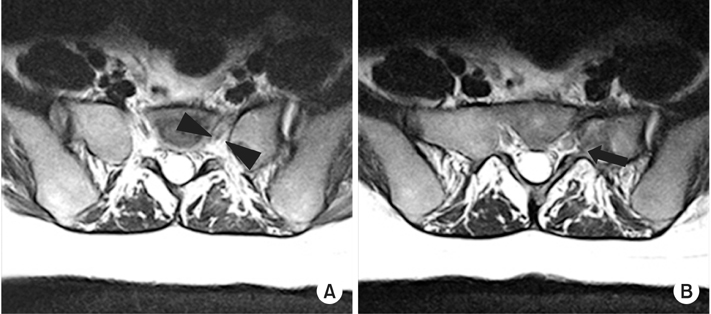
(A, B) T2-weighted axial images show an enlarged S1 nerve root with increased signal intensity, suggesting nerve root injury (arrow heads and arrow).
Fig. 4
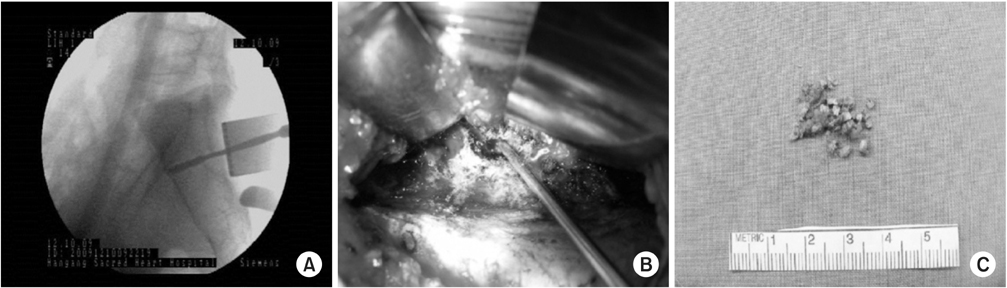
(A-C) Decompressive S1 foraminotomy was performed. The S1 foramen was explored under an image intensifier with a penfield probe. We used a Kerrison punch (2 mm, 3 mm) in the foraminotomy, under a loupe magnification. The foraminal encroachment and nerve root release were identified with a nerve hook probe.
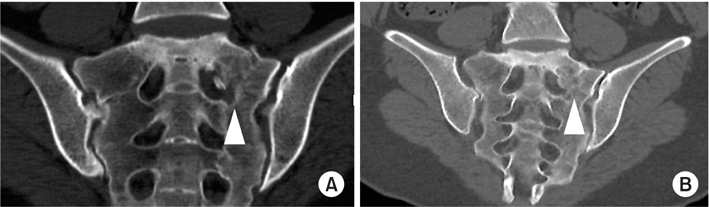
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteDecompressive Sacral Foraminotomy for Nerve Root Injury during Conservative Treatment of Sacral Fracture: A Case Report


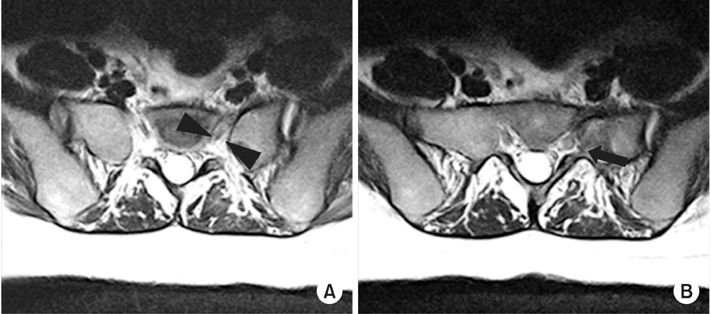
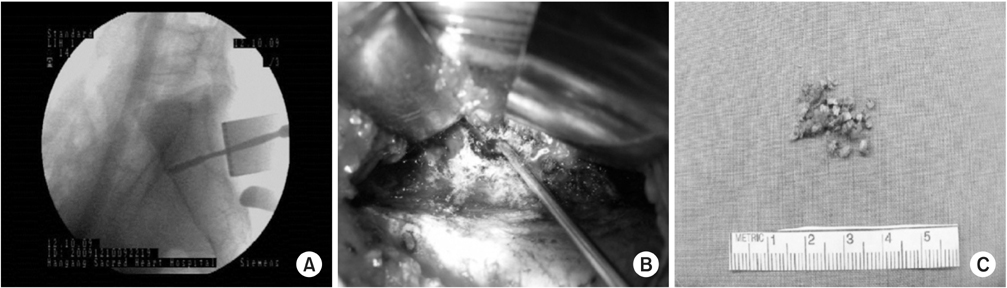
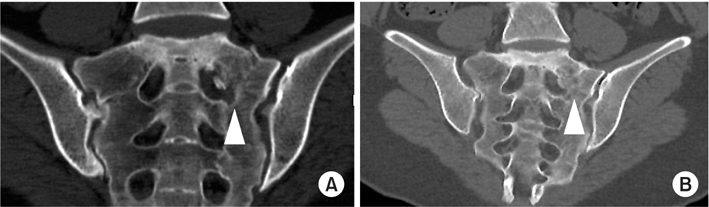
Fig. 1
This schematic drawing of the sacrum shows a classification of sacral fractures according to Denis et al.1) 1: Zone I-ala region; 2: Zone II-foramina region; 3: Zone III-central sacral canal region.
Fig. 2
A, B) Anteroposterior pelvic radiograph and 3-dimensional computed tomography (CT) shows a fracture at the left sacral ala, sacral foramina (white arrows) anterior acetabulum, and pubic ramus. Coronal (C), and axial (D) view of the CT image show S1 left foraminal encroachment by the fracture fragment (arrows).
Fig. 3
(A, B) T2-weighted axial images show an enlarged S1 nerve root with increased signal intensity, suggesting nerve root injury (arrow heads and arrow).
Fig. 4
(A-C) Decompressive S1 foraminotomy was performed. The S1 foramen was explored under an image intensifier with a penfield probe. We used a Kerrison punch (2 mm, 3 mm) in the foraminotomy, under a loupe magnification. The foraminal encroachment and nerve root release were identified with a nerve hook probe.
Fig. 5
(A) Postoperative computed tomography images demonstrate decompression by S1 foraminotomy (arrow head). (B) Postoperative 4 months follow-up image shows union and remodeling processes of the fracture around the S1 neural foramen.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Decompressive Sacral Foraminotomy for Nerve Root Injury during Conservative Treatment of Sacral Fracture: A Case Report

