 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Most cited articles
- Page Path
- HOME > Browse articles > Most cited articles
Most-cited are based on citations from 2024 ~ 2026.
Review Articles
- Current concepts and applications of bone graft substitutes in orthopedic surgery
- Jae Ho Cho, Hyung Keun Song
- J Musculoskelet Trauma 2025;38(4):169-177. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00248

-
 Abstract
Abstract
 PDF
PDF - Bone defects, which often arise from high-energy injuries, infections, tumor resections, or nonunions, represent a persistent challenge in orthopedic trauma surgery. Autologous bone grafting remains the gold standard due to its unique combination of osteogenic, osteoinductive, and osteoconductive properties. However, issues such as donor site morbidity, limited graft volume, and increased surgical time have driven the development of bone graft substitutes. These substitutes vary widely in origin, composition, biological activity, and mechanical characteristics, encompassing allografts, xenografts, synthetic materials, and biologically enhanced constructs. This review outlines the fundamental biological principles underlying bone regeneration—including osteogenesis, osteoinduction, and osteoconduction—and addresses additional key factors such as biocompatibility, biodegradability, and mechanical strength. Current bone graft materials are classified by biological origin and functional characteristics, with an emphasis on their use in trauma surgery. Particular attention is given to the clinical applications, indications, and limitations of allograft-based solutions (such as structural allografts and demineralized bone matrix), synthetic ceramics (including calcium phosphate and bioactive glass), and biologically enhanced options, such as recombinant growth factors and stem cell therapies. In trauma settings, graft selection must be tailored to the characteristics of the defect, mechanical demands, the biological environment, and patient-specific factors. Integration with surgical technique and fixation is crucial for optimizing outcomes. Although modern substitutes show promise, none fully replicate the complex biology of autografts. Looking ahead, emerging technologies such as 3D printing, nanotechnology, and smart biomaterials offer exciting possibilities but face translational challenges. This review aims to provide practicing orthopedic surgeons with a concise, evidence-based overview of bone substitute options and their roles in trauma care. By applying core biological principles and clinical judgment, surgeons can better navigate the expanding array of graft materials to improve outcomes for patients with complex skeletal defects.
-
Citations
Citations to this article as recorded by
- Safety and Efficacy of rhBMP-2 for Treating Acute Traumatic Fractures of the Upper and Lower Extremities: A Multicenter Prospective Study
Seungyeob Sakong, Seokjun Hong, Wonseok Choi, Seonghyun Kang, Jae-Woo Cho, Whee Sung Son, Jeong-Seok Choi, Chang-Jin Yon, Won-Tae Cho, Jong-Keon Oh
Journal of Clinical Medicine.2026; 15(3): 1176. CrossRef - Plasma‐Assisted KR‐12 Conjugated PLGA Nanofibers With Dual Osteogenic and Biofilm‐Inhibitory Activity
Günnur Pulat, Eda Bilgiç, Buse Sezer
Journal of Biomedical Materials Research Part A.2026;[Epub] CrossRef - Histological Study of a Novel 3D-Printed Hydroxyapatite/PLGA Bone Graft in the Regeneration of Critical-Sized Long Bone Defects
Marijana Popović Bajić, Smiljana Paraš, Milutin Mićić, Božana Petrović, Vladimir Biočanin, Slavoljub Živković, Marija Živković, Damjana Drobne, Vukoman Jokanović
Bioengineering.2026; 13(4): 394. CrossRef - The Use of Osteo-Inductive 3D-Printed Scaffolds Covered with a Pleiotrophin Peptide for Bone Defects: An In Vivo Experimental Study
Dimitrios Tsoumanis, Emilios E. Pakos, Ioannis Gkiatas, Ioannis Gelalis, Anna Batistatou, Evangelia Lampri, Despoina Deligianni, Evangelia Papadimitriou, Dimitrios Fotiadis, Anastasios Korompilias
Bioengineering.2026; 13(6): 608. CrossRef - Research advances in bioactive bone graft materials and bone marrow enrichment techniques for bone defect treatment
Zhezheng Shen, Xueyuan Li, Zijun Ye, Yuhao Zhou, Di Tu, Zongying Tian, Wei Qian
Cell Transplantation.2026;[Epub] CrossRef - A Novel Technique of Overlapping Distal Stump Within Femoral Allograft-Prosthesis Composite for Extensive Humeral Bone Loss in Revision Total Elbow Arthroplasty
Chul-Hyun Cho, Bum-Soon Park, Eun-Seok Son, Du-Han Kim
Techniques in Orthopaedics.2026;[Epub] CrossRef - Enhancing Bone Healing with a Priming Stimulus
Michael Tanzer, Misghana Kassa, Nitin Chandra Teja Dadi, Tarek Klaylat, Rahul Gawri, Paul Martineau, Adam Hart
Life.2026; 16(7): 1111. CrossRef
- Safety and Efficacy of rhBMP-2 for Treating Acute Traumatic Fractures of the Upper and Lower Extremities: A Multicenter Prospective Study
- 10,964 View
- 287 Download
- 7 Crossref

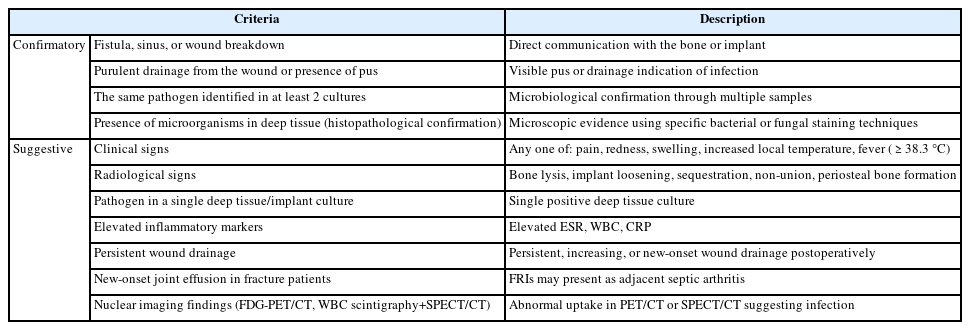
- Fracture-related infections: a comprehensive review of diagnosis and prevention
- HoeJeong Chung, Hoon-Sang Sohn
- J Musculoskelet Trauma 2025;38(2):86-95. Published online April 25, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00164
-
Abstract
PDF
- Fracture-related infections are challenging complications in orthopedic trauma that often require prolonged treatment and impose a significant healthcare burden. Accurate diagnosis and effective prevention strategies are essential for minimizing their occurrence. A recent international consensus has established standardized diagnostic criteria based on clinical, microbiological, radiological, and histopathological findings. Prevention is the top priority and involves a thorough preoperative risk assessment, along with glycemic control, nutritional optimization, and management of comorbidities, as well as intraoperative and postoperative measures such as appropriate antibiotic prophylaxis, surgical site antisepsis, and meticulous wound care. A multidisciplinary approach involving orthopedic surgeons, infectious disease specialists, and microbiologists is crucial for successfully reducing the burden of fracture-related infections.
-
Citations
Citations to this article as recorded by- Incidence and risk factors of postoperative infection after wrist arthroscopy: an 11-year nationwide population-based cohort study in South Korea
Jisu Park, Hyunsun Lim, SeongJu Choi, Jin Rok Oh, Jun-Ku Lee
Orthopaedics & Traumatology: Surgery & Research.2026; : 104771. CrossRef - Personalized Approaches to Diagnostic and Therapeutic Strategies in Periprosthetic Fracture-Related Infections (PFRIs): Case Series and Literature Review
Marianna Faggiani, Marco Zugnoni, Matteo Olivero, Salvatore Risitano, Giuseppe Malizia, Silvia Scabini, Marcello Capella, Stefano Artiaco, Simone Sanfilippo, Alessandro Massè
Journal of Personalized Medicine.2025; 15(12): 576. CrossRef - Pathogen-Specific Risk for Iterative Surgical Debridement in Orthopedic Infections: A Prospective Multicohort Analysis
Flamur Zendeli, Anna Jędrusik, Raymond O. Schaefer, David Albrecht, Michael Betz, Felix W. A. Waibel, Tanja Gröber, Nathalie Kühne, Sören Könneker, İlker Uçkay
Journal of Clinical Medicine.2025; 14(24): 8750. CrossRef
- Incidence and risk factors of postoperative infection after wrist arthroscopy: an 11-year nationwide population-based cohort study in South Korea
- 10,439 View
- 482 Download
- 3 Crossref
- Atypical femoral fractures: an update
- Won-Tae Cho, Jeong-Hyun Koh, Seungyeob Sakong, Jung-Taek Kim
- J Musculoskelet Trauma 2025;38(2):41-52. Published online March 28, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00031
-
Abstract
PDF
- This narrative review provides an up-to-date overview of atypical femoral fractures (AFFs), emphasizing diagnostic criteria, epidemiology, pathophysiology, risk factors, and evaluation with screening strategies. AFFs are rare but significant complications associated with prolonged bisphosphonate (BP) therapy for osteoporosis. Although the pathogenesis of AFFs has not been fully elucidated, its primary mechanism is thought to involve impaired bone remodeling, leading to unhealed microfractures that progress to stress fractures under repetitive loading. AFFs can occur in various regions of the femur, influenced by femoral geometry and the lower limb axis. Other risk factors include prolonged steroid use, arthroplasty, genetic predispositions, and metabolic bone disorders. The diagnosis of AFFs is based on criteria established by the American Society for Bone and Mineral Research. Key radiographic features include lateral cortical transverse fracture lines and localized cortical thickening, typically with minimal or no comminution on the medial cortex. Dual-energy X-ray absorptiometry for screening tests and magnetic resonance imaging as an advanced imaging modality enable the early detection of incomplete fractures. This multi-modal approach facilitates the prompt identification of prodromal cortical changes, reducing the risk of complete fractures in high-risk populations, particularly patients undergoing prolonged BP therapy. Level of Evidence: V
-
Citations
Citations to this article as recorded by- Clinical Images: Bisphosphonate‐associated atypical femoral fracture with contralateral cortical beaking
Andreina Martinez Paulino, Valentin Marian
ACR Open Rheumatology.2026;[Epub] CrossRef - Atypical femoral fracture: The periprosthetic variant about two cases without bisphosphonate use
Guillaume Auberger, Thomas Aubert, Younes Kerroumi, Philippe Leclerc, Simon Marmor
SICOT-J.2026; 12: 41. CrossRef - Atypical Femur Fractures Without Bisphosphonate Exposure (AFFwB): A Retrospective Report of 21 Cases
Lorenzo Lucchetta, Carmelinda Ruggiero, Samuele Berardi, Alice Franceschi, Michele Bisaccia, Giuseppe Rinonapoli
Journal of Clinical Medicine.2025; 15(1): 25. CrossRef
- Clinical Images: Bisphosphonate‐associated atypical femoral fracture with contralateral cortical beaking
- 65,535 View
- 704 Download
- 3 Crossref
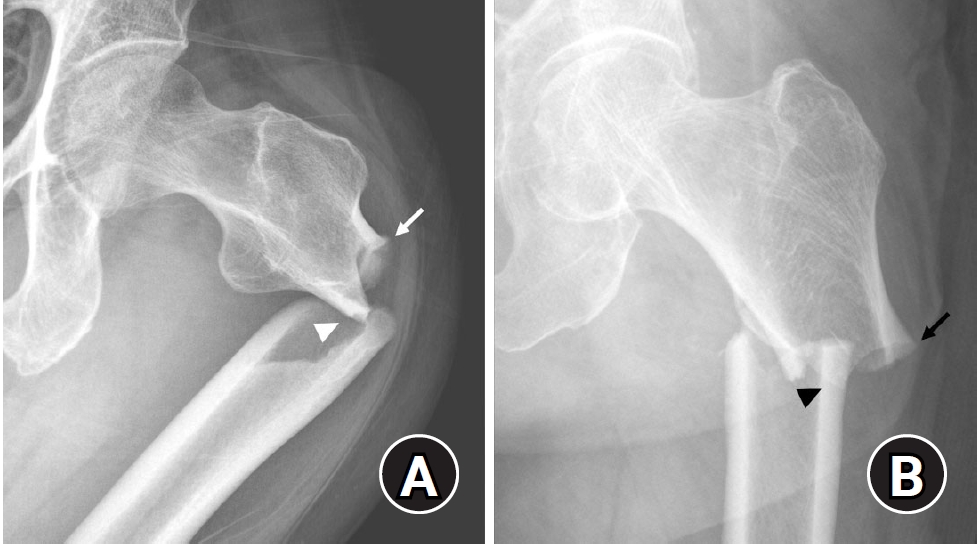
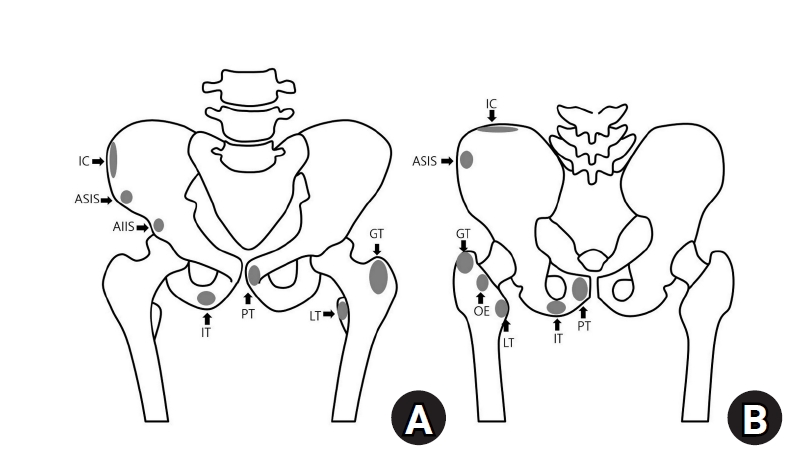
- Avulsion fractures around the hip joint and pelvis
- Won-Sik Choy, Yonghan Cha, Jung-Taek Kim, Jun-Il Yoo, Jin-Woo Kim
- J Musculoskelet Trauma 2025;38(2):53-62. Published online March 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00010
-
Abstract
PDF
- Avulsion fractures occur when tendons or ligaments are subjected to forces greater than they can withstand at the apophysis or enthesis, regardless of fusion status. The pelvis and hip joint are vulnerable to these injuries due to the diverse muscular structures in these structures, which serve as origins for multiple muscles leading to the lower extremities. Pelvic avulsion fractures commonly affect young athletes, but can also occur in adults. The diagnosis typically involves assessing trauma history, a clinical examination, and radiographic imaging. If the diagnosis is unclear, additional tests such as computed tomography and magnetic resonance imaging may assist in the diagnosis and provide useful information for treatment decisions. While most avulsion fractures respond well to conservative treatment, surgical intervention may be preferred in severe displacements, cases of significant retraction in active athletes, or when a faster recovery is necessary. Chronic or neglected injuries may lead to excessive osseous formation around the pelvis, causing impingement syndromes. Recognizing characteristic radiological findings based on pelvic anatomy helps to make an accurate diagnosis, as chronic injuries can mimic tumors or infectious conditions, necessitating a careful differential diagnosis.
-
Citations
Citations to this article as recorded by- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
Dawid Bartosik, Bartlomiej Cwikla, Anna Kowalczyk, Michalina Loson-Kawalec, Anna Palka-Szymaniec, Bartosz Starzynski, Alina Keska, Jakub Szkuta, Klaudia Wojcik
Cureus.2026;[Epub] CrossRef - Outcomes of Conservative Versus Surgical Treatment of Adolescent Pelvic and Hip Avulsion Fractures: A Systematic Review and Meta-Analysis
Lindsey L. Molina, Andrew M. Block, Sasha Carsen, Allison E. Crepeau, Tyler J. Stavinoha, Michael M. Chau, Jeffrey J. Nepple
Journal of Pediatric Orthopaedics.2026;[Epub] CrossRef - Diagnostic Accuracy of Ultrasound for Adolescent Pelvic Avulsion Fractures: A Blinded Multirater Study
Meena Meiyyappan, Robert Van Pelt, Kate Lampe, Jane Chung, Matthew Ditzler, Shane Miller, Henry Ellis, Hamza Alizai, Matthew Hammer, Ben Johnson, Charles Wyatt, Jacob Jones
Journal of Clinical Ultrasound.2026;[Epub] CrossRef
- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
- 20,158 View
- 213 Download
- 3 Crossref
Original Articles
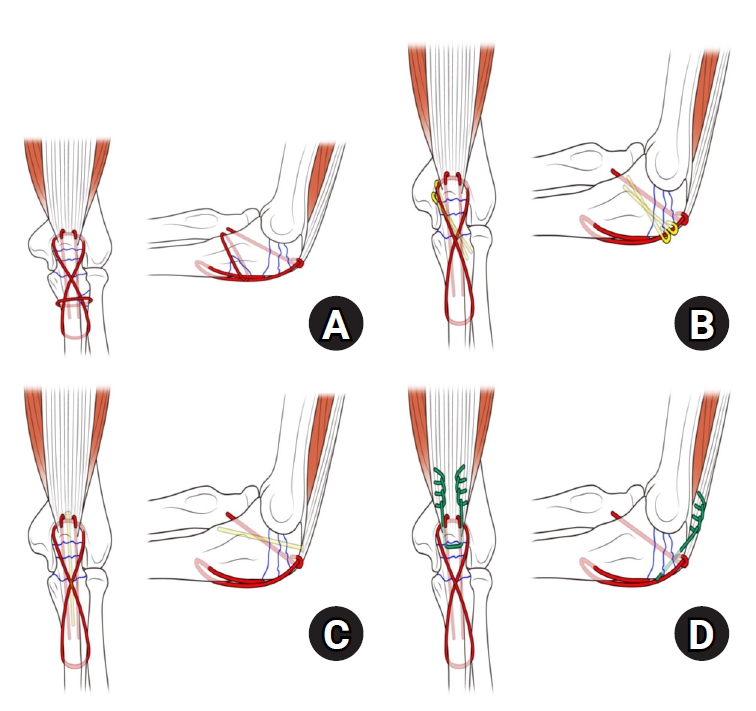
- Comparison of outcomes of reinforced tension band wiring and precontoured plate and screw fixation in the management of Mayo type IIIB olecranon fractures
- Hyun Goo Kang, Tong Joo Lee, Samuel Jaeyoon Won
- J Musculoskelet Trauma 2025;38(2):96-101. Published online February 28, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00059
- Correction in: J Musculoskelet Trauma 2025;38(3):168
-
Abstract
PDF
- Background
Mayo type IIIB olecranon fractures are characterized by significant displacement and comminution, presenting a challenge in selecting the appropriate fixation technique. This study compared the clinical and radiographic outcomes, complications, and reoperation rates of reinforced tension band wiring (TBW) and precontoured plate and screw fixation (PF) in the surgical treatment of Mayo type IIIB olecranon fractures.
Methods
This retrospective review analyzed 24 patients diagnosed with Mayo type IIIB olecranon fractures, who were treated between 2005 and 2023. Of these, 11 patients underwent reinforced TBW, and 13 received precontoured PF. Clinical outcomes were assessed using Disabilities of the Arm, Shoulder, and Hand (DASH) scores and the Mayo Elbow Performance Score (MEPS). Radiographic outcomes focused on fracture union. Operative times, complication rates, and reoperation rates were compared between the groups.
Results
Both the reinforced TBW and PF groups achieved satisfactory clinical outcomes, with no significant between-group differences in DASH and MEPS scores (P>0.05). Radiographic union was achieved in all patients. The reinforced TBW group demonstrated a significantly shorter operative time than the PF group (93.6±7.4 min vs. 132.3±13.7 min; P<0.001). Complication rates were similar between the two groups (reinforced TBW, 38.4%; PF, 36.3%), but hardware-related irritation occurred more frequently in the reinforced TBW group. Reoperations were required in 15.8% of the reinforced TBW group due to hardware irritation, whereas no reoperations were necessary in the PF group.
Conclusions
Reinforced TBW and PF are both effective surgical options for managing Mayo type IIIB olecranon fractures, yielding comparable clinical and radiographic outcomes. While reinforced TBW offers shorter operative times and lower costs, PF is associated with fewer hardware-related complications. Further prospective studies are needed to optimize treatment strategies for these complex fractures. Level of Evidence: Level III. -
Citations
Citations to this article as recorded by- Suture tension band fixation of olecranon fractures: description and early outcomes of a novel technique
Joseph G. Monir, Frank L. Vazquez, Musab Gulzar, Kevin Cuneo, Thomas McQuillan, Michael B. Gottschalk, Eric R. Wagner
JSES Reviews, Reports, and Techniques.2026; 6(2): 100707. CrossRef - Comparative Efficacy and Safety of Tension Band Wiring versus Plate Fixation for Olecranon Fractures: A Meta-Analysis and Trial Sequential Analysis of Randomized Clinical Trials
Malik A. Alshayban, Amr Khaleel Ibraheem, Abdulrahman Ali Aloudah, Turki S. Alqahtani, Mohamed Nabawy Elseaidy, Mohammed Abdelmalek, Mohamed Abdelhady Mourad
JSES Reviews, Reports, and Techniques.2026; : 100817. CrossRef - Are posterior olecranon locking plates a problem for patients after fracture healing because of prominence?
Reva Qiu, Mallika Makkar, Richard Buckley
Injury.2025; 56(11): 112769. CrossRef
- Suture tension band fixation of olecranon fractures: description and early outcomes of a novel technique
- 3,878 View
- 62 Download
- 3 Crossref
- Does the Operator’s Experience Affect the Occurrence of Complications after Distal Radius Fracture Volar Locking Plate Fixation? A Comparative Study of the First Four Years and Thereafter
- Kee-Bum Hong, Chi-Hoon Oh, Chae Kwang Lim, Sungwoo Lee, Soo-Hong Han, Jun-Ku Lee
- J Musculoskelet Trauma 2024;37(4):175-183. Published online October 25, 2024
- DOI: https://doi.org/10.12671/jmt.2024.37.4.175
- Correction in: J Musculoskelet Trauma 2025;38(1):40
-
Abstract
PDF
- Purpose
The management of distal radius fractures (DRFs) has evolved with the introduction of volar locking plate (VLP) fixation, offering stable fixation and better outcomes. Nevertheless, the impact of the surgeon’s experience on the complication rates in VLP fixation remains to be determined, particularly for less-experienced surgeons. This study compared the complication rates during the initial four years and subsequent two years of a hand surgeon’s practice of VLP fixation for DRFs.
Materials and Methods
The data between March 2016 and December 2022 were analyzed retrospectively under the Institutional Review Board approval. A single surgeon performed all VLP fixation surgeries after finishing regular hand surgery training, with the first four years representing the less experienced phase (Group 1) and the following two years indicating the experienced phase (Group 2). The patients’ characteristics, operation-related factors, and postoperative complications, including tendon injuries, nerve-related complications, fixation and instrument-related issues, osteosynthesis-related problems, and infections, were compared. In addition, the authors compared the data with a large multicenter study conducted by experienced hand surgeons.
Results
Three hundred and nineteen patients (321 wrists) were included. The mean age was 63.3 years, and 26.3% were male and 73.7% were female. The operation time was 53.7±14.5 minutes and 74.4±26.5 minutes in groups 1 and 2, respectively, which was statistically significantly shorter (p<0.001). The complication rates between the two groups were similar, except for the higher implant removal rates in Group 1. A comparison with a previous multicenter study revealed higher reduction losses and carpal tunnel syndrome in this study, but the overall complication rate was low.
Conclusion
In DRF management, when the operating surgeon has completed an accredited training course, VLP fixation is a good treatment method that can be performed effectively even by less experienced surgeons with low complication rates. -
Citations
Citations to this article as recorded by- Epidemiological changes and surgical trends of distal radius fractures in adults over 50 years during the COVID-19 pandemic in Korea: a nationwide repeated cross-sectional study
Han-Kook Yoon, So Ra Yoon, Kee-Bum Hong, Youngsu Jung, SeongJu Choi, Jun-Ku Lee
Journal of Musculoskeletal Trauma.2026; 39(1): 12. CrossRef - Author correction: “Does the operator's experience affect the occurrence of complications after distal radius fracture volar locking plate fixation? A comparative study of the first four years and thereafter”
Kee-Bum Hong, Chi-Hoon Oh, Chae Kwang Lim, Sungwoo Lee, Soo-Hong Han, Jun-Ku Lee
Journal of Musculoskeletal Trauma.2025; 38(1): 40. CrossRef - Characteristics of patients with distal radius fracture requiring arthroscopic foveal repair after bone union
Min Jung Park, Cheungsoo Ha, Hyun Tak Kang, Yong Hyun Yoon, Jun-Ku Lee, Soo-Hong Han
Arthroscopy and Orthopedic Sports Medicine.2025; 12(2): 70. CrossRef
- Epidemiological changes and surgical trends of distal radius fractures in adults over 50 years during the COVID-19 pandemic in Korea: a nationwide repeated cross-sectional study
- 4,597 View
- 57 Download
- 3 Crossref
Review Articles
- Treatment of avulsion fractures around the knee
- Jeong-Hyun Koh, Hyung Keun Song, Won-Tae Cho, Seungyeob Sakong, Sumin Lim
- J Musculoskelet Trauma 2025;38(2):63-73. Published online March 31, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00073

-
Abstract
PDF
- Avulsion fractures of the knee occur when tensile forces cause a bone fragment to separate at the site of soft tissue attachment. These injuries, which frequently affect adolescent athletes, can involve the cruciate and collateral ligaments, arcuate complex, iliotibial band, and patellar and quadriceps tendons. Radiographs aid in the initial diagnosis, while computed tomography and magnetic resonance imaging facilitate a comprehensive evaluation of injury severity and concomitant damage. Specific avulsion fracture types include: anterior cruciate ligament avulsions (tibial site, Meyers and McKeever classification), posterior cruciate ligament avulsions (tibial attachment, Griffith's classification), Segond fractures (anterolateral complex injury), iliotibial band avulsions, medial collateral ligament avulsions (reverse Segond, Stieda fractures), arcuate complex avulsions ("arcuate sign"), medial patellofemoral avulsions (patellar dislocations), and patellar/quadriceps tendon avulsions. The treatment depends on the fracture location, displacement, and associated injuries. Non-displaced fractures can be managed conservatively, while displaced fractures or those with instability require surgical reduction and fixation. Prompt recognition and appropriate intervention prevent complications such as deformity, nonunion, malunion, and residual instability. This review provides an overview of the pathogenesis, diagnosis, and management of knee avulsion fractures to guide clinical decision-making.
-
Citations
Citations to this article as recorded by- Avulsionsfrakturen am Kniegelenk – eine Übersicht
Anton Ferdinand Schmidt, Christoph Kittl, Adrian Deichsel, Larissa Eckl, Riccardo D’Ambrosi, Arasch Wafaisade, Josina Maiti Münchgesang, Jakob Ackermann, Dominic T. Mathis, Lukas Münch, Gergo Merkely, Lena Eggeling, Andreas Martin Seitz, Karl F. Schüttler
Arthroskopie.2026; 39(4): 255. CrossRef - Lateral marginal fractures of the patella and patellofemoral pain
Jae-Ang Sim, Chul-Ho Kim, Ji Wan Kim
Journal of Musculoskeletal Trauma.2025; 38(3): 152. CrossRef
- Avulsionsfrakturen am Kniegelenk – eine Übersicht
- 42,004 View
- 305 Download
- 2 Crossref
- How to obtain the desired results from distal tibial nailing based on anatomy, biomechanics, and reduction techniques
- Jungtae Ahn, Se-Lin Jeong, Gu-Hee Jung
- J Musculoskelet Trauma 2025;38(2):74-85. Published online March 31, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00024

-
Abstract
PDF
- Distal tibial metaphyseal fractures are commonly caused by high-energy injuries in young men and osteoporosis in older women. These fractures should be clearly distinguished from high-energy pilon fractures. Although the optimal surgical intervention methods for distal tibial metaphyseal fractures remain uncertain and challenging, surgical treatments for nonarticular distal tibia fractures can be broadly divided into two types: plate fixation and intramedullary nail (IMN) fixation. Once functional reduction is achieved using an appropriate technique, distal tibial nailing might be slightly superior to plate fixation in reducing postoperative complications. Thus, the surgical strategy should focus on functional realignment and proceed in the following sequence: (1) restoring the original tibial length, regardless of whether fibular fixation is to be done; (2) making the optimal entry point through an anteroposterior (AP) projection based on the overlapping point between the fibular tip and lateral plateau margin; (3) placing Kirschner wires (Ø2.4 mm) as blocking pins (in the AP orientation for coronal control and in the mediolateral [ML] orientation for sagittal control) as close to the upper locking hole as possible without causing further comminution on the concave aspect of the short fragment; and (4) making the the distal fixation construct with at least two ML and one AP interlocking screw or two ML interlocking screws and blocking screws. After the IMN is adequately locked, blocking pins (Ø2.4 mm) need to be replaced by a 3.5 mm screw.
-
Citations
Citations to this article as recorded by- Rigid intramedullary nailing with suprapatellar approach for tibial shaft fractures in adolescents with open physes
Jong Wha Lee, Jae Ho Cho, Tae Hun Kim, Hyung Keun Song, Won-Tae Cho, Seungyeob Sakong, Hyun Il Choi, Sumin Lim
Injury.2026; 57(4): 113130. CrossRef - Impact of Foot Width on Patient-Reported Outcomes Assessed by 3-Dimensional Foot Morphometry in Hallux Valgus
Jungtae Ahn, Dae-Cheol Nam, Gu-Hee Jung
Clinics in Orthopedic Surgery.2025; 17(6): 1062. CrossRef
- Rigid intramedullary nailing with suprapatellar approach for tibial shaft fractures in adolescents with open physes
- 5,659 View
- 123 Download
- 2 Crossref
- Easily missed nondisplaced fractures accompanying complete fractures in the lower extremity and pelvis: a narrative review
- Young-Chang Park
- J Musculoskelet Trauma 2025;38(1):5-12. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00017

-
Abstract
PDF
- Nondisplaced fractures accompanying complete fractures are often difficult to detect on plain radiographs or computed tomography scans, posing a diagnostic challenge. The diagnosis of these frequently overlooked injuries can be delayed, potentially leading to suboptimal patient outcomes. This review discusses four commonly missed fracture patterns in the lower extremity and pelvis, including posterior involvement in fragility fractures of the pelvis, intertrochanteric extensions in isolated greater trochanter fractures, ipsilateral femoral neck fractures in high energy femoral shaft fractures, and posterior malleolar fractures in distal spiral tibial shaft fractures. An accurate diagnosis of these accompanying nondisplaced fractures is critical for optimizing surgical outcomes. Surgeons should incorporate thorough preoperative evaluations into their clinical practice to facilitate early detection and appropriate treatment strategies. Prompt identification and comprehensive management remain essential for improving patient outcomes.
-
Citations
Citations to this article as recorded by- Selective Anterior Fixation for Rami Fractures in Anteroposterior Compression-Type Pelvic Ring Injuries: Impact of Posterior Stability
Jeong-Hyun Koh, Sumin Lim, Won-Tae Cho, Seungyeob Sakong, Wan-Sun Choi, Daehyun Han, Hyung Keun Song
Journal of Clinical Medicine.2026; 15(10): 3773. CrossRef - Initial lateral stress radiographs predict instability in fragility fractures of the pelvis type I and II: a prospective observational study
Kyu-Hyun Yang, Jun-Young An, Young-Chang Park
Scientific Reports.2026;[Epub] CrossRef
- Selective Anterior Fixation for Rami Fractures in Anteroposterior Compression-Type Pelvic Ring Injuries: Impact of Posterior Stability
- 4,224 View
- 65 Download
- 2 Crossref
Original Article
- Biomechanical Investigation to Establish Stable Fixation Strategies for Distal Tibial Fractures in Various Situations: Finite Element Analysis Studies
- Sung Hun Yang, Jun Young Lee, Gu-Hee Jung, Hyoung Tae Kim, Ba Woo Ko
- J Korean Fract Soc 2024;37(2):71-81. Published online April 30, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.2.71
-
Abstract
PDF
- Purpose
This study examined the structural and mechanical stability as well as the clinical significance of various fixation constructs for distal tibial fractures using finite element analysis.
Materials and Methods
Fracture models with 20 mm and 120 mm defects were produced, and implants of an intramedullary nail and anatomical plate model were applied. An axial load of 800 N with 60% distribution in the medial compartment and 40% in the lateral compartment was applied and analyzed using Ansys ® software.
Results
In the intramedullary nail model, the maximum von Mises stress occurred at the primary lag screw hole and adjacent medial cortex, while in the plate model, it occurred at the locking holes around the fracture. The maximum shear stress on the bone and metal implant in the fracture model with a 20 mm defect was highest in the plate assembly model, and in the fracture model with a 120 mm defect, it was highest in the two-lag screw assembly model.
Conclusion
Based on an analysis of the maximum shear stress distribution, securing the fixation strength of the primary lag screw hole is crucial, and the assembly model of the intramedullary nail with two lag screws and a blocking screw applied was the model that best withstood the optimal load. Securing the locking hole directly above the fracture is believed to provide the maximum fixation strength because the maximum pressure in the plate model is concentrated in the proximal locking hole and the surrounding cortex. -
Citations
Citations to this article as recorded by- Loading-Condition Hierarchy of Anisotropy and Heterogeneity in Tibial Biomechanics: A Finite Element Study
Azadeh Ghouchani, Saba Mirzakhani, Amir M. Rashnavadi
Results in Engineering.2026; : 112129. CrossRef - How to obtain the desired results from distal tibial nailing based on anatomy, biomechanics, and reduction techniques
Jungtae Ahn, Se-Lin Jeong, Gu-Hee Jung
Journal of Musculoskeletal Trauma.2025; 38(2): 74. CrossRef
- Loading-Condition Hierarchy of Anisotropy and Heterogeneity in Tibial Biomechanics: A Finite Element Study
- 1,536 View
- 26 Download
- 2 Crossref
Review Article
- Innovative applications of artificial intelligence in orthopedics focusing on fracture and trauma treatment: a narrative review
- Chul-Ho Kim, Ji Wan Kim
- J Musculoskelet Trauma 2025;38(4):178-185. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00283
-
Abstract
PDF
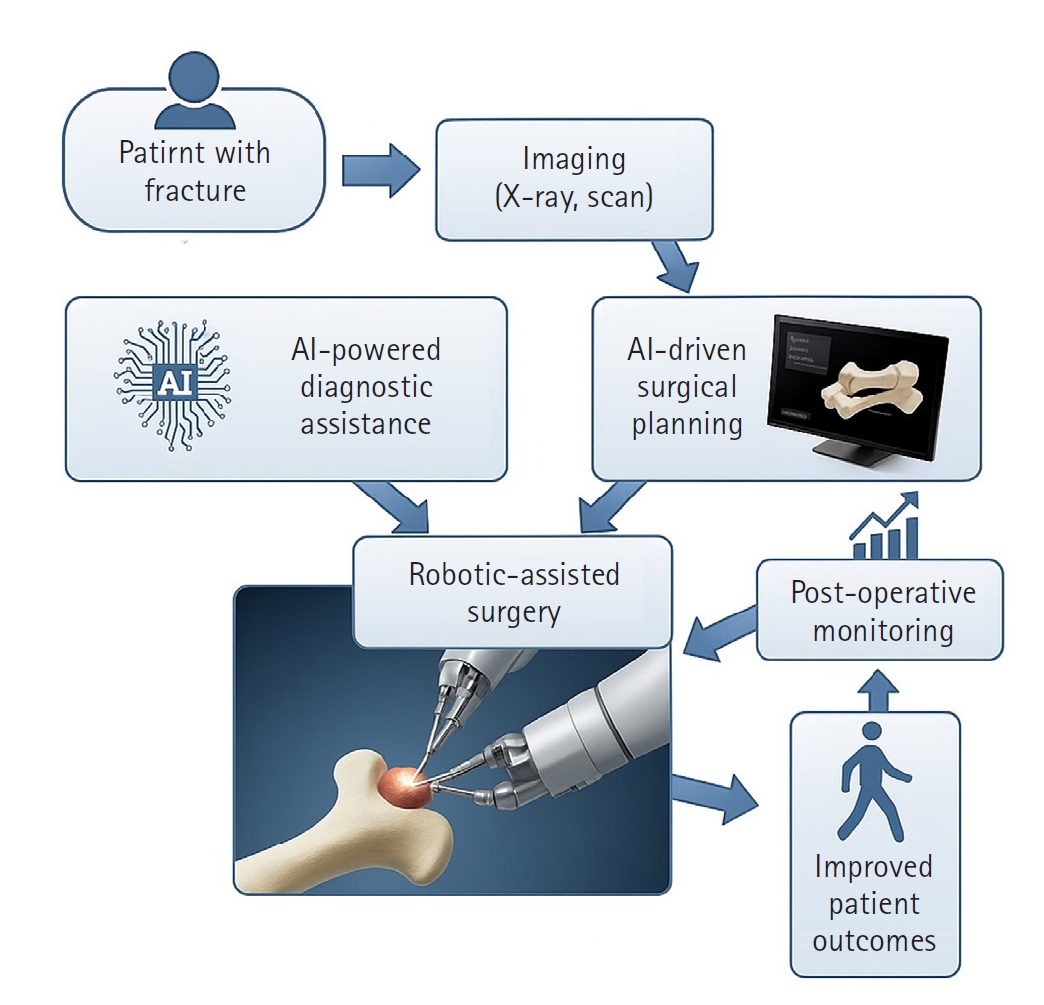
- Artificial intelligence (AI) is bringing about transformative changes in orthopedic surgery, with its potential being particularly prominent in the field of fracture and trauma treatment. This review explores the current applications and future prospects of AI-driven surgical planning and simulation, robot and image-based navigation surgery, and image-assisted diagnostic technologies. Robotic assistance in orthopedic surgery, which was initially applied to improve accuracy in component implantation for knee and hip arthroplasty and to achieve high precision in spinal screw placement, has recently expanded its use to include accurate, minimally invasive reduction of pelvic fractures. In diagnostics, AI aids in the early prediction and classification of ambiguous fractures in various anatomical regions—for example, detecting shoulder or hip fractures, identifying incomplete atypical femur fractures, and classifying femoral neck fractures—through X-ray image analysis. This improves diagnostic accuracy and reduces medical costs. However, significant challenges remain, including high initial costs, steep learning curves, a lack of long-term studies, data bias, and ethical concerns. Continued research, interdisciplinary collaboration, and policy support are crucial for the widespread adoption of these technologies.
-
Citations
Citations to this article as recorded by- AI-Assisted Fracture Detection in Orthopedic and Trauma Imaging: Where It Works, Where It Fails, and Principles for Safe Clinical Deployment
Wojciech Michał Glinkowski, Paweł Kaminski, Rafał Obuchowicz
Diagnostics.2026; 16(10): 1420. CrossRef
- AI-Assisted Fracture Detection in Orthopedic and Trauma Imaging: Where It Works, Where It Fails, and Principles for Safe Clinical Deployment
- 1,624 View
- 38 Download
- 1 Crossref
Original Articles
- Hook plate versus periarticular-type volar locking plate for distal radius fractures involving the volar lunate facet in Korea: a retrospective cohort study
- Hyun-Jae Park, Joo-Hak Kim
- J Musculoskelet Trauma 2025;38(4):221-228. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00241
-
Abstract
PDF
- Background
This study investigated the clinical and radiographic outcomes of hook plate (HP) fixation for volar lunate facet fractures, comparing them with periarticular-type volar locking plates (PVLPs).
Methods
A retrospective review was conducted on 24 patients with distal radius fractures involving volar lunate facet fragments who underwent surgery between January 2016 and April 2021. Patients were divided into two groups: HP (n=12) and PVLP (n=12). Radiographic union, wrist range of motion, Disabilities of the Arm, Shoulder and Hand (DASH) scores, and implant-related complications were compared. Statistical analyses included the Mann-Whitney U test and Fisher exact test.
Results
Radiographic union was achieved in all patients (100%), without secondary displacement or hardware failure. No significant differences were observed between the two groups in wrist flexion (P=0.152), extension (P=0.832), pronation (P=0.792), or supination (P=0.328). The mean DASH scores were 12.8±5.5 in the HP group and 14.6±6.0 in the volar plate group (P=0.449). One patient in the HP group experienced mild flexor tendinopathy that resolved with conservative management. No cases of tendon rupture or early reoperation were reported.
Conclusions
Fixation of volar lunate facet fractures using a HP yielded clinical and radiographic outcomes comparable to those of PVLPs, with a low rate of complications and reliable bony union. Due to its mechanical stability, compatibility with standard surgical approaches, and low risk of flexor tendon irritation, the HP may serve as a valuable alternative for managing volar lunate facet fractures. Level of evidence: IV. -
Citations
Citations to this article as recorded by- Open distal radius fracture with ulnar neurovascular injury treated with dorsal spanning plate fixation and vein interposition grafting: a case report
Kyeong-Eon Kim, Ho-Yong Lee, Shin-Woo Lee, Ji-Sup Kim
Journal of Musculoskeletal Trauma.2026; 39(3): 262. CrossRef
- Open distal radius fracture with ulnar neurovascular injury treated with dorsal spanning plate fixation and vein interposition grafting: a case report
- 1,261 View
- 32 Download
- 1 Crossref
- Risk factors of surgical complications after use of the femoral neck system: a random forest analysis
- Chul-Ho Kim, Hyun-Chul Shon, Han Soul Kim, Ji Wan Kim, Eic Ju Lim
- J Musculoskelet Trauma 2025;38(3):160-167. Published online July 23, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00157
-
Abstract
PDF
- Background
The femoral neck system (FNS), a novel fixation device for managing femoral neck fractures (FNFs), has gained popularity in recent years. However, analyses of the surgical complications and reoperation risks associated with the use of FNS remain limited.
Methods
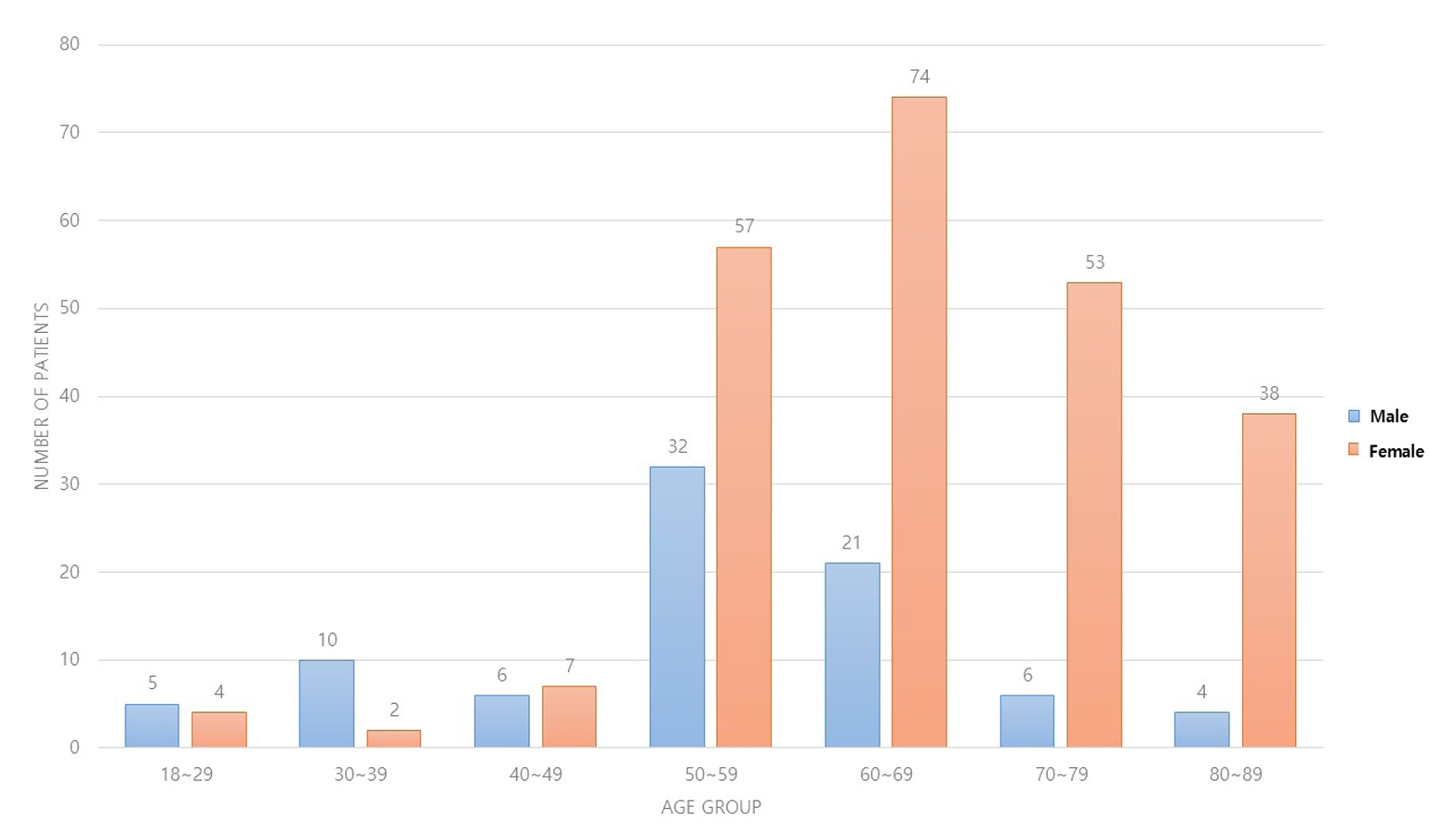
This retrospective observational study analyzed 57 patients who had undergone FNS fixation for FNF at two university hospitals between July 2019 and February 2024. Demographic, perioperative, and outcome variables, including age, sex, fracture classification (Garden, Pauwels, and AO), implant characteristics, tip-apex distance (TAD), neck shortening, and neck-shaft alignment, were analyzed. In addition to univariate analysis, a machine learning analysis was conducted using a random forest classifier with stratified sampling (80% training, 20% testing). The accuracy, precision, recall, F1-score, and area under the receiver’s operating curve were calculated to assess model performance.
Results
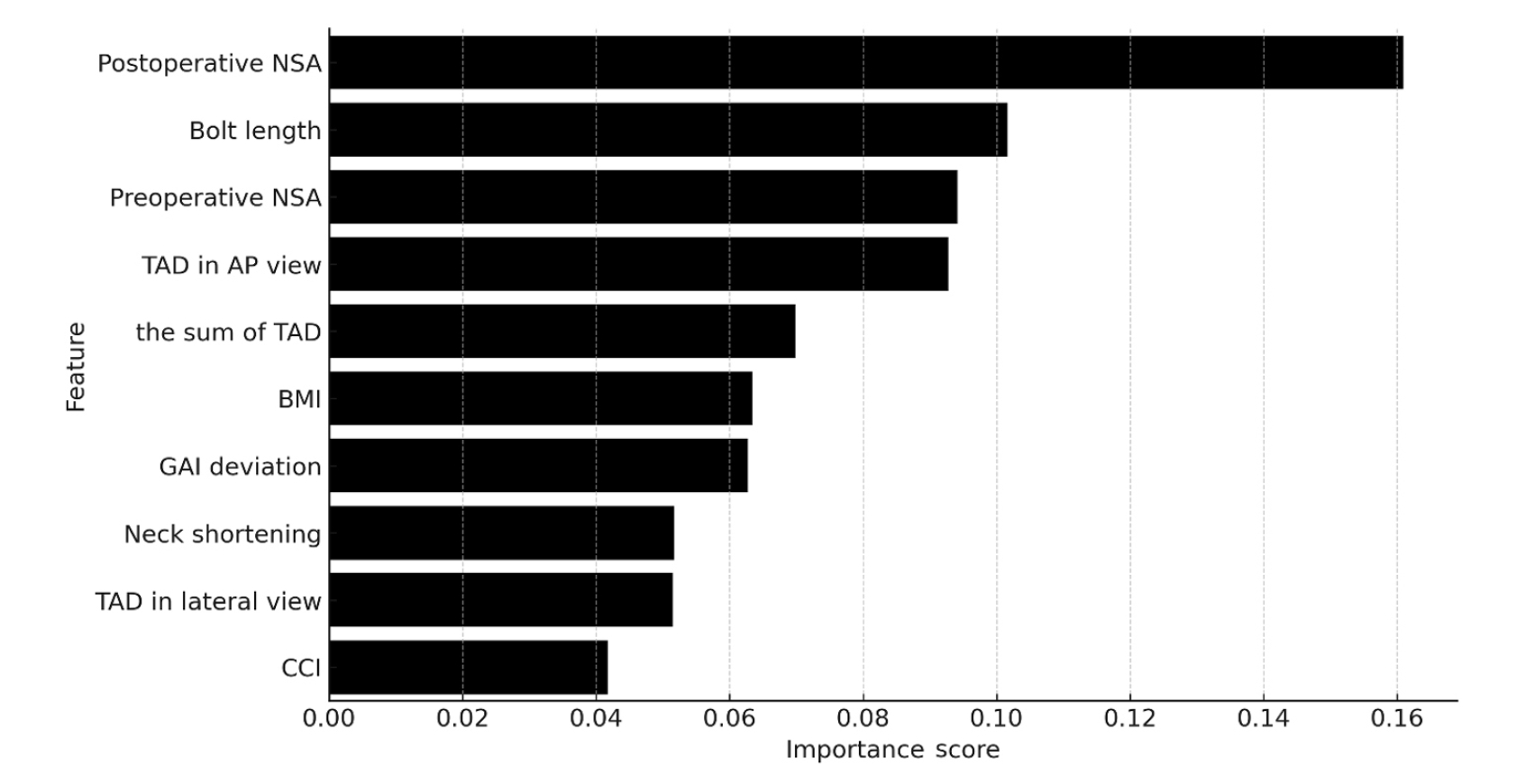
Ten patients experienced osteonecrosis of the femoral head (n=6), implant cut-out or penetration (n=3), and peri-implant fracture (n=1). Univariate analysis revealed that the TAD in the complication group was significantly shorter than that in the control group (12.1 vs. 16.7 mm; P=0.012). Additionally, neck shortening in the complication group was greater than that in the control group (4.9 vs. 2.3 mm; P=0.011). The random forest model achieved an accuracy of 83.3% and identified postoperative neck-shaft angle (NSA) as the most important predictor of complications (feature importance, 0.161), followed by bolt length (0.102) and preoperative NSA (0.094).
Conclusions
Risk factor analysis conducted using a random forest model identified postoperative NSA as the most important feature associated with postoperative complications following FNS. Therefore, care should be taken to normalize the postoperative NSA during FNF surgery. Level of Evidence: III. -
Citations
Citations to this article as recorded by- Length-stable fixation reduces femoral neck shortening in unstable femoral neck fractures: A retrospective comparative study of length-stable dynamic hip screw versus femoral neck system fixation
Seonghyun Kang, Wonseok Choi, Jeong Seok Choi, Eic Ju Lim, SungJin Ahn, Jong-Keon Oh, William T. Kent, Whee Sung Son, Jae-Woo Cho
Journal of Orthopaedic Surgery.2026;[Epub] CrossRef
- Length-stable fixation reduces femoral neck shortening in unstable femoral neck fractures: A retrospective comparative study of length-stable dynamic hip screw versus femoral neck system fixation
- 2,760 View
- 57 Download
- 1 Crossref
Review Article
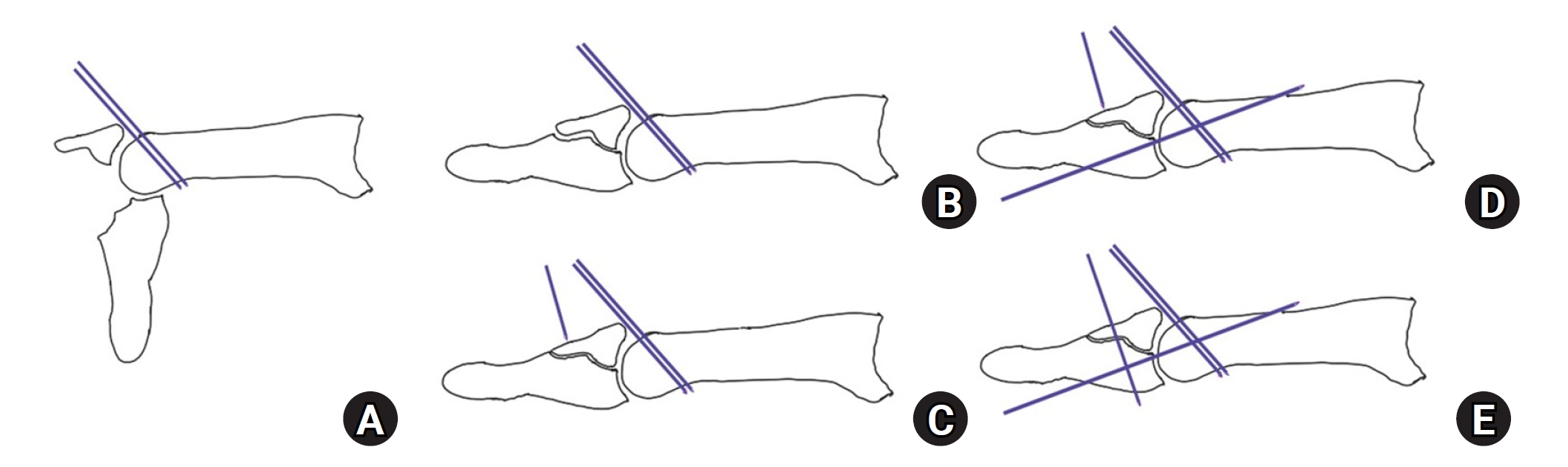
- Current concepts in the management of phalangeal fractures in the hand
- Hyun Tak Kang, Jun-Ku Lee
- J Musculoskelet Trauma 2025;38(3):109-123. Published online July 22, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00136
-
Abstract
PDF
- This review focuses on the treatment of hand fractures based on the anatomical location of the fractured phalanx, excluding the thumb, and examines recent studies on the topic. The main points are as follows: in most cases of hand fractures, conservative treatment should be prioritized over surgical intervention. The three key factors in determining whether surgical treatment is necessary are (1) whether the fracture is intraarticular, (2) the stability of the fracture itself, and (3) the extent of damage to surrounding soft tissues. The primary surgical treatment is closed reduction and Kirschner-wire fixation. The risk of rotational deformity increases with fractures closer to the proximal region. Intra- articular fractures may lead to subsequent stiffness and arthritis; thus, computed tomography is recommended to assess the fracture pattern. Anatomic reduction of intraarticular fragments is required, along with correction of the inherent joint instability. No surgical method has proven to be superior; it is advantageous for the surgeon to choose a surgical approach they are familiar with and confident in, based on the specific fracture and patient factors. Complications in hand fractures are various; the most frequent is stiffness, and nonunion is uncommon. Early joint motion is crucial in minimizing the risk of stiffness.
-
Citations
Citations to this article as recorded by- Imaging of hand and wrist injuries in alpine skiing: common injury mechanisms, imaging findings, and treatment
Andreas Josef Walch, Andreas Schweizer, Reto Sutter
Skeletal Radiology.2026;[Epub] CrossRef
- Imaging of hand and wrist injuries in alpine skiing: common injury mechanisms, imaging findings, and treatment
- 61,149 View
- 782 Download
- 1 Crossref
Original Articles
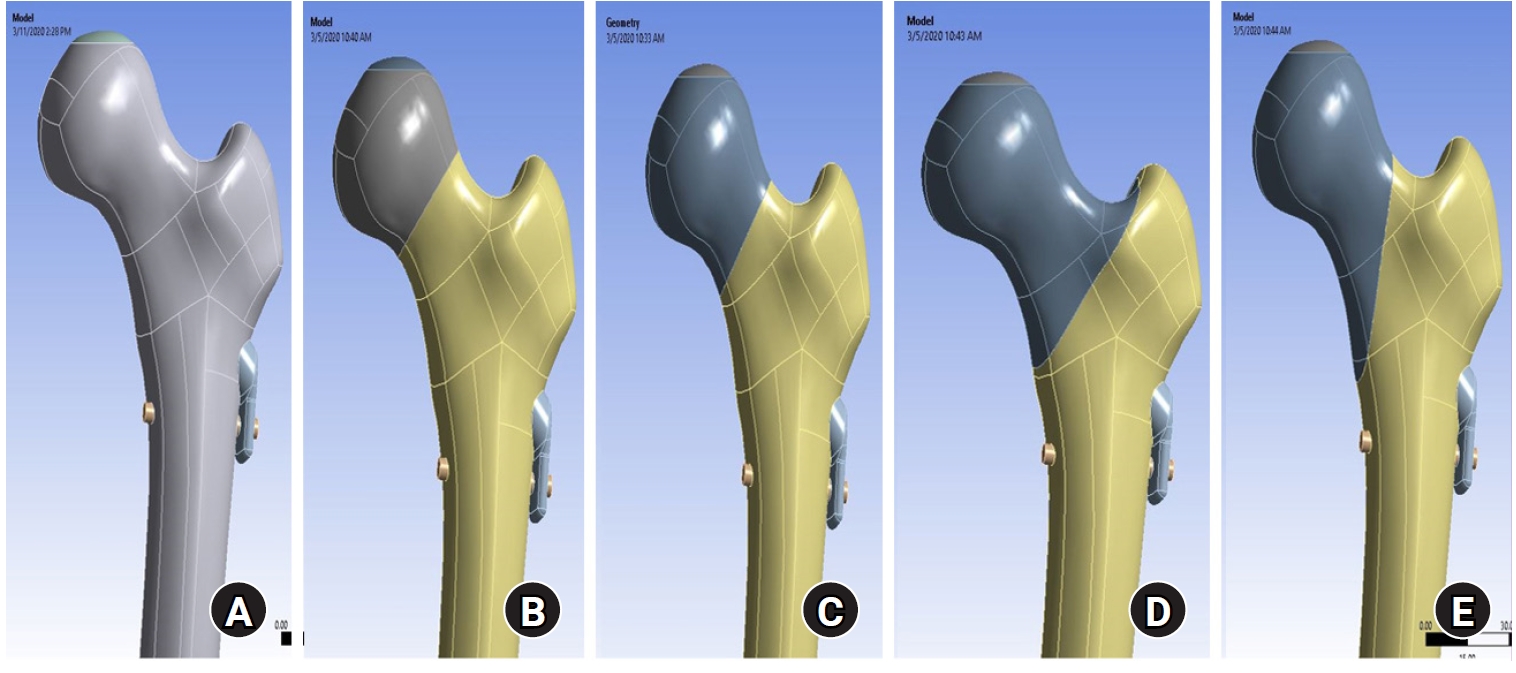
- Biomechanical finite element analysis of a femoral neck system fixation construct for femur neck fractures and clinical implications
- Hoon-Sang Sohn, Se-Lin Jeong, Gu-Hee Jung
- J Musculoskelet Trauma 2025;38(3):133-142. Published online July 22, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00108
-
Abstract
PDF
- Background
This study assessed the structural/mechanical stability of fixation constructs with a femoral neck system (FNS) via finite element analysis after simulating femoral neck fractures and explored the clinical implications.
Methods
We simulated subcapital, transcervical, basicervical, and vertical fracture models using a right femur (SAWBONES) and imported the implant model of FNS to Ansys (Ansys 19.0, Ansys Inc.) to place the implant in the optimal position. The distal end of the femur model was completely fixed and was abducted 7°. The force vector was set laterally at an angle of 3° and posteriorly at an angle of 15° in the vertical ground. The analysis was conducted using Ansys software with the von Mises stress (VMS) in megapascals (MPa).
Results
The maximum VMS of the fracture site was 67.01 MPa for a subcapital, 68.56 MPa for a transcervical, 344.54 MPa for a basicervical, and 130.59 MPa for a vertical model. The maximum VMS of FNS was 840.34 MPa for a subcapital, 637.37 MPa for a transcervical, 464.07 MPa for a basicervical, and 421.01 MPa for a vertical model. The stress distribution of basicervical and vertical fractures differed significantly, and the basicervical fracture had higher VMS at the bone, implant, and fracture sites.
Conclusions
FNS fixation should be performed with consideration the osseous anchorage in the femoral head, and this technique might be appropriate for vertical fractures. Regarding the VMS at the fracture site, FNS might be applied cautiously only to basicervical fractures with anatomical reduction without a gap or comminution. Level of evidence: IV. -
Citations
Citations to this article as recorded by- Finite element analysis of screw thread geometry and titanium plate materials in internal fixation of the human femur
Abdessamed Bachiri, Mustapha Amine Arab, Nadia Kadouri
Computer Methods in Biomechanics and Biomedical Engineering.2026; : 1. CrossRef
- Finite element analysis of screw thread geometry and titanium plate materials in internal fixation of the human femur
- 3,305 View
- 105 Download
- 1 Crossref
- The clinical outcome of treating elderly distal radius fractures by long volar locking plate with the elimination of irreducible metaphyseal comminuted volar cortical fragments: a retrospective case series
- Soo Min Cha
- J Musculoskelet Trauma 2025;38(1):13-22. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00003

-
Abstract
PDF
- Background
In severe comminuted metaphyseal distal radius fracture (DRF) of elderly patients, after maintaining only radiological parameters of the radius using long volar locking plates (VLPs), we inevitably eliminated a few volar cortical fragments of metaphysis. Here, we report the final radiological and clinical outcomes of our method. Methods: For the patients who were treated between 2014 and 2018, the demographic factors, the preoperative radiologic factors, area of the eliminated volar cortical fragment, and final radiologic parameter, were evaluated. Clinical outcomes and ranges of active motion were evaluated. Results: In total, 31 patients were included. The mean patient age was 77.3 years and the mean eliminated cortical area was 3.30 cm2. At the final follow-up, the mean volar tilt, radial inclination, articular step-off, and ulnar variance were 10.35°, 20.00°, 0.58 mm, and 0.71 mm, respectively. There were no definitive correlations between bone mineral density, fragment area, the largest cortical fragment diameter ratio and differences in final and immediate postoperative measurements of these radiological parameters, respectively. Visual analog scale and disabilities of the arm, shoulder, and hand (DASH) scores were satisfactory, and the mean arcs of flexion-extension and pronation-supination were 124.35° and 133.23°. Clinical outcomes were not significantly different according to the AO system category. Conclusions: For maintenance of radiological parameters of the radius, long VLPs are useful in older patients with DRFs who exhibit volar metaphyseal comminution, despite concurrent ulnar fractures. Inevitable elimination of irreducible free comminuted cortical fragments when filling the defect does not affect final radiological and clinical outcomes. Level of evidence: Level IV, case series. -
Citations
Citations to this article as recorded by- Open distal radius fracture with ulnar neurovascular injury treated with dorsal spanning plate fixation and vein interposition grafting: a case report
Kyeong-Eon Kim, Ho-Yong Lee, Shin-Woo Lee, Ji-Sup Kim
Journal of Musculoskeletal Trauma.2026; 39(3): 262. CrossRef
- Open distal radius fracture with ulnar neurovascular injury treated with dorsal spanning plate fixation and vein interposition grafting: a case report
- 3,805 View
- 52 Download
- 1 Crossref
- Clinical Outcomes of Triple Tension Band Wirings in Comminuted Patellar Fracture: A Comparison with Conventional Tension Band Wiring
- Hyun-Cheol Oh, Han-Kook Yoon, Joong-Won Ha, Sang Hoon Park, Sungwoo Lee
- J Korean Fract Soc 2024;37(2):82-86. Published online April 30, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.2.82
-
Abstract
PDF
- Purpose
This study devised triple tension band wirings (TTBW) fixation in patients with comminuted patella fractures to compare the clinical result of TTBW with that of tension band wiring (TBW).
Materials and Methods
This study was conducted on 91 patients who had undergone surgery diagnosed with acute patella fracture from January 2011 to December 2016. The study included 51 double TBW patients (Group 1) and 40 patients with TTBW (Group 2).
Results
Five out of 51 cases had a loss of reduction and fixation failure in Group 1, and no failure of fracture formation healing occurred in Group 2. Nonunion was noted in one case in Group 1 and no case in Group 2. Eight K-wire migration cases were observed in Group 1, which was not observed in Group 2. Six patients in Group 1 underwent revisional surgery. No patients in Group 2 had a reoperation. As a result of a one-year follow-up after the operation, the mean range of motion of the knee joint in groups 1 and 2 was 128.3°±11.3° and 127.9°±10.8°, respectively. The Lysholm’s scores for groups 1 and 2 were 90.8±4.2 and 90.3±3.8 points, respectively, which was not statistically significant.
Conclusion
TTBW is a helpful technique for the surgical treatment of comminuted patella fractures. The TTBW method has less reoperation due to nonunion and fixation failure. After a one-year followup, the clinical results were similar to the conventional TBW method. -
Citations
Citations to this article as recorded by- Lateral marginal fractures of the patella and patellofemoral pain
Jae-Ang Sim, Chul-Ho Kim, Ji Wan Kim
Journal of Musculoskeletal Trauma.2025; 38(3): 152. CrossRef
- Lateral marginal fractures of the patella and patellofemoral pain
- 1,454 View
- 9 Download
- 1 Crossref
- Prediction of Syndesmotic Instability according to the Lateral Malleolus Fracture Pattern in Supination-External Rotation Type Ankle Fractures: Short Oblique versus Long Oblique Fracture
- Chan-Jin Park, Min-Su Lee, Keun-Bae Lee
- J Korean Fract Soc 2024;37(1):39-45. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.39
-
Abstract
PDF
- Purpose
This study examined whether preoperative radiological evaluations can predict syndesmotic instability according to the lateral malleolus fracture pattern in supination-external rotation-type ankle fractures.
Materials and Methods
This study enrolled 132 patients (132 ankles) with supination-external rotation stage 3 and 4 ankle fractures. Three-dimensional computed tomography was used for the morphological classification of the lateral malleolus fractures. A long oblique fracture was defined when the posterior cortical bone height of the fracture was 4.5 cm or more from the plafond of the distal tibial articular surface. A short oblique fracture was defined when the height was less than 4.5 cm. The demographic characteristics and syndesmotic instability of the two groups were evaluated.
Results
Short oblique fractures were confirmed in 102 cases, and long oblique fractures were confirmed in 30 cases. Long oblique fractures occurred at a statistically significantly higher incidence in younger ages and among males compared to short oblique fractures. Syndesmotic instability was more common in long oblique fractures.
Conclusion
In supination-external rotation-type ankle fractures, syndesmotic instability was observed in approximately 13%. Specifically, when the fracture pattern of the lateral malleolus is long oblique, the incidence of syndesmotic instability is approximately three times higher than in short oblique fractures. Therefore, meticulous evaluations of the lateral malleolus fracture pattern and establishing an appropriate treatment plan before surgery are crucial. -
Citations
Citations to this article as recorded by- Relationship of lateral malleolar fracture patterns to posterior malleolar fracture morphology in supination-external rotation ankle fractures in Korea: a retrospective cohort stduy
Jong-Eun Kim, Chan-Jin Park, Jun-Young Lee, Keun-Bae Lee, Gun-Woo Lee
Journal of Musculoskeletal Trauma.2025; 38(4): 212. CrossRef
- Relationship of lateral malleolar fracture patterns to posterior malleolar fracture morphology in supination-external rotation ankle fractures in Korea: a retrospective cohort stduy
- 1,204 View
- 14 Download
- 1 Crossref
- Triplane Fracture Management: Prediction of Periosteal Entrapment and the Need for Open Reduction by Measurements of the Physeal Fracture Gap in Preoperative Computed Tomography Scans
- Dae Hee Lee, Joo Han Kwon, Jae Uk Jung
- J Korean Fract Soc 2024;37(1):1-7. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.1
-
Abstract
PDF
- Purpose
This study measured the physeal fracture gap on preoperative ankle computed tomography (CT) to predict the periosteal entrapment that requires an open reduction in distal tibia triplane fractures.
Materials and Methods
This study retrospectively reviewed patients who had undergone internal fixation for a triplane fracture from April 2004 to September 2022. The demographic data, including age,body mass index, and past medical history, were analyzed. In the radiographic evaluations, ankle CT and ankle simple radiographs, including anteroposterior (AP), lateral, and mortise views, were taken preoperatively. Postoperatively, simple ankle radiographs were obtained periodically, including AP, mortise, and lateral views. The physeal fracture gap was measured on ankle CT, and the larger gap between the coronal and sagittal view of CT was selected. The residual physeal gap <2 mm was considered an adequate reduction.
Results
Of 17 cases, three demonstrated successful reduction using closed reduction techniques. Periosteal entrapment was observed in 14 cases open reduction cases. In all three closed reduction cases, the physeal gap estimated on preoperative ankle CT was under 3 mm with a mean gap of 2.4±0.2 mm (range, 2.1-2.5 mm). In the remaining 14 open reduction cases, the measured physeal gap was over 3 mm, averaging 5.0±2.7 mm (range, 3.1-12.2 mm). There was a significant difference in the preoperative physeal gap between the two groups (p<0.01). Overall, good reduction was achieved in all 17 cases; the postoperative physeal gap was under 2 mm with a mean of 1.0±0.5 mm (closed reduction group, 0.5±0.2 mm; open reduction group, 1.1±0.5 mm).
Conclusion
Open reduction is strongly recommended for triplane fractures with a physeal fracture gap of 3 mm or more in preoperative ankle CT, suggesting the possibility of an entrapped periosteum in the fracture gap. -
Citations
Citations to this article as recorded by- Diagnostic values of radiographic indices for predicting periosteal entrapment in pediatric proximal phalangeal base physeal fractures of toes
Ho Young Park, Jeong-Seok Moon, Kiwook Kim
Skeletal Radiology.2026; 55(1): 97. CrossRef
- Diagnostic values of radiographic indices for predicting periosteal entrapment in pediatric proximal phalangeal base physeal fractures of toes
- 2,553 View
- 32 Download
- 1 Crossref
 First
First Prev
Prev

