 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Review Articles
- Treatment of avulsion fractures around the knee
- Jeong-Hyun Koh, Hyung Keun Song, Won-Tae Cho, Seungyeob Sakong, Sumin Lim
- J Musculoskelet Trauma 2025;38(2):63-73. Published online March 31, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00073

-
 Abstract
Abstract
 PDF
PDF - Avulsion fractures of the knee occur when tensile forces cause a bone fragment to separate at the site of soft tissue attachment. These injuries, which frequently affect adolescent athletes, can involve the cruciate and collateral ligaments, arcuate complex, iliotibial band, and patellar and quadriceps tendons. Radiographs aid in the initial diagnosis, while computed tomography and magnetic resonance imaging facilitate a comprehensive evaluation of injury severity and concomitant damage. Specific avulsion fracture types include: anterior cruciate ligament avulsions (tibial site, Meyers and McKeever classification), posterior cruciate ligament avulsions (tibial attachment, Griffith's classification), Segond fractures (anterolateral complex injury), iliotibial band avulsions, medial collateral ligament avulsions (reverse Segond, Stieda fractures), arcuate complex avulsions ("arcuate sign"), medial patellofemoral avulsions (patellar dislocations), and patellar/quadriceps tendon avulsions. The treatment depends on the fracture location, displacement, and associated injuries. Non-displaced fractures can be managed conservatively, while displaced fractures or those with instability require surgical reduction and fixation. Prompt recognition and appropriate intervention prevent complications such as deformity, nonunion, malunion, and residual instability. This review provides an overview of the pathogenesis, diagnosis, and management of knee avulsion fractures to guide clinical decision-making.
-
Citations
Citations to this article as recorded by
- Avulsionsfrakturen am Kniegelenk – eine Übersicht
Anton Ferdinand Schmidt, Christoph Kittl, Adrian Deichsel, Larissa Eckl, Riccardo D’Ambrosi, Arasch Wafaisade, Josina Maiti Münchgesang, Jakob Ackermann, Dominic T. Mathis, Lukas Münch, Gergo Merkely, Lena Eggeling, Andreas Martin Seitz, Karl F. Schüttler
Arthroskopie.2026;[Epub] CrossRef - Lateral marginal fractures of the patella and patellofemoral pain
Jae-Ang Sim, Chul-Ho Kim, Ji Wan Kim
Journal of Musculoskeletal Trauma.2025; 38(3): 152. CrossRef
- Avulsionsfrakturen am Kniegelenk – eine Übersicht
- 35,960 View
- 299 Download
- 2 Crossref

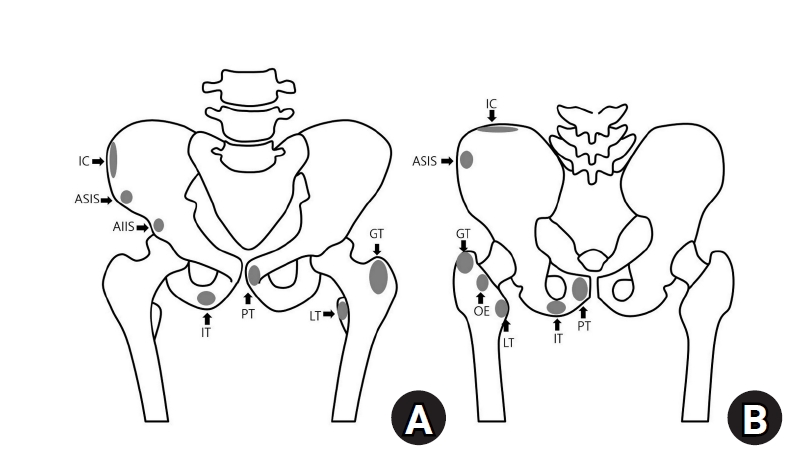
- Avulsion fractures around the hip joint and pelvis
- Won-Sik Choy, Yonghan Cha, Jung-Taek Kim, Jun-Il Yoo, Jin-Woo Kim
- J Musculoskelet Trauma 2025;38(2):53-62. Published online March 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00010
-
Abstract
PDF
- Avulsion fractures occur when tendons or ligaments are subjected to forces greater than they can withstand at the apophysis or enthesis, regardless of fusion status. The pelvis and hip joint are vulnerable to these injuries due to the diverse muscular structures in these structures, which serve as origins for multiple muscles leading to the lower extremities. Pelvic avulsion fractures commonly affect young athletes, but can also occur in adults. The diagnosis typically involves assessing trauma history, a clinical examination, and radiographic imaging. If the diagnosis is unclear, additional tests such as computed tomography and magnetic resonance imaging may assist in the diagnosis and provide useful information for treatment decisions. While most avulsion fractures respond well to conservative treatment, surgical intervention may be preferred in severe displacements, cases of significant retraction in active athletes, or when a faster recovery is necessary. Chronic or neglected injuries may lead to excessive osseous formation around the pelvis, causing impingement syndromes. Recognizing characteristic radiological findings based on pelvic anatomy helps to make an accurate diagnosis, as chronic injuries can mimic tumors or infectious conditions, necessitating a careful differential diagnosis.
-
Citations
Citations to this article as recorded by- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
Dawid Bartosik, Bartlomiej Cwikla, Anna Kowalczyk, Michalina Loson-Kawalec, Anna Palka-Szymaniec, Bartosz Starzynski, Alina Keska, Jakub Szkuta, Klaudia Wojcik
Cureus.2026;[Epub] CrossRef - Outcomes of Conservative Versus Surgical Treatment of Adolescent Pelvic and Hip Avulsion Fractures: A Systematic Review and Meta-Analysis
Lindsey L. Molina, Andrew M. Block, Sasha Carsen, Allison E. Crepeau, Tyler J. Stavinoha, Michael M. Chau, Jeffrey J. Nepple
Journal of Pediatric Orthopaedics.2026;[Epub] CrossRef - Diagnostic Accuracy of Ultrasound for Adolescent Pelvic Avulsion Fractures: A Blinded Multirater Study
Meena Meiyyappan, Robert Van Pelt, Kate Lampe, Jane Chung, Matthew Ditzler, Shane Miller, Henry Ellis, Hamza Alizai, Matthew Hammer, Ben Johnson, Charles Wyatt, Jacob Jones
Journal of Clinical Ultrasound.2026;[Epub] CrossRef
- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
- 18,737 View
- 202 Download
- 3 Crossref
- Avulsion Fractures of around the Hand
- Dong Whan Kim, Jung Il Lee
- J Korean Fract Soc 2024;37(3):158-168. Published online July 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.3.158
-
Abstract
PDF
- An avulsion fracture occurs when soft tissues, including the tendons and ligaments, are forcibly detached from the main bone by an external force. The hand contains numerous anatomical structures, such as ligaments, tendons, and volar plates, which are essential for maintaining multidirectional motion and joint stability. Excessive force applied in a specific direction can damage these structures, leading to avulsion fractures around the joint. These fractures can result in severe complications if left untreated or improperly managed, including joint deformity, contracture, nonunion or malunion of the fracture, secondary osteoarthritis, and limited range of motion. Therefore, an accurate examination, diagnosis, and appropriate treatment are crucial for preventing these adverse outcomes. An avulsion fracture can be managed conservatively when the avulsed fragment does not compromise joint stability or motion. Nevertheless, surgical intervention is required to stabilize the fragment if it affects joint stability or motion. The use of internal fixation has become more prevalent because of recent advances in small implants for fixation.
- 2,203 View
- 30 Download
- Avulsion Fractures around the Hip Joint and Pelvis
- Ha-Yong Kim, Hajun Jang, Jung-Taek Kim, Jin-Woo Kim, Jun-Il Yoo, Won-Sik Choy, Yonghan Cha
- J Korean Fract Soc 2024;37(3):150-157. Published online July 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.3.150
-
Abstract
PDF
- Avulsion fractures occur when tendons or ligaments are subjected to forces greater than they can withstand at the apophysis or enthesis, regardless of the fusion status. Given the diverse muscular structures around the pelvis and hip joint, which serve as origins for multiple muscles leading to the lower extremities, these areas are vulnerable to such injuries. Pelvic avulsion fractures commonly af-fect young athletes, but they can also occur in adults. Diagnosis typically involves assessing the trauma history, clinical examination, and radiographic imaging. In cases of unclear diagnosis, additional tests, such as computed tomography or magnetic resonance imaging, may assist in treatment decisions and diagnosis. Although most avulsion fractures respond well to conservative treatment, surgical interven-tion may be preferred in severe displacements, significant retraction in active athletes, or when a faster recovery is necessary. Chronic or neglected injuries may lead to excessive osseous formation around the pelvis, causing impingement syndromes. Recognizing the characteristic radiological findings based on the pelvic anatomy aids in accurate diagnosis because chronic injuries might mimic tumors or infectious conditions, necessitating a careful differential diagnosis.
- 2,589 View
- 51 Download
- Treatment of Avulsion Fractures around the Knee
- Sumin Lim
- J Korean Fract Soc 2024;37(2):117-124. Published online April 30, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.2.117
-
Abstract
PDF
- Avulsion fractures are common in athletes and result from high-impact or sudden, forceful movements involving the separation of a bone fragment at the ligament or tendon attachment site. The key focus areas include the anterior and posterior cruciate ligaments, medial collateral ligament, anterolateral complex, arcuate complex, medial patellofemoral ligament, patellar tendon, and quadriceps tendon. Diagnostic approaches combine radiography with advanced imaging techniques, such as computed tomography and magnetic resonance imaging, to elucidate the extent of injury and guide treatment decisions. Treatment ranges from conservative management for non-displaced fractures to surgical intervention for displaced fractures, with strategies customized based on the specific ligament involved and the nature of the fracture.
- 2,725 View
- 16 Download
- Avulsion Fractures in the Ankle and Foot
- Gyeong Hoon Lim, Jae Won Kim, Sung Hyun Lee
- J Korean Fract Soc 2024;37(2):102-116. Published online April 30, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.2.102
-
Abstract
PDF
- An avulsion fracture occurs when a muscle-tendon unit attached to a bone produces sufficient force to tear a fragment of the bone. If not treated properly, this injury can lead to deformity, nonunion, malunion, pain, and disability. Although avulsion fractures around the foot and ankle can occur anywhere there are tendon and ligament attachments, they are common in the anterior talofibular ligament, anterior-inferior tibiotalar ligament, calcaneal tuberosity, the base of the fifth metatarsal, and navicular bone. The optimal treatment for each fracture depends on the location and severity of the fracture. Conservative treatment involves limiting weight bearing for a period, splint immobilization, and using various orthoses. Surgical treatment is usually reserved for cases of severe displacement or when nonsurgical treatment has failed. The goals of surgery include reduction of the fracture fragment, prevention of nonunion or malunion and soft tissue injury, and early return to function. The decision for each treatment modality may depend on the patient demographics or preferences and the surgeon experience. This review summarizes previous and current views on the pathogenesis, diagnosis, and treatment of common avulsion fractures to guide the treatment and diagnosis.
- 4,779 View
- 73 Download
Case Reports
- Isolated Avulsion Fracture of the Subscapularis from the Lesser Tuberosity of the Humerus in a 12-Year-Old Boy - A Case Report -
- Shin Seung Park, Chung Shik Shin, Won Bin Song
- J Korean Fract Soc 2022;35(2):68-73. Published online April 30, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.2.68
-
Abstract
PDF
- An isolated avulsion fracture of the subscapularis from the lesser tuberosity of the proximal humerus is rare in the pediatric population and only a couple of cases have been described in literature. A 12-yearold right-handed boy, was admitted to the hospital with left shoulder pain after falling down the previ-ous day. Physical examination revealed tenderness on the lesser tuberosity and intertubercular groove of the humerus and a limited range of motion. Ultrasonography, computed tomography, and magnetic resonance imaging showed an isolated avulsion fracture of the subscapularis tendon from the lesser tuberosity of the humerus, accompanied by medial subluxation of the long head of the biceps tendon. In this case, a subscapularis avulsion fracture which is rare in this age group was detected at an early stage, and surgical treatment resulted in positive outcomes. Subscapularis avulsion fractures in children are difficult to diagnose in the early stages, and if not treated on time, the symptomatic improvement may be delayed. Timely and accurate diagnosis and treatment can help faster return to normal activi-ties. We would therefore like to report this case with a literature review.
- 795 View
- 4 Download
- Avulsion Fracture of the Posterior Cruciate Ligament from Femoral Insertion Occurred in a Patient with Residual Poliomyelitis: A Case Report
- Wonchul Choi, Taesup Kim
- J Korean Fract Soc 2018;31(4):149-153. Published online October 31, 2018
- DOI: https://doi.org/10.12671/jkfs.2018.31.4.149
-
Abstract
PDF
- Avulsion fracture of the posterior cruciate ligament from its femoral insertion is quite rare, particularly in adults, and the treatment guidelines have not been established. A 68-year-old female patient with residual poliomyelitis presented with an avulsion fracture of the femoral insertion of the posterior cruciate ligament after a falling accident and was treated with arthroscopic headless compression screw fixation and pull-out suture of the avulsed ligament. We report this case with a relevant discussion of this type of injury.
- 652 View
- 0 Download
- Avulsion of the Femoral Attachment of Anterior Cruciate Ligament Associated with Ipsilateral Femoral Shaft Fracture in Skeletally Mature Patient: A Case Report
- Seong Eun Byun, Taesup Kim, Bang Hyun Kim, Jae Hwa Kim, Soo Hong Han, Wonchul Choi
- J Korean Fract Soc 2016;29(3):200-205. Published online July 31, 2016
- DOI: https://doi.org/10.12671/jkfs.2016.29.3.200
-
Abstract
PDF
- Avulsion fracture at the femoral attachment of the anterior cruciate ligament (ACL) is very rare and has been reported mostly in skeletally immature patients. Authors experienced a case of avulsion fracture at the femoral attachment of ACL in a skeletally mature, a 21-year-old male associated with ipsilateral femoral shaft fracture. Here, authors report on the case with a literature review. Care should be taken because an avulsion fracture at the femoral attachment of ACL can be accompanied by ipsilateral femoral shaft fracture in skeletally mature patients.
- 776 View
- 2 Download
- Isolated Avulsion Fracture of the Lesser Tuberosity of the Humerus: A Case Report
- Tae Ho Kim, Ki Do Hong, Sung Sik Ha, Jae Chun Sim, Min Chul Sung
- J Korean Fract Soc 2014;27(1):72-76. Published online January 31, 2014
- DOI: https://doi.org/10.12671/jkfs.2014.27.1.72
-
Abstract
PDF
- Isolated avulsion of the lesser tuberosity of the humerus is a rare injury. The mechanism of injury is the avulsion of the lesser tuberosity from forced contractions of the subscapularis muscle when the arm is forced into an externally rotated position on shoulder abduction. Authors report a case for isolated avulsion of the lesser tuberosity of the humerus which was treated with open reduction and transosseous suture fixation, as well as a view of the literature.
-
Citations
Citations to this article as recorded by- What are the patient-reported outcomes, functional limitations, and complications after lesser tuberosity fractures? a systematic review of 172 patients
Reinier W.A. Spek, Bram J.A. Schoolmeesters, Chantal den Haan, Ruurd L. Jaarsma, Job N. Doornberg, Michel P.J. van den Bekerom
JSES International.2021; 5(4): 754. CrossRef
- What are the patient-reported outcomes, functional limitations, and complications after lesser tuberosity fractures? a systematic review of 172 patients
- 1,223 View
- 5 Download
- 1 Crossref
- Surgical Management of Comminuted Avulsion Fracture of the Proximal Fibula with Lateral Collateral Ligament Injury: Technical Note
- Jong Min Kim, Byeong Mun Park, Sang Hoo Lee, Seung Ju Jeon, Jun Beum Shin, Kyeong Seop Song
- J Korean Fract Soc 2013;26(1):77-80. Published online January 31, 2013
- DOI: https://doi.org/10.12671/jkfs.2013.26.1.77
-
Abstract
PDF
- Anteromedial force to the knee in an extended position can cause an avulsion fracture of the proximal fibula with combined injuries to the posterolateral ligaments. Avulsion fractures of the proximal fibula are rare and current management of these fractures is based on few descriptions in literature. Various surgical methods of fixation for these fractures have been reported, but there is still no standard treatment modality. Anatomic reduction of these fractures is technically difficult, and failure of reduction may cause posterolateral instability, secondary arthritis and other complications. We present our experience with two such cases of comminuted avulsion fractures of the proximal fibular with posterolateral ligament ruptures surgically fixated with a locking compression hook plate and non absorbable sutures.
-
Citations
Citations to this article as recorded by- Fixation of fibular head avulsion fractures with the proximal tibiofibular screw: Technique guide and clinical experience
Ryan A. Paul, Shu Yang Hu, Ananya Pathak, Ryan Khan, Daniel B. Whelan
Trauma Case Reports.2025; 57: 101175. CrossRef - Treatment of avulsion fractures around the knee
Jeong-Hyun Koh, Hyung Keun Song, Won-Tae Cho, Seungyeob Sakong, Sumin Lim
Journal of Musculoskeletal Trauma.2025; 38(2): 63. CrossRef - Treatment of Avulsion Fractures around the Knee
Sumin Lim
Journal of the Korean Fracture Society.2024; 37(2): 117. CrossRef
- Fixation of fibular head avulsion fractures with the proximal tibiofibular screw: Technique guide and clinical experience
- 2,324 View
- 54 Download
- 3 Crossref
- Avulsion Fracture of Calcaneal Tubercle Treated with Cannulated Cancellous Screws and Wire: Surgical Technique
- Chang Ho Yi, Jin Rok Oh
- J Korean Fract Soc 2011;24(3):262-266. Published online July 31, 2011
- DOI: https://doi.org/10.12671/jkfs.2011.24.3.262
-
Abstract
PDF
- The incidence rate of calcaneal fracture consists about 2% of all fractures, and, of the fracture, calcaneal tubercle avulsion fracture is known to be rare. To treat non-displaced calcaneal tubercle avulsion fracture, conservative treatment such as cast fixation is applied. However, most cases accompany displacement of the avulsion fragment, and, usually, surgery is necessary to treat the displaced fracture. Although surgical fixation simply by cancellous screw or tension wire is widely used, fixation failure is potential complication in this method. Thus, this study wants to introduce a prospective and useful method that further strengthens the calcaneal fixation by using both cannulated screw and tension band wiring.
- 1,151 View
- 10 Download
- Avulsion Fracture of Calcaneal Apophysis in an Adolescent Gymnast: A Case Report
- Youn Moo Heo, Whan Young Chung, Sang Bum Kim, Cheol Yong Park, Jin Woong Yi
- J Korean Fract Soc 2009;22(4):288-291. Published online October 31, 2009
- DOI: https://doi.org/10.12671/jkfs.2009.22.4.288
-
Abstract
PDF
- The avulsion fracture of calcaneal apophysis by Achilles tendon in children is quite rare. It may occur with the injury of the apophysis on the calcaneal tuberosity in the children below the age of 12 to 15 before the union of the apophysis. The authors surgically treated a 14-year-old gymnast with the avulsion fracture of the calcaneal tuberosity who injured at the landing of the floor exercise. Radiographs at the fourteen months of follow-up showed slight irregularity of the calcaneal tuberosity but there were no pain or limitation of activity. We report a case with the review of literatures.
- 1,127 View
- 12 Download
- Bilateral PCL Avulsion Fracture from Tibial Attatchment Site in a 16-years-old Male : A Case Report
- Hee Gon Park
- J Korean Fract Soc 2009;22(3):189-192. Published online July 31, 2009
- DOI: https://doi.org/10.12671/jkfs.2009.22.3.189
-
Abstract
PDF
- Posterior cruciate ligament avulsion fracture is occurred by high energy trauma, usually in motor vehicle accident or sports injury. Bilateral posterior cruciate ligament avulsion fracture is not yet reported in Korea. Authors report a case of bilateral posterior cruciate ligament avulsion fracture in 16-years-old man treated with anatomical reduction and internal fixation with a review of literature.
- 694 View
- 1 Download
Original Article
- Comparison of the Surgical Treatment Results of Avulsion Fracture of the Anterior Cruciate Ligament between Children and Adults
- Eun Kyoo Song, Sang Jin Park, Keun Bae Lee
- J Korean Fract Soc 2007;20(2):196-201. Published online April 30, 2007
- DOI: https://doi.org/10.12671/jkfs.2007.20.2.196
-
Abstract
PDF
- PURPOSE
To compare the clinical and radiological results after surgical treatments of the avulsion fractures of ACL between children and adults.
MATERIALS AND METHODS
40 cases (18 cases of children, 22 cases of adults), who underwent surgical treatments after avulsion fractures of the ACL and followed up more than one year, were enrolled. Fractures were classified by modified Meyers & McKeever criteria. Range of motion, LK score, Lachman test, Pivot-Shift test, quadriceps muscle atropy and Telos® stress arthrometer were compared.
RESULTS
The types of fracture in children were categorized into 8 cases of type II, 10 cases of type III, and 2, 15, 5 cases of type II, III, IV each in adult group. Mean LK score showed significant difference between 99.3 points in children and 89.5 points in adults (p<0.05). In addition, accompanied injuries and the high degree of fracture leaded low LK score. However, there was no significant difference in range of motion, Lachman test and Pivot-Shift test. Anterior laxity by Telos® device showed an average of 2.0 mm in children, 2.5 mm in adults (p>0.05).
CONCLUSION
Children group showed better treatment results of avulsion fracture of ACL. Higher incidence of type II fractures and less combined injuries considered to be factors for better results.
- 834 View
- 1 Download
Case Report
- Avulsion Facture of Short External Rotators in the Proximal Femur: A Case Report
- Myung Rae Cho, Sang Bong Ko, Dae Ui Jeung
- J Korean Fract Soc 2005;18(3):345-348. Published online July 31, 2005
- DOI: https://doi.org/10.12671/jkfs.2005.18.3.345
-
Abstract
PDF
- Although avulsion fractures of greater and lesser trochanters rarely develop in hip fractures, avulsion fracture of short external rotators has not reported still online literature. Moreover, avulsion fracture of short external rotators can simulate the intertrochanteric fracture, and is difficult to differentiate from it on plain radiograph. This study is on the case 74-year old male patient who had avulsion fracture of short external rotators, and had the internal fixation with wire by open reduction under the diagnosis of the intertrochanteric fracture.
- 703 View
- 1 Download
Original Articles
- Avulsion Fracture of Calcaneus in Diabetic Patients
- Sung Jin Park, Nam Yong Choi, In Tak Chu, Suk Ku Han, Ki Ho Nah, Hyun Seok Song, Jung Ho Kim
- J Korean Fract Soc 2004;17(2):173-176. Published online April 30, 2004
- DOI: https://doi.org/10.12671/jkfs.2004.17.2.173
-
Abstract
PDF
- Avulsion fracture of the calcaneal tuberosity is an uncommon injury. Usually it occurs from indirect trauma, and can be seen in old patients with osteoporosis or in patients with diabetic neuropathy. Follow-up studies showed fracture healing in most cases, but skeletal deformity may develop in some cases. Therefore we should do plain X-ray evaluations in diabetic patients with foot and ankle pain, even though there have been no definite trauma history. Four cases of calcaneus avulsion fracture were treated operatively in diabetic patients, and reported.
-
Citations
Citations to this article as recorded by- Avulsion Fracture of Calcaneal Apophysis in an Adolescent Gymnast : A Case Report
Youn Moo Heo, Whan Young Chung, Sang Bum Kim, Cheol Yong Park, Jin Woong Yi
Journal of the Korean Fracture Society.2009; 22(4): 288. CrossRef
- Avulsion Fracture of Calcaneal Apophysis in an Adolescent Gymnast : A Case Report
- 1,077 View
- 8 Download
- 1 Crossref
- Avulsion Fracture of the Calcaneal Tuberosity: 2 Cases Report
- Woo Sik Kim, Kwang Kyun Kim
- J Korean Soc Fract 2002;15(4):455-458. Published online October 31, 2002
- DOI: https://doi.org/10.12671/jksf.2002.15.4.455
-
Abstract
PDF
- Fractures of the calcaneus have received much attention because a large number involve the subtalar joint. Avulsion fracture of the tuberosity of the calcaneus is rare injury, and it is reported that the avulsion of the calcaneal tuberosity accounted for less than 1 % of these injuries. We have experienced two cases of avulsion of the calcaneal tuberosity and report these cases.
- 680 View
- 2 Download
Case Reports
- Atraumatic Avulsion Fracture of Calcaneal Tuberosity in a Patient with Peripheral Neuropathy: A Case Report
- Woo Chun Lee, Ki Heon Nam
- J Korean Soc Fract 2001;14(1):85-90. Published online January 31, 2001
- DOI: https://doi.org/10.12671/jksf.2001.14.1.85
-
Abstract
PDF
- Atraumatic calcaneal fractures associated with neurological abnormalities have been reported by several authors, and most of them are associated with diabetes. Chronic alcoholism is also a cause of neurological abnormality and neuropathic arthropathies associated with chronic alcoholism were reported. However we could not find any report of atraumatic calcaneal avulsion fracture associated with chronic alcoholism. We have treated a calcaneal avulsion fracture in a chronic alcoholic patient with open reduction and internal fixation, and the result was not satisfactory. We suggest that conservative treatment is better for the atraumatic calcaneal avulsion fracture in a chronic alcoholic patient with severe osteoporosis and neurological abnormalities.
- 2,671 View
- 0 Download
- Isolated Avulsion Fracture of the Superior Border of the Scapula: A Case Report
- Suk Woong Yoon, Sang Deog Kim
- J Korean Soc Fract 2000;13(4):948-951. Published online October 31, 2000
- DOI: https://doi.org/10.12671/jksf.2000.13.4.948
-
Abstract
PDF
- Avulsion fracture of the scapula by the indirect trauma, especially avulsion fracture of isolated superior border is very rare. We experienced a case of isolated avulsion fracture of the superior border of the scapula and report the clinical and radiographic findings in detail.
- 597 View
- 1 Download
Original Articles
- Avulsion Fracture of The Medial Meniscus: A Case Report
- Hyoung Soo Kim, Seung Rim Park, Joon Soon Kang, Woo Hyeong Lee, Kil Seok Ko
- J Korean Soc Fract 2000;13(1):109-112. Published online January 31, 2000
- DOI: https://doi.org/10.12671/jksf.2000.13.1.109
-
Abstract
PDF
- Post-traumatic meniscal ossicle due to avulsion fracture of medial meniscus was very rare. They were often associated with meniscal tear, but caused symptoms without a tear, by mass effect from protruding meniscal contour. so it had to be differential diagnosised with free loose body in the knee joint. We experienced a symptomatic meniscal ossicle due to post-traumatic avulsion fracture of the posterior horn of medial meniscus, and managed with open reduction, internal fixation with screw and washer after arthroscopic examination. We report a rare case of meniscal ossicle in detail with literature
- 686 View
- 0 Download
- Operative Treatment of Avulsion Fractures of the Calcaneal Tuberosity
- Ik Su Choi, Woo Il Kim, Hong Ju Ha, Jin Goo Kang, Seung Chan Ko
- J Korean Soc Fract 1999;12(4):968-974. Published online October 31, 1999
- DOI: https://doi.org/10.12671/jksf.1999.12.4.968
-
Abstract
PDF
- Avulsion fractures of the calcaneal tuberosity are rare injuries in extraarticular fractures of the calcaneus and were resulted from a separation of a shell of the posterior portion of the os calcis due to the pull of the Achilles tendon. Importance of anatomic reduction for the restoration of functional length of Achilles tendon were emphasized by many authors in the treatment of the fractures. The purpose of this study is to evaluate the results of operative treatment in avulsion fractures of the calcaneal tuberosity and to analyse the results in accordance with various prognostic factors. This article has reviewed a series of 6 avulsion fractures of calcaneal tuberosity, treated from March 1991 to November 1996. The results were as follows ; 1. In case of avulsion fracture of os calcaneus, open reduction and internal fixation was needed for the accurate anatomical reduction and maintenance of firm internal fixation. 2. The method of operative treatment was not significant influencing factor on the treatment result, however, it is more convenient to fix when cannulated screws were used because of the compressive effect on the fracture site. 3. Complications included superficial skin necrosis in one case, which resulted from the compression of bony fragment in case of avulsion fracture and another, wire fixation failure because of bone resorption resulted from wide soft tissue dissection.
- 670 View
- 7 Download
- Treatment of Avulsion Fracture of posterior Cruciate Ligament from Tibial Attachment: Retrospective Study
- Moon Jib Yoo, Suk Joo Lyu, Kwang Ho Jin, Myung Ho Kim
- J Korean Soc Fract 1999;12(3):607-613. Published online July 31, 1999
- DOI: https://doi.org/10.12671/jksf.1999.12.3.607
-
Abstract
PDF
- PURPOSE
If PCL injury is not treated properly, it may result in progressive instability and functional disability, ultimately degenerative changes of the knee joint. So, we classified fracture type according to extent of displacement and comminution. We will investigate the result and prognosis of operative treatment, and fracture type, associated injuries, and fixation device affect the result. Finally we will ascertain the effectiveness of MRI. MATERIAL AND METHODS: 15 patients were treated in our hospital during the period september 1995 to july 1998. All of them were male. 14 of the 15 patients were treated operatively and 1 patient conservatively. The follow-up period after operative treatment varied from 9 to 30 months.
RESULTS
The roentgenograms showed union in all patients. There was subjective satisfaction in 11 of 15 patients. According to the measurement using objective device(KT-2000), in 12 patients, posterior displacement of tibia was less than 2mm, and in 3 patients, less than 4mm. According to Lysholm and Gillquist scoring scale, 11 patients were excellent, 3 patients were good, and 1 patient was fair. The fracture type and fixation device exerts no effect on the results, while associated injury around the knee joint had significant effect on the results.
CONCLUSION
Firstly, In avulsion fracture of PCL from tibial attachment, we were able to obtain satisfactory result by operative treatment using the small curvilinear posterior incision. Secondly, By using MRI, we were able to classify the fracture type more exactly and also find associated soft tissue injuries on the traumatized knee joint. As a result, MRI was quite helpful in determining the treatment and prospection of prognosis. Thirdly, The type of device had no effects on the results, no need of removal of fixation devices. Finally, Fixation was made possible by small curvilinear skin incision.
- 804 View
- 0 Download
Case Report
- Osteochondral Avulsion Fracture in Patella after Treatment of Abscess around Knee: A Case report
- Keun Soo Lee, Geon Woo Lee, Sang Ho Song, Hyun Seo
- J Korean Soc Fract 1999;12(2):290-293. Published online April 30, 1999
- DOI: https://doi.org/10.12671/jksf.1999.12.2.290
-
Abstract
PDF
- Osteochondral avulsion fracture of patella has been rarely reported. We experienced one case of osteochondral avulsion fracture which was developed after abscess around knee. The patient was a 16year old with the history of abscess. The presenting symptom was knee pain and loss of extension power. Radiologic and operative findings suggested that osteochondral avulsion fracture of the patella, was caused by minor trauma near the insertion site of quadriceps tendon. In usual case of quadriceps tendon rupture, the rupture occurred at the musculotendinous junction, caused by sudden contracture of the muscle without trauma history. This case was treated successfully with tension band wiring technique. Differential diagnosis between osteochondral avulsion fracture and osteomyelitis of patella was emphasized.
- 641 View
- 0 Download
Original Articles
- Compartment Syndrome Complicating Avulsion Fractures of the Tibial Tubercle
- Yerl Bo Sung, Jin Hyok Kim, Hyung Jin Chung, Dong Soo Kim, Byung Hyun Jung, Jong Guk Ahn, Chil Soo Kwon, Kook Jin Chung, Bong Gyun Kang
- J Korean Soc Fract 1999;12(2):284-289. Published online April 30, 1999
- DOI: https://doi.org/10.12671/jksf.1999.12.2.284
-
Abstract
PDF
- Avulsion of the tibial tubercle is an uncommon physeal injury. Complications from this fracture have rarely been reported and seldom affect the long-term outcome. Three adolescent boys who sustained avulsion fracture of the tibial tubercle, were complicated by compartment syndrome and treated at Inje University Sang-Gye Paik Hospital from September 1989 to February 1995. Injury to the soft tissue surrounding the tibial tubercle avulsion may be more extensive than is usually appreciated. The anatomy of the proximal tibia and the tibial tubercle with nearby branches of the anterior tibial recurrent artery suggest a predisposing factor for the development of compartment syndrome. So, compartment syndrome should be added to the list of possible complications of this type of fracture.
- 698 View
- 2 Download
- Treatment of the Avulsion Injury of the Posterior Cruciate Ligament
- Dong Wha Lee, Kyoo Seog Shin, Jong Soon Kim, Jin Jwan Seo
- J Korean Soc Fract 1998;11(3):718-723. Published online July 31, 1998
- DOI: https://doi.org/10.12671/jksf.1998.11.3.718
-
Abstract
PDF
- The posterior cruciate ligament (PCL) plays an integral role in stabilizing the knee joint as a main restraint to posterior displacement of the tibia. When the tibial insertion of the PCL is avulsed, the knee becomes unstable, so that rotational instability, meniscus injury and degenerative change may develop within several years. Therefore early repair is necessary. The purpose of this report is to evaluate the usefullness of the direct posterior approach to the avulsion site of PCL. We treated 8 isolated avulsion injury of the PCL from January 1995 to May 1997 through the way of using the Burks and Schaffer's simplified posterior approach. The results were as follows; 1. The stability was achieved with screw fixation. and the outcome was above good in 87.5% of cases. 2. The Burks and Schaffer's simplified posterior approach ws concerned as an useful one for the fixation of an avulsion fragment of PCL. 3. The patients returned daily living within 3 months after operation.
-
Citations
Citations to this article as recorded by- Bilateral PCL Avulsion Fracture from Tibial Attatchment Site in a 16-years-old Male: A Case Report
Hee-Gon Park
Journal of the Korean Fracture Society.2009; 22(3): 189. CrossRef
- Bilateral PCL Avulsion Fracture from Tibial Attatchment Site in a 16-years-old Male: A Case Report
- 1,077 View
- 1 Download
- 1 Crossref
Case Report
- Avulsion Fractures of the Tibial Tuberosity: Three Cases Reports
- Ho Jung Kang, Koon Soon Kang, Jun Seop Jahng, Young June Park
- J Korean Soc Fract 1992;5(2):372-377. Published online November 30, 1992
- DOI: https://doi.org/10.12671/jksf.1992.5.2.372
-
Abstract
PDF
- The talus is a important bone because it supports and distributes the body forces above it. Avulslon Fractures of the tibial tubercle prior to epiphyseal closure are uncommon. Fractures that are seen most frequently in adolescents. Watson-Jones classified these injuries into three types. The authors treated three cases of the tuberosity fractures. Two adolescent boys were treated with open reduction and screw fixation and K-wire fixation. One adult man was treated with open reduction and circumferential wire fixation. The Osgood-schlatter disease was diagnosed in two patients. There were small flecks of calcification 3 to 4cm proximal to the tubercle in the two adolescent cases. Functional motion was started within six weaks after operation. No early complications occurred, and no later defermities. such as genu recurvatum as reported by Blount, were detected. All patients returned to normal activity in one year after an operation.
- 764 View
- 0 Download
 First
First Prev
Prev

