 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 35(2); 2022 > Article
- Case Report Isolated Avulsion Fracture of the Subscapularis from the Lesser Tuberosity of the Humerus in a 12-Year-Old Boy - A Case Report -
- Shin Seung Park, Chung Shik Shin, Won Bin Song
-
Journal of Musculoskeletal Trauma 2022;35(2):68-73.
DOI: https://doi.org/10.12671/jkfs.2022.35.2.68
Published online: April 30, 2022
Department of Orthopedic Surgery, Presbyterian Medical Center, Jeonju, Korea
- 627 Views
- 4 Download
- 0 Crossref
- 0 Scopus
Abstract
An isolated avulsion fracture of the subscapularis from the lesser tuberosity of the proximal humerus is rare in the pediatric population and only a couple of cases have been described in literature. A 12-yearold right-handed boy, was admitted to the hospital with left shoulder pain after falling down the previ-ous day. Physical examination revealed tenderness on the lesser tuberosity and intertubercular groove of the humerus and a limited range of motion. Ultrasonography, computed tomography, and magnetic resonance imaging showed an isolated avulsion fracture of the subscapularis tendon from the lesser tuberosity of the humerus, accompanied by medial subluxation of the long head of the biceps tendon. In this case, a subscapularis avulsion fracture which is rare in this age group was detected at an early stage, and surgical treatment resulted in positive outcomes. Subscapularis avulsion fractures in children are difficult to diagnose in the early stages, and if not treated on time, the symptomatic improvement may be delayed. Timely and accurate diagnosis and treatment can help faster return to normal activi-ties. We would therefore like to report this case with a literature review.
J Korean Fract Soc. 2022 Apr;35(2):68-73. Korean.
Published online Apr 25, 2022.
https://doi.org/10.12671/jkfs.2022.35.2.68
Published online Apr 25, 2022.
https://doi.org/10.12671/jkfs.2022.35.2.68
Copyright © 2022 The Korean Fracture Society.
Case Report
12세 남아에서 상완골 소결절 견갑하건 부착부의 견열성 골절: 증례 보고

Isolated Avulsion Fracture of the Subscapularis from the Lesser Tuberosity of the Humerus in a 12-Year-Old Boy: A Case Report
초록
소아에서 상완골 소결절의 단독 견열 골절은 매우 드물며 문헌상에서 몇 가지 사례만 보고되고 있어 증례에 대하여 보고하고자 한다. 오른손잡이인 12세 소년이 내원 하루 전 운동하다가 넘어진 후 발생한 좌측 어깨 통증으로 내원했고 시행한 이학적 검사상 소결절 부위 및 결절간구 쪽에 압통이 있었으며, 운동 범위는 내회전 S1, 저항성 내회전 강도가 감소된 소견을 보였다. 추가적으로 belly press test와 lift-off test, bear hug test에서 양성 소견을 보였으며, Yergason test와 speed test에서도 양성 소견을 보였다. 초음파, CT 및 MRI상에서 상완골 소결절의 견열 골절 및 상완 이두장건의 내측 아탈구가 관찰되어 수술적 치료를 시행하였다. 이 연령대에서 드문 외상성 견갑하건 부착 부위의 소결절의 견열 골절을 조기에 발견하여 수술적 치료를 통하여 좋은 결과를 얻었다. 소아에서 견갑하건 견열 골절은 초기 진단이 어렵고 치료를 하지 않았을 시에 증상 개선이 되지 않아 정확한 진단과 치료가 필요하여 이에 대해 문헌 고찰과 함께 보고하고자 한다.
Abstract
An isolated avulsion fracture of the subscapularis from the lesser tuberosity of the proximal humerus is rare in the pediatric population and only a couple of cases have been described in literature. A 12-year-old right-handed boy, was admitted to the hospital with left shoulder pain after falling down the previous day. Physical examination revealed tenderness on the lesser tuberosity and intertubercular groove of the humerus and a limited range of motion. Ultrasonography, computed tomography, and magnetic resonance imaging showed an isolated avulsion fracture of the subscapularis tendon from the lesser tuberosity of the humerus, accompanied by medial subluxation of the long head of the biceps tendon. In this case, a subscapularis avulsion fracture which is rare in this age group was detected at an early stage, and surgical treatment resulted in positive outcomes. Subscapularis avulsion fractures in children are difficult to diagnose in the early stages, and if not treated on time, the symptomatic improvement may be delayed. Timely and accurate diagnosis and treatment can help faster return to normal activities. We would therefore like to report this case with a literature review.
Keywords
Subscapularis, Lesser tubercle, Avulsion fracture
견갑하건, 소결절, 견열골절
소아에서 발생한 상완골 소결절의 단독 견열 골절은 매우 드물게 발생하며, 문헌에도 몇 가지 사례만 보고되었다. 이에 저자들은 12세 남아에서 발생한 좌측 어깨의 상완골 소결절의 단독 견열 골절 사례에 대하여 보고하고자 한다.
증례 보고
12세 남아로 내원 하루 전에 운동하다가 넘어진 후에 발생한 좌측 어깨 통증으로 본원 외래로 내원하였다. 외래에서 시행한 이학적 검사상 좌측 어깨 소결절 부위 및 결절간구 쪽에 압통이 있었으며, 운동 범위는 굴곡 80°, 신전 60°, 외전 70°, 내전 60°, 외회전 60°, 내회전 S1 수준으로 내회전이 감소되었으며 저항성 내회전 근력이 감소된 소견을 보였다. 추가적으로 belly press test에서 양성, lift off test에서 양성, bear hug test에서 양성 소견을 보였고(Fig. 1) Yergason test와 speed test에서도 양성 소견을 보였다. X-ray상에서는 특이소견을 보이지 않았으나(Fig. 2A), 내원 당일 외래에서 시행한 초음파 검사상 견갑하건 견열 골절 및 상완 이두장건의 내측 아탈구가 관찰되었다(Fig. 2B).
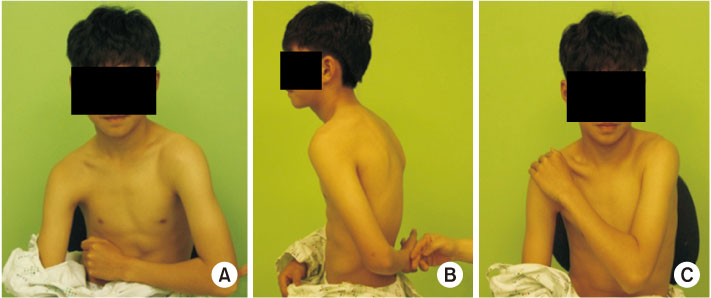
Fig. 1
Preoperative physical exam, belly press test (A), lift off test (B), bear hug sign (C).
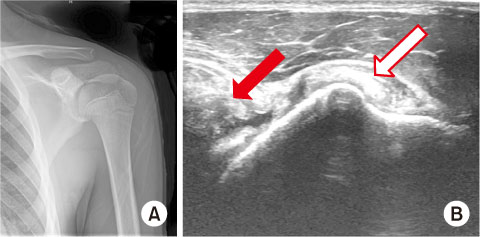
Fig. 2
(A) Preoperative radiograph shows no abnormal findings. (B) The long axis of the ultrasound image shows a bone fragment of the avulsion fracture of lesser tuberosity (red arrow) and subluxation of long head of the biceps tendon (white arrow).
컴퓨터 단층촬영(computed tomography, CT)상에서는 소결절 부위에서 떨어진 골편이 관찰되었고(Fig. 3A), 자기공명영상(magnetic resonance imaging, MRI)상에서 소결절의 골편 및 상완 이두장건의 내측 아탈구가 관찰되었다(Fig. 3B).
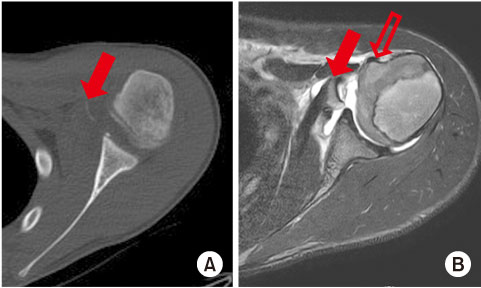
Fig. 3
(A) Preoperative computed tomography shows an avulsion fracture of the lesser tuberosity (arrow). (B) T2-weighted axial magnetic resonance imaging shows an avulsion fracture of the lesser tuberosity (arrow) and subluxation of the long head of the biceps tendon (open arrow).
수상 후 7일째 수술을 시행하였고, 환자를 전신마취 후 해변위자세로 환자를 위치시킨 후에 진단적 관절경을 통해 관절 내 구조물을 관찰하였다. 관절경상에서 견갑하건 부착 부위의 소결절의 견열 골절 및 상완 이두장건은 활차의 파열로 인한 내측 아탈구가 관찰되었다(Fig. 4). 견봉의 전외측에 절개를 가한 후에 삼각근의 전방과 중간 부위를 결에 따라 벌려서 견갑하건에 부착된 상태의 견열된 골편을 확인하고 원 위치에 정복후 교량형 봉합술을 이용하여 고정하였고, 부분 파열된 상완 이두장건 활차에 대해서는 주변 조직과 함께 봉합술을 시행하여 상완 이두장건 아탈구를 방지하였다(Fig. 5). 창상 봉합 후 관절경을 통하여 견갑하건 견열 골편의 정복을 확인하였다.
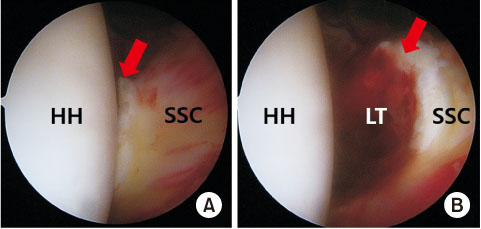
Fig. 4
Intra-articular arthroscopic image of an avulsion fracture of the lesser tubercle. (A) Reduced lesser tuberosity (arrow). (B) Displaced lesser tuberosity (arrow). HH: humeral head, SSC: subscapularis tendon, LT: lesser tuberosity.
Fig. 5
Bone fracture fragment of lesser tuberosity was fixed using the suture bridge technique. (A) Front view. (B) Top view.
환자는 수술 후에 6주간 견관절 외전 보조기를 이용해 고정하였고, 수술 후 2주째부터 수동적 운동을 시작하였다. 수술 후 5주째 X-ray 및 CT상에서 소결절 견열 골편의 전위는 관찰되지 않았으며, 골유합이 진행되고 있음을 관찰하였다(Fig. 6). 수술 후 8개월째 환자는 증상을 호소하지 않았고, 관절운동 범위와 근력은 반대측과 비교하였을 때 정상으로 관찰되었다(Fig. 7).
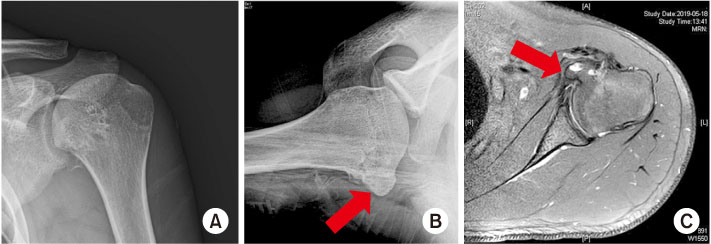
Fig. 6
X-ray (A, B) and magnetic resonance imaging (C) 4 years after the operation showed hypertrophied lesser tuberosity (arrows).
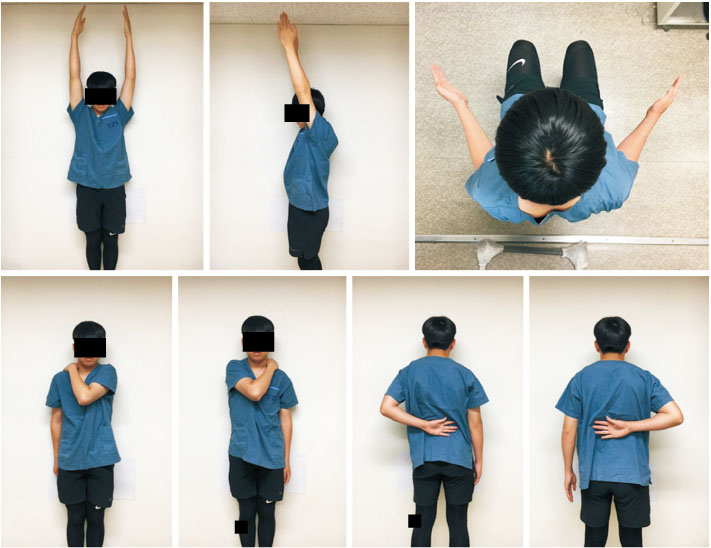
Fig. 7
Postoperative active range of motion at 4 years after operation shows normal range of motion.
고찰
상완과 근위부 골절이나 견관절의 후방 탈구 등을 동반하지 않은 상완골 소결절의 견열 골절은 국내외 문헌 연구에서 매우 드물게 보고되고 있다.
상완골 소결절의 견열 골절은 주로 젊은 연령대에서 발생하며,1) 주로 스포츠 손상으로 발생한 경우가 대부분이다. 소아에서는 성인과 달리 견갑하건의 손상보다 견열 골절이 많이 발생하는 것으로 보고되고 있다.2)
이는 Kocher 등3)에 의하면 소아에서는 견갑하건과 소결절은 하나의 기능적 단위로 생각되어야 한다고 주장한 것으로 설명할 수 있을 것이다.
상완골 소결절의 골화중심은 약 5세경 시작하여 대결절과 유합이 되며, 약 7세경에 상완골 두 골화중심과 유합이 된다. 따라서 소결절 골단은 청소년기에 잘 유합이 되어있다. 상완골 간부와 상완골두 간의 유합은 약 19세경에 이루어진다. 이런 과정은 청소년기 상완골 소결절의 견열 골절은 성장판에서 생기는 것이 아님을 의미한다.
상완골 소결절의 단독 견열 골절 진단을 위해서는 우선 손상 기전을 확인하는 것이 중요하다. 일반적으로 상완부가 외전된 상태에서 갑자기 외회전력이 가해지면서 견갑하근의 견열로 인해 발생한다.4)
환자가 최초 호소하는 증상으로는 견관절부 통증과 함께 수동적 및 능동적 관절 운동 시 심해지는 통증이 있다.
이학적 검사 방법으로 견갑하건의 기능과 강도를 평가하는 ‘lift off test’ 또는 ‘belly press test’ 및 ‘bear hug test’와 같은 특별한 검사 방법이 중요하다. Lift off test는 견갑하건의 약화나 파열을 평가하기 위해 시행한다. 환자는 팔을 등하부 뒤쪽에 놓고 검사자의 손에 저항하여 몸으로부터 팔을 떨어뜨린다. 환자가 검사자의 손으로부터 팔을 밀어내지 못하면 파열이 있는 양성으로 진단한다. Belly press test는 운동 범위가 감소하여 lift off test를 시행하지 못할 때에 견갑하건을 평가하기 위해 사용한다. 팔꿈치를 구부려 손바닥을 배에 위치시킨 후 팔꿈치의 움직임 없이 배를 눌렀을 때, 그 상태를 유지하지 못하면 양성으로 진단한다. Bear hug test는 검사를 시행할 방향의 손바닥을 팔꿈치와 함께 반대편 어깨에 위치시킨다. 환자는 이 자세로 내회전을 유지하며, 검사자가 팔을 외회전시키는 힘을 가한다. 이때 반대편과 비교했을 때 힘이 떨어지면 양성으로 진단한다.
진단 방법으로 단순 방사선 검사상 골편이 크다면 전후면 사진에서도 잘 관찰할 수 있지만, 골편이 작거나 전위가 적다면 액와면 사진을 통해서 진단 가능하다.
Sugalski 등5)은 액와면 사진에서 소결절 골편이 잘 관찰되므로 모든 어깨 외상 후 방사선 검사에서 액와면 사진을 포함하여야 한다고 주장하였다.
저자들도 이 환자의 경우 액와면 사진을 촬영하려고 하였지만 환자 통증으로 인한 자세 협조가 되지 않은 문제로 액와면 사진은 촬영하지 못하였으며, 이로 인하여 단순 방사선 사진에서는 진단을 하지 못하였다.
영상학적 검사 방법 중 초음파는 외래 진료실에서 손쉽게 사용할 수 있고 방사선 조사 없이 다양한 구조물을 관찰할 수 있는 장점이 있는 반면 술자의 술기에 의해 영향을 많이 받는 단점이 있는 진단 방법 중 하나이며, MRI는 소결절의 견열 골절이나 근육의 완전 파열이 의심될 때 초기에 시행할 수 있다. 다른 진단도 고려되어야 하는데, 극상근의 부분 또는 완전한 파열, 전방 어깨 아탈구 또는 탈구, 대흉근 또는 소흉근의 파열, 관절와순 파열 또는 관절낭 파열 등을 MRI 관절조영술로 구분할 수 있다. 상완 이두장건의 내측 아탈구는 견갑하건 파열의 특징적인 징후로 보고되었다.6)
치료 방법으로, 지금까지 보고된 논문들에 의하면 수술적 치료를 시행 후 좋은 결과를 얻었다는 의견이 대부분이지만 수술적 치료와 보존적 치료를 비교한 논문은 없었다.
관절경적 수술 및 개방적 수술의 결과는 유사한 것으로 보고되고 있다.
전위가 없거나 내회전력의 감소가 없는 등의 증상이 경한 견열 골절인 경우 휴식 및 관절 가동 범위 제한 등의 보존적 치료를 통해서 좋은 결과를 얻었다는 연구도 있지만,7) 진단이 지연되었거나 전위가 있는 경우, 해부학적 정복이 되지 않는 경우에 부정 유합, 이소성 골화 및 견갑하건 근력의 약화 등을 야기할 수 있기 때문에 수술적 치료가 필요한 것으로 알려져 있다.8)
소아에서 발생한 견갑하건의 견열 골절인 경우 단순 방사선 촬영에서 골편이 발견되는 경우도 있지만,2,4,8) 발견이 되지 않는 경우도 보고되고 있어 자세한 병력 청취를 통하여 견갑하건의 견열 골절이 의심된다면 MRI를 반드시 시행할 필요가 있다(Table 1).9,10)
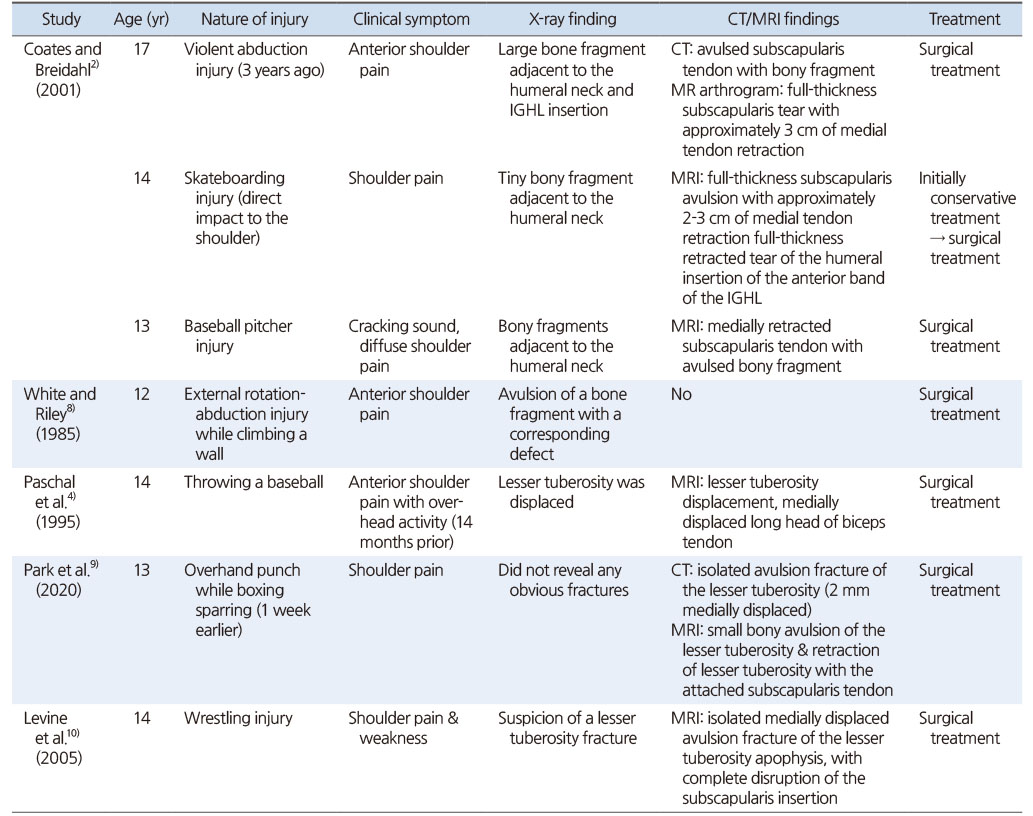
Table 1
Case Report of Subscapularis Avulsion Fracture in Padiatric
수술적 치료에 대한 명확한 적응증은 정해져 있지 않지만 환자가 지속적인 통증을 호소하고, 신체검사에서 견갑하건의 근력저하가 동반되어 있고, MRI에서 골편의 전위가 확인이 되는 경우에는 보존적 치료보다는 수술적 치료가 좋은 결과를 기대할 수 있을 것으로 보인다.2,4,9,10)
저자들의 경우 환자의 내회전력의 감소가 있었고 초음파 검사 및 MRI 검사에서 골절편의 전위가 확인되어 수술적 치료를 결정하고 시행하였다.
결론적으로, 소아에서 견갑하건 견열 골절은 초기 진단이 어렵고 치료를 하지 않았을 시에 증상 개선이 되지 않아 정확한 진단과 치료가 필요하여 저자들은 이에 대해 문헌 고찰과 함께 보고하고자 한다.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Scheibel M, Martinek V, Imhoff AB. Arthroscopic reconstruction of an isolated avulsion fracture of the lesser tuberosity. Arthroscopy 2005;21:487–494.
-
-
Coates MH, Breidahl W. Humeral avulsion of the anterior band of the inferior glenohumeral ligament with associated subscapularis bony avulsion in skeletally immature patients. Skeletal Radiol 2001;30:661–666.
-
-
Kocher MS, Waters PM, Micheli LJ. Upper extremity injuries in the paediatric athlete. Sports Med 2000;30:117–135.
-
-
Paschal SO, Hutton KS, Weatherall PT. Isolated avulsion fracture of the lesser tuberosity of the humerus in adolescents. A report of two cases. J Bone Joint Surg Am 1995;77:1427–1430.
-
-
Sugalski MT, Hyman JE, Ahmad CS. Avulsion fracture of the lesser tuberosity in an adolescent baseball pitcher: a case report. Am J Sports Med 2004;32:793–796.
-
-
Clark RJ, Marchessault J, Sizer PS Jr, Slauterbeck J. Isolated traumatic rupture of the subscapularis tendon. J Am Board Fam Pract 2002;15:304–308.
-
-
Robinson CM, Teoh KH, Baker A, Bell L. Fractures of the lesser tuberosity of the humerus. J Bone Joint Surg Am 2009;91:512–520.
-
-
White GM, Riley LH Jr. Isolated avulsion of the subscapularis insertion in a child. A case report. J Bone Joint Surg Am 1985;67:635–636.
-
-
Park SG, Shim BJ, Seok HG. Isolated avulsion fracture of the lesser tuberosity of the humerus in an adolescent amateur boxer. JSES Int 2020;4:759–764.
-
-
Levine B, Pereira D, Rosen J. Avulsion fractures of the lesser tuberosity of the humerus in adolescents: review of the literature and case report. J Orthop Trauma 2005;19:349–352.
-
 Cite
Cite
