 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 37(4); 2024 > Article
-
Original Article
- Does the Operator’s Experience Affect the Occurrence of Complications after Distal Radius Fracture Volar Locking Plate Fixation? A Comparative Study of the First Four Years and Thereafter
-
Kee-Bum Hong, M.D.*,†
 , Chi-Hoon Oh, M.D., Ph.D.‡, Chae Kwang Lim, M.D.*,†, Sungwoo Lee, M.D.*,†, Soo-Hong Han, M.D., Ph.D.‡, Jun-Ku Lee, M.D., Ph.D.*,†
, Chi-Hoon Oh, M.D., Ph.D.‡, Chae Kwang Lim, M.D.*,†, Sungwoo Lee, M.D.*,†, Soo-Hong Han, M.D., Ph.D.‡, Jun-Ku Lee, M.D., Ph.D.*,† -
Journal of Musculoskeletal Trauma 2024;37(4):175-183.
DOI: https://doi.org/10.12671/jmt.2024.37.4.175
Published online: October 25, 2024
*Department of Orthopedic Surgery, National Health Insurance Service Ilsan Hospital, Goyang, Korea
†Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea
‡Department of Orthopedic Surgery, CHA Bundang Medical Center, Seongnam, Korea
- Correspondence to: Jun-Ku Lee, M.D., Ph.D. Department of Orthopedic Surgery, National Health Insurance Service Ilsan Hospital, 100 Ilsan-ro, Ilsandong-gu, Goyang 10444, Korea Tel: +82-31-900-0340 Fax: +82-31-900-0343 E-mail: jg197@naver.com
- Chi-Hoon Oh’s current affiliation: Department of Orthopedic Surgery, Korea University Ansan Hospital, Ansan, Korea
• Received: May 1, 2024 • Revised: July 1, 2024 • Accepted: September 2, 2024
© 2024 The Korean Fracture Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,567 Views
- 57 Download
- 3 Crossref
This article has been corrected. See "Author correction: “Does the operator's experience affect the occurrence of complications after distal radius fracture volar locking plate fixation? A comparative study of the first four years and thereafter”" in Volume 38 on page 40.
Abstract
-
Purpose The management of distal radius fractures (DRFs) has evolved with the introduction of volar locking plate (VLP) fixation, offering stable fixation and better outcomes. Nevertheless, the impact of the surgeon’s experience on the complication rates in VLP fixation remains to be determined, particularly for less-experienced surgeons. This study compared the complication rates during the initial four years and subsequent two years of a hand surgeon’s practice of VLP fixation for DRFs.
-
Materials and Methods The data between March 2016 and December 2022 were analyzed retrospectively under the Institutional Review Board approval. A single surgeon performed all VLP fixation surgeries after finishing regular hand surgery training, with the first four years representing the less experienced phase (Group 1) and the following two years indicating the experienced phase (Group 2). The patients’ characteristics, operation-related factors, and postoperative complications, including tendon injuries, nerve-related complications, fixation and instrument-related issues, osteosynthesis-related problems, and infections, were compared. In addition, the authors compared the data with a large multicenter study conducted by experienced hand surgeons.
-
Results Three hundred and nineteen patients (321 wrists) were included. The mean age was 63.3 years, and 26.3% were male and 73.7% were female. The operation time was 53.7±14.5 minutes and 74.4±26.5 minutes in groups 1 and 2, respectively, which was statistically significantly shorter (p<0.001). The complication rates between the two groups were similar, except for the higher implant removal rates in Group 1. A comparison with a previous multicenter study revealed higher reduction losses and carpal tunnel syndrome in this study, but the overall complication rate was low.
-
Conclusion In DRF management, when the operating surgeon has completed an accredited training course, VLP fixation is a good treatment method that can be performed effectively even by less experienced surgeons with low complication rates.
Introduction
Distal radius fractures (DRF) are very common, accounting for about one-sixth of all upper extremity fractures.1) Various treatment options are available, including closed reduction followed by percutaneous pinning, external fixation, and open reduction followed by dorsal or volar plate fixation. Despite the range of choices, the predominant approach remains conservative treatment such as immobilization with or without closed reduction.
Since the introduction of volar locking plate (VLP) fixation in the early 2000s, there has been a notable shift toward operative treatments.2,3) With the increased adoption of VLP fixation, there has naturally been an evolution in associated complications. These can range from errors during surgical exposure, hardware-related errors, flexor and extensor tendon complications, inadequate reduction and internal fixation.4) Nevertheless, in a large-scale multicenter study, the incidence of complications was reported to be very low, establishing VLP fixation as a safe and major treatment method for DRFs.5) However, most studies reporting complications after VLP were performed by experienced and expert surgeons, whose outcomes might not necessarily reflect those of less experienced practitioners.
This brings up the question: What happens when a novice hand surgeon undertakes VLP fixation for DRFs after completing a training course? What are the complication rates under these circumstances? To detail this, we undertook a comparison of surgical complication rates during the first four years and the subsequent two years after a surgeon starts operating independently. Second, we compared and analyzed the overall complications in this study with those reported in a large multicenter study involving five experienced hand surgeons.
Materials and Methods
This retrospective study was conducted between March 2016 and December 2022 at National Health Insurance Service Ilsan Hospital and Inje University Seoul Paik Hospital and was approved by the local institutional review boards (IRBs) of the two hospitals where the surgeries were conducted (IRB Nos. PAIK 2023-01-003, NHIMC 2023-01-005).
All surgical interventions for DRFs were performed by a single hand surgeon using the modified volar Henry approach between the flexor carpi radialis and brachioradialis with the radial artery.
The surgeon completed formal orthopedic training for four years, eventually becoming an orthopedic specialist. From May 2016 to February 2017, the surgeon undertook a fellowship under a hand surgery expert at a university hospital. The first independent DRF operation with VLP fixation was carried out in March 2016. Until February 2021, the surgeon worked at a university hospital as a ‘specialist – less experience’, based on reported levels of experience.6) In March 2021, he transitioned to a general hospital and continued his career as a hand surgeon. Since then, he has been classified as a ‘specialist – experienced’.6)
To ensure meticulous data collection, two separate orthopedic surgeons and an orthopedic nurse were engaged in the data survey process. Finally, the another main author who did not involve operation meticulously reviewed and refined the data collection procedure. During the study period, a total of 344 patients with DRF were treated operatively.
Patients with insufficient information and those lost to follow-up before bony union were identified and contacted via phone surveys. Patients unreachable through this method were excluded. This process yielded 335 surgically treated DRF cases. Additionally, patients under 18 years of age were excluded (n=5). We included only VLP fixation in DRF, excluding other treatment modalities: closed pinning or screw fixation (n=4, 1.2%), external fixation (n=0, 0%), and dorsal plate fixation (n=5, 1.5%). Finally, this study included 319 patients (321 wrists) including two individuals who underwent bilateral surgery.
The study population was divided into two groups based on the time of operation: Group 1, comprising cases within the first four years, and Group 2, covering the subsequent four years until the study’s conclusion. Patient characteristics including age, sex, height, and weight were investigated.
Fracture-related factors, such as the side of the fractured arm and associated distal ulnar fracture, were also investigated. The AO Foundation and Orthopedic Trauma Association (AO/OTA) classification of the DRF was assessed based on plain radiography and computed tomography. Operation-related factors, including the mean interval from injury to surgery, commercial instruments used, operation durations, and postoperative follow-up period, were also scrutinized.
Postoperative follow-up radiographs were analyzed to identify fracture union and potential complications. Medical records were reviewed to determine the incidence of complications during follow-up.
The operating surgeon had previously participated in a multicenter study of on postoperative complications of DRF after VLP fixation, although his cases were not included in the multicenter study due to this then-limited experience.5)
The definition of each complication was based on the determination from the multicenter study.5)
The overall complications were categorized into (1) tendon injury: flexor tendon and extensor tendon injury; (2) nerve-related: median nerve palmar sensory branch damage, complex regional pain syndrome (CRPS), and carpal tunnel syndrome (CTS); (3) fixation and instrument-related reduction loss after VLP fixation, instrument breakage, screw penetration into the radial carpal joint, and reoperation for implant removal; (4) osteosynthesis-related: delayed union or non-union; (5) infection: superficial or deep infection, and (6) others: compartment syndrome, and radial artery injury.7)
The summary statistics are presented as mean±standard deviation or numbers and percentages. Pearson’s chi-square test and Fisher’s exact test were used to compare the categorical variables and Student’s t-test was used for comparison of continuous variables between groups. Before Student’s t-test was performed, a normality test (Shapiro– Wilk test) was performed. A p-value of less than 0.05 was considered statistically significant. With software R (v. 3.1.0; The R Foundation), the statistical evaluation was conducted.
Results
The study population had a mean age of 63.3 years, with a standard deviation of 13.8. Among the participants, 84 were male (26.3%) and 235 were female (73.7%). The age and sex distributions of the study population are depicted in Fig. 1. Fractures were localized to the right wrist in 151 patients (47.0%), and distal ulnar fractures were observed in 212 patients (66.0%). Postoperatively, patients were followed up for a mean of 253 days.
The assessment of inserted plates revealed that the surgeons used products from four different manufacturers. The Deputy Synthes® distal radius system was utilized for 284 wrists (88.5%), followed by APTUS® for 32 wrists (10.0%), and rest minor rates (5 wrists, 1.6%). There was no statistical difference between groups (p=0.161).
There were no significant differences between the two groups in terms of sex, height, or weight. However, in the age comparison, the mean age of 64 years in Group 2 was significantly higher than that of 61 years in Group 1 (Table 1).
When comparing operation-related factors, there were no significant differences between the two groups with regards to the fractured arm, AO/OTA classification, combined ulnar fracture occurrence, or union time. The operative time was significantly shorter in Group 2 (53 minutes) than in Group 1 (74 minutes) (Table 2). The follow-up duration was significantly longer in Group 1 (mean, 292 days) than in Group 2 (mean, 213 days).
Table 3 provides an overview of overall complications and the comparisons between the two groups.
1) Tendon related
A total of seven patients were identified with tendon injuries: two with flexor and five with extensor tendon injuries. Group 1 had one patient with flexor pollicis longus tendon injury, while Group 2 had another such case. Both injuries were categorized as grade 2 according to the Soong classification.8) In Group 1, a patient had flexor tendon irritation during follow-up, confirmed on physical examination, reporting partial rupture intraoperatively during the plate removal at the 4 months after initial operation. In Group 2, a complete rupture prompted plate removal and palmaris longus tendon graft reconstructed at 10 months after surgery.
In terms of extensor tendon injury complications, three patients (1.9%) were noted in Group 1 and two patients (1.2%) were found in Group 2, with no significant statistical difference. One patient noted the extensor tendon irritation due to a long radial screw in the distal row in extensor compartment 2. Rest four patients involved extensor pollicis longus (EPL) rupture and none of the four patients with EPL tendon rupture had a long distal screw protruding over the dorsal cortex; however, it occurred in patients with dorsal fracture fragments around the Lister’s tubercle at the time of DRF fracture.9) Extensor pollicis indicis transfer was performed in two cases, one patient was lost to follow-up, and another declined additional surgery based on age considerations.
2) Nerve related
The palmar sensory branch of the median nerve was injured in three patients: two in Group 1 and one in Group 2. Surgical repair was undertaken in one instance of intraoperative palmar sensory nerve laceration. The remaining two patients presented with transient numbness and tingling sensation along the nerve sensory dermatome, which resolved during follow-up.
Four patients with CRPS noted after surgery, and there were no significant differences between the groups. These patients received active physical therapy and analgesics at a rehabilitation center.
There were no differences in the incidence of CTS and subsequent carpal tunnel release (CTR) after surgery between the groups.
3) Fixation and instrument related
Fracture displacement, even after VLP fixation, was recorded in eight patients in Group 1 and three patients in Group 2, without significant differences. There were ten females and two males averaging 76 years in age. Regarding fracture classification, seven patients had AO/OTA type C3 fractures, followed by C2, and one of C1 type fracture.
Among the above 11 patients, four instances of screw breakage were identified in Group 1. One patient in Group 2 presented with cortical screw loosening without fracture displacement. There were no cases of the distal locking screws violating the radiocarpal joints immediate after operation. However, a total of four patients, three from Group 1 and one from Group 2, had a distal locking screw penetrating the radiocarpal joint due to joint surface collapse. All three Group 1 patients underwent distal screw removal, whereas the remaining patient in Group 2 refused screw removal because of old age and a lack of severe symptoms.
Significantly, Group 1 underwent a higher rate of implant removal as a second operation (42 cases, 26.4%) than Group 2 (18 cases, 11.1%).
4) Osteosynthesis related
Two patients had a dorsal metaphyseal cortex bony defects from the initial trauma that remained incompletely filled with hard callus even 16-week post-plate fixation. Nevertheless, the two patients eventually achieved union without specific interventions. Non-union was not observed after VLP fixation for DRFs.
5) Infection
Among the patients, one in Group 1 and three patients in Group 2 required extended oral antibiotic treatment during outpatient follow-up due to superficial infections. None of the patients required a secondary procedure for deep soft tissue infection.
6) Others
There were no occurrences of compartment syndrome associated with fractures or post-fracture fixation. The modified Henry approach led to radial artery injury in two cases (1.3%), followed by arterial repair under loupe magnification.
When comparing complication rates with a previous retrospective multicenter study,5) certain divergences were noted. The present study showed a higher frequency of CTS incidence and subsequent CTR rates, reduction loss, and implant failure rates. However, plate removal was performed in a small number of cases, and superficial infection rates were lower in our study (Table 4).
Discussion
The authors conducted a comparative analysis of VLP fixation in DRFs over the initial four years as a hand surgeon following formal fellowship training and the subsequent two years, focusing on complication rates. Group 2 demonstrated a notable reduction in operation time (53 minutes) in contrast to Group 1 (74 minutes). Overall, surgical complications were not high, and there was no statistical difference between the two groups except for the rate of plate removal. However, the incidence of reduction in loss, even after VLP fixation, was significantly higher than that reported in a previous large-scale retrospective study.
In 2020, Lee et al.5) analyzed 1,955 cases managed by five hand surgeons at five university hospitals, covering a decade and the largest sample size in such studies. They found VLP fixation to be effective with low complication rates for DRF management. However, three surgeons were experienced specialists, and two were highly experienced, suggesting that inexperienced surgeons may not achieve similar results, highlighting the importance of surgeon experience.6)
As highlighted by Tang,6) assessing the surgical technique of a famous surgeon remains incomplete if the surgeon who performs the technique does not report his level of expertise. Determining whether the outcome is attributed to the surgical technique or skill level of the surgeon can be challenging.10) This emphasizes the importance of the level of expertise. In this context, evaluating the technical advantages of DRF volar plating by comparing novice and experienced surgeons, as per the established level of expertise classification, holds meaningful value.6)
The present study examined VLP fixation in DRFs initiated after an orthopedic residency and 1-year hand fellowship training. The observed complication rates, were comparably low, with slightly higher rates of reduction loss and implant failure complications. The two groups (Group 1, first four years after the operation, and Group 2 thereafter) did not significantly differ in the incidence of most complications except for the implant removal rates. A previous study has reported instrument removal rates ranging from 0% to 100% in previous studies.11) In addition, the removal rate varies depending on the surgeon, institution, and country.11-13)
The reasons for the higher implant removal rates were explained by the fact that more time had passed since Group 1 VLP fixation procedure; conversely, the removal rate for Group 2 could potentially increase over time. Moreover, some patients sought routine removal despite the absence of clinical symptoms. The operating surgeon in this study no longer recommended routine plate removal after bone union, as was partially done from patient’s request in Group 1. Consequently, the recorded removal rates were significantly lower than those reported in the retrospective multicenter study.6)
Operative management principles for DRF prioritize anatomical reduction and stable fixation, fostering early range of motion (ROM) and mitigating complications. Since the introduction of VLP fixation for DRF in the year 2000, this approach has offered advantages such as enhanced stability in fixation and a reduction in complications compared to alternative surgical methods.14-19) As a result, surgical treatment rates have increased and are currently the mainstay of operative management in DRF.20) The precise positioning of a distal locking screw within the subchondral area plays a crucial role in supporting the distal radioulnar joint. Furthermore, it not only sustains fracture alignment but also preserves radial bone length and prevents undesirable dorsal displacement. Finally, VLP fixation enabled early ROM and facilitates functional recovery.21) The operating author pursued early ROM with less than two weeks of immobilization, regardless of age and fracture pattern.22) However, it is worth noting that despite a lack of statistical difference between the two groups, fracture displacement post-VLP fixation was observed in eight patients in Group 1 and three patients in Group 2. The incidence of this complication was significantly higher than that reported in the previous multicenter retrospective study. Subsequently, four cases of screw breakage occurred together, and four cases presented with distal screw secondary radiocarpal joint violation as fracture displacement and articular collapse. It is pertinent to highlight that of the patients with fracture displacement, the majority were female (eight out of ten) and their mean age was 76 years surpassing the overall patient mean age of 63 years. Moreover, all ten patients were of the AO/OTA C type, with C3 type being the most common (six patients). While the operator’s limited experience might have played a role, we believe that the swift joint movement after routine surgery in elderly patients with C-type fractures could clarify the occurrence of displacement even after VLP fixation. Therefore, during Group 2 operations, the surgeon implemented a cautious approach, advocating for a minimum two-week period of splint immobilization, especially for C3 type fractures in the elderly. This strategic adjustment contributed to a reduction in the incidence of such complications when compared to Group 1.
Volar plating for DRF is a surgical technique with good reproducibility and several advantages. However, it is essential not only in terms of experience but also for training in surgical techniques by skilled experts. A study that focused on educating junior surgeons about DRF anterior plating showed that results were superior when these surgeons received personalized training through “deliberate practice,” as opposed to mere repetition of plating or passive viewing of educational videos several times.23) This underscores the crucial role of mentorship and structured training in achieving proficiency.
The surgeon in this study was trained by an expert-level orthopedic surgeon with more than 20 years of surgical experience. The significance of imparting effective teaching in the domain of volar plating for DRF cannot be overlooked.
Our study had several limitations. First, being a retrospective study, it inherently possesses certain drawbacks. Secondly, the operating surgeon performed VLP fixation for groups 1 and 2 while practicing at different hospitals, which could introduce variations. Additionally, we did not report the functional outcomes. Although the incidence of postoperative complications was low, we cannot assert that we achieved the optimal result. Finally, the assessment of complications depends considerably on the surgeon’s subjective inspection and physical examination, including tendon irritation after surgery, delayed union, superficial infection, compartment syndrome, CRPS, and CTS. Hence, debates may arise concerning the accurate determination of these complications.
Conclusion
In DRF management, when the operating surgeon has completed an accredited training course, VLP fixation emerges as a good treatment method that can be effectively performed even by less experienced surgeons, resulting in low complication rates.

Table 1.
Basic Characteristic Comparison between the Groups
| Characteristic | Group 1 (157 patients) | Group 2 (162 patients) | p-value |
|---|---|---|---|
| Sex | 0.422 | ||
| Female | 112 (71.3) | 123 (75.9) | |
| Male | 45 (28.7) | 39 (24.1) | |
| Age (yr) | 61.6±12.6 | 64.8±14.7 | 0.038* |
| Weight (kg) | 61.9±10.9 | 62.1±12.4 | 0.907 |
| Height (m) | 1.6±0.1 | 1.6±0.1 | 0.389 |
| BMI (kg/m2) | 24.5±3.9 | 24.1±3.6 | 0.465 |
Table 2.
Group Comparison of the Fracture Characteristics and Operation-Associated Factors
| Group 1 (159 wrists) | Group 2 (162 wrists) | p-value | |
|---|---|---|---|
| Fractured arm | 0.204 | ||
| Right | 68 (42.8) | 83 (51.2) | |
| Left | 91 (57.2) | 79 (48.8) | |
| AO-OTA classification | 0.133 | ||
| A2 | 24 (15.1) | 12 (7.4) | |
| A3 | 21 (13.2) | 26 (16.0) | |
| B2 | 6 (3.8) | 3 (1.9) | |
| B3 | 10 (6.3) | 12 (7.4) | |
| C1 | 26 (16.4) | 24 (14.8) | |
| C2 | 35 (22.0) | 53 (32.7) | |
| C3 | 37 (23.3) | 32 (19.8) | |
| Ulnar fracture combined | 0.904 | ||
| None | 55 (34.6) | 54 (33.3) | |
| Yes | 104 (65.4) | 108 (66.7) | |
| Preoperative duration (d) | 3.9±5.4 | 5.2±10.8 | 0.169 |
| Operation time (min) | 74.4±26.5 | 53.7±14.5 | <0.001* |
| Union time (d) | 53.5±25.7 | 53.5±23.6 | 0.988 |
| Total follow-up duration (d) | 292.6±240.9 | 213.3±146.0 | <0.001* |
Table 3.
Comparison of the Complication between the Groups
| Complication | Group 1 (159 wrists) | Group 2 (162 wrists) | p-value | |
|---|---|---|---|---|
| Tendon injury | Tendon rupture | 4 (2.5) | 3 (1.9) | |
| Flexor tendon rupture | 1 (0.6) | 1 (0.6) | >0.999 | |
| Extensor tendon rupture | 3 (1.9) | 2 (1.2) | 0.987 | |
| Nerve related | Palmar sensory branch damage of median nerve | 2 (1.3) | 1 (0.6) | 0.628 |
| CRPS | 1 (0.6) | 3 (1.9) | 0.628 | |
| Carpal tunnel syndrome | 13 (8.2) | 17 (10.5) | 0.602 | |
| Acute | 0 | 3 (1.9) | ||
| Subacute | 9 (5.7) | 7 (4.3) | ||
| Delayed | 4 (2.5) | 7 (4.3) | ||
| Carpal tunnel release | 3 (1.9) | 9 (5.6) | 0.102 | |
| Fixation and instrument related | Reduction loss | 8 (5.0) | 3 (1.9) | 0.136 |
| Implant failure or screw breakage | 4 (2.5) | 1 (0.6) | 0.211 | |
| Screw penetration | 3 (1.9) | 1 (0.6) | 0.368 | |
| Implant removal | 42 (26.4) | 18 (11.1) | 0.001* | |
| Osteosynthesis | Delayed union | 0 | 2 (1.2) | 0.486 |
| Non-union | 0 | 0 | - | |
| Infection | Superficial | 1 (0.6) | 3 (1.9) | 0.628 |
| Deep | 0 | 0 | - | |
| Others | Compartment | 0 | 0 | - |
| Radial artery injury | 2 (1.3) | 0 | 0.470 | |
Table 4.
Total Complication Comparison with Previous Report
| This study (321 wrists in 319 patients) | Lee et al.5) (2020) (1,955 wrists in 1,921 patients) | p-value | ||
|---|---|---|---|---|
| Age (yr) | 63.3±13.8 | 60.3±14.6 | ||
| Sex | Male | 84 (26.3) | 587 (30.6) | 0.205 |
| Female | 235 (73.7) | 1,334 (69.4) | ||
| Complication | ||||
| Tendon injury | Tendon rupture | 7 (2.2) | 21 (1.1) | 0.106 |
| Flexor tendon rupture | 2 (0.6) | 9 (0.5) | >0.999 | |
| Extensor tendon rupture | 5 (1.6) | 12 (0.6) | 0.141 | |
| Nerve related | Palmar sensory branch damage of median nerve | 3 (0.9) | 9 (0.5) | 0.502 |
| CRPS | 4 (1.2) | 15 (0.8) | 0.587 | |
| Carpal tunnel syndrome | 30 (9.3) | 36 (1.8) | <0.001* | |
| Carpal tunnel release | 12 (3.7) | 17 (0.9) | <0.001* | |
| Fixation and Instrument related | Reduction loss | 11 (3.4) | 4 (0.2) | <0.001* |
| Implant failure including screw loosening or breakage | 5 (1.6) | 6 (0.3) | 0.010* | |
| Screw penetration in joint | 4 (1.2) | 26 (1.3) | >0.999 | |
| Implant removal | 60 (18.7) | 511 (26.1) | 0.005* | |
| Osteosynthesis | Delayed union | 2 (0.6) | 5 (0.3) | 0.577 |
| Non-union | 0 | 3 (0.2) | >0.999 | |
| Infection | Superficial | 4 (1.2) | 83 (4.2) | 0.015* |
| Deep | 0 | 2 (0.1) | >0.999 | |
| Others | Compartment | 0 | 2 (0.1) | >0.999 |
| Radial artery injury | 2 (0.6) | 3 (0.2) | 0.307 | |
- 1. Tang JB: Distal radius fracture: diagnosis, treatment, and controversies. Clin Plast Surg, 41: 481-499, 2014.PubMed
- 2. Wilcke MK, Hammarberg H, Adolphson PY: Epidemiology and changed surgical treatment methods for fractures of the distal radius: a registry analysis of 42,583 patients in Stockholm County, Sweden, 2004-2010. Acta Orthop, 84: 292-296, 2013.PubMedPMC
- 3. Hevonkorpi TP, Launonen AP, Huttunen TT, Kannus P, Niemi S, Mattila VM: Incidence of distal radius fracture surgery in Finns aged 50 years or more between 1998 and 2016 - too many patients are yet operated on? BMC Musculoskelet Disord, 19: 70, 2018.ArticlePubMedPDF
- 4. Medoff RJ, Saucedo JM: Common errors of volar plate fixation. In: del Piñal F, Haerle M, Krimmer H eds. Distal radius fractures and carpal instabilities. FESSH IFSSH 2019 Instructional Book. Thieme: 146-148, 2019.
- 5. Lee JH, Lee JK, Park JS, et al: Complications associated with volar locking plate fixation for distal radius fractures in 1955 cases: a multicentre retrospective study. Int Orthop, 44: 2057-2067, 2020.ArticlePubMedPDF
- 6. Tang JB: Re: Levels of experience of surgeons in clinical studies. J Hand Surg Eur Vol, 34: 137-138, 2009.ArticlePubMedPDF
- 7. Wolfe SW: Distal radius fractures. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, Cohen MS eds. Green’s operative hand surgery. 7th ed. Elsevier: 516-587, 2017.
- 8. Soong M, Earp BE, Bishop G, Leung A, Blazar P: Volar locking plate implant prominence and flexor tendon rupture. J Bone Joint Surg Am, 93: 328-335, 2011.ArticlePubMed
- 9. Lee JK, Bang JY, Choi YS, Kim TH, Yu WJ, Han SH: Extensor pollicis longus tendon rupture caused by a displaced dorsal "beak" fragment of Lister's tubercle in distal radius fractures. Handchir Mikrochir Plast Chir, 51: 199-204, 2019.ArticlePubMed
- 10. Tang JB, Giddins G: Why and how to report surgeons’ levels of expertise. J Hand Surg Eur Vol, 41: 365-366, 2016.ArticlePubMedPDF
- 11. Yamamoto M, Fujihara Y, Fujihara N, Hirata H: A systematic review of volar locking plate removal after distal radius fracture. Injury, 48: 2650-2656, 2017.ArticlePubMed
- 12. Tan A, Chong A: Reasons for implant removal after distal radius fractures. J Hand Surg Asian Pac Vol, 21: 321-325, 2016.ArticlePubMed
- 13. Lee JK, Lee Y, Kim C, Kim M, Han SH: Volar locking plate removal after distal radius fracture: a 10-year retrospective study. Arch Orthop Trauma Surg, 141: 1711-1719, 2021.ArticlePubMedPDF
- 14. Orbay JL, Badia A, Indriago IR, et al: The extended flexor carpi radialis approach: a new perspective for the distal radius fracture. Tech Hand Up Extrem Surg, 5: 204-211, 2001.Article
- 15. Costa ML, Achten J, Rangan A, Lamb SE, Parsons NR: Percutaneous fixation with Kirschner wires versus volar locking-plate fixation in adults with dorsally displaced fracture of distal radius: five-year follow-up of a randomized controlled trial. Bone Joint J, 101-B: 978-983, 2019.ArticlePubMedPMCPDF
- 16. Jeudy J, Steiger V, Boyer P, Cronier P, Bizot P, Massin P: Treatment of complex fractures of the distal radius: a prospective randomised comparison of external fixation 'versus' locked volar plating. Injury, 43: 174-179, 2012.ArticlePubMed
- 17. McFadyen I, Field J, McCann P, Ward J, Nicol S, Curwen C: Should unstable extra-articular distal radial fractures be treated with fixed-angle volar-locked plates or percutaneous Kirschner wires? A prospective randomised controlled trial. Injury, 42: 162-166, 2011.ArticlePubMed
- 18. Orbay JL, Fernandez DL: Volar fixed-angle plate fixation for unstable distal radius fractures in the elderly patient. J Hand Surg Am, 29: 96-102, 2004.ArticlePubMed
- 19. Twigt B, Bemelman M, Lansink K, Leenen L: Type C distal radial fractures treated with conventional AO plates: an easy and cost-saving solution in a locking plate era. Int Orthop, 37: 483-488, 2013.ArticlePubMedPMCPDF
- 20. Orbay JL: The treatment of unstable distal radius fractures with volar fixation. Hand Surg, 5: 103-112, 2000.ArticlePubMed
- 21. Ruch DS, McQueen MM: Distal radius and ulna fractures. In: Bucholz RW, Beaty JH, Rockwood CA, Green DP eds. Rockwood and Green’s fractures in adults. Lippincott Williams & Wilkins: 829-880, 2010.
- 22. Lee JK, Yoon BH, Kim B, et al: Is early mobilization after volar locking plate fixation in distal radius fractures really beneficial? A meta-analysis of prospective randomized studies. J Hand Ther, 36: 196-207, 2023.ArticlePubMed
- 23. Cafarelli L, El Amiri L, Facca S, Chakfé N, Sapa MC, Liverneaux P: Anterior plating technique for distal radius: comparing performance after learning through naive versus deliberate practice. Int Orthop, 46: 1821-1829, 2022.ArticlePubMedPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Epidemiological changes and surgical trends of distal radius fractures in adults over 50 years during the COVID-19 pandemic in Korea: a nationwide repeated cross-sectional study
Han-Kook Yoon, So Ra Yoon, Kee-Bum Hong, Youngsu Jung, SeongJu Choi, Jun-Ku Lee
Journal of Musculoskeletal Trauma.2026; 39(1): 12. CrossRef - Author correction: “Does the operator's experience affect the occurrence of complications after distal radius fracture volar locking plate fixation? A comparative study of the first four years and thereafter”
Kee-Bum Hong, Chi-Hoon Oh, Chae Kwang Lim, Sungwoo Lee, Soo-Hong Han, Jun-Ku Lee
Journal of Musculoskeletal Trauma.2025; 38(1): 40. CrossRef - Characteristics of patients with distal radius fracture requiring arthroscopic foveal repair after bone union
Min Jung Park, Cheungsoo Ha, Hyun Tak Kang, Yong Hyun Yoon, Jun-Ku Lee, Soo-Hong Han
Arthroscopy and Orthopedic Sports Medicine.2025; 12(2): 70. CrossRef
 ePub Link
ePub Link Cite
CiteDoes the Operator’s Experience Affect the Occurrence of Complications after Distal Radius Fracture Volar Locking Plate Fixation? A Comparative Study of the First Four Years and Thereafter
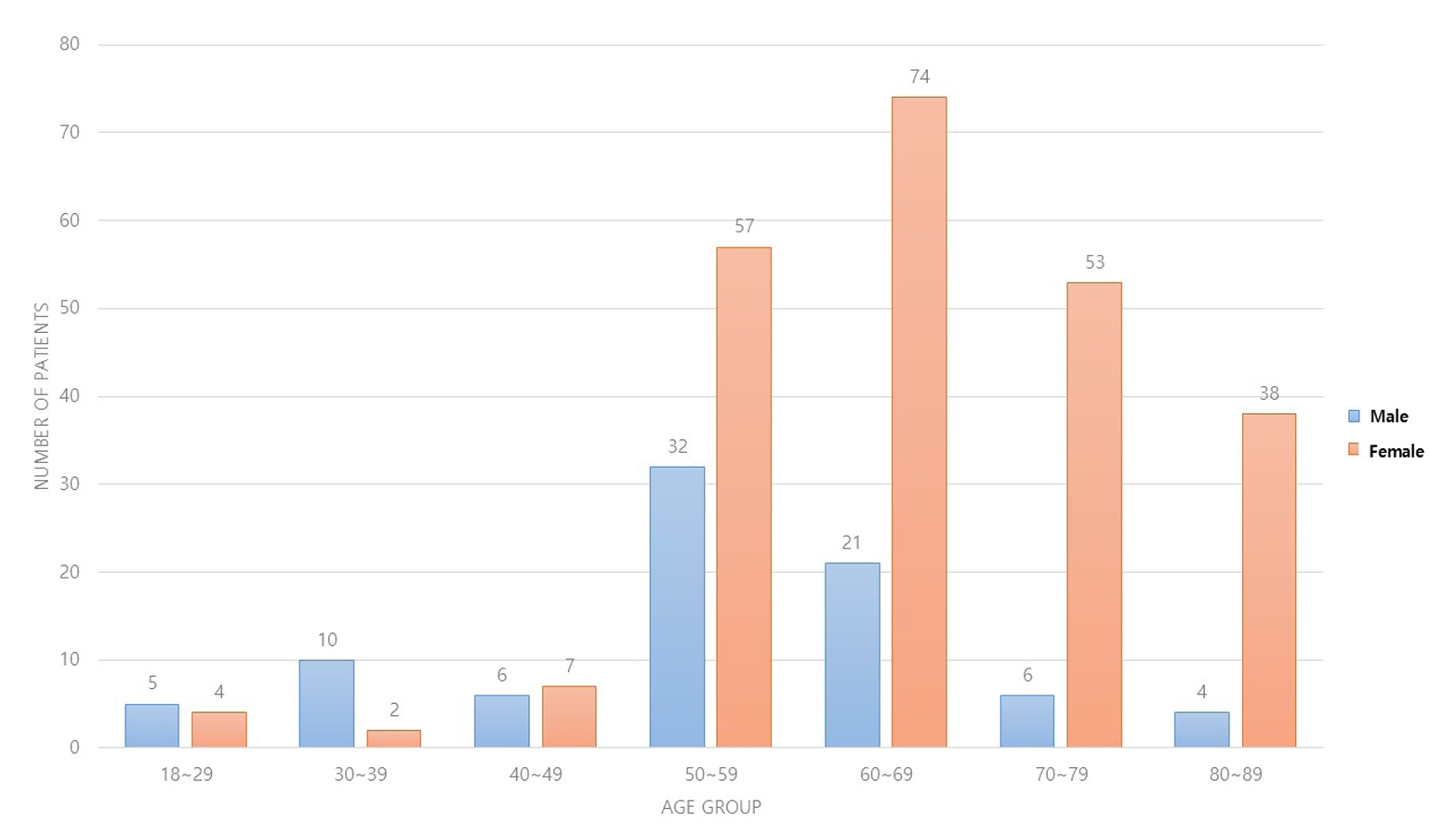
Fig. 1. Number of patients distributed depends on sex and age groups.
Fig. 1.
Does the Operator’s Experience Affect the Occurrence of Complications after Distal Radius Fracture Volar Locking Plate Fixation? A Comparative Study of the First Four Years and Thereafter
| Characteristic | Group 1 (157 patients) | Group 2 (162 patients) | p-value |
|---|---|---|---|
| Sex | 0.422 | ||
| Female | 112 (71.3) | 123 (75.9) | |
| Male | 45 (28.7) | 39 (24.1) | |
| Age (yr) | 61.6±12.6 | 64.8±14.7 | 0.038 |
| Weight (kg) | 61.9±10.9 | 62.1±12.4 | 0.907 |
| Height (m) | 1.6±0.1 | 1.6±0.1 | 0.389 |
| BMI (kg/m2) | 24.5±3.9 | 24.1±3.6 | 0.465 |
| Group 1 (159 wrists) | Group 2 (162 wrists) | p-value | |
|---|---|---|---|
| Fractured arm | 0.204 | ||
| Right | 68 (42.8) | 83 (51.2) | |
| Left | 91 (57.2) | 79 (48.8) | |
| AO-OTA classification | 0.133 | ||
| A2 | 24 (15.1) | 12 (7.4) | |
| A3 | 21 (13.2) | 26 (16.0) | |
| B2 | 6 (3.8) | 3 (1.9) | |
| B3 | 10 (6.3) | 12 (7.4) | |
| C1 | 26 (16.4) | 24 (14.8) | |
| C2 | 35 (22.0) | 53 (32.7) | |
| C3 | 37 (23.3) | 32 (19.8) | |
| Ulnar fracture combined | 0.904 | ||
| None | 55 (34.6) | 54 (33.3) | |
| Yes | 104 (65.4) | 108 (66.7) | |
| Preoperative duration (d) | 3.9±5.4 | 5.2±10.8 | 0.169 |
| Operation time (min) | 74.4±26.5 | 53.7±14.5 | <0.001 |
| Union time (d) | 53.5±25.7 | 53.5±23.6 | 0.988 |
| Total follow-up duration (d) | 292.6±240.9 | 213.3±146.0 | <0.001 |
| Complication | Group 1 (159 wrists) | Group 2 (162 wrists) | p-value | |
|---|---|---|---|---|
| Tendon injury | Tendon rupture | 4 (2.5) | 3 (1.9) | |
| Flexor tendon rupture | 1 (0.6) | 1 (0.6) | >0.999 | |
| Extensor tendon rupture | 3 (1.9) | 2 (1.2) | 0.987 | |
| Nerve related | Palmar sensory branch damage of median nerve | 2 (1.3) | 1 (0.6) | 0.628 |
| CRPS | 1 (0.6) | 3 (1.9) | 0.628 | |
| Carpal tunnel syndrome | 13 (8.2) | 17 (10.5) | 0.602 | |
| Acute | 0 | 3 (1.9) | ||
| Subacute | 9 (5.7) | 7 (4.3) | ||
| Delayed | 4 (2.5) | 7 (4.3) | ||
| Carpal tunnel release | 3 (1.9) | 9 (5.6) | 0.102 | |
| Fixation and instrument related | Reduction loss | 8 (5.0) | 3 (1.9) | 0.136 |
| Implant failure or screw breakage | 4 (2.5) | 1 (0.6) | 0.211 | |
| Screw penetration | 3 (1.9) | 1 (0.6) | 0.368 | |
| Implant removal | 42 (26.4) | 18 (11.1) | 0.001 |
|
| Osteosynthesis | Delayed union | 0 | 2 (1.2) | 0.486 |
| Non-union | 0 | 0 | - | |
| Infection | Superficial | 1 (0.6) | 3 (1.9) | 0.628 |
| Deep | 0 | 0 | - | |
| Others | Compartment | 0 | 0 | - |
| Radial artery injury | 2 (1.3) | 0 | 0.470 | |
| This study (321 wrists in 319 patients) | Lee et al.5) (2020) (1,955 wrists in 1,921 patients) | p-value | ||
|---|---|---|---|---|
| Age (yr) | 63.3±13.8 | 60.3±14.6 | ||
| Sex | Male | 84 (26.3) | 587 (30.6) | 0.205 |
| Female | 235 (73.7) | 1,334 (69.4) | ||
| Complication | ||||
| Tendon injury | Tendon rupture | 7 (2.2) | 21 (1.1) | 0.106 |
| Flexor tendon rupture | 2 (0.6) | 9 (0.5) | >0.999 | |
| Extensor tendon rupture | 5 (1.6) | 12 (0.6) | 0.141 | |
| Nerve related | Palmar sensory branch damage of median nerve | 3 (0.9) | 9 (0.5) | 0.502 |
| CRPS | 4 (1.2) | 15 (0.8) | 0.587 | |
| Carpal tunnel syndrome | 30 (9.3) | 36 (1.8) | <0.001 |
|
| Carpal tunnel release | 12 (3.7) | 17 (0.9) | <0.001 |
|
| Fixation and Instrument related | Reduction loss | 11 (3.4) | 4 (0.2) | <0.001 |
| Implant failure including screw loosening or breakage | 5 (1.6) | 6 (0.3) | 0.010 |
|
| Screw penetration in joint | 4 (1.2) | 26 (1.3) | >0.999 | |
| Implant removal | 60 (18.7) | 511 (26.1) | 0.005 |
|
| Osteosynthesis | Delayed union | 2 (0.6) | 5 (0.3) | 0.577 |
| Non-union | 0 | 3 (0.2) | >0.999 | |
| Infection | Superficial | 4 (1.2) | 83 (4.2) | 0.015 |
| Deep | 0 | 2 (0.1) | >0.999 | |
| Others | Compartment | 0 | 2 (0.1) | >0.999 |
| Radial artery injury | 2 (0.6) | 3 (0.2) | 0.307 | |
Table 1. Basic Characteristic Comparison between the Groups
Values are presented as number (%) or mean±standard deviation. Group 1: comprising cases within the first four years, Group 2: covering the subsequent four years until the study’s conclusion. p<0.05.
Table 2. Group Comparison of the Fracture Characteristics and Operation-Associated Factors
Values are presented as number (%) or mean±standard deviation. Group 1: comprising cases within the first four years, Group 2: covering the subsequent four years until the study’s conclusion. p<0.05.
Table 3. Comparison of the Complication between the Groups
Values are presented as number (%). Group 1: comprising cases within the first four years, Group 2: covering the subsequent four years until the study’s conclusion. p<0.05. CRPS: complex regional pain syndrome.
Table 4. Total Complication Comparison with Previous Report
Values are presented as mean±standard deviation or number (%). Group 1: comprising cases within the first four years, Group 2: covering the subsequent four years until the study’s conclusion. p<0.05. CRPS: complex regional pain syndrome.

