 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Articles
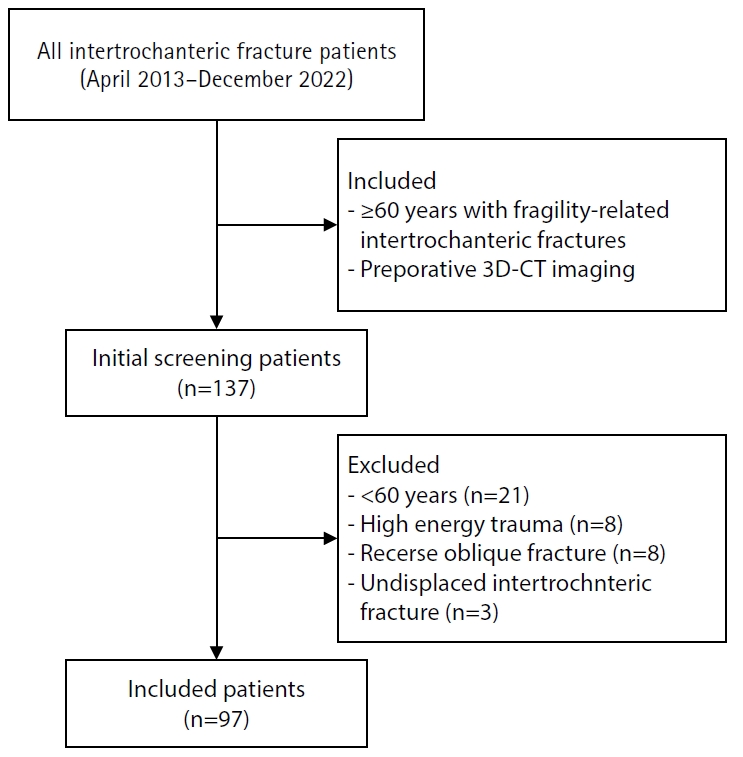
- Three-dimensional computed tomography-based differentiation of engaged versus displaced intertrochanteric fractures using the anterior fracture line: a cross-sectional study from Korea
- Jae-Suk Chang, Jin Yeob Park, Sang-Ok Chun, Chul-Ho Kim
- J Musculoskelet Trauma 2026;39(1):30-37. Published online January 25, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00318
-
 Abstract
Abstract
 PDF
PDF - Background
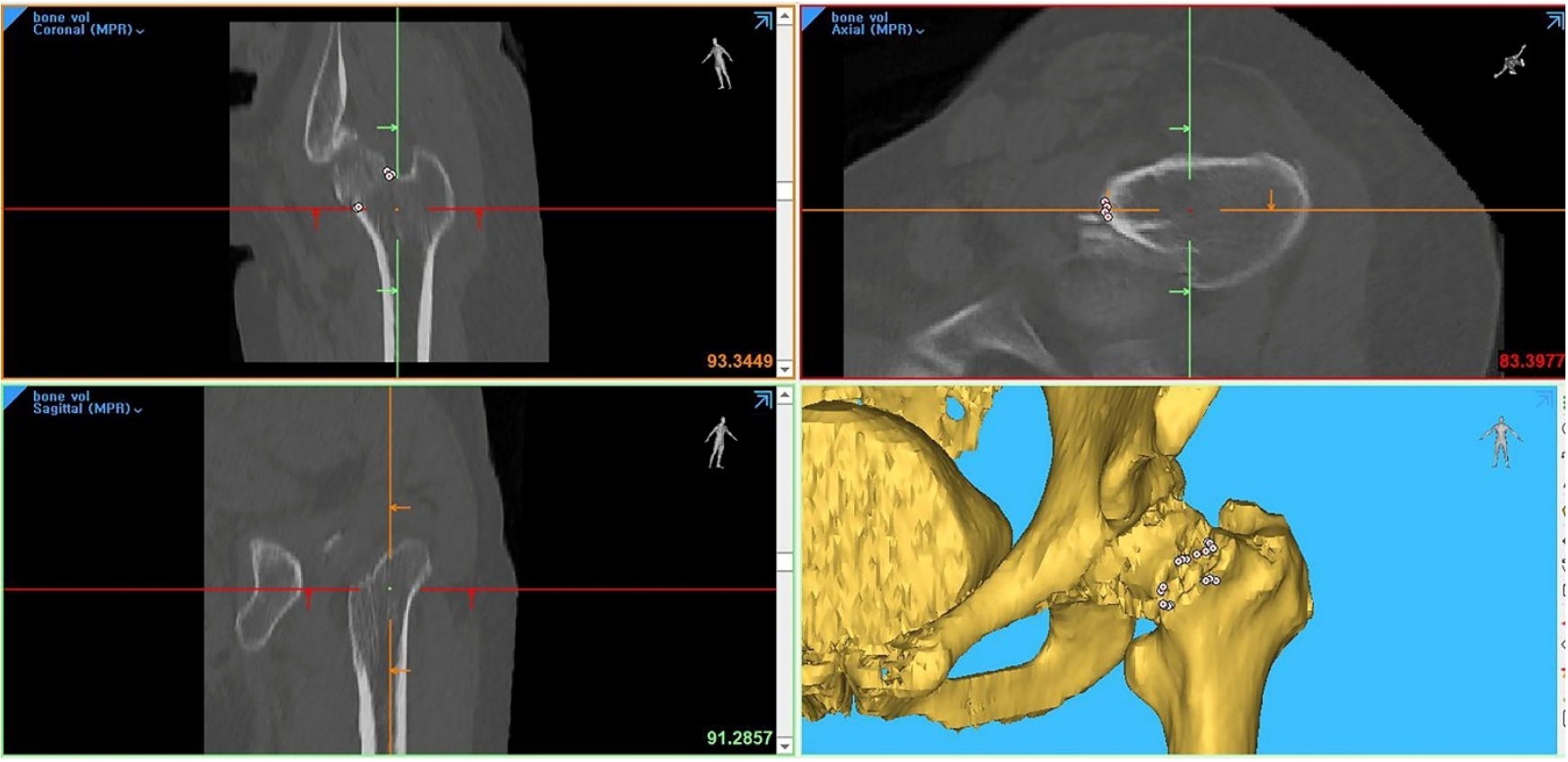
With the advent of an aging society, osteoporotic fractures—particularly hip fractures—are increasing, with a 1-year mortality rate of 17%. Achieving stable fixation that enables early ambulation is essential but remains challenging because complex intertrochanteric (IT) fracture patterns are often underestimated on plain radiographs. Using three-dimensional computed tomography (3D-CT), this study analyzed whether the anterior fracture line lies medial or lateral to the IT line and examined its relationship with displacement or distal medullary canal engagement, highlighting the potential influence of the joint capsule and capsular ligaments on fracture morphology and fixation stability.
Methods
A retrospective review was conducted on 96 osteoporotic IT fractures in patients aged ≥60 years treated between April 2013 and December 2022 at National Police Hospital and Asan Medical Center, Seoul, Korea. Fractures were classified as engaged, completely displaced, and partially displaced based on 3D-CT findings. The anterior fracture-line position (medial or lateral to the IT line) and the status of the lesser trochanter (LT) were evaluated. The chi-square or Fisher exact test was used for statistical comparisons.
Results
In total, 96 patients were analyzed. Of these, 49 cases (51.0%) were classified as engaged type, 27 cases (28.1%) as completely displaced type, and 20 cases (20.8%) as partially displaced type. When comparing fracture pattern with anterior fracture-line position, the completely displaced type showed a significantly higher proportion of lateral anterior fracture lines than the other two types (P<0.001). However, no significant association was identified between fracture pattern and LT displacement. When the anterior fracture-line position and LT displacement were evaluated together, only the engaged type demonstrated a possible association between a lateral anterior fracture line and LT displacement, though the statistical significance was weak (P=0.047).
Conclusions
Fracture lines lateral to the IT line were strongly associated with displacement in IT fractures; however, their relationship with LT involvement, reflecting iliopsoas tendon traction, was not clearly demonstrated. Although the factors contributing to the engaged-type fracture remain uncertain, the statistical association between fracture pattern and anterior fracture-line position suggests that capsular structures may play a stabilizing role in select fracture configurations. Further studies are needed to clarify these anatomical interactions. Level of evidence:
- 1,099 View
- 19 Download

- Computed tomography plane reformatting to reduce projection error in measuring Pauwels angle of femoral neck fractures: a cross-sectional study
- Gyu Min Kong, Jae-Young Lim, Se-Lin Jeong, Gu-Hee Jung
- J Musculoskelet Trauma 2026;39(1):38-47. Published online January 25, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00038
-
Abstract
PDF
- Objectives
This study aimed to assess fracture verticality in both coronal and axial planes after eliminating projection error in femoral neck fractures among non-older adults, and to demonstrate its clinical utility using computed tomography (CT)-based modeling at actual size.
Methods
This retrospective observational study enrolled 57 patients (30 males and 27 females), aged 20–65 years, with displaced femoral neck fractures. Based on CT images, an actual-size fracture model was constructed. The CT scanning plane was reformatted with the neck-shaft fragment realigned vertically to the ground and parallel to the femoral neck axis. Three consecutive images were used to generate coronal reformats at the centerline and posterior border to measure central and posterior coronal plane verticality as Pauwels’ angle (PA). The central image of the reformatted axial plane was used to assess axial plane verticality. Differences in verticality were analyzed using analysis of variance.
Results
Three coronal morphology types were identified: linear (n=30), concave (n=25), and convex (n=2). Two axial morphology types were observed: cephalad (n=35) and trochanteric (n=22). The mean central PA, posterior PA, and axial verticality were 55.43°±13.79°, 51.44°±11.13°, and 85.74°±18.41°, respectively. Only the central PA showed a significant difference (P<0.001). The PA was significantly higher in the linear coronal type between images (P<0.05) and in the trochanteric axial type (P<0.05).
Conclusions
After reformatting the scanning plane, the central PA showed significant variation between images. Femoral neck fractures of the linear type in the coronal plane and the trochanteric type in the axial plane demonstrated greater verticality than other morphological types. Level of evidence:
- 746 View
- 14 Download
- Risk factors of surgical complications after use of the femoral neck system: a random forest analysis
- Chul-Ho Kim, Hyun-Chul Shon, Han Soul Kim, Ji Wan Kim, Eic Ju Lim
- J Musculoskelet Trauma 2025;38(3):160-167. Published online July 23, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00157
-
Abstract
PDF
- Background
The femoral neck system (FNS), a novel fixation device for managing femoral neck fractures (FNFs), has gained popularity in recent years. However, analyses of the surgical complications and reoperation risks associated with the use of FNS remain limited.
Methods
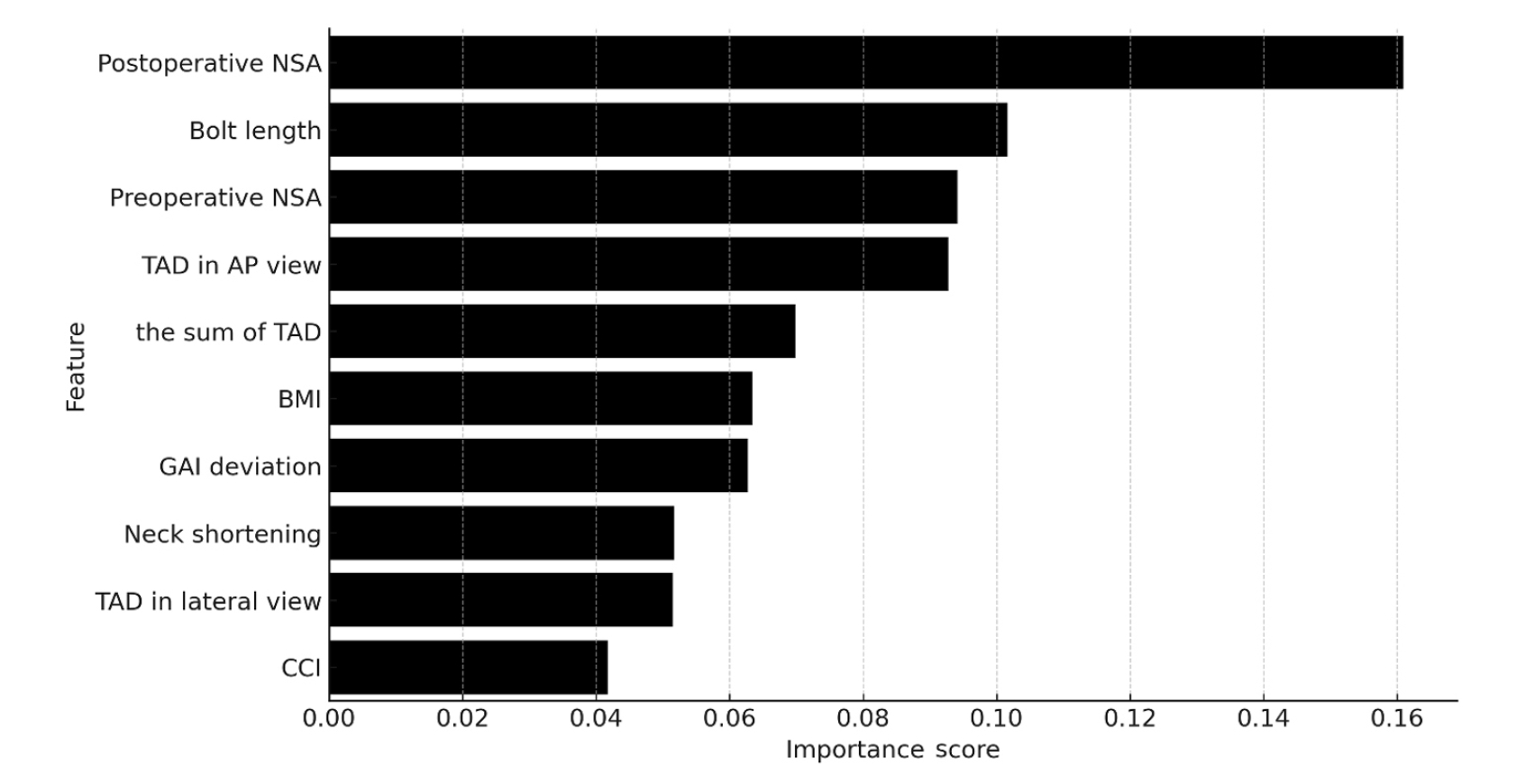
This retrospective observational study analyzed 57 patients who had undergone FNS fixation for FNF at two university hospitals between July 2019 and February 2024. Demographic, perioperative, and outcome variables, including age, sex, fracture classification (Garden, Pauwels, and AO), implant characteristics, tip-apex distance (TAD), neck shortening, and neck-shaft alignment, were analyzed. In addition to univariate analysis, a machine learning analysis was conducted using a random forest classifier with stratified sampling (80% training, 20% testing). The accuracy, precision, recall, F1-score, and area under the receiver’s operating curve were calculated to assess model performance.
Results
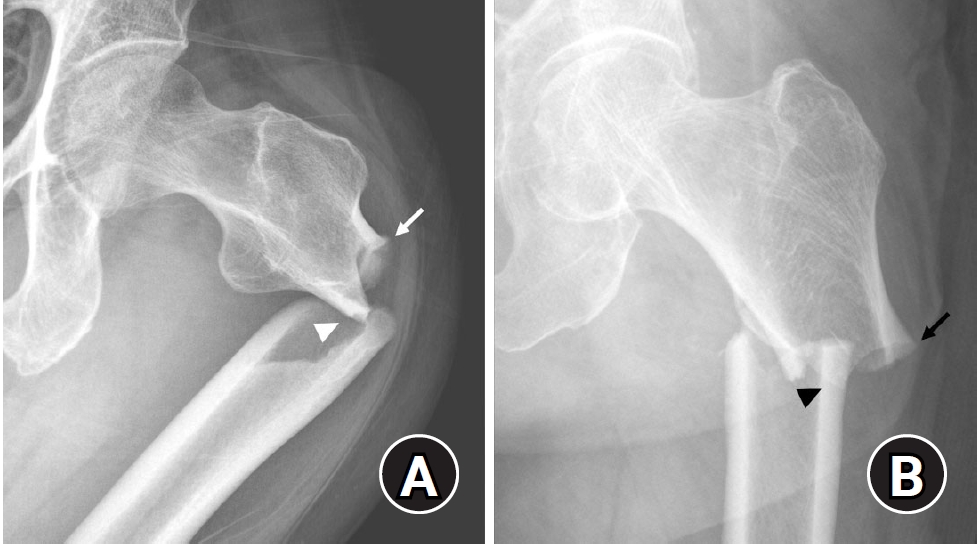
Ten patients experienced osteonecrosis of the femoral head (n=6), implant cut-out or penetration (n=3), and peri-implant fracture (n=1). Univariate analysis revealed that the TAD in the complication group was significantly shorter than that in the control group (12.1 vs. 16.7 mm; P=0.012). Additionally, neck shortening in the complication group was greater than that in the control group (4.9 vs. 2.3 mm; P=0.011). The random forest model achieved an accuracy of 83.3% and identified postoperative neck-shaft angle (NSA) as the most important predictor of complications (feature importance, 0.161), followed by bolt length (0.102) and preoperative NSA (0.094).
Conclusions
Risk factor analysis conducted using a random forest model identified postoperative NSA as the most important feature associated with postoperative complications following FNS. Therefore, care should be taken to normalize the postoperative NSA during FNF surgery. Level of Evidence: III. -
Citations
Citations to this article as recorded by
- Length-stable fixation reduces femoral neck shortening in unstable femoral neck fractures: A retrospective comparative study of length-stable dynamic hip screw versus femoral neck system fixation
Seonghyun Kang, Wonseok Choi, Jeong Seok Choi, Eic Ju Lim, SungJin Ahn, Jong-Keon Oh, William T. Kent, Whee Sung Son, Jae-Woo Cho
Journal of Orthopaedic Surgery.2026;[Epub] CrossRef
- Length-stable fixation reduces femoral neck shortening in unstable femoral neck fractures: A retrospective comparative study of length-stable dynamic hip screw versus femoral neck system fixation
- 2,234 View
- 56 Download
- 1 Crossref
Review Article
- Atypical femoral fractures: an update
- Won-Tae Cho, Jeong-Hyun Koh, Seungyeob Sakong, Jung-Taek Kim
- J Musculoskelet Trauma 2025;38(2):41-52. Published online March 28, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00031
-
Abstract
PDF
- This narrative review provides an up-to-date overview of atypical femoral fractures (AFFs), emphasizing diagnostic criteria, epidemiology, pathophysiology, risk factors, and evaluation with screening strategies. AFFs are rare but significant complications associated with prolonged bisphosphonate (BP) therapy for osteoporosis. Although the pathogenesis of AFFs has not been fully elucidated, its primary mechanism is thought to involve impaired bone remodeling, leading to unhealed microfractures that progress to stress fractures under repetitive loading. AFFs can occur in various regions of the femur, influenced by femoral geometry and the lower limb axis. Other risk factors include prolonged steroid use, arthroplasty, genetic predispositions, and metabolic bone disorders. The diagnosis of AFFs is based on criteria established by the American Society for Bone and Mineral Research. Key radiographic features include lateral cortical transverse fracture lines and localized cortical thickening, typically with minimal or no comminution on the medial cortex. Dual-energy X-ray absorptiometry for screening tests and magnetic resonance imaging as an advanced imaging modality enable the early detection of incomplete fractures. This multi-modal approach facilitates the prompt identification of prodromal cortical changes, reducing the risk of complete fractures in high-risk populations, particularly patients undergoing prolonged BP therapy. Level of Evidence: V
-
Citations
Citations to this article as recorded by- Clinical Images: Bisphosphonate‐associated atypical femoral fracture with contralateral cortical beaking
Andreina Martinez Paulino, Valentin Marian
ACR Open Rheumatology.2026;[Epub] CrossRef - Atypical femoral fracture: The periprosthetic variant about two cases without bisphosphonate use
Guillaume Auberger, Thomas Aubert, Younes Kerroumi, Philippe Leclerc, Simon Marmor
SICOT-J.2026; 12: 41. CrossRef - Atypical Femur Fractures Without Bisphosphonate Exposure (AFFwB): A Retrospective Report of 21 Cases
Lorenzo Lucchetta, Carmelinda Ruggiero, Samuele Berardi, Alice Franceschi, Michele Bisaccia, Giuseppe Rinonapoli
Journal of Clinical Medicine.2025; 15(1): 25. CrossRef
- Clinical Images: Bisphosphonate‐associated atypical femoral fracture with contralateral cortical beaking
- 65,535 View
- 658 Download
- 3 Crossref
Original Articles
- The Results of Intramedullary Nailing with Sliding Restriction and Dynamization Method in Treating Intertrochanteric Fractures
- Hyun Cheol Oh, Sang Hoon Park, Jae Seok Chae, Han Kook Yoon
- J Korean Fract Soc 2024;37(1):8-14. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.8
-
Abstract
PDF
- Purpose
To evaluate the results of intramedullary nailing with sliding restriction and dynamization methods in treating intertrochanteric fractures.
Materials and Methods
From August 2016 to March 2019, patients aged 65 years and older who underwent intramedullary nailing in treating intertrochanteric fractures were enrolled in this study. The radiological and clinical results were analyzed in 49 patients who had undergone lag screw sliding re-striction and dynamization of the distal interlocking screw method.
Results
Forty-seven patients achieved union without complications (95.9%). The mean union period was 6.5 weeks (range, 6-9 weeks). Complications occurred in two patients (4.1%), including the cut through of the lag screw in one patient and varus deformity of more than 10° in the other. The preinjury mean Koval grade was 2.8 (range, 1-7). The mean was 3.3 (range, 1-7) at the final follow-up, and the mean difference was 0.5 (range, 0-2).
Conclusion
Intramedullary nailing with a sliding restriction and dynamization method for treating in-tertrochanteric fractures achieved union. The reduction achieved during surgery was maintained with good clinical results. This method is a safe and effective treatment technique for femoral intertrochanteric fractures.
- 1,069 View
- 17 Download
- Effect of Additional Medial Locking Plate Fixation and Autogenous Bone Graft for Distal Femur Nonunion after Lateral Locking Plate Fixation
- Ho Min Lee, Jong Pil Kim, In Hwa Baek, Han Sol Moon, Sun Kyo Nam
- J Korean Fract Soc 2024;37(1):30-38. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.30
-
Abstract
PDF
- Purpose
This study examined the outcomes of additional medial locking plate fixation and autogenous bone grafting in the treatment of nonunions that occurred after initial fixation for distal femoral fractures using lateral locking plates.
Materials and Methods
The study involved eleven patients who initially underwent minimally invasive lateral locking plate fixation for distal femoral fractures between January 2008 and December 2020. The initial procedure was followed by additional medial locking plate fixation and autogenous bone grafting for clinically and radiographically confirmed nonunions, while leaving the stable lateral locking plate in situ. A clinical evaluation of the bone union time, knee joint range of motion, visual analog scale (VAS) pain scores, presence of postoperative complications, and functional evaluations using the lower extremity functional scale (LEFS) were performed.
Results
In all cases, bone union was achieved in an average of 6.1 months after the secondary surgery. The range of knee joint motion, weight-bearing ability, and VAS and LEFS scores improved at the final follow-up compared to the preoperative conditions. All patients could walk without walking assistive devices and did not experience pain at the fracture site. On the other hand, three patients complained of pain in the lateral knee joint caused by irritation by the lateral locking plate; hence, lateral hardware removal was performed. One patient complained of mild paresthesia at the anteromedial incision site. Severe complications, such as deep infection or metal failure, were not observed.
Conclusion
For nonunion with stable lateral locking plates after minimally invasive lateral locking plate fixation of distal femur fractures, additional medial locking plate fixation and autogenous bone grafting, while leaving the lateral locking plate intact, can achieve successful bone union.
- 771 View
- 7 Download
- Cephalomedullary Nailing with an Additional Cannulated Screw Fixation in Basicervical Femur Fractures
- Keong-Hwan Kim, Woo Dong Nam, Yeon Sik Heo, Gu-Hee Jung
- J Korean Fract Soc 2024;37(1):22-29. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.22
-
Abstract
PDF
- Purpose
The purpose of this study is to analyze the clinical results of patients with basicervical fracture undergoing cephalomedullary nailing (CMN) with an additional cannulated screw fixation compared to only performing CMN. We hypothesized that a difference may exist in the clinical outcomes if an ad-ditional screw is fixed with CMN compared to only performing CMN in basicervical fracture.
Materials and Methods
A total of 28 consecutive patients who underwent CMN for basicervical fracture were included. In 9 cases, only CMN was conducted, and in 19 cases, an additional cannulated screw fixation was performed with CMN. Bone union, sliding distance, reduction status, and fixation failure were evaluated by postoperative radiography, and ambulatory ability was evaluated by functional results. These findings were compared between a group of CMN and a group of CMN with an additional cannulated screw.
Results
There were 4 males and 24 females with a mean age of 84 years (range, 69–100 years). No significant difference was found in postoperative reduction, tip-apex distance, bone union, and walking function recovery after surgery between the two groups, but in the sliding distance of the lag screw, the CMN group demonstrated more sliding (6.2 mm [range, 2.5–13.4 mm] vs 3.5 mm [range, 0.1– 9.2 mm]; p=0.045). Among the two groups, only one case of fixation failure at the postoperative four months was observed in the CMN group (p=0.321), and hemiarthroplasty with nail construct removal was performed.
Conclusion
CMN with additional cannulated screw fixation is a safe and reliable surgical option in basicervical fracture. It provided favorable clinical outcomes and may be a good alternative for treating basicervical fracture.
- 2,273 View
- 20 Download
- Bone Union Time of Simple Distal Femur Fractures in the Elderly according to Fracture Gap after Treated with Minimally Invasive Plate Osteosynthesis
- Young Ho Cho, Sangwoo Kim, Jaewook Koo
- J Korean Fract Soc 2023;36(4):133-138. Published online October 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.4.133
-
Abstract
PDF
- Purpose
This study examined the difference in bone union time according to the fracture gap after minimally invasive plate osteosynthesis (MIPO) for simple distal femoral fractures in elderly patients.
Materials and Methods
From January 2010 to December 2019, patients aged 60 years or older who underwent surgical treatment for distal femoral fractures due to a low-energy injury were investigated retrospectively. Forty patients were enrolled in the study. The patients were divided into two groups according to the fracture gap after reduction: no more than 2 mm (Group A) and more than 2 mm (Group B) in the anteroposterior and lateral plane. The demographic, operation time, presence or absence of cerclage wiring, plate screw density, plate span ratio, plate length, bone union period, non-union, and complications were evaluated.
Results
No statistical differences in operation time, cerclage wiring, plate screw density, plate span ratio, and plate length were observed between the two groups, and the bone union was achieved in all patients without complication. The bone union period was 17.24±1.48 weeks in Group A and 24.53± 5.20 weeks in Group B, which was statistically significant (p<0.001).
Conclusion
The bone union time in treating geriatric simple distal femur fractures using the MIPO tech-nique was significantly shorter in the 2 mm or less fracture gap than in the greater than 2 mm group.
- 1,173 View
- 7 Download
- Risk Factors of Fixation Failure in Femoral Neck Fractures
- Sung Hyun Yoon, Kyu Beom Kim, Hyung Jun Lee, Kyung Wook Kim
- J Korean Fract Soc 2023;36(4):118-124. Published online October 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.4.118
-
Abstract
PDF
- Purpose
Internal fixation after a femoral neck fracture (FNF) is one of the conventional treatment options for the young and active elderly patients. However, fixation failure of internal fixation is a probable complication. The treatment of fixation failure after a primary internal fixation of the FNF remains a challenge.
Materials and Methods
Between July 2002 and March 2017, 83 patients who underwent internal fixation after FNF were retrospectively analyzed. Radiological assessments, including Pauwels’ angle, fracture level, reduction quality, and bone union, were measured, preoperatively and postoperatively. Moreover, intraoperative variables such as time to surgery, surgical time, and estimated blood loss were also evaluated.
Results
The patients were divided into the fixation failure and the non-failure groups. Among the 83 patients, 17 cases (20.5%) of fixation failure after the primary internal fixation of the FNF were identi-fied. When comparing the two groups according to the radiographic data, Pauwels’ angle and the reduction quality based on Garden’s angle showed significant differences (p<0.001). Moreover, when comparing the intraoperative variables, unlike the surgical time and estimated blood loss, significant differences were noted in the time interval from injury to surgery and specifically in whether the surgery was performed within 12 hours after injury (p<0.001).
Conclusion
Pauwels’ angle, reduction quality, and time to surgery are the major factors that can predict the possibility of internal fixation failure of the FNF. Early and accurate anatomical reduction is needed to decrease complications after the internal fixation of the FNF. -
Citations
Citations to this article as recorded by- Factors associated with implant- and bone-related complications and fixation-failure–related readmissions after internal fixation for femoral neck fractures in young and middle-aged adults: a population-based study
Jiong Mei
International Orthopaedics.2026;[Epub] CrossRef
- Factors associated with implant- and bone-related complications and fixation-failure–related readmissions after internal fixation for femoral neck fractures in young and middle-aged adults: a population-based study
- 3,897 View
- 50 Download
- 1 Crossref
- Comparison of Clinical Outcomes for Femoral Neck System and Cannulated Compression Screws in the Treatment of Femoral Neck Fracture
- Jae Kwang Hwang, KiWon Lee, Dong-Kyo Seo, Joo-Yul Bae, Myeong-Geun Song, Hansuk Choi
- J Korean Fract Soc 2023;36(3):77-84. Published online July 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.3.77
-
Abstract
PDF
- Purpose
This study compared the clinical and radiological results of the femoral neck system (FNS) and cannulated compression screws (CCS) for the fixation of femoral neck fractures.
Materials and Methods
Patients who underwent FNS or CCS internal fixation for femoral neck fractures between January 2016 and January 2022 were analyzed retrospectively. The hip joint function using the Harris hip score (HHS) was evaluated three months and one year after surgery. The operation time, fracture healing time, and associated surgical complications in the two groups were compared and analyzed statistically.
Results
Seventy-nine patients were categorized into 38 FNS and 41 CCS groups. The FNS group had a longer operation time and higher postoperative HHS at three months (p<0.01). Femoral neck shortening was lower in the FNS group (p=0.022). There were no significant differences in the fracture healing time and other complications.
Conclusion
There were no differences in most clinical outcomes and complications between the two groups except for the three-month HHS and femoral neck shortening. This study suggests that FNS could be an alternative to CCS for treating femoral neck fractures.
- 1,630 View
- 30 Download
Technical Note
- Usefulness of Reduction and Internal Fixation Using a 2.4 mm Hand Plating System in Type AO 33-A3 Distal Femur Fracture - Technical Note -
- Bong-Ju Lee, Ja-Yeong Yoon, Seungha Woo
- J Korean Fract Soc 2023;36(1):25-28. Published online January 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.1.25
-
Abstract
PDF
- Open reduction in an AO 33-A3 class distal femur transverse and comminuted fracture is often difficult due to frequent reduction loss during surgery, leading to longer operative time and increased blood loss intra-operation. In this study, the authors report a case in which the use of an offset grid plate (OsteoMed, USA) using 2.4 mm HPS (hand plating system) eased the process of fracture reduction and achieved a stable internal fixation, ultimately leading to successful osteosynthesis. The authors experienced no need for temporary fixation devices such as K-wires or screws, which are otherwise required to stabilize the reduction. The fracture reduction was stable throughout the primary fixation of the fracture using a locking plate and screws. The authors report that the advantage of the HPS plate is fitting into the cortical contour and providing stable maintenance of fracture reduction intra-operation, which would be beneficial in certain distal femoral fracture patterns.
- 874 View
- 9 Download
Original Articles
- Distal Femur Fractures Treated with Distal Femoral Locking Plate Fixation: A Retrospective Study of One Year Mortality and Risk Factors
- Kwang-Hwan Jung, Yoon-Seok Youm, Seung-Hyun Jung, Jae-Min Oh, Ki Bong Park
- J Korean Fract Soc 2023;36(1):10-16. Published online January 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.1.10
-
Abstract
PDF
- Purpose
This study examined the one-year mortality after locking plate fixation for distal femur fractures and the risk factors related to death.
Materials and Methods
From July 2011 to June 2020, 128 patients who underwent locking plate fixation for distal femur fractures were analyzed retrospectively. Epidemiologic information of the patients, characteristics related to fracture and surgery, and death were investigated. The risk factors related to death were investigated using Cox analysis, and a subgroup analysis was also performed based on the age of 65 years.
Results
The one-year mortality rate after locking plate fixation for distal femur fractures was 3.9%, and the mortality rates in patients younger than 65 years and older than 65 years were 0% and 6.7%, respectively. There were no significant risk factors related to death in the total population. On the other hand, in patients aged 65 years or older, however, high-energy fracture and high comorbidity index increased the risk of death after surgery by 6.9-fold and 1.9-fold, respectively.
Conclusion
The one-year mortality rate for the total patients was 3.9%, but the mortality rate for patients over 65 years of age increased to 6.7%. High-energy fractures and high comorbidity index were risk factors related to death after surgery for distal femur fractures in patients aged 65 years or older.
- 887 View
- 5 Download
- Computational Simulation of Femoral Neck System and Additional Cannulated Screws Fixation for Unstable Femoral Neck Fractures and the Biomechanical Features for Clinical Applications
- Ju-Yeong Kim
- J Korean Fract Soc 2023;36(1):1-9. Published online January 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.1.1
-
Abstract
PDF
- Purpose
To identify the biomechanical features for clinical applications through a computational simulation of the fixation of the Femoral Neck System (FNS) with additional cannulated screws for a Pauwels type III femoral neck fractures.
Materials and Methods
Thirty cadaveric femurs underwent computed tomography, and the images were transferred to the Mimics ® program, resulting in three-dimensional proximal femur models. A three-dimensional scan of the FNS and 6.5 mm and 7.0 mm cannulated screws was performed to enable computerized virtual fixation of FNS with additional cannulated screws for unstable femoral neck fractures. Furthermore, the cannulated screw used for additional fixation was modeled and used as a cylinder within the Ansys program. The biomechanical characteristics of these models were investigated by applying a physiological load virtually.
Results
The maximum von Mises stress value at bone was 380.14 MPa in FNS and 297.87 MPa in FNS+7.0 mm full-thread cannulated screw. The maximum von Mises stress value at FNS was 786.83 MPa in FNS and 435.62 MPa in FNS+7.0 mm full-thread cannulated screw. The FNS group showed the highest maximum von Mises stress values at bone and FNS. For total deformation, the maximum deformation value was 10.0420 mm in FNS and 9.2769 mm in FNS+7.0 mm full-thread cannulated screws. The FNS group represented the highest maximum deformation compared to the other groups.
Conclusion
Considering the anatomical spatiality and biomechanical characteristics of the FNS in unstable femoral neck fractures, when one 7.0 mm full thread cannulated screw was also fixed to the anterosuperior portion of the FNS, significant biomechanical stability was demonstrated.
- 1,283 View
- 14 Download
- Comparison of the Clinical and Radiological Outcomes of TFNA (Trochanteric Fixation Nail-Advanced) and PFNA-II (Proximal Femoral Nail Antirotation-II) Treatment in Elderly Patients with Intertrochanteric Fractures
- Min Sung Kwon, Young Bok Kim, Gyu Min Kong
- J Korean Fract Soc 2022;35(4):162-168. Published online October 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.4.162
-
Abstract
PDF
- Purpose
Trochanteric fixation nail advanced (TFNA) was modified to compensate for the shortcomings of proximal femoral nail antirotation-II (PFNA-II). The clinical and radiological outcomes of surgeries us-ing the PFNA-II and TFNA for femoral intertrochanteric fractures were compared.
Materials and Methods
Eighty-two patients who underwent surgeries using PFNA-II or TFNA were analyzed. Only those who were followed up for more than a year were enrolled. Bone union, shortening of the femoral neck, and the tip–apex distance of the intramedullary nail were compared in the radiological findings. Clinical outcomes, including the frequency of complications and gait ability (Koval score), were also assessed.
Results
The mean follow-up periods were 22 and 19 months for the PFNA-II and TFNA groups, re-spectively. In the PFNA-II group, two cases of femoral head cut-out and one case of varus collapse were observed. In the TFNA group, only one case of femoral head cut-out was observed; however, there was no significant difference in the frequency of complications between the two groups (p=0.37). Ad-ditionally, both the shortening of the femoral neck and the decrease in gait ability after surgery showed relative improvement in the TFNA group compared to the PFNA-II group; however, there was no sig-nificant difference between the two groups.
Conclusion
The use of both TFNA and PFNA-II was associated with satisfactory outcomes. In patients who underwent surgeries using TFNA, the recovery of gait ability, frequency of complications, and short-ening of the femoral neck were not significantly different from PFNA-II, suggesting that both are suitable instrument choices for intertrochanteric fracture treatment. However, the clinical significance must be further assessed using a larger group of patients over a longer follow-up period in future studies. -
Citations
Citations to this article as recorded by- Treatment of Incompletely Displaced Femoral Neck Fractures Using Trochanteric Fixation Nail-Advanced in Patients Older Than 50 Years of Age
Jee Young Lee, Gyu Min Kong
Journal of Orthopaedic Trauma.2025; 39(7): 352. CrossRef - Clinical and Radiological Outcomes of Unstable Intertrochanteric Fractures Treated with Trochanteric Fixation Nail-Advanced and Proximal Femoral Nail Antirotation-II: Correlation between Lateral Sliding of the Helical Blade and Lateral Trochanteric Pain
Sung Yoon Jung, Myoung Jin Lee, Lih Wang, Hyeon Jun Kim, Dong Hoon Sung, Jun Ha Park
Journal of the Korean Orthopaedic Association.2024; 59(3): 208. CrossRef
- Treatment of Incompletely Displaced Femoral Neck Fractures Using Trochanteric Fixation Nail-Advanced in Patients Older Than 50 Years of Age
- 6,291 View
- 79 Download
- 2 Crossref
Case Report
- Insufficiency Fracture of Simultaneously Bilateral Femur Neck in Patient Treated with Long-Term Bisphosphonate Treatment - A Case Report -
- Seong Kee Shin, Hyung Gon Ryu, Dae Won Shin, Beom Su Han
- J Korean Fract Soc 2022;35(3):109-113. Published online July 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.3.109
-
Abstract
PDF
- Bisphosphonate is used widely for osteoporosis management. On the other hand, some studies have reported that prolonged use of bisphosphonate without a proper resting period can cause insufficiency fracture and, in rare cases, fractures on the femur neck. This paper reports a case of an elderly patient who suffered bilateral femur neck insufficiency fractures induced by non-stopped long-term bisphosphonate therapy. The patient complained of pain in her buttocks at the first visit. During the admission period, inguinal area pain newly developed. Both a femur neck insufficiency fracture was observed on the hip radiographic image. Hip pinning and postoperative parathyroid hormone treatment were performed. The patient was discharged without specific complications and reported improvement in symptoms on the last follow-up. Several authors have reported one-sided femoral neck insufficiency fractures due to bisphosphonate use, but the present case is uncommon in that it occurred simultaneously in both femur necks. In addition, in the case of bilateral femur fractures, the walking ability after surgery is lower than that of one-sided fracture cases, so active rehabilitation is necessary.
- 931 View
- 5 Download
Original Articles
- Mortality-Related Risk Factors in Total Hip Arthroplasty for Femoral Neck Fractures in Elderly Patients
- Jae Sung Suh, Hyung Gon Ryu, Young Ju Roh, Dae Won Shin
- J Korean Fract Soc 2022;35(2):51-56. Published online April 30, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.2.51
-
Abstract
PDF
- Purpose
Total hip arthroplasty (THA) using dual mobility components (DMC) is a reasonable surgical option for displaced femoral neck fractures in elderly patients, resulting in lower dislocation rates and improved stability. The purpose of this study was to investigate the clinical outcomes and risk factors responsible for mortality in elderly patients who were diagnosed with a displaced femoral neck fracture and had undergone DMC-THA.
Materials and Methods
Out of 147 cases of THA from December 2018 to June 2020, a total of 79 cases were enrolled in this study, with the following characteristics: (1) Garden stage III or IV, (2) over 75 years of age, and (3) over 1 year of follow-up. All the patients received DMC-THA surgery using the anterolateral approach.
Results
The mean follow-up period was 15.0±8.43 months and a total of one dislocation case was observed. The mortality rate was 17.7% (14/79), and it was especially higher in patients with a past medical history of malignancy (odds ratio [OR]=7.18, p=0.03) or a cognitive disorder such as dementia (OR=5.48, p=0.03). Preoperative low initial hemoglobin levels (OR=0.65, p=0.04) and low UCLA (Uni-versity of California at Los Angeles) score (OR=0.47, p=0.02) were also associated with mortality.
Conclusion
When considering THA as a treatment approach in elderly patients with a displaced femoral neck fracture, a high mortality rate is expected in patients with low preoperative hemoglobin levels or a history of malignancy or cognitive disorders. Hence, thorough monitoring and management should be undertaken before and after surgery. -
Citations
Citations to this article as recorded by- Comparison of Operation Time, Vital Signs, Bleeding Tendency, and Recovery Time Based on Anesthesia Methods in Patients Undergoing Hip Fracture Surgery
Je Bog Yoo, Woo Young In, Chang Ok Pyo, Jeung Hee Kwon, Min Ji Lee, Kwang Hee Kim, Kyoung Ok Kim, Mi Yu
Journal of PeriAnesthesia Nursing.2026; 41(3): 591. CrossRef
- Comparison of Operation Time, Vital Signs, Bleeding Tendency, and Recovery Time Based on Anesthesia Methods in Patients Undergoing Hip Fracture Surgery
- 834 View
- 29 Download
- 1 Crossref
- Surgical Treatment of AO/OTA 33-C Intra-Articular Distal Femoral Fractures through Parapatellar Approach
- Suk Kyu Choo, Sung Tan Cho, Hyoung Keun Oh
- J Korean Fract Soc 2022;35(1):1-8. Published online January 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.1.1
-
Abstract
PDF
- Purpose
To report the surgical results of the parapatellar approach for AO/OTA 33-C distal femoral intra-articular fractures.
Materials and Methods
Twenty-one patients with AO/OTA 33-C distal femoral intra-articular fracture were included. There were 11 cases of C2 and 10 cases of C3 fractures. The time of union and the coronal alignment were radiographically investigated. The complications related to surgery were clinically investigated, and a functional evaluation using the range of motion and Oxford knee score was performed to compare the surgical results according to fracture classification.
Results
In all cases, sufficient articular exposure and anatomical reduction were achieved with the parapatellar approach. No cases of coronal malalignment, loss of reduction, and plate failure were noted. On the other hand, in four cases (19.0%), an autogenous bone graft was performed due to delayed union on the meta-diaphyseal fracture site. There were no differences in the radiological and clinical outcomes of the C2 and C3 fractures. The knee joint pain and Oxford knee score were poorer in the delayed union group than the normal union group.
Conclusion
The parapatellar approach is useful for achieving an anatomical reduction of the articular surface of the distal femur and minimally invasive plating technique. Although satisfactory surgical results could be obtained regardless of the degree of articular comminution, a study of the risk factors of delayed metaphyseal fusion may be necessary.
- 918 View
- 5 Download
Case Report
- Helical Blade Locking Sleeve Disassembly Following Failed Femur Intertrochanter Fracture
- Soon Ho Huh, Hong-Man Cho, Ji-Yeon Park
- J Korean Fract Soc 2021;34(3):112-116. Published online July 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.3.112
-
Abstract
PDF
- A helical blade type of hip screw is used widely for the operative management of femoral trochanteric fractures. A 73-year-old female patient was admitted for femoral trochanteric fracture AO/OTA type 31A2.2. A helical blade locking sleeve dissembled 18 weeks after surgery did not achieve accurate reduction. The patient underwent bipolar hip hemiarthroplasty because the fracture reduction was lost, and it was impossible to remove the remaining helical blade without bone loss. The authors report this case of a rare complication of helical blade.
- 957 View
- 4 Download
Original Articles
- Clinical and Radiologic Outcome of Intertrochanteric Fracture Treatment Using TFNA (Trochanteric Fixation Nail-Advanced)
- Hyeon Joon Lee, Hyun Bai Choi, Ba Rom Kim, Seung Hwan Jo, Sang Hong Lee
- J Korean Fract Soc 2021;34(3):105-111. Published online July 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.3.105
-
Abstract
PDF
- Purpose
This study evaluated the clinical and radiological outcomes of TFNA (Trochanteric Fixation NailAdvanced; Depuy Synthes) for the treatment of proximal femur fractures.
Materials and Methods
This was a retrospective study of 64 patients diagnosed with a proximal femur fracture from January 2019 to November 2019. The patient’s demographic data, preoperatively and postoperatively Koval grade, modified Harris hip score, EQ-5D (Euro-Qol-5 Dimension), sliding and advancement of the blade, radiologic outcome, and complications were investigated.
Results
Fifty patients were available for evaluation at one year postoperatively. The patients reported the following: the Koval grade decreased after surgery; the modified Harris hip score decreased from 78.56±8.88 to 72.74±6.59 (p=0.149); the mean EQ-5D decreased from 0.75±0.09 to 0.72±0.06 (p=0.000). Satisfactory reduction was achieved on a postoperative radiographic examination in 47 patients in six months. Complications occurred in seven cases.
Conclusion
TFNA is considered an appropriate implant for treating intertrochanteric fractures of the femur with a minimum follow-up of one year. -
Citations
Citations to this article as recorded by- Outcomes of Intertrochanteric Fracture Fixation Using the Trochanteric Fixation Nail Advanced (TFNA): A Retrospective Analysis
Ramprasad Jasti, Prithvi Mohandas, Mahesh K Ragavan, Sunil D Magadam, Umesh Kannadasan
Cureus.2025;[Epub] CrossRef - GS Hip Nail versus Affixus Hip Fracture Nail for the Intramedullary Nailing of Intertrochanteric Fractures
Seungcheol Kwon, Minjae Lee, Heeyeon Lee, Jihyo Hwang
Journal of Clinical Medicine.2023; 12(21): 6720. CrossRef - Comparison of the Clinical and Radiological Outcomes of TFNA (Trochanteric Fixation Nail-Advanced) and PFNA-II (Proximal Femoral Nail Antirotation-II) Treatment in Elderly Patients with Intertrochanteric Fractures
Min Sung Kwon, Young Bok Kim, Gyu Min Kong
Journal of the Korean Fracture Society.2022; 35(4): 162. CrossRef
- Outcomes of Intertrochanteric Fracture Fixation Using the Trochanteric Fixation Nail Advanced (TFNA): A Retrospective Analysis
- 2,091 View
- 34 Download
- 3 Crossref
- Comparison of Reductions of Left and Right Proximal Portions of Intertrochanteric Fractures Treated by Intramedullary Nailing
- Hyun Cheol Oh, Joong Won Ha, Yung Park, Sang Hoon Park, Han Kook Yoon
- J Korean Fract Soc 2021;34(2):64-70. Published online April 30, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.2.64
-
Abstract
PDF
- Purpose
This study examined the effect of lag screw insertion on proximal fragments by separating the right and left sides of intertrochanteric fractures in elderly patients that underwent intramedullary nailing.
Materials and Methods
Patients aged ≥65 years that underwent intramedullary nailing after a diag-nosis of intertrochanteric fractures during the period February 2012 to May 2016 were included in the study. The subjects were divided into right and left side groups. The effect of the clockwise rotational force generated when a lag screw was inserted on the proximal fragment was evaluated in both groups.
Results
In the right and left groups, most proximal fragments were located in the intramedullary canal after surgery (45 cases [75.0%] and 67 cases [73.6%], respectively). Clockwise rotation due to lag screw placement in the right group occurred in two cases (3.3%), which both showed internal rotation, and in four cases (4.4%) in the left group, all of which showed external rotation.
Conclusion
After intramedullary nailing of intertrochanteric fractures in elderly patients, proximal fragments were mostly located in the intramedullary cavity. The results obtained confirmed that the clockwise rotational force generated by lag screw insertion did not affect left or right sides. -
Citations
Citations to this article as recorded by- Which side should be taken care of when positioning a lag screw in intertrochanteric femoral fracture: right or left?
Min Uk Do, Kyeong Baek Kim, Sang-Min Lee, Hyun Tae Koo, Won Chul Shin
European Journal of Trauma and Emergency Surgery.2025;[Epub] CrossRef - Midterm Outcomes of Intramedullary Fixation of Intertrochanteric Femoral Fractures Using Compression Hip Nails: Radiologic and Clinical Results
You-Sung Suh, Jae-Hwi Nho, Min Gon Song, Dong Woo Lee, Byung-Woong Jang
Clinics in Orthopedic Surgery.2023; 15(3): 373. CrossRef
- Which side should be taken care of when positioning a lag screw in intertrochanteric femoral fracture: right or left?
- 1,133 View
- 6 Download
- 2 Crossref
- Comparison of the U-Blade Gamma3 Nail and the Zimmer Natural Nail for the Treatment of Intertrochanteric Fracture
- Jae Sung Suh, Hyung-Gon Ryu, Young Ju Roh, Dae Won Shin, Sang-Min Kim
- J Korean Fract Soc 2021;34(2):57-63. Published online April 30, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.2.57
-
Abstract
PDF
- Purpose
This study was performed to compare the clinical results and radiological follow-up differences between intertrochanteric fractures treated with the U-blade Gamma3 nail or the Zimmer natural nail (ZNN).
Materials and Methods
The medical records of 129 cases diagnosed with an intertrochanteric frac-ture (90 cases of U-blade Gamma3 nail, 39 cases of ZNN) from July 2015 to December 2018 were reviewed. Patients were assigned to a U-blade Gamma3 nail (n=39) or a ZNN (n=39) group. To reduce selective bias, groups were subjected to Propensity score matching by age, body mass index, bone mineral density, and fracture type. Patients that met the following criteria were excluded; age <65 years, non-ambulatory, high energy or pathologic fracture, and a follow-up of <6 months. Operation times, estimated blood losses, preoperative and postoperative Koval grades, Harris hip score and radiological lag screw positions in the femoral head, reduction quality, cut-out, tip-apex distance (TAD), lag screw sliding distances, and times to union were compared.
Results
Clinical results were similar in the two groups, but lag screw TAD was significantly greater in Ublade Gamma3 nail group (23.4 mm vs. 21.0 mm) (p=0.042). One case of cut-out occurred in the Ublade Gamma3 nail group, but no other nail-related postoperative complication was noted.
Conclusion
No significant difference was observed between the outcomes of U-blade Gamma3 nail or ZNN treatments of intertrochanteric fractures. We conclude that the U-blade confers no specific advan-tage.
- 2,048 View
- 10 Download
- Comparison of the Clinical and Radiographic Results between 125° and 130° Caput-Collum-Diaphyseal Angle Proximal Femoral Nail Anti-Rotation II in Patients with Intertrochanteric Fracture
- Soo Jae Yim, Yong Bok Park, Hyun Kwon Kim, Sin Hyung Park
- J Korean Fract Soc 2020;33(4):210-216. Published online October 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.4.210
-
Abstract
PDF
- Purpose
This study compared the clinical and radiographic results of two proximal femoral nail antirotation II (PFNA-II) angled by 125° and 130° in patients with intertrochanteric fractures.
Materials and Methods
From March in 2015 to September in 2016, 65 patients who underwent a closed reduction and internal fixation with PFNA-II for a femoral intertrochanteric fracture were evaluated retrospectively. The minimum follow-up period was two years. Of those, 30 and 35 patients underwent 125° angled PFNA-II and 130° angled PFNA-II, respectively. The clinical performance was evaluated using the Harris hip score, WOMAC (Western Ontario and McMaster Universities Osteoarthrtis Index), and UCLA (University of California Los Angeles) score. Radiographic analyses were performed using standardized anteroposterior and lateral radiographs to assess the implant position and quality of reduction. The blade length, distance between the blade tip and the tip of the greater trochanter, and distance between the blade tip and the most lateral protrusion point of the greater trochanter in the two groups were measured and compared.
Results
The clinical results, including the Harris hip score, WOMAC, and UCLA, were similar in the two groups at the last follow-up postoperatively. In the radiography evaluation, the implant position, quality of reduction, and the blade length were similar in the two groups. The distances between the blade tip and the tip of the greater trochanter were 52.60±3.53 mm and 58.07±5.54 mm in the 125° angled PFNA-II and 130° angled PFNA-II groups, respectively. The distance between the blade tip and the most lateral protrusion point of greater trochanter were 16.48±2.54 mm and 21.19±4.43 mm in the 125° angled PFNA-II and 130° angled PFNA-II groups, respectively. The differences were significant (p=0.031, p=0.012).
Conclusion
The operation with the 125° angled PFNA-II showed a more superior and lateral position of the blade than that with the 130° angled PFNA-II. Nevertheless, lateral thigh pain can occur when the blade is positioned superolaterally.
- 1,023 View
- 9 Download
- Risk Factors Affecting the Early Complications of Femoral Head Fractures
- HoeJeong Chung, Jin-Woo Lee, Dong Woo Lee, Hoon-Sang Sohn
- J Korean Fract Soc 2020;33(4):204-209. Published online October 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.4.204
-
Abstract
PDF
- Purpose
This study analyzed the prognostic factors in patients with femoral head fractures by comparing two groups with and without complications.
Materials and Methods
A retrospective study was performed on femoral head fracture patients who visited two different level-1 trauma centers from January 1, 2014 to June 30, 2018. Thirty-three patients with a follow-up period of more than one year were included. Early complications were defined as fair or poor in the Thompson–Epstein clinical evaluation criteria and grades 3 or 4 in the Kellgren– Lawrence classification within one year after the fracture. The patients were divided into two groups, with and without early complications. Statistical analysis was performed for the nominal variables with a Fisher’s exact test and continuous variables using a Mann–Whitney U test.
Results
Nine patients (27.3%) had early complications, and there were no significant differences according to age, sex, treatment method, combined fractures, Pipkin classification, and AO/OTA classification between the two groups.
Conclusion
The prognosis in femoral head fractures is difficult to predict. Therefore, the validation of existing classifications or a new classification is necessary.
- 910 View
- 1 Download
- Retrospective Comparative Study of the Intraoperative Fracture Gap Compression in the Treatment of Intertrochanteric Fracture Using Proximal Femoral Nail Antirotation
- Se Jin Kim, Hong Man Cho, Jiyeon Park, Ki Yong An, Young Woo Chung, Woojin Shin
- J Korean Fract Soc 2020;33(4):179-188. Published online October 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.4.179
-
Abstract
PDF
- Purpose
Intertrochanteric fractures can be treated using proximal femoral nail antirotation (PFNA). This study examined the clinical and radiological results of the intraoperative fracture compression.
Materials and Methods
Ninety-four patients underwent intraoperative compression (Group I), and 88 patients underwent natural sliding only (Group II). The patients were followed-up for more than two years. All patients met the following seven conditions: (1) AO/OTA 31-A1, A2 type intertrochanter fracture, (2) availability of compression of more than one cortical bone in the anterior or medial region of the fracture site under the preoperative imaging test, (3) Singh index grade ≥3, (4) blade position: center-center, center-inferior, (5) tip-apex distance <25 mm, (6) reduction status of good or very good, and (7) positive or neutral medial cortical support position with slightly valgus reduction.
Results
A slight tendency toward significant differences in acute phase pain between the two groups was observed at six weeks postoperatively (p=0.073). Twenty-four months after surgery, lateral extension of the PFNA helical blade between the two groups showed significant differences (p=0.017). Fracture gaps measured immediately after surgery showed significant differences (p=0.001), and a clear tendency for a significant difference in the average fracture union time was found (p=0.065).
Conclusion
Intraoperative fracture compression, intraoperative fracture compression appears beneficial to achieve a successful union of trochanteric fractures provided that all conditions are met to apply the method safely. -
Citations
Citations to this article as recorded by- Benefits of a Demineralized Bone Matrix in Osteoporotic Intertrochanteric Femoral Fracture Patients
Se Jin Kim, Hong-Man Cho, Myung Cheol Jung
Journal of the Korean Fracture Society.2022; 35(4): 151. CrossRef
- Benefits of a Demineralized Bone Matrix in Osteoporotic Intertrochanteric Femoral Fracture Patients
- 1,331 View
- 4 Download
- 1 Crossref
Case Reports
- Rendezvous Surgery for Peri-Implant Fractures around Locking Compression Plate on Anterolateral Bowed Femur - A Case Report -
- Hong Man Cho, Jiyeon Park
- J Korean Fract Soc 2020;33(3):159-163. Published online July 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.3.159
-
Abstract
PDF
- An 84-year-old female visited with an intertrochanteric femoral fracture. The patient had undergone an open reduction and internal fixation with a compressive plate and elastic nail in an ipsilateral atypical diaphyseal femoral fracture in the past. Compressive plate and elastic nail remained, and anterolateral bowing was presented. To treat the periprosthetic trochanteric fracture, a proximal femoral nail was used without removing the previously inserted compressive plate. Under the “rendezvous” technique, using a combination of fixating intramedullary nail and compressive plate simultaneously, the distal screw was fixed, and a femoral head lag screw was inserted after reducing the fracture. Complete union of the fracture was achieved 16 months after the operation, and a decrease in mobility function was not found postoperatively. The authors report this case for the “rendezvous” technique as a treatment option for elderly patients with periprosthetic trochanteric fractures, who had previously undergone surgical treatment for ipsilateral atypical diaphyseal femoral fractures with anterolateral bowing.
- 814 View
- 8 Download
- Rare Experience of Bilateral Femoral Neck and Shaft Fractures - A Case Report -
- DaeHyun Choe, Jae-Ho Lee, Ki-Chul Park
- J Korean Fract Soc 2020;33(3):154-158. Published online July 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.3.154
-
Abstract
PDF
- Ipsilateral fractures of the femoral neck and shaft are relatively common injuries and accompany 2% to 9% of all femoral shaft fractures. On the other hand, it is extremely rare for these injuries to occur bilaterally. This paper reports the authors’ experience of a case with bilateral femoral neck and shaft fractures. The patient sustained multiple injuries, including liver laceration with hemoperitoneum, bilateral open fractures of the tibia, and bilateral femoral neck, and shaft fractures caused by a high-speed motor vehicle accident. Under the circumstances, damage-control orthopedic principles were applied, and external fixators were initially placed. After the patient’s general condition showed improvement, both femurs were fixed with a reconstruction nail. Fracture healing was achieved without complications, such as avascular necrosis of the femoral head. Despite the rare occurrence, this paper describes this case because these injuries must be managed with meticulous attention.
- 893 View
- 8 Download
Original Articles
- Clinical and Radiological Outcomes of Polished Cemented Bipolar Hemiarthroplasty for Intertrochanteric Fractures in Elderly Patients
- Suc-Hyun Kweon, Chang-Hyun Shin, Yeong-Chang Lee, Min-Woo Kim, Tae-Ho Kim
- J Korean Fract Soc 2020;33(3):134-141. Published online July 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.3.134
-
Abstract
PDF
- Purpose
To evaluate the clinical and radiological outcomes of bipolar hemiarthroplasty using a polished cemented femoral stem for intertrochanteric fractures in elderly patients.
Materials and Methods
From July 2005 to May 2015, 48 patients diagnosed with intertrochanteric fractures underwent bipolar hemiarthroplasty. The mean age and follow-up period were 80.5 years and 30.5 months, respectively. The postoperative results were evaluated clinically and radiologically.
Results
The mean operation time was 100 minutes (range, 90-120 minutes), and the mean amount of blood loss was 334 ml (range, 170-500 ml). At the last follow-up, the mean Harris hip score (HHS), visual analogue scale (VAS), and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores were 82.2 (range, 76-90), 0.8 (range, 1-3), and 36 (range, 30-40), respectively. Walking was initiated using a walker for partial weight-bearing, and the mean walking time was 5.8 days (range, 3-14 days). Ambulatory ability was restored to a walking state before the injury in 36 cases (75.0%), and wheelchair ambulation was possible in 12 cases (25.0%). The instrumental activities of daily living (IADLs) were 17 patients (35.4%), and the basic activities of daily living (BADLs) were 31 patients (64.6%).
Conclusion
Polished cemented bipolar hemiarthroplasty can achieve secure fixation with no postoperative thigh pain. Restoring the preoperative walking ability will be more helpful for intertrochanteric fractures in elderly patients.
- 1,238 View
- 9 Download
- Three-Dimensional Analysis of the Morphological Features in the Femur of Atypical Fracture and Practical Implications of Intramedullary Nailing
- Yong Uk Kwon, Kyung-Jae Lee, Joo Young Choi, Gu-Hee Jung
- J Korean Fract Soc 2020;33(2):87-95. Published online April 30, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.2.87
-
Abstract
PDF
- Purpose
This study analyzed the morphological features of the contralateral femur without an atypical fracture by constructing a three-dimensional model with an actual size medullary canal.
Materials and Methods
Lateral and anterior bowing of the shaft were measured for 21 models, and the shape of the medullary canal was analyzed. To eliminate the projection error, the anteroposterior (AP) femur was rotated internally to the extent that the centerline of the head and neck, which is the ideal position of cephalomedullary nail screw, was neutral, and the lateral femur matched the medial and lateral condyle exactly.
Results
The lateral bowing and anterior bowing was an average of 5.5° (range, 2.8°-10.7°; standard deviation [SD], 2.4°) and 13.1° (range, 6.2°-21.4°; SD, 3.2°), respectively. In the area where lateral bowing increased, the lateral cortex became thicker, and the medullary canal was straightened. On the lateral femur, the anterior angle was increased significantly, and the diameter of curvature averaged 1,370.2 mm (range, 896-1,996 mm; SD, 249.5 mm).
Conclusion
Even if the anterolateral bowing increases in the atypical femur, the medullary canal tends to be straightened in the AP direction. So, it might be considered as a reference to the modification of an intramedullary nail to increase the conformity.
- 817 View
- 6 Download
- Analysis of the Changes in Femoral Varus Bowing and the Factors Affecting Nonunion for the Treatment of Femoral Shaft Fractures over 60 Years Old Using Piriformis Fossa Insertion Intramedullary Nailing
- Yonghan Cha, Chan Ho Park, Jun-Il Yoo, Jung-Taek Kim, WooSuk Kim, Ha-Yong Kim, Won-Sik Choy
- J Korean Fract Soc 2020;33(2):65-71. Published online April 30, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.2.65
-
Abstract
PDF
- Purpose
This study examined the bony morphological changes to analyze the factors affecting bony union in the treatment of elderly femoral shaft fractures with varus bowing using piriformis fossa insertion intramedullary nailing.
Materials and Methods
This study included 26 patients over 60 years of age, who were admitted for femoral shaft fractures between January 2005 and December 2014 and treated with piriformis fossa insertion intramedullary nailing. Age, sex, height, weight, bone mineral density, injury mechanism, fracture type, diameter and length of the nail, postoperative lengthening of the femur, postoperative change in varus angle, contact between the lateral and anterior cortex, and the gap between the fracture line and the bony union were checked. The patients were divided into a varus group and nonvarus group, as well as a bone union group and nonunion group. Logistic regression analysis was performed to analyze the factors affecting nonunion.
Results
The patients were classified into 11 in the varus group and 15 in the non-varus group and 24 in the union group and 2 in the nonunion group. The varus group showed a larger increase in leg length and varus angle reduction than the non-varus group (p<0.05). The union group had more contact with the lateral cortical bone than that of the nonunion group (p<0.05). The factor affecting bone union in regression analysis was contact of the lateral cortical bone (p<0.05).
Conclusion
Treatment of a femoral shaft fracture in elderly patients with a varus deformity of the femur using piriformis fossa insertion intramedullary nail increases the length of the femur and decreases the varus deformity. For bony union, the most important thing during surgery is contact of the lateral cortical bone with the fracture site. -
Citations
Citations to this article as recorded by- Straight nail insertion through a laterally shifted entry for diaphyseal atypical femoral fractures with bowing: good indications and limitations of this technique
Seong-Eun Byun, Young-Ho Cho, Young-Kyun Lee, Jung-Wee Park, Seonguk Kim, Kyung-Hoi Koo, Young Soo Byun
International Orthopaedics.2021; 45(12): 3223. CrossRef
- Straight nail insertion through a laterally shifted entry for diaphyseal atypical femoral fractures with bowing: good indications and limitations of this technique
- 1,826 View
- 9 Download
- 1 Crossref
Review Article
- Treatment of Periprosthetic Femoral Fractures after Hip Arthroplasty
- Jung Hoon Choi, Jong Hyuk Jeon, Kyung Jae Lee
- J Korean Fract Soc 2020;33(1):43-51. Published online January 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.1.43
-
Abstract
PDF
- Although the incidence of postoperative periprosthetic femoral fractures after hip arthroplasty is expected to increase, these complex fractures are still challenging complications. To obtain optimal results for these fractures, thorough clinical and radiographic evaluation, precise classification, and understanding of modern management principles are mandatory. The Vancouver classification system is a simple, effective, and reproducible method for planning proper treatments of these injuries. The fractures associated with a stable femoral stem can be effectively treated with osteosynthesis, though periprosthetic femoral fractures associated with a loose stem require revision arthroplasty. We describe here the principles of proper treatment for the patients with periprosthetic femoral fractures as well as how to avoid complications.
- 2,148 View
- 16 Download
Original Articles
- Failure of Intramedullary Nailing for Subtrochanteric Atypical Femoral Fractures Caused by Endosteal Cortical Thickening
- Young Ho Roh, Kimoon Kang, Hee Joong Kim, Kwang Woo Nam
- J Korean Fract Soc 2019;32(4):211-221. Published online October 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.4.211
- Correction in: J Musculoskelet Trauma 2020;33(1):63
-
Abstract
PDF
- PURPOSE
Recent literature has noted incidences of subtrochanteric atypical femoral fractures (AFFs) in patients who have taken long-term bisphosphonates (BPs). Most cases of subtrochanteric AFFs have been treated with intramedullary nailing and cases of delayed union have been reported. On the other hand, there is no data available on the complications associated with endosteal thickening or cortical thickening. This study evaluated the results of surgical treatment according to the endosteal thickening of the lateral cortex in subtrochanteric AFFs.
MATERIALS AND METHODS
Investigation was performed at the Department of Orthopaedic Surgery, Jeju National University Hospital. The study consisted of patients with subtrochanteric AFFs, defined by the American Society for Bone and Mineral Research (ASBMR) major criteria, who underwent intramedullary nailing from March 2012 to October 2014. The cases were categorized into two groups based on the presence of endosteal thickening. The evaluation included the demographic data, radiographic data of initial reduction state, and duration of BPs.
RESULTS
The demographic data and duration of BPs were similar in the two groups. On the other hand, varus reduction (Group I: 12.5% vs. Group II: 78.9%; p=0.001), delayed union (Group I: 0% vs. Group II: 70.0%; p=0.003), nonunion (Group I: 0% vs. Group II: 47.4%; p=0.017), and union time (Group I: 5.5 months vs. Group II: 8.3 months; p<0.001) were significantly different in the two groups.
CONCLUSION
Endosteal thickening of the lateral cortex in subtrochanteric AFFs was identified as an independent factor that decides the reduction of the fracture and nonunion. The endosteal thickening should be removed to obtain anatomical alignment for successful surgical results. -
Citations
Citations to this article as recorded by- Controlled bending of proximal femoral nails used in fractures of bowed femurs: biomechanical study with clinical application
Hong Moon Sohn, Suenghwan Jo
Medical Biological Science and Engineering.2022; 5(2): 63. CrossRef
- Controlled bending of proximal femoral nails used in fractures of bowed femurs: biomechanical study with clinical application
- 2,052 View
- 8 Download
- 1 Crossref
- Outcomes following Treatment of Geriatric Distal Femur Fractures with Analyzing Risk Factors for the Nonunion
- Soo young Jeong, Jae Ho Lee, Ki Chul Park
- J Korean Fract Soc 2019;32(4):188-195. Published online October 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.4.188
- Correction in: J Musculoskelet Trauma 2020;33(1):62
-
Abstract
PDF
- PURPOSE
Many international journals have published studies on the results of distal femoral fractures in elderly people, but only a few studies have been conducted on the Korean population. The aim of this study was to determine the factors that are associated with the outcomes and prognosis of fixation of distal femur fractures using the minimally invasive plate osteosynthesis (MIPO) technique in elderly patients (age≥60) and to determine the risk factors related witht he occurrence of nonunion.
MATERIALS AND METHODS
This study is a retrospective study. From January 2008 to June 2018, distal femur fracture (AO/OTA 33) patients who underwent surgical treatment (MIPO) were analyzed. A total of 52 patients were included in the study after removing 121 patients that met with the exclusion criteria. Medical records, including surgical records, were reviewed to evaluate the patients' underlying disease, bone mineral density, the number of days delayed from surgery, complications and mortality. In addition, follow-up radiographs were used to determine bone union, delayed union and nonunion.
RESULTS
The average time to achieve bone union was 19.95 weeks, the rate of nonunion was 20.0% (10/50) and the overall mortality was 3.8% (2/52). There were no significant differences in the clinical and radiological results of those patients with or without periprosthetic fracture. On the univariate analysis, which compared the union group vs. the nonunion group, no factors were identified as significant risk factors for nonunion. On the multiple logistic regression analysis, medical history of cancer was identified as a significant risk factor for nonunion (p=0.045).
CONCLUSION
The rate of nonunion is high in the Korean population of elderly people suffering from distal femur fracture, but the mortality rate appears to be low. A medical history of cancer is a significant risk factor for nonunion. Further prospective studies are required to determine other associated factors. -
Citations
Citations to this article as recorded by- Comparison of Clinical Outcomes for Femoral Neck System and Cannulated Compression Screws in the Treatment of Femoral Neck Fracture
Jae Kwang Hwang, KiWon Lee, Dong-Kyo Seo, Joo-Yul Bae, Myeong-Geun Song, Hansuk Choi
Journal of the Korean Fracture Society.2023; 36(3): 77. CrossRef
- Comparison of Clinical Outcomes for Femoral Neck System and Cannulated Compression Screws in the Treatment of Femoral Neck Fracture
- 2,210 View
- 9 Download
- 1 Crossref
- Safety and Effectiveness of the Anchor Augmentation with Bone Cement on Osteoporotic Femoral Fracture: A Systematic Reviews
- So Young Kim
- J Korean Fract Soc 2019;32(2):89-96. Published online April 30, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.2.89
-
Abstract
PDF
- PURPOSE
This paper reviewed the safety and effectiveness of anchor augmentation with bone cement in osteoporotic femoral fractures.
MATERIALS AND METHODS
A systematic review was conducted by searching multiple databases including five Korean databases, Ovid-MEDLINE, Ovid-EMBASE, and Cochrane Library. Safety was assessed through the incidence of complication. The effectiveness was assessed through the failure rate of anchor fixation, improvement of function and radiological assessment (sliding distance of lag screw and cutout). The safety and effectiveness of anchor augmentation with bone cement were assessed by reviewing all articles reporting on the treatment. Two researchers carried out independently each stage from the literature search to data extraction. The tools of Scottish Intercollegiate Guidelines Networks were used to assess the quality of studies.
RESULTS
Six studies were considered eligible. The safety results revealed a small amount of cement leakage (1 case), but no other severe complications were encountered. Regarding the effectiveness, the failure rate of anchor fixation was 16.7% and the Harris's hip score showed no significant improvement. The sliding distance of the anchor was similar in the cement augmentation group and non-cement group but there was no cutout.
CONCLUSION
The results of the assessment suggest that the safety is acceptable, but further research will be needed to verify the effectiveness of the treatment.
- 1,174 View
- 5 Download
- Results of Exchange Nailing in Hypertrophic Nonunion of Femoral Shaft Fracture Treated with Nailing
- Suenghwan Jo, Gwang Chul Lee, Sang Hong Lee, Jun Young Lee, Dong Hwi Kim, Sung Hae Park, Young Min Cho
- J Korean Fract Soc 2019;32(2):83-88. Published online April 30, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.2.83
-
Abstract
PDF
- PURPOSE
This study examined the outcomes of exchange nailing for the hypertrophic nonunion of femoral shaft fractures treated with intramedullary nailing as well as the factors affecting the treatment outcomes.
MATERIALS AND METHODS
From January 1999 to March 2015, 35 patients, who had undergone intramedullary nailing with a femoral shaft fracture and underwent exchange nailing due to hypertrophic nonunion, were reviewed. This study investigated the time of union and complications, such as nonunion after exchange nailing, and analyzed the factors affecting the results.
RESULTS
Bone union was achieved in 31 cases (88.6%) after exchange nailing and the average bone union period was 22 weeks (14–44 weeks). Complications included persistent nonunion in four cases, delayed union in one case, and superficial wound infection in one case. All four cases with nonunion were related to smoking, three of them were distal shaft fractures, and one was a midshaft fracture with underlying disease.
CONCLUSION
Exchange nailing produced satisfactory results as the treatment of hypertrophic nonunion after intramedullary nailing. Smoking is considered a factor for continuing nonunion even after exchange nailing. In the case of a distal shaft, where the intramedullary fixation is relatively weak, additional efforts are needed for stability.
- 1,447 View
- 15 Download
Review Article
- Locked Plating in Elderly Patients with Distal Femur Fracture: How to Avoid Complications?
- Chul Young Jang, Je Hyun Yoo
- J Korean Fract Soc 2019;32(2):112-119. Published online April 30, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.2.112
-
Abstract
PDF
- Distal femur fractures in elderly patients with osteoporosis are complicated because poor bone quality makes screw purchase and fixation less secure, presenting many clinical challenges to the orthopedic surgeon. Minimally invasive locked plating using an angularly stable locking compression plate has become an integral tool for achieving secure fixation in osteoporotic distal femur fractures with improved biomechanical performance. On the other hand, complications, such as implant failure and periplate fracture, have still occurred. This paper describes the principles of internal fixation in minimally invasive lateral locked plating in elderly patients with osteoporotic distal femur fractures as well as how to avoid complications.
- 1,784 View
- 33 Download
Case Report
- Cortical Perforation Misidentified with Medial Condylar Fracture of Femur in Total Knee Arthroplasty: Case Report
- Seung Suk Seo, Sang Won Moon
- J Korean Fract Soc 2019;32(1):52-55. Published online January 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.1.52
-
Abstract
PDF
- Intraoperative fracture in total knee arthroplasty (TKA) is a rare complication. However, when it happens, additional surgery to fix the fracture site is needed. Therefore, it is important to diagnose intraoperative fractures in TKA exactly. The authors experienced two cases of cortical perforation of medial femoral condyle misidentified as the fracture in TKA. Cortical perforation could be misdiagnosed as the fracture, which could lead to unnecessary surgery. This is the first report about cortical perforation in TKA. We report two cases of intraoperative cortical perforations and describe the radiological characteristics.
- 1,257 View
- 2 Download
Original Articles
- Treatment of the Proximal Femoral Fracture Using the New Design Cephalomedullary Nail: Prospective Outcomes Study
- Young Ho Roh, Joseph Rho, Kwang Woo Nam
- J Korean Fract Soc 2019;32(1):35-42. Published online January 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.1.35
-
Abstract
PDF
- PURPOSE
The aim of this study is to investigate the clinical performance and safety of Zimmer® natural nail cephalomedullary nail (ZNN CM nail) in the treatment of proximal femur fractures.
MATERIALS AND METHODS
The following research was conducted as a prospective, non-comparative, single center outcome study. Upon providing written informed consent, enrolled patients' data were collected and analyzed. Postoperative follow-up visits were scheduled at 6 weeks, 3 months, 6 months, and 1 year. Follow-up evaluation included radiographic assessment, physical examination, and quality of life and adverse events reports.
RESULTS
Thirty-nine patients were available for evaluation at one year postoperative. The patients reported the mean EuroQol-5 Dimension score increased after surgery: from 0.4 points at discharge (n=49) to 0.6 points at 1-year post-surgery (n=39). The mean Harris hip score also increased after surgery: from 56.3 points at discharge (n=49) to 72.1 points at 1 year (n=12). Bone union was seen in 64% (n=16) in 6 months and 95% (n=37) in 1 year.
CONCLUSION
The results of this 1-year follow-up study affirmed the effectiveness and safety of the ZNN CM nail in the treatment of proximal femur fractures. -
Citations
Citations to this article as recorded by- Clinical and Radiologic Outcome of Intertrochanteric Fracture Treatment Using TFNA (Trochanteric Fixation Nail-Advanced)
Hyeon Joon Lee, Hyun Bai Choi, Ba Rom Kim, Seung Hwan Jo, Sang Hong Lee
Journal of the Korean Fracture Society.2021; 34(3): 105. CrossRef - Treatment of Proximal Femur Fracture with a Newly Designed Nail: Trochanteric Fixation Nail-Advanced (TFNA)
Jae Youn Yoon, Ji Wan Kim
Journal of the Korean Fracture Society.2020; 33(4): 189. CrossRef
- Clinical and Radiologic Outcome of Intertrochanteric Fracture Treatment Using TFNA (Trochanteric Fixation Nail-Advanced)
- 1,576 View
- 0 Download
- 2 Crossref
- Results after Less Invasive Locking Plating in Intra-Articular Fractures of the Distal Femur
- Sung Hyun Kim, Sung Hyun Yoon, Hee Gon Park, Jae Uk Jung
- J Korean Fract Soc 2019;32(1):14-20. Published online January 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.1.14
-
Abstract
PDF
- PURPOSE
The purpose of this study was to determine the clinical outcomes after a less invasive locking plating technique in intra-articular fractures of the distal femur.
MATERIALS AND METHODS
This was a retrospective 19 case series of patients with distal femoral intraarticular fractures treated with a less invasive locking plating technique in a single center (Dankook University Hospital) from June 2010 to April 2016. Nineteen patients (11 males and 8 females) with a mean age of 55.9 years were enrolled. The functional outcomes were evaluated using the visual analogue scale (VAS), range of knee joint motion (flexion & extension), and Knee Society score. The radiology outcomes were evaluated with parameters measured in a plain radiograph (deviation angle of alignment axis on coronal and sagittal plane, mechanical lateral distal femur angle).
RESULTS
The mean follow-up period was 26.4 months (range, 12–72 months) and the mean duration to union was 15.94 weeks (range, 11–28 weeks). The mean VAS was 1.36 (range, 0–8) and the range of motion of the knee joint was extension 4.73° (range, 0°–30°) and flexion 107.36° (range, 60°–135°). The mean Knee Society score was 85.47 (range, 47–100). The mean deviation angle of the coronal alignment axis was 4.07° (range, 1.3°–8.8°), the mean deviation angle of the sagittal alignment axis was 3.23° (range, 0.7°–7.0°), and the mechanical lateral femoral angle was 87.75° (range, 82.8°–95.5°). Six patients had traumatic osteoarthritis at the final follow-up.
CONCLUSION
The purpose of this study was to evaluate the clinical and radiologic outcomes of intraarticular fractures of the distal femur in patients who underwent an anatomical reduction through an open reduction, and converted to an extra-articular fracture with rigid internal fixation. The results were relatively satisfactory.
- 950 View
- 3 Download
- Factors Affecting Posterior Angulation in Retrograde Intramedullary Nailing for Distal Femoral Fractures
- Hohyoung Lee, Ji Ho Jeong, Min Su Kim, Bum Soo Kim
- J Korean Fract Soc 2018;31(2):50-56. Published online April 30, 2018
- DOI: https://doi.org/10.12671/jkfs.2018.31.2.50
-
Abstract
PDF
- PURPOSE
To analyze the factors that cause a posterior angulatory deformity in the retrograde intramedullary nailing of distal femoral fractures.
MATERIALS AND METHODS
Fifty-five patients with distal femur fractures who were treated with retrograde intramedullary nailing were enrolled in this study. They were followed-up for at least one year postoperatively. The posterior angulatory deformity was evaluated according to the fracture location, pattern, and insertion point and the insertion point was compared with the ideal point derived from the radiographs of 100 normal adults. The correlation between the posterior angulation and the entry point of the nail was analyzed.
RESULTS
The posterior angulation was similar in terms of the fracture location; a meaningful difference was noted among the fracture patterns (p=0.047). The posterior angulation was significantly greater when the entry point was located more posteriorly, accepting a malreduced state (p=0.012).
CONCLUSION
Posterior angulation was smaller in the transverse fracture and the posterior location of the entry point from the apex of the Blumensaat's line increased the posterior angulation.
- 665 View
- 8 Download
- Computational Simulation of Multiple Cannulated Screw Fixation for Femoral Neck Fractures and the Anatomic Features for Clinical Applications
- Jin Hoon Jeong, Gu Hee Jung
- J Korean Fract Soc 2018;31(2):37-44. Published online April 30, 2018
- DOI: https://doi.org/10.12671/jkfs.2018.31.2.37
-
Abstract
PDF
- PURPOSE
To identify the anatomic features for clinical applications through a computational simulation of the fixation of three cannulated screws for a femoral neck fracture.
MATERIALS AND METHODS
Thirty cadaveric femurs underwent computed tomography and the images were transferred to the Mimics® program, resulting in three-dimensional proximal femur models. A three-dimensional scan of the 7.0 mm cannulated screw was performed to enable computerized virtual fixation of multiple cannulated screws for femoral neck fractures. After positioning the screws definitively for cortical support, the intraosseous position of the cannulated screws was evaluated in the anteroposterior image and axial image direction.
RESULTS
Three cannulated screws located at the each ideal site showed an array of tilted triangles with anterior screw attachment and the shortest spacing between posterior and central screws. The central screw located at the lower side was placed in the mid-height of the lesser trochanter and slightly posterior, and directed toward the junction of femoral head and neck to achieve medial cortical support. All the posterior screws were limited in height by the trochanteric fossa and were located below the vastus ridge, but the anterior screws were located higher than the vastus ridge in 10 cases. To obtain the maximum spacing of the anterior and posterior screws on the axial plane, they should be positioned parallel to the cervical region nearest the cortical bone at a height not exceeding the vastus ridge.
CONCLUSION
The position of cannulated screws for cortical support were irregular triangular arrangements with the anterosuperior apex. The position of the ideal central screw in the anteroposterior view was at the mid-height of the lesser trochanter toward the junction of the femoral head and neck, and the anterior and posterior screws were parallel to the neck with a maximal spread just inferior to the vastus ridge. -
Citations
Citations to this article as recorded by- Computational Simulation of Femoral Neck System and Additional Cannulated Screws Fixation for Unstable Femoral Neck Fractures and the Biomechanical Features for Clinical Applications
Ju-Yeong Kim
Journal of the Korean Fracture Society.2023; 36(1): 1. CrossRef
- Computational Simulation of Femoral Neck System and Additional Cannulated Screws Fixation for Unstable Femoral Neck Fractures and the Biomechanical Features for Clinical Applications
- 1,109 View
- 0 Download
- 1 Crossref
- The Determination of Optimal Entry Point for Proximal Femoral Nail Antirotation-II by Fluoroscopic Simulation: A Cadaveric Study
- Jin Hoon Jeong, Gu Hee Jung
- J Korean Fract Soc 2017;30(4):173-179. Published online October 31, 2017
- DOI: https://doi.org/10.12671/jkfs.2017.30.4.173
-
Abstract
PDF
- PURPOSE
This study seeks to determine the anatomically optimal entry point of proximal femoral nail antirotation-II (PFNA-II®) according to geographic features of Korean cadaveric femoral trochanters for successful reduction of osteoporotic proximal femoral fractures.
MATERIALS AND METHODS
Forty-three adult cadaveric femurs without previous fractures or surgeries were included. Anteroposterior (AP) and lateral images of all femurs and PFNA-II® were taken with an image intensifier. Using the image synthesis process via the image editing program (Adobe Photoshop CS6), the optimal entry point was verified and compared with the tip of the greater trochanter (GT) and the cervicotro-chanteric junction on AP images, as well as the width of the trochanter and the neck on lateral images.
RESULTS
The optimal entry point of PFNA-II® was an average distance of 9.1 mm (range, 7–15 mm) medially from the tip of GT on AP images. The center of the nail was located at an average of 30% (range, 21%–44%) area from the posterior margin of the middle neck, which is an average area of 38% (range, 26%–48%) from the posterior cortex of the trochanter on lateral images. Furthermore, the ideal entry point was at the extended line of the cervico-trochanteric junction.
CONCLUSION
The optimal entry point, which was found to be medial to the tip of the GT and posterior to the center of the middle femoral neck and the trochanter, was at on the extended line of the cervicotrochanteric junction. -
Citations
Citations to this article as recorded by- Clinical Research through Computational Anatomy and Virtual Fixation
Ju Yeong Kim, Dong-Geun Kang, Gu-Hee Jung
Journal of the Korean Orthopaedic Association.2023; 58(4): 299. CrossRef - Does the Entry Point of Proximal Femoral Nail Antirotation Affect the Malalignment of Intertrochanteric Fracture? A Cadaveric Study
Chittawee Jiamton, Nonpawit Nimmankiatkul, Pongsakorn Rungchamrassopa, Wichan Kanchanatawan, Pariyut Chiarapatanakom, Wirat Kongcharoensombat
Journal of Southeast Asian Orthopaedics.2022;[Epub] CrossRef
- Clinical Research through Computational Anatomy and Virtual Fixation
- 2,957 View
- 89 Download
- 2 Crossref
- The Role of Beta-Tricalcium Phosphate Graft in the Dynamic Hip Screw Fixation of Unstable Intertrochanter Fracture
- Chul Ho Kim, Ji Wan Kim, Eic Ju Lim, Jae Suk Chang
- J Korean Fract Soc 2016;29(4):250-257. Published online October 31, 2016
- DOI: https://doi.org/10.12671/jkfs.2016.29.4.250
-
Abstract
PDF
- PURPOSE
The purpose of this study was to introduce our method of stabilizing unstable intertrochanteric fractures by using the dynamic hip screw (DHS) with a beta-tricalcium phosphate (β-TCP) graft and to compare the outcomes of this procedure with those of the conventional DHS without β-TCP.
MATERIALS AND METHODS
Patients who underwent surgery by using DHS between March 2002 and January 2016 were retrospectively reviewed for analysis of the outcomes. The inclusion criteria were: 1) age of 60 years and older; 2) low-energy fracture resulting from a fall from no greater than the standing height; 3) multifragmentary pertrochanteric fracture (AO classification 31-A2.2, 2.3); and 4) follow-up of over 3 months. We compared 29 patients (29 hips) who underwent surgery, using DHS without β-TCP, with 29 age-sex matched patients (29 hips) who underwent surgery using DHS with grafted β-TCP granules to empty the trochanter area after reaming. We investigated the fracture union rate, union time, and length of lag screw sliding.
RESULTS
Bone union was achieved in all cases. The mean union time was 7.0 weeks in the β-TCP group and 8 .8 weeks in the non-β-TCP group. The length of lag screw sliding was 3.6 mm in the β-TCP group and 5 .5 mm in the non-β-TCP group. There were no implant failure cases in both groups.
CONCLUSION
The β-TCP graft for reinforcement DHS acquired satisfactory clinical outcomes for treating unstable intertrochanteric fractures.
- 721 View
- 4 Download
- The Mid-Term Result after Osteosynthesis of Intra-Articular Fractures of Distal Femur
- Sam Guk Park, Jeong Jae Moon, Oog Jin Shon
- J Korean Fract Soc 2016;29(4):242-249. Published online October 31, 2016
- DOI: https://doi.org/10.12671/jkfs.2016.29.4.242
-
Abstract
PDF
- PURPOSE
This study was to evaluate the radiological and clinical mid-term results and the presence of post-traumatic osteoarthritis after osteosynthesis in patients under the age of 50 years undergoing osteosynthesis for distal femur intra-articular fractures (AO/OTA 33-B & C) from high-energy trauma.
MATERIALS AND METHODS
Between January 2008 and January 2013, a total of twenty-one patients with more than three years of follow-up were enrolled. Recovery of the alignment of the lower extremity, union period, and the presence of post-traumatic osteoarthritis were confirmed by follow-up radiographs. Clinically, the range of motion, pain on fracture lesion, and Knee Society score (KSS) were evaluated.
RESULTS
The average duration of union was 18.2 weeks (10-28 weeks), and the alignment of the lower extremity was within normal range in all patients. Seven patients showed post-traumatic osteoarthritis at the final follow-up after more than three years. The presence of post-traumatic osteoarthritis was associated with the classification of fractures, coronal plane fracture, and age. The average range of motion, knee score among KSS, and function score at the last follow-up were 128.7°, 86.1, and 85.1, all showing a greater improvement when compared with the one-year follow-up scores.
CONCLUSION
The mid-term result was radiologically and clinically satisfactory. Furthermore, only 33.3% of patients showed a slight progress of post-traumatic osteoarthritis, which critically effects the prognosis. -
Citations
Citations to this article as recorded by- Incidence of nonunion after surgery of distal femoral fractures using contemporary fixation device: a meta‐analysis
Byung-Ho Yoon, In Keun Park, Youngwoo Kim, Hyoung-Keun Oh, Suk Kyu Choo, Yerl-Bo Sung
Archives of Orthopaedic and Trauma Surgery.2021; 141(2): 225. CrossRef
- Incidence of nonunion after surgery of distal femoral fractures using contemporary fixation device: a meta‐analysis
- 1,119 View
- 3 Download
- 1 Crossref
Case Report
- Medial Plating of Distal Femoral Fracture with Locking Compression Plate-Proximal Lateral Tibia: Cases' Report
- Se Ang Jang, Young Soo Byun, In Ho Han, Dongju Shin
- J Korean Fract Soc 2016;29(3):206-212. Published online July 31, 2016
- DOI: https://doi.org/10.12671/jkfs.2016.29.3.206
-
Abstract
PDF
- Generally, lateral plating is used for a comminuted fracture of the distal femur. However, in some cases, it has been shown that using a medial plate is necessary to achieve better outcome. Nevertheless, there are no available anatomical plates that fit either the distal medial femoral condyle or fracture fixation, except for the relatively short plate developed for distal femoral osteotomy. We found that locking compression plate-proximal lateral tibia (LCP-PLT) fits anatomically well for the contour of the ipsilateral medial femoral condyle. Moreover, LCP-PLT has less risk of breaking the thread holes since it rarely needs to be bent. We report a plastic bone model study and two cases of distal femoral fractures fixed with medial plating using LCP-PLT.
-
Citations
Citations to this article as recorded by- A novel anatomical locked medial femoral condyle plate: a biomechanical study
M. A. Ozer, S. Keser, D. Barıs, O. Yazoglu
European Journal of Orthopaedic Surgery & Traumatology.2024; 34(5): 2767. CrossRef - Medial plating of distal femur: which pre-contoured angular stable plate fits best?
Shaam Achudan, Rex Premchand Antony Xavier, Sze Ern Tan
European Journal of Orthopaedic Surgery & Traumatology.2024; 34(6): 3297. CrossRef - Medial augmentation of distal femur fractures using the contralateral distal femur locking plate: A technical note
Jaime Andrés Leal
OTA International.2024;[Epub] CrossRef - The missing piece of the trauma armoury-medial femoral condyle plate
Piyush Upadhyay, Farhan Syed, Darryl N Ramoutar, Jayne Ward
Injury.2022; 53(3): 1237. CrossRef - Surgical Tips and Tricks for Distal Femur Plating
Christopher Lee, Dane Brodke, Ajay Gurbani
Journal of the American Academy of Orthopaedic Surgeons.2021; 29(18): 770. CrossRef - Medial minimally invasive helical plate osteosynthesis of the distal femur – a new technique
G.M. Hohenberger, A.M. Schwarz, P. Grechenig, B. Clement, Mario Staresinic, Bore Bakota
Injury.2021; 52: S27. CrossRef - Feature-Based Design of Personalized Anatomical Plates for the Treatment of Femoral Fractures
Xiaozhong Chen, Zhijian Mao, Xi Jiang
IEEE Access.2021; 9: 43824. CrossRef
- A novel anatomical locked medial femoral condyle plate: a biomechanical study
- 2,646 View
- 127 Download
- 7 Crossref
Original Articles
- Surgical Treatment for Stable 2-Part Intertrochanteric Femur Fracture Using Dynamic Hip Screw with 2-Hole Side Plate in Elderly Patients
- Kyung Hoon Lee, Suk Ku Han, Seung Jae Chung, Jongho Noh, Kee Haeng Lee
- J Korean Fract Soc 2016;29(3):192-199. Published online July 31, 2016
- DOI: https://doi.org/10.12671/jkfs.2016.29.3.192
-
Abstract
PDF
- PURPOSE
The purpose of this study is to evaluate the postoperative outcomes of elderly patients with stable 2-part intertrochanteric femur fractures surgically treated using dynamic hip screw with 2-hole side plate.
MATERIALS AND METHODS
From February 2008 to January 2014, 50 patients older than the age of 65 years, who had been followed-up for more than 6 months after the operation at The Catholic University of Korea, Bucheon St. Mary's Hospital were enrolled. A clinical evaluation of the skin incision length, operating time, and ambulatory status, using Clawson's Ambulation Capacity Classification, was performed, and a radiologic evaluation of Fogagnolo reduction quality, tip-apex distance (TAD), Cleveland index, sliding extent of lag screws, time duration till bony union, and complications was also done.
RESULTS
The mean skin incision length was 9.8 cm (range, 8-13 cm), the mean operating time was 41.4 minutes (range, 30-60 minutes), and 32 patients recovered their ambulatory function. Forty-eight patients gained bony union, and the time lapsed till union was average 10.6 weeks (range, 8-16 weeks). The evaluation of postoperative radiologic images showed the following reduction statuses by the Fogagnolo classification: 46 cases of "Good", 3 cases of "Acceptable," and 1 case of "Poor." Moreover, the mean TAD was 18.9 mm (range, 9.0-24.9 mm). While 45 cases fit into the zone 5 of the Cleveland index, other 3 were within zone 8 and the other 2 were within zone 6. The mean sliding length of the lag screws were 4.9 mm (range, 0.1-19.4 mm). There were a case of nonunion and a case of periprosthetic infection with nonunion as complications.
CONCLUSION
Using dynamic hip screws with 2-hole side plate for stable 2-part intertrochanteric femur fractures in elderly patients showed satisfactory results with respect to the recovery of ambulatory functions and bony union.
- 811 View
- 0 Download
- Radiologic Assessment of Postoperative Stability in Unstable Intertrochanteric Fracture Using Lateral Radiograph
- Suc Hyun Kweon, Jin Yeong Park, Seng Hwan Kook, Byung Min Yoo
- J Korean Fract Soc 2016;29(3):171-177. Published online July 31, 2016
- DOI: https://doi.org/10.12671/jkfs.2016.29.3.171
-
Abstract
PDF
- PURPOSE
The purpose of this study was to compare the sliding distance of lag screw in patients with unstable femoral intertrochanteric fractures treated with intramedullary fixation using a cephalomedullary nail with a fixed angle between the neck and shaft of the femur in relation to reduction type by lateral radiographs.
MATERIALS AND METHODS
Between January 2009 to October 2013, 86 cases (86 patients) with unstable femoral intertrochanteric fractures were treated with intramedullary fixation using a metal nail with a fixed neck-shaft angle and followed for at least 6 months. We used AO/OTA classification, and all cases were unstable fractures. Twenty cases were 31-A22, 54 cases were 31-A23, and 12 cases were 31-A3. There were 30 men and 56 women. Average patient age was 73.7 years (range, 47-97 years). We classified reduction types into three groups as postoperative lateral radiologic findings. Group 1 showed no displacement, group 2 showed anterior displacement of the femur neck, and group 3 showed posterior displacement of the femur neck. The radiological assessment compared the sliding distance of the lag screw between postoperative X-ray and last follow-up X-ray.
RESULTS
Forty-two cases were in group 1, 22 cases were in group 2, and the other 22 cases were in group 3. There was no significant difference in the patient characteristics of each group. The sliding distances of the lag screw were 4.9±3.2 mm, 4.6±3.6 mm, and 8.5±4.9 mm, respectively, and group 3 showed a significant result (p<0.0001, p=0.024).
CONCLUSION
In cases treated with intramedullary fixation using a cephalomedullary nail with a fixed neck-shaft angle, appropriate reduction with a lateral radiograph before screw fixation is needed to prevent excessive lag screw sliding.
- 792 View
- 7 Download
Case Reports
- Breakage of Cephalomedullary Nail Used in the Treatment of Proximal Femur Fractures: Case Report
- Seok Hyun Kweon, Chang Hyun Shin, Jin Sung Park, Byoung San Choi
- J Korean Fract Soc 2016;29(1):42-49. Published online January 31, 2016
- DOI: https://doi.org/10.12671/jkfs.2016.29.1.42
-
Abstract
PDF
- Internal fixation using a cephalomedullary nail as treatment for proximal femur fracture has recently been popular for early ambulation and rehabilitation. However metal breakage at the lag screw insertion site was reported due to non-union, delayed-union, and early weight bearing. In our orthopedic department, we experienced 2 cases of nail breakage at the lag screw insertion site, therefore we report on evaluation of the cause of metal failure and prevention of complications with literature review.
-
Citations
Citations to this article as recorded by- Breakage of the Tail Portion of the Lag Screw during Removal of Proximal Femoral Zimmer Natural Nail: Report of Two Cases with Technical Notes
Asep Santoso, Ik-Sun Choi, Kyung-Soon Park, Taek-Rim Yoon
Hip & Pelvis.2017; 29(3): 199. CrossRef
- Breakage of the Tail Portion of the Lag Screw during Removal of Proximal Femoral Zimmer Natural Nail: Report of Two Cases with Technical Notes
- 1,139 View
- 5 Download
- 1 Crossref
- Iatrogenic Subtrochanteric Fractures Related to the Surgical Error: Two Cases Report
- Kook Jin Chung, June Young Jeon, Hyun Woo Na, Ji Hyo Hwang
- J Korean Fract Soc 2015;28(4):250-255. Published online October 31, 2015
- DOI: https://doi.org/10.12671/jkfs.2015.28.4.250
-
Abstract
PDF
- Iatrogenic fracture is not popular and might be recognized as a malpractice. Surgical error related to iatrogenic fracture which has occurred after an operation can be detected only by a surgeon. Stress riser fracture is another form of iatrogenic fracture also known as a Young's modulus fracture. As the majority of surgical related stress riser fractures can be preventive, the accurate prevalence is not known. The majority of fractures occurred in the weight bearing bones such as femur and tibia. The subtrochanter area is the most stress concentrated area in the human body, thus it is a common area for occurrence of stress riser iatrogenic fractures. We experienced 2 cases of stress riser iatrogenic fractures, which are related to technical errors, thus we report cases with literature review.
-
Citations
Citations to this article as recorded by- Mechanical and Physical Characteristics Analysis of Radius Trauma Plate by EBM Additive Manufacturing
Kwun-Mook Lim, Sung-Jun Park
Journal of the Korean Society of Manufacturing Technology Engineers.2020; 29(2): 147. CrossRef
- Mechanical and Physical Characteristics Analysis of Radius Trauma Plate by EBM Additive Manufacturing
- 914 View
- 2 Download
- 1 Crossref
Original Articles
- The Usefulness of Poller Screw with Antegrade Nailing in the Initial Treatment of Infraisthmal Femur Shaft Fracture
- Jeong Hyun Yoo, Hyoung Soo Kim, Chang Geun Kim, Ho Il Kwak, Sang Heon Song
- J Korean Fract Soc 2015;28(4):230-236. Published online October 31, 2015
- DOI: https://doi.org/10.12671/jkfs.2015.28.4.230
-
Abstract
PDF
- PURPOSE
The purpose of this study was to evaluate the radiologic and clinical outcomes after intramedullary nailing with Poller screw insertion at initial stage in infraisthmal femur shaft fractures.
MATERIALS AND METHODS
Seven consecutive patients (7 femurs) treated with antegrade intramedullary nailing with Poller screw insertion for the infraisthmal femur shaft fracture were reviewed retrospectively. There were 4 male and 3 female patients. Mean age was 46.1 years (20-72 years). Operative time including Poller screw insertion, time for union, malalignment, and range of motion were evaluated.
RESULTS
All 7 cases had primarily healed successfully. Mean time for radiologic union was 19.1 weeks (16-24 weeks) postoperatively. One case had 5 degree valgus malalignment. One case of 15 mm shortening was reported and he required shoe lift orthosis. All cases had a full range of motion in hip and knee joint.
CONCLUSION
Antegrade intramedullary nailing with Poller screw insertion is useful in the initial treatment of infraisthmal femur shaft fracture, because it could provide additional stability. An additional 20 minutes were required but a Poller screw should be considered according to the anatomic location of a femur shaft fracture.
- 795 View
- 7 Download
- A Comparison of Quality of Life Using Short Form 36 between Femoral Shaft Fracture and Tibia Shaft Fracture Treated with Antegrade Nailing
- Sangbong Ko, Hojin Chang
- J Korean Fract Soc 2015;28(3):163-168. Published online July 31, 2015
- DOI: https://doi.org/10.12671/jkfs.2015.28.3.163
-
Abstract
PDF
- PURPOSE
We sought to compare the quality of life between two similar groups of patients; one group who sustained an isolated femoral shaft fracture, and the other group who sustained an isolated tibial shaft fracture.
MATERIALS AND METHODS
From February 1995 to July 2010, two groups of 168 patients who underwent implant removal operations after intramedullary nailing for an isolated femoral shaft fracture or an isolated tibial shaft fracture were enrolled. Short Form 36 (SF-36) questionnaires were completed at the final follow-up visit. Data analysis was performed by another physician not otherwise involved with clinical evaluation or the surgeries.
RESULTS
Patients ranged in age from 18 to 37 years old. The two groups had similar characteristics, including age, gender ratio, body weight, smoking, and mean follow-up period (all p>0.05). No significant difference in functional outcome using SF-36 was observed between the groups except in the domain of physical functioning (PF) where femoral shaft fracture patients had a slightly higher score (p=0.002).
CONCLUSION
Femoral shaft fracture patients and tibial shaft fracture patients who underwent intramedullary nailing and subsequent implant removal after fracture union with similar epidemiological characteristics had similar functional outcomes using the SF-36 survey, except in the domain of PF, where femoral shaft fracture patients had a slightly better outcome. -
Citations
Citations to this article as recorded by- Health‐related quality of life outcomes after surgical treatment of atypical femur fractures: a multicenter retrospective cohort study
Jonathon Spanyer, Lauren A. Barber, Harrison Lands, Alexander Brown, Mary Bouxsein, Marilyn Heng, Madhusudhan Yakkanti
JBMR Plus.2021;[Epub] CrossRef
- Health‐related quality of life outcomes after surgical treatment of atypical femur fractures: a multicenter retrospective cohort study
- 1,124 View
- 1 Download
- 1 Crossref
 First
First Prev
Prev

