 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 33(2); 2020 > Article
- Original Article Three-Dimensional Analysis of the Morphological Features in the Femur of Atypical Fracture and Practical Implications of Intramedullary Nailing
- Yong Uk Kwon, Kyung-Jae Lee, Joo Young Choi, Gu-Hee Jung
-
Journal of Musculoskeletal Trauma 2020;33(2):87-95.
DOI: https://doi.org/10.12671/jkfs.2020.33.2.87
Published online: April 30, 2020
1Department of Orthopaedic Surgery, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea
2Department of Orthopaedic Surgery, Keimyung University Dongsan Hospital, Keimyung University School of Medicine, Daegu, Korea
3Institute of Health Sciences (Medical ICT Convergence Research Center), Gyeongsang National University College of Medicine, Jinju, Korea
4Department of Orthopaedic Surgery, Gyeongsang National University Changwon Hospital, Gyeongsang National University College of Medicine, Changwon, Korea
2Department of Orthopaedic Surgery, Keimyung University Dongsan Hospital, Keimyung University School of Medicine, Daegu, Korea
3Institute of Health Sciences (Medical ICT Convergence Research Center), Gyeongsang National University College of Medicine, Jinju, Korea
4Department of Orthopaedic Surgery, Gyeongsang National University Changwon Hospital, Gyeongsang National University College of Medicine, Changwon, Korea
- 840 Views
- 6 Download
- 0 Crossref
- 0 Scopus
Abstract
Purpose
This study analyzed the morphological features of the contralateral femur without an atypical fracture by constructing a three-dimensional model with an actual size medullary canal.
Materials and Methods
Lateral and anterior bowing of the shaft were measured for 21 models, and the shape of the medullary canal was analyzed. To eliminate the projection error, the anteroposterior (AP) femur was rotated internally to the extent that the centerline of the head and neck, which is the ideal position of cephalomedullary nail screw, was neutral, and the lateral femur matched the medial and lateral condyle exactly.
Results
The lateral bowing and anterior bowing was an average of 5.5° (range, 2.8°-10.7°; standard deviation [SD], 2.4°) and 13.1° (range, 6.2°-21.4°; SD, 3.2°), respectively. In the area where lateral bowing increased, the lateral cortex became thicker, and the medullary canal was straightened. On the lateral femur, the anterior angle was increased significantly, and the diameter of curvature averaged 1,370.2 mm (range, 896-1,996 mm; SD, 249.5 mm).
Conclusion
Even if the anterolateral bowing increases in the atypical femur, the medullary canal tends to be straightened in the AP direction. So, it might be considered as a reference to the modification of an intramedullary nail to increase the conformity.
J Korean Fract Soc. 2020 Apr;33(2):87-95. Korean.
Published online Apr 28, 2020.
https://doi.org/10.12671/jkfs.2020.33.2.87
Published online Apr 28, 2020.
https://doi.org/10.12671/jkfs.2020.33.2.87
Copyright © 2020 The Korean Fracture Society. All rights reserved.
Original Article
Three-Dimensional Analysis of the Morphological Features in the Femur of Atypical Fracture and Practical Implications of Intramedullary Nailing
Yong Uk Kwon , M.D.,
Kyung-Jae Lee, M.D., Ph.D.,*
Joo Young Choi, B.D.,†
and Gu-Hee Jung, M.D., Ph.D.†,‡
, M.D.,
Kyung-Jae Lee, M.D., Ph.D.,*
Joo Young Choi, B.D.,†
and Gu-Hee Jung, M.D., Ph.D.†,‡
, M.D.,
Kyung-Jae Lee, M.D., Ph.D.,*
Joo Young Choi, B.D.,†
and Gu-Hee Jung, M.D., Ph.D.†,‡
Abstract
Purpose
This study analyzed the morphological features of the contralateral femur without an atypical fracture by constructing a three-dimensional model with an actual size medullary canal.
Materials and Methods
Lateral and anterior bowing of the shaft were measured for 21 models, and the shape of the medullary canal was analyzed. To eliminate the projection error, the anteroposterior (AP) femur was rotated internally to the extent that the centerline of the head and neck, which is the ideal position of cephalomedullary nail screw, was neutral, and the lateral femur matched the medial and lateral condyle exactly.
Results
The lateral bowing and anterior bowing was an average of 5.5° (range, 2.8°–10.7°; standard deviation [SD], 2.4°) and 13.1° (range, 6.2°–21.4°; SD, 3.2°), respectively. In the area where lateral bowing increased, the lateral cortex became thicker, and the medullary canal was straightened. On the lateral femur, the anterior angle was increased significantly, and the diameter of curvature averaged 1,370.2 mm (range, 896–1,996 mm; SD, 249.5 mm).
Conclusion
Even if the anterolateral bowing increases in the atypical femur, the medullary canal tends to be straightened in the AP direction. So, it might be considered as a reference to the modification of an intramedullary nail to increase the conformity.
Keywords
Femur, Atypical fracture, Three-dimensional modeling, Anterolateral bowing, Intramedullary nail fixation
Figures
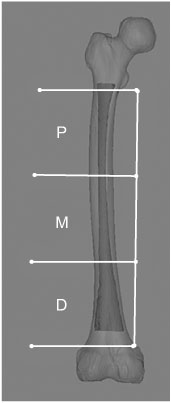
Fig. 1
The fracture location was classified into three parts (i.e., proximal [P], middle [M], and distal [D]) to trisect the femoral diaphysis from just distal to the lesser trochanter to just proximal to the supracondylar flare.

Fig. 2
To analyze the morphological features, (A) a line through the tip of the great trochanter and a condylar center (tip line) was made using a three-dimensional method and (B) compared with the young adult femur. (C) Lines of 60 mm perpendicular to the proximal and distal shaft were drawn and verified in the anteroposterior and lateral projection.

Fig. 3
The proximal (a) and distal angles (b) between the tip line and shaft lines were measured in the anteroposterior and lateral projection (c, d) and then, minus the sum of the proximal and distal angles at 180°, which was defined as the anterior bowing and lateral bowing.

Fig. 4
The diameter of curvature of the posterior surface of the medullary canal was measured to assess the anterior bowing.

Fig. 5
Despite the increased anterolateral bowing, (A) the medullary canal of the atypical femur tended to be straightened on the anteroposterior projection, and the anterior bowing was increased markedly. (B) By comparison, the femur of a 21-year-old adult male showed medial bowing of 2.9° in the femoral shaft.

Fig. 6
According to the degree of femur rotation, the relationship between the tip line and the center of the medullary canal was different. Thus, the projection error might be preoperatively assessed in the preoperative planning.

Fig. 7
Because the atypical femur showed increased anterolateral bowing compared with a normal young adult (A, B), the conventional intramedullary nailing of a 70-year-old female showed several problems, such as iatrogenic fracture, straightening of the femur, and lower limb malalignment (C, D).

Fig. 8
Computation simulations of intramedullary nailing, including the conventional technique (A), rotational technique (B), and cannulated femoral nail (CFN) technique (C), were performed. The results demonstrated that the CFN technique had the best conformity with the medullary canal.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Shane E, Burr D, Abrahamsen B, et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res 2014;29:1–23.
-
-
Koh JH, Myong JP, Jung SM, et al. Atypical femoral fracture in rheumatoid arthritis patients treated with bisphosphonates: a nested case-control study. Arthritis Rheumatol 2016;68:77–82.
-
-
Spinelli MS, Marini E, Daolio PA, Piccioli A. Atypical diaphyseal femoral fractures: considerations on surgical technique. Injury 2019;50 Suppl 2:S65–S69.
-
-
Bronson WH, Kaye ID, Egol KA. Atypical femur fractures: a review. Curr Osteoporos Rep 2014;12:446–453.
-
-
Park YC, Song HK, Zheng XL, Yang KH. Intramedullary nailing for atypical femoral fracture with excessive anterolateral bowing. J Bone Joint Surg Am 2017;99:726–735.
-
-
Yoo H, Cho Y, Park Y, Ha S. Lateral femoral bowing and the location of atypical femoral fractures. Hip Pelvis 2017;29:127–132.
-
-
Shin WC, Moon NH, Jang JH, Park KY, Suh KT. Anterolateral femoral bowing and loss of thigh muscle are associated with occurrence of atypical femoral fracture: effect of failed tension band mechanism in mid-thigh. J Orthop Sci 2017;22:99–104.
-
-
Soh HH, Chua IT, Kwek EB. Atypical fractures of the femur: effect of anterolateral bowing of the femur on fracture location. Arch Orthop Trauma Surg 2015;135:1485–1490.
-
-
Zhang YQ, Chang SM, Huang YG, Wang X. The femoral neck safe zone: a radiographic simulation study to prevent cortical perforation with multiple screw insertion. J Orthop Trauma 2015;29:e178–e182.
-
-
Byun YS, Jung GH. Three-dimensional correlation between trochanteric fossa and the ideal entry point for antegrade femoral nailing. Injury 2016;47:2539–2543.
-
-
Hyodo K, Nishino T, Kamada H, Nozawa D, Mishima H, Yamazaki M. Location of fractures and the characteristics of patients with atypical femoral fractures: analyses of 38 Japanese cases. J Bone Miner Metab 2017;35:209–214.
-
-
Buford WL Jr, Turnbow BJ, Gugala Z, Lindsey RW. Three-dimensional computed tomography-based modeling of sagittal cadaveric femoral bowing and implications for intramedullary nailing. J Orthop Trauma 2014;28:10–16.
-
-
Park YC, Yoon SP, Yang KH. Localization of atypical femoral fracture on straight and bowed femurs. J Bone Metab 2019;26:123–131.
-
-
Lee KJ, Min BW. Surgical treatment of the atypical femoral fracture: overcoming femoral bowing. Hip Pelvis 2018;30:202–209.
-
-
Schilcher J. High revision rate but good healing capacity of atypical femoral fractures. A comparison with common shaft fractures. Injury 2015;46:2468–2473.
-
-
Park JH, Lee Y, Shon OJ, Shon HC, Kim JW. Surgical tips of intramedullary nailing in severely bowed femurs in atypical femur fractures: simulation with 3D printed model. Injury 2016;47:1318–1324.
-
-
Haider IT, Schneider PS, Edwards WB. The role of lower-limb geometry in the pathophysiology of atypical femoral fracture. Curr Osteoporos Rep 2019;17:281–290.
-
-
Thiesen DM, Prange F, Berger-Groch J, et al. Femoral antecurvation-a 3D CT analysis of 1232 adult femurs. PLoS One 2018;13:e0204961
-
-
Chon CS, Kang B, Kim HS, Jung GH. Implications of three-dimensional modeling of the proximal femur for cephalomedullary nailing: an Asian cadaver study. Injury 2017;48:2060–2067.
-
-
Prasarn ML, Cattaneo MD, Achor T, et al. The effect of entry point on malalignment and iatrogenic fracture with the Synthes lateral entry femoral nail. J Orthop Trauma 2010;24:224–229.
-
-
Tan M, Siow JWX, Kwek EBK. Intramedullary nailing of abnormally bowed atypical femoral shaft fractures: surgical technique. Arch Orthop Trauma Surg 2020;140:353–357.
-
 Cite
Cite
