 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 33(2); 2020 > Article
- Original Article Analysis of the Changes in Femoral Varus Bowing and the Factors Affecting Nonunion for the Treatment of Femoral Shaft Fractures over 60 Years Old Using Piriformis Fossa Insertion Intramedullary Nailing
- Yonghan Cha, Chan Ho Park, Jun-Il Yoo, Jung-Taek Kim, WooSuk Kim, Ha-Yong Kim, Won-Sik Choy
-
Journal of Musculoskeletal Trauma 2020;33(2):65-71.
DOI: https://doi.org/10.12671/jkfs.2020.33.2.65
Published online: April 30, 2020
1Department of Orthopedic Surgery, Daejeon Eulji Medical Center, Daejeon, Korea
2Department of Orthopedic Surgery, Yeungnam University Medical Center, Daegu, Korea
3Department of Orthopedic Surgery, Gyeongsang National University Hospital, Jinju, Korea
4Department of Orthopedic Surgery, Ajou University Medical Center, Suwon, Korea
2Department of Orthopedic Surgery, Yeungnam University Medical Center, Daegu, Korea
3Department of Orthopedic Surgery, Gyeongsang National University Hospital, Jinju, Korea
4Department of Orthopedic Surgery, Ajou University Medical Center, Suwon, Korea
- 1,866 Views
- 9 Download
- 1 Crossref
- 0 Scopus
Abstract
Purpose
This study examined the bony morphological changes to analyze the factors affecting bony union in the treatment of elderly femoral shaft fractures with varus bowing using piriformis fossa insertion intramedullary nailing.
Materials and Methods
This study included 26 patients over 60 years of age, who were admitted for femoral shaft fractures between January 2005 and December 2014 and treated with piriformis fossa insertion intramedullary nailing. Age, sex, height, weight, bone mineral density, injury mechanism, fracture type, diameter and length of the nail, postoperative lengthening of the femur, postoperative change in varus angle, contact between the lateral and anterior cortex, and the gap between the fracture line and the bony union were checked. The patients were divided into a varus group and nonvarus group, as well as a bone union group and nonunion group. Logistic regression analysis was performed to analyze the factors affecting nonunion.
Results
The patients were classified into 11 in the varus group and 15 in the non-varus group and 24 in the union group and 2 in the nonunion group. The varus group showed a larger increase in leg length and varus angle reduction than the non-varus group (p<0.05). The union group had more contact with the lateral cortical bone than that of the nonunion group (p<0.05). The factor affecting bone union in regression analysis was contact of the lateral cortical bone (p<0.05).
Conclusion
Treatment of a femoral shaft fracture in elderly patients with a varus deformity of the femur using piriformis fossa insertion intramedullary nail increases the length of the femur and decreases the varus deformity. For bony union, the most important thing during surgery is contact of the lateral cortical bone with the fracture site.
J Korean Fract Soc. 2020 Apr;33(2):65-71. Korean.
Published online Apr 28, 2020.
https://doi.org/10.12671/jkfs.2020.33.2.65
Published online Apr 28, 2020.
https://doi.org/10.12671/jkfs.2020.33.2.65
Copyright © 2020 The Korean Fracture Society. All rights reserved.
Original Article
Analysis of the Changes in Femoral Varus Bowing and the Factors Affecting Nonunion for the Treatment of Femoral Shaft Fractures over 60 Years Old Using Piriformis Fossa Insertion Intramedullary Nailing
Yonghan Cha , M.D.,
Chan Ho Park, M.D.,*
Jun-Il Yoo, M.D.,†
Jung-Taek Kim, M.D.,‡
WooSuk Kim, M.D.,
Ha-Yong Kim, M.D., Ph.D.
and Won-Sik Choy, M.D., Ph.D.
, M.D.,
Chan Ho Park, M.D.,*
Jun-Il Yoo, M.D.,†
Jung-Taek Kim, M.D.,‡
WooSuk Kim, M.D.,
Ha-Yong Kim, M.D., Ph.D.
and Won-Sik Choy, M.D., Ph.D.
, M.D.,
Chan Ho Park, M.D.,*
Jun-Il Yoo, M.D.,†
Jung-Taek Kim, M.D.,‡
WooSuk Kim, M.D.,
Ha-Yong Kim, M.D., Ph.D.
and Won-Sik Choy, M.D., Ph.D.
Abstract
Purpose
This study examined the bony morphological changes to analyze the factors affecting bony union in the treatment of elderly femoral shaft fractures with varus bowing using piriformis fossa insertion intramedullary nailing.
Materials and Methods
This study included 26 patients over 60 years of age, who were admitted for femoral shaft fractures between January 2005 and December 2014 and treated with piriformis fossa insertion intramedullary nailing. Age, sex, height, weight, bone mineral density, injury mechanism, fracture type, diameter and length of the nail, postoperative lengthening of the femur, postoperative change in varus angle, contact between the lateral and anterior cortex, and the gap between the fracture line and the bony union were checked. The patients were divided into a varus group and nonvarus group, as well as a bone union group and nonunion group. Logistic regression analysis was performed to analyze the factors affecting nonunion.
Results
The patients were classified into 11 in the varus group and 15 in the non-varus group and 24 in the union group and 2 in the nonunion group. The varus group showed a larger increase in leg length and varus angle reduction than the non-varus group (p<0.05). The union group had more contact with the lateral cortical bone than that of the nonunion group (p<0.05). The factor affecting bone union in regression analysis was contact of the lateral cortical bone (p<0.05).
Conclusion
Treatment of a femoral shaft fracture in elderly patients with a varus deformity of the femur using piriformis fossa insertion intramedullary nail increases the length of the femur and decreases the varus deformity. For bony union, the most important thing during surgery is contact of the lateral cortical bone with the fracture site.
Keywords
Femur, Shaft fracture, Intramedullary nail, Varus deformity, Nonunion
Figures
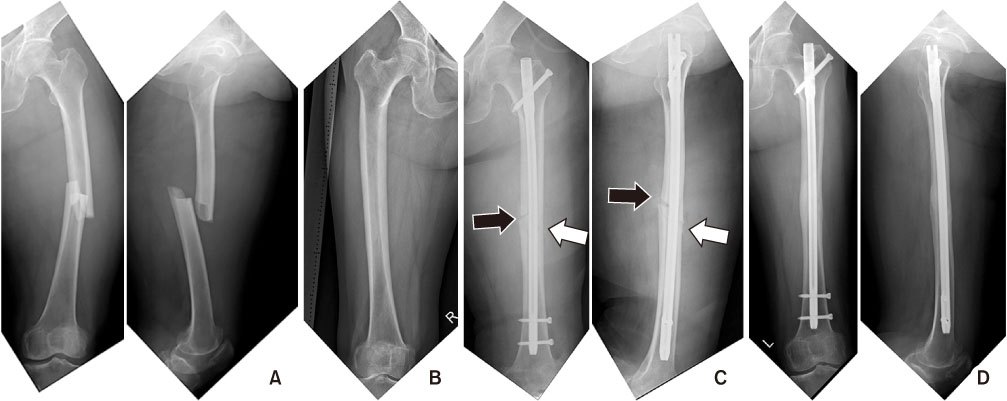
Fig. 1
(A) A 72-year-old female had a femoral diaphyseal fracture. (B) There are more than 5° of femoral bowing on the contralateral radiograph. (C) Radiographs after fracture fixation using an intramedullary nail. Bony contacts are observed at the anterior and lateral cortex of the fracture site (white arrows). On the other hand, fracture gaps are observed at the posterior and medial cortex of fracture sites (black arrows). (D) These are radiographs at postoperative 1-year, and the complete bone union is observed.

Fig. 2
(A) A 65-year-old female had an atypical femoral diaphyseal fracture. (B) There was more than 5° of femoral bowing on the right radiograph. (C) Radiographs after fracture fixation using an intramedullary nail. Bony contacts are observed at the anterior and lateral cortex of the fracture site (white arrows). On the other hand, fracture gaps were observed at the posterior and medial cortex of fracture sites (black arrows). (D) These are radiographs at postoperative 1-year, and the complete bone union was observed.

Fig. 3
Radiograph showing that the medial fracture gap widened after the femoral diaphyseal fracture fixed by an intramedullary nail. The white arrow means the length of the gap at the medial fracture cortex.
Tables

Table 1
Comparison between the Varus Bowing Group and the Non-Varus Bowing Group

Table 2
Comparison of the Nonunion Group and Union Bowing Group
Notes
Financial support:None.
Conflict of interests:None.
References
-
Karakaş HM, Harma A. Femoral shaft bowing with age: a digital radiological study of Anatolian Caucasian adults. Diagn Interv Radiol 2008;14:29–32.
-
-
Vaidya R, Anderson B, Elbanna A, Colen R, Hoard D, Sethi A. CT scanogram for limb length discrepancy in comminuted femoral shaft fractures following IM nailing. Injury 2012;43:1176–1181.
-
-
Yau WP, Chiu KY, Tang WM, Ng TP. Coronal bowing of the femur and tibia in Chinese: its incidence and effects on total knee arthroplasty planning. J Orthop Surg. Hong Kong 2007;15:32–36.
-
-
Wiss DA, Brien WW, Stetson WB. Interlocked nailing for treatment of segmental fractures of the femur. J Bone Joint Surg Am 1990;72:724–728.
-
-
Park JH, Lee Y, Shon OJ, Shon HC, Kim JW. Surgical tips of intramedullary nailing in severely bowed femurs in atypical femur fractures: simulation with 3D printed model. Injury 2016;47:1318–1324.
-
-
Park YC, Song HK, Zheng XL, Yang KH. Intramedullary nailing for atypical femoral fracture with excessive anterolateral bowing. J Bone Joint Surg Am 2017;99:726–735.
-
-
Özsoy MH, Aksekili MA, Kızılay O, Dinçel VE, Aydoğan NH, Ozsoy A. Femoral insufficiency fractures in the elderly-excessive medial femoral bowing complicates intramedullary nailing. Acta Orthop Traumatol Turc 2014;48:507–512.
-
-
Egol KA, Chang EY, Cvitkovic J, Kummer FJ, Koval KJ. Mismatch of current intramedullary nails with the anterior bow of the femur. J Orthop Trauma 2004;18:410–415.
-
-
Yoo JH, Moon SH, Ha YC, et al. Osteoporotic fracture: 2015 position statement of the Korean Society for Bone and Mineral Research. J Bone Metab 2015;22:175–181.
-
-
Shane E, Burr D, Abrahamsen B, et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res 2014;29:1–23.
-
-
Wittkowske C, Raith S, Eder M, et al. Computer assisted evaluation of plate osteosynthesis of diaphyseal femur fracture considering interfragmentary movement: a finite element study. Biomed Tech (Berl) 2017;62:245–255.
-
-
Whelan DB, Bhandari M, McKee MD, et al. Interobserver and intraobserver variation in the assessment of the healing of tibial fractures after intramedullary fixation. J Bone Joint Surg Br 2002;84:15–18.
-
-
Thippanna RK, Kumar MN. Lateralization of femoral entry point to improve the coronal alignment during total knee arthroplasty in patients with bowed femur. J Arthroplasty 2016;31:1943–1948.
-
-
Crossley K, Bennell KL, Wrigley T, Oakes BW. Ground reaction forces, bone characteristics, and tibial stress fracture in male runners. Med Sci Sports Exerc 1999;31:1088–1093.
-
-
Donnelly E, Meredith DS, Nguyen JT, et al. Reduced cortical bone compositional heterogeneity with bisphosphonate treatment in postmenopausal women with intertrochanteric and subtrochanteric fractures. J Bone Miner Res 2012;27:672–678.
-
-
Koh JS, Goh SK, Png MA, Ng AC, Howe TS. Distribution of atypical fractures and cortical stress lesions in the femur: implications on pathophysiology. Singapore Med J 2011;52:77–80.
-
-
Kim JW, Kim H, Oh CW, et al. Surgical outcomes of intramedullary nailing for diaphyseal atypical femur fractures: is it safe to modify a nail entry in bowed femur. Arch Orthop Trauma Surg 2017;137:1515–1522.
-
-
Harris I, Hatfield A, Walton J. Assessing leg length discrepancy after femoral fracture: clinical examination or computed tomography. ANZ J Surg 2005;75:319–321.
-
-
Karapinar L, Kaya A, Oztürk H, Altay T, Kayali C. Leg length discrepancies in adult femoral shaft fractures treated with intramedullary nailing. Ulus Travma Acil Cerrahi Derg 2009;15:256–261.
-
-
Iagulli ND, Mallory TH, Berend KR, et al. A simple and accurate method for determining leg length in primary total hip arthroplasty. Am J Orthop. Belle Mead NJ 2006;35:455–457.
-
-
Upadhyay A, York S, Macaulay W, McGrory B, Robbennolt J, Bal BS. Medical malpractice in hip and knee arthroplasty. J Arthroplasty 2007;22(6 Suppl 2):2–7.
-
-
Wylie JD, Jones DL, Hartley MK, et al. Distal femoral osteotomy for the valgus knee: medial closing wedge versus lateral opening wedge: a systematic review. Arthroscopy 2016;32:2141–2147.
-
 Cite
Cite
