 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 33(4); 2020 > Article
- Original Article Retrospective Comparative Study of the Intraoperative Fracture Gap Compression in the Treatment of Intertrochanteric Fracture Using Proximal Femoral Nail Antirotation
- Se Jin Kim, Hong Man Cho, Jiyeon Park, Ki Yong An, Young Woo Chung, Woojin Shin
-
Journal of Musculoskeletal Trauma 2020;33(4):179-188.
DOI: https://doi.org/10.12671/jkfs.2020.33.4.179
Published online: October 31, 2020
1Department of Orthopedic Surgery, St. Carollo Hospital, Suncheon, Korea
2Department of Orthopedic Surgery, Gwangju Veterans Hospital, Gwangju, Korea
2Department of Orthopedic Surgery, Gwangju Veterans Hospital, Gwangju, Korea
- 1,331 Views
- 4 Download
- 1 Crossref
- 0 Scopus
Abstract
Purpose
Intertrochanteric fractures can be treated using proximal femoral nail antirotation (PFNA). This study examined the clinical and radiological results of the intraoperative fracture compression.
Materials and Methods
Ninety-four patients underwent intraoperative compression (Group I), and 88 patients underwent natural sliding only (Group II). The patients were followed-up for more than two years. All patients met the following seven conditions: (1) AO/OTA 31-A1, A2 type intertrochanter fracture, (2) availability of compression of more than one cortical bone in the anterior or medial region of the fracture site under the preoperative imaging test, (3) Singh index grade ≥3, (4) blade position: center-center, center-inferior, (5) tip-apex distance <25 mm, (6) reduction status of good or very good, and (7) positive or neutral medial cortical support position with slightly valgus reduction.
Results
A slight tendency toward significant differences in acute phase pain between the two groups was observed at six weeks postoperatively (p=0.073). Twenty-four months after surgery, lateral extension of the PFNA helical blade between the two groups showed significant differences (p=0.017). Fracture gaps measured immediately after surgery showed significant differences (p=0.001), and a clear tendency for a significant difference in the average fracture union time was found (p=0.065).
Conclusion
Intraoperative fracture compression, intraoperative fracture compression appears beneficial to achieve a successful union of trochanteric fractures provided that all conditions are met to apply the method safely.
J Korean Fract Soc. 2020 Oct;33(4):179-188. Korean.
Published online Oct 22, 2020.
https://doi.org/10.12671/jkfs.2020.33.4.179
Published online Oct 22, 2020.
https://doi.org/10.12671/jkfs.2020.33.4.179
Copyright © 2020 The Korean Fracture Society. All rights reserved.
Original Article
Retrospective Comparative Study of the Intraoperative Fracture Gap Compression in the Treatment of Intertrochanteric Fracture Using Proximal Femoral Nail Antirotation
Se Jin Kim , M.D.,
Hong Man Cho, M.D.,*
Jiyeon Park, M.D.,*
Ki Yong An, M.D.,*
Young Woo Chung, M.D.,*
and Woojin Shin, M.D.*
, M.D.,
Hong Man Cho, M.D.,*
Jiyeon Park, M.D.,*
Ki Yong An, M.D.,*
Young Woo Chung, M.D.,*
and Woojin Shin, M.D.*
, M.D.,
Hong Man Cho, M.D.,*
Jiyeon Park, M.D.,*
Ki Yong An, M.D.,*
Young Woo Chung, M.D.,*
and Woojin Shin, M.D.*
Abstract
Purpose
Intertrochanteric fractures can be treated using proximal femoral nail antirotation (PFNA). This study examined the clinical and radiological results of the intraoperative fracture compression.
Materials and Methods
Ninety-four patients underwent intraoperative compression (Group I), and 88 patients underwent natural sliding only (Group II). The patients were followed-up for more than two years. All patients met the following seven conditions: (1) AO/OTA 31-A1, A2 type intertrochanter fracture, (2) availability of compression of more than one cortical bone in the anterior or medial region of the fracture site under the preoperative imaging test, (3) Singh index grade ≥3, (4) blade position: center-center, center-inferior, (5) tip-apex distance <25 mm, (6) reduction status of good or very good, and (7) positive or neutral medial cortical support position with slightly valgus reduction.
Results
A slight tendency toward significant differences in acute phase pain between the two groups was observed at six weeks postoperatively (p=0.073). Twenty-four months after surgery, lateral extension of the PFNA helical blade between the two groups showed significant differences (p=0.017). Fracture gaps measured immediately after surgery showed significant differences (p=0.001), and a clear tendency for a significant difference in the average fracture union time was found (p=0.065).
Conclusion
Intraoperative fracture compression, intraoperative fracture compression appears beneficial to achieve a successful union of trochanteric fractures provided that all conditions are met to apply the method safely.
Keywords
Femur, Proximal femoral fracture, Proximal femoral nail antirotation
Figures

Fig. 1
(A, B) True reamer head and blade diameter was measured in two ways using a ruler and calipers. The tip apex distance (TAD) was calculated using the intraoperative image intensifier films. The measured anteroposterior (AP) and lateral radiograph distances were combined to calculate the measured TAD. (C) Intraoperative image intensifier shows AP and lateral radiograph after reaming. To calculate the TAD, XAP is the distance from the tip of the reamer to the apex of the femoral head in the AP image, and XLAT is the distance in the translateral image. (D) Intraoperative image intensifier shows AP and lateral radiographs of the inserted blade before locking. The TAD was calculated using the same method. (E) Radiographs show the AP and lateral images of the inserted blade after locking. The TAD was calculated using the same method. (F) Radiograph shows an AP image after locking the blade and removing the impactor. The image shows that the lateral extension of the blade is small.

Fig. 2
Radiographs of a 73-year-old female patient with AO/OTA 31-A2 trochanteric fracture treated with proximal femoral nail antirotation. (A) Preoperative hip anteroposterior and translateral radiographs suggesting a right trochanteric femoral fracture AO/OTA 31-A2. (B) Intraoperative radiograph under fluoroscopy before intraoperative fracture compression. (C) After intraoperative fracture compression, intraoperative radiograph under fluoroscopy, showing a reduction of the fracture gap.

Fig. 3
(A) Immediate postoperative hip anteroposterior (AP) and translateral (Lat) radiographs showing a good reduction state. The blade position was within the center-inferior tip apex distance of 25 mm. (B) Complete union was achieved in the follow-up hip AP and Lat radiographs four months after the operation.
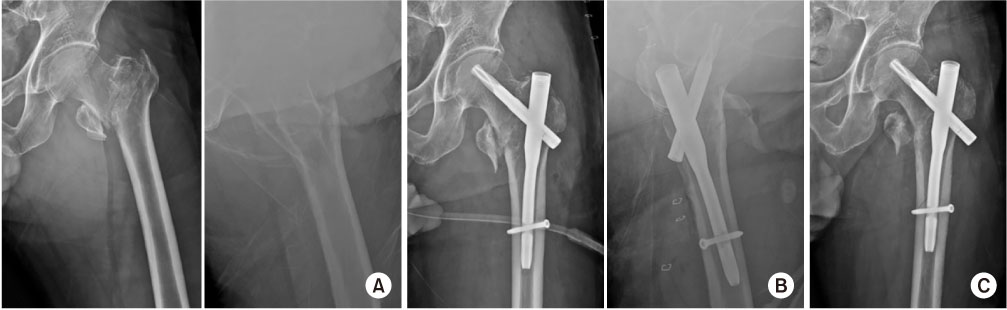
Fig. 4
Radiograph of a 70-year-old male patient with AO/OTA 31-A2 trochanteric fracture treated with proximal femoral nail antirotation. (A) Preoperative hip anteroposterior (AP) and translateral (Lat) radiographs, suggesting a left trochanteric femoral fracture AO/OTA 31-A2. (B) Immediate postoperative hip AP and Lat radiographs showing a good reduction state. (C) Non-displaced fracture was found around the distal screw at five months after the operation due to falling from a ladder.
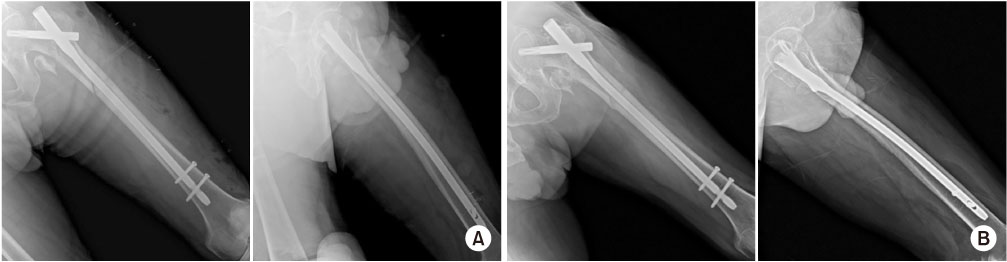
Fig. 5
(A) Immediate postoperative hip anteroposterior and lateral radiographs after revision with a longer nail showing a good reduction state. (B) Complete union was achieved in the follow-up radiograph at four months after revision surgery.
Tables

Table 1
Demographic Data of Group I and Group II

Table 2
Perioperative Results and Complications in Group I and Group II

Table 3
Clinical Results in Group I and Group II

Table 4
Radiological Results and Complications in Group I and Group II
Notes
Financial support:None.
Conflict of interests:None.
References
-
Langlais F, Burdin P, Bourgin T, Sassi N, Levasseur M, Chagneau F. Weight-bearing early after osteosynthesis of the femoral neck by nail-plate (100 cases). Rev Chir Orthop Reparatrice Appar Mot 1987;73:624–636.
-
-
Wirtz C, Abbassi F, Evangelopoulos DS, Kohl S, Siebenrock KA, Krüger A. High failure rate of trochanteric fracture osteosynthesis with proximal femoral locking compression plate. Injury 2013;44:751–756.
-
-
Zhang S, Zhang K, Jia Y, Yu B, Feng W. InterTan nail versus Proximal Femoral Nail Antirotation-Asia in the treatment of unstable trochanteric fractures. Orthopedics 2013;36:e288–e294.
-
-
Gavaskar AS, Tummala NC, Srinivasan P, Gopalan H, Karthik B, S S. Helical blade or the integrated lag screws: a matched pair analysis of 100 patients with unstable trochanteric fractures. J Orthop Trauma 2018;32:274–277.
-
-
Goldhahn J, Suhm N, Goldhahn S, Blauth M, Hanson B. Influence of osteoporosis on fracture fixation--a systematic literature review. Osteoporos Int 2008;19:761–772.
-
-
Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification compendium - 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007;21 10 Suppl:S1–S133.
-
-
Singh M, Nagrath AR, Maini PS. Changes in trabecular pattern of the upper end of the femur as an index of osteoporosis. J Bone Joint Surg Am 1970;52:457–467.
-
-
Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am 1995;77:1058–1064.
-
-
Lenich A, Mayr E, Rüter A, Möckl Ch. Füchtmeier B: First results with the trochanter fixation nail (TFN): a report on 120 cases. Arch Orthop Trauma Surg 2006;126:706–712.
-
-
Von Korff M, Ormel J, Keefe FJ, Dworkin SF. Grading the severity of chronic pain. Pain 1992;50:133–149.
-
-
Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An endresult study using a new method of result evaluation. J Bone Joint Surg Am 1969;51:737–755.
-
-
Seyhan M, Turkmen I, Unay K, Ozkut AT. Do PFNA devices and Intertan nails both have the same effects in the treatment of trochanteric fractures? A prospective clinical study. J Orthop Sci 2015;20:1053–1061.
-
-
Audigé L, Hanson B, Swiontkowski MF. Implant-related complications in the treatment of unstable intertrochanteric fractures: meta-analysis of dynamic screw-plate versus dynamic screwintramedullary nail devices. Int Orthop 2003;27:197–203.
-
-
Haidukewych GJ. Intertrochanteric fractures: ten tips to improve results. J Bone Joint Surg Am 2009;91:712–719.
-
-
Loch DA, Kyle RF, Bechtold JE, Kane M, Anderson K, Sherman RE. Forces required to initiate sliding in second-generation intramedullary nails. J Bone Joint Surg Am 1998;80:1626–1631.
-
-
Davis TR, Sher JL, Horsman A, Simpson M, Porter BB, Checketts RG. Intertrochanteric femoral fractures. Mechanical failure after internal fixation. J Bone Joint Surg Br 1990;72:26–31.
-
-
Liu W, Zhou D, Liu F, Weaver MJ, Vrahas MS. Mechanical complications of intertrochanteric hip fractures treated with trochanteric femoral nails. J Trauma Acute Care Surg 2013;75:304–310.
-
-
Kaufer H. Mechanics of the treatment of hip injuries. Clin Orthop Relat Res 1980;(146):53–61.
-
-
Jung EY, Oh IT, Shim SY, Yoon BH, Sung YB. The effect of valgus reduction on the position of the blade of the proximal femoral nail antirotation in intertrochanteric hip fractures. Clin Orthop Surg 2019;11:36–42.
-
-
Cho MR, Lee JH, Kwon JB, Do JS, Chae SB, Choi WK. The effect of positive medial cortical support in reduction of pertrochanteric fractures with posteromedial wall defect using a dynamic hip screw. Clin Orthop Surg 2018;10:292–298.
-
-
Tsukada S, Okumura G, Matsueda M. Postoperative stability on lateral radiographs in the surgical treatment of pertrochanteric hip fractures. Arch Orthop Trauma Surg 2012;132:839–846.
-
-
Chang SM, Zhang YQ, Du SC, et al. Anteromedial cortical support reduction in unstable pertrochanteric fractures: a comparison of intra-operative fluoroscopy and post-operative three dimensional computerised tomography reconstruction. Int Orthop 2018;42:183–189.
-
-
Wild M, Jungbluth P, Thelen S, et al. The dynamics of proximal femoral nails: a clinical comparison between PFNA and Targon PF. Orthopedics 33;2010 [doi: 10.3928/01477447-2010062504]
-
-
Xu Y, Geng D, Yang H, Wang X, Zhu G. Treatment of unstable proximal femoral fractures: comparison of the proximal femoral nail antirotation and gamma nail 3. Orthopedics 2010;33:473.
-
-
de Soucanye;A. Bertani;P. Candoni;C. Charpail,E Demortiere.Proximal femoral nail antirotation (PFN-ATM) fixation of extra-capsular proximal femoral fractures in the elderly: retrospective study in 102 patients. Orthop Traumatol Surg Res 2012;98:288–295.
-
-
Park BJ, Cho HM, Kim JH, Sin WJ. Excessive sliding of the helical blade and the femoral neck fracture after insertion of proximal femoral nail anti-rotation for type A2 intertrochanteric fractures: a case report. J Korean Fract Soc 2013;26:151–155.
-
 Cite
Cite
