 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 33(3); 2020 > Article
- Case Report Rendezvous Surgery for Peri-Implant Fractures around Locking Compression Plate on Anterolateral Bowed Femur - A Case Report -
- Hong Man Cho, Jiyeon Park
-
Journal of Musculoskeletal Trauma 2020;33(3):159-163.
DOI: https://doi.org/10.12671/jkfs.2020.33.3.159
Published online: July 31, 2020
Department of Orthopedic Surgery, Gwangju Veterans Hospital, Gwangju, Korea
- 841 Views
- 9 Download
- 0 Crossref
- 0 Scopus
Abstract
An 84-year-old female visited with an intertrochanteric femoral fracture. The patient had undergone an open reduction and internal fixation with a compressive plate and elastic nail in an ipsilateral atypical diaphyseal femoral fracture in the past. Compressive plate and elastic nail remained, and anterolateral bowing was presented. To treat the periprosthetic trochanteric fracture, a proximal femoral nail was used without removing the previously inserted compressive plate. Under the “rendezvous” technique, using a combination of fixating intramedullary nail and compressive plate simultaneously, the distal screw was fixed, and a femoral head lag screw was inserted after reducing the fracture. Complete union of the fracture was achieved 16 months after the operation, and a decrease in mobility function was not found postoperatively. The authors report this case for the “rendezvous” technique as a treatment option for elderly patients with periprosthetic trochanteric fractures, who had previously undergone surgical treatment for ipsilateral atypical diaphyseal femoral fractures with anterolateral bowing.
J Korean Fract Soc. 2020 Jul;33(3):159-163. Korean.
Published online Jul 24, 2020.
https://doi.org/10.12671/jkfs.2020.33.3.159
Published online Jul 24, 2020.
https://doi.org/10.12671/jkfs.2020.33.3.159
Copyright © 2020 The Korean Fracture Society. All rights reserved.
Case Report
Rendezvous Surgery for Peri-Implant Fractures around Locking Compression Plate on Anterolateral Bowed Femur: A Case Report
Hong Man Cho , M.D.,
and Jiyeon Park, M.D.
, M.D.,
and Jiyeon Park, M.D.
, M.D.,
and Jiyeon Park, M.D.
Abstract
An 84-year-old female visited with an intertrochanteric femoral fracture. The patient had undergone an open reduction and internal fixation with a compressive plate and elastic nail in an ipsilateral atypical diaphyseal femoral fracture in the past. Compressive plate and elastic nail remained, and anterolateral bowing was presented. To treat the periprosthetic trochanteric fracture, a proximal femoral nail was used without removing the previously inserted compressive plate. Under the “rendezvous” technique, using a combination of fixating intramedullary nail and compressive plate simultaneously, the distal screw was fixed, and a femoral head lag screw was inserted after reducing the fracture. Complete union of the fracture was achieved 16 months after the operation, and a decrease in mobility function was not found postoperatively. The authors report this case for the “rendezvous” technique as a treatment option for elderly patients with periprosthetic trochanteric fractures, who had previously undergone surgical treatment for ipsilateral atypical diaphyseal femoral fractures with anterolateral bowing.
Keywords
Femur, Trochanteric fractures, Periprosthetic fracture, Rendezvous technique
Figures
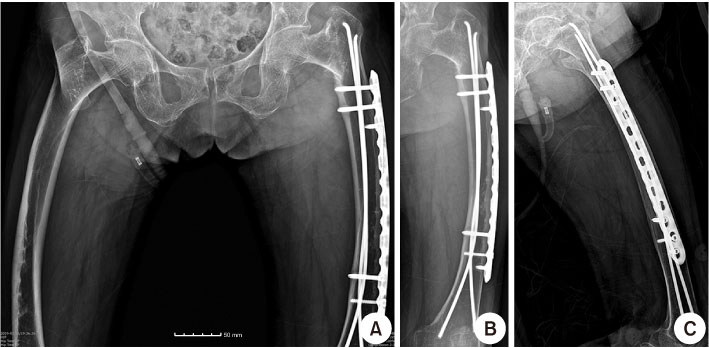
Fig. 1
Simple radiograph of total hip anteroposterior (AP) (A), left femur AP (B), and lateral (C), intertrochanteric femoral fracture AO Foundation/Orthopaedic Trauma Association classification 31-A2 fracture in the left femur with anterolateral bowing and complete union of a previous atypical diaphyseal fracture. A decrease in bone density in the lateral cortex of the femur and pull-out of the distal screw of the compression plate can be found in the left femur AP and lateral (B, C).
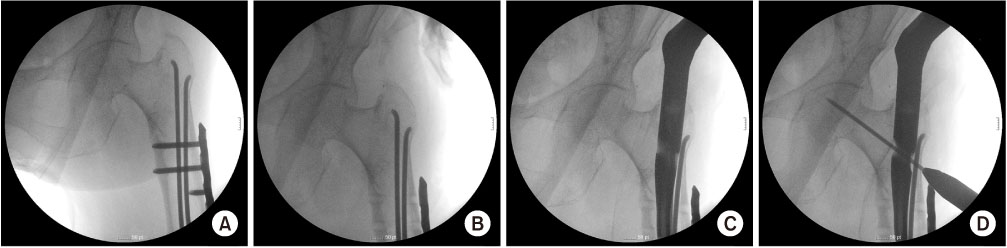
Fig. 2
(A) In the C-arm image intensifier image, stable reduction of a trochanteric fracture was achieved. (B) Three screws inserted in the proximal hole of the compression plate, which can be interrupted for insertion of the proximal femoral nail, were removed. (C) A compression hip nail was inserted successfully without interrupting previously inserted elastic nails. (D) A guidewire for the femoral head lag screw was inserted.
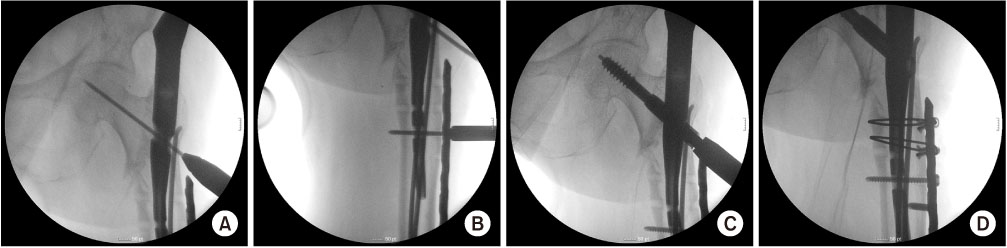
Fig. 3
(A) In the C-arm image intensifier image, a guidewire for the femoral head lag screw was inserted in the center-center position of the femoral head and fixed primarily. (B) A distal screw was inserted, achieving simultaneous fixation of compression plate and compression hip nail. (C) After reaming the femoral head, the lag screw of the femoral head was inserted. (D) For the three screws removed in the proximal compression plate, an additional screw was inserted for the most distal hole, and AO cable wiring was performed for two proximal removed screw holes.
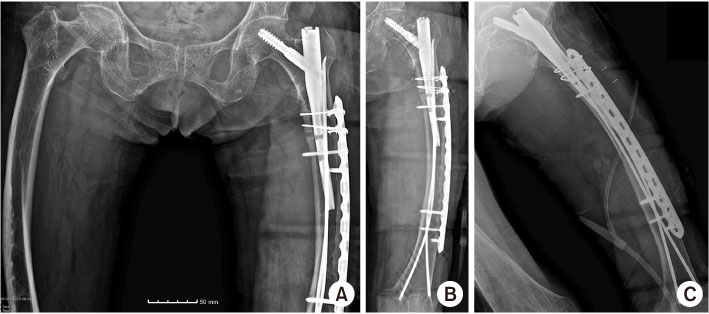
Fig. 4
In the postoperative simple radiograph, successful reduction of the femoral trochanteric fracture can be found in the total hip anteroposterior (AP) (A), left femur AP (B), and lateral (C).
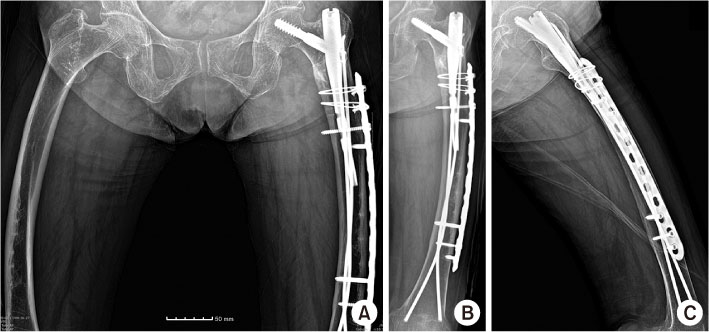
Fig. 5
Sixteen months after the operation, complete union of the femoral trochanteric fracture can be found in the total hip anteroposterior (AP) (A), left femur AP (B), and lateral (C).
Notes
Financial support:None.
Conflict of interests:None.
References
-
Bottlang M, Doornink J, Byrd GD, Fitzpatrick DC, Madey SM. A nonlocking end screw can decrease fracture risk caused by locked plating in the osteoporotic diaphysis. J Bone Joint Surg Am 2009;91:620–627.
-
-
Lindahl H. Epidemiology of periprosthetic femur fracture around a total hip arthroplasty. Injury 2007;38:651–654.
-
-
Koval KJ, Aharonoff GB, Rosenberg AD, Bernstein RL, Zuckerman JD. Functional outcome after hip fracture. Effect of general versus regional anesthesia. Clin Orthop Relat Res 1998;(348):37–41.
-
-
Ooi LH, Wong TH, Toh CL, Wong HP. Hip fractures in nonagenarians: a study on operative and non-operative management. Injury 2005;36:142–147.
-
-
Winquist RA, Hansen ST Jr, Clawson DK. Closed intramedullary nailing of femoral fractures. A report of five hundred and twenty cases. J Bone Joint Surg Am 1984;66:529–539.
-
-
Kovar FM, Strasser E, Jaindl M, Endler G, Oberleitner G. Complications following implant removal in patients with proximal femur fractures: an observational study over 16 years. Orthop Traumatol Surg Res 2015;101:785–789.
-
-
Mamczak CN, Gardner MJ, Bolhofner B, Borrelli J Jr, Streubel PN, Ricci WM. Interprosthetic femoral fractures. J Orthop Trauma 2010;24:740–744.
-
-
von Rüden C, Tauber M, Woltmann A, et al. Surgical treatment of ipsilateral multi-level femoral fractures. J Orthop Surg Res 2015;10:7
-
-
Sommer C, Gautier E, Müller M, Helfet DL, Wagner M. First clinical results of the locking compression plate (LCP). Injury 2003;34 Suppl 2:B43–B54.
-
-
Lee KJ, Min BW. Surgical treatment of the atypical femoral fracture: overcoming femoral bowing. Hip Pelvis 2018;30:202–209.
-
 Cite
Cite
