 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Articles
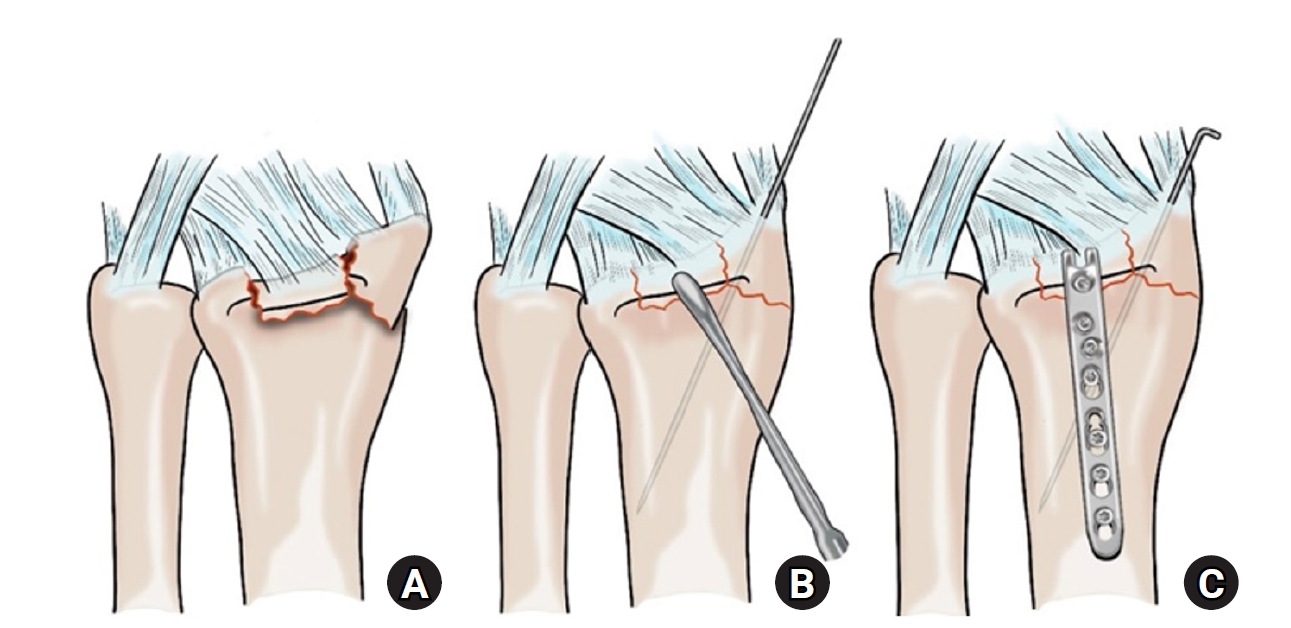
- Hook plate versus periarticular-type volar locking plate for distal radius fractures involving the volar lunate facet in Korea: a retrospective cohort study
- Hyun-Jae Park, Joo-Hak Kim
- J Musculoskelet Trauma 2025;38(4):221-228. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00241
-
 Abstract
Abstract
 PDF
PDF - Background
This study investigated the clinical and radiographic outcomes of hook plate (HP) fixation for volar lunate facet fractures, comparing them with periarticular-type volar locking plates (PVLPs).
Methods
A retrospective review was conducted on 24 patients with distal radius fractures involving volar lunate facet fragments who underwent surgery between January 2016 and April 2021. Patients were divided into two groups: HP (n=12) and PVLP (n=12). Radiographic union, wrist range of motion, Disabilities of the Arm, Shoulder and Hand (DASH) scores, and implant-related complications were compared. Statistical analyses included the Mann-Whitney U test and Fisher exact test.
Results
Radiographic union was achieved in all patients (100%), without secondary displacement or hardware failure. No significant differences were observed between the two groups in wrist flexion (P=0.152), extension (P=0.832), pronation (P=0.792), or supination (P=0.328). The mean DASH scores were 12.8±5.5 in the HP group and 14.6±6.0 in the volar plate group (P=0.449). One patient in the HP group experienced mild flexor tendinopathy that resolved with conservative management. No cases of tendon rupture or early reoperation were reported.
Conclusions
Fixation of volar lunate facet fractures using a HP yielded clinical and radiographic outcomes comparable to those of PVLPs, with a low rate of complications and reliable bony union. Due to its mechanical stability, compatibility with standard surgical approaches, and low risk of flexor tendon irritation, the HP may serve as a valuable alternative for managing volar lunate facet fractures. Level of evidence: IV.
- 1,050 View
- 30 Download

- Does the Operator’s Experience Affect the Occurrence of Complications after Distal Radius Fracture Volar Locking Plate Fixation? A Comparative Study of the First Four Years and Thereafter
- Kee-Bum Hong, Chi-Hoon Oh, Chae Kwang Lim, Sungwoo Lee, Soo-Hong Han, Jun-Ku Lee
- J Musculoskelet Trauma 2024;37(4):175-183. Published online October 25, 2024
- DOI: https://doi.org/10.12671/jmt.2024.37.4.175
- Correction in: J Musculoskelet Trauma 2025;38(1):40
-
Abstract
PDF
- Purpose
The management of distal radius fractures (DRFs) has evolved with the introduction of volar locking plate (VLP) fixation, offering stable fixation and better outcomes. Nevertheless, the impact of the surgeon’s experience on the complication rates in VLP fixation remains to be determined, particularly for less-experienced surgeons. This study compared the complication rates during the initial four years and subsequent two years of a hand surgeon’s practice of VLP fixation for DRFs.
Materials and Methods
The data between March 2016 and December 2022 were analyzed retrospectively under the Institutional Review Board approval. A single surgeon performed all VLP fixation surgeries after finishing regular hand surgery training, with the first four years representing the less experienced phase (Group 1) and the following two years indicating the experienced phase (Group 2). The patients’ characteristics, operation-related factors, and postoperative complications, including tendon injuries, nerve-related complications, fixation and instrument-related issues, osteosynthesis-related problems, and infections, were compared. In addition, the authors compared the data with a large multicenter study conducted by experienced hand surgeons.
Results
Three hundred and nineteen patients (321 wrists) were included. The mean age was 63.3 years, and 26.3% were male and 73.7% were female. The operation time was 53.7±14.5 minutes and 74.4±26.5 minutes in groups 1 and 2, respectively, which was statistically significantly shorter (p<0.001). The complication rates between the two groups were similar, except for the higher implant removal rates in Group 1. A comparison with a previous multicenter study revealed higher reduction losses and carpal tunnel syndrome in this study, but the overall complication rate was low.
Conclusion
In DRF management, when the operating surgeon has completed an accredited training course, VLP fixation is a good treatment method that can be performed effectively even by less experienced surgeons with low complication rates. -
Citations
Citations to this article as recorded by
- Epidemiological changes and surgical trends of distal radius fractures in adults over 50 years during the COVID-19 pandemic in Korea: a nationwide repeated cross-sectional study
Han-Kook Yoon, So Ra Yoon, Kee-Bum Hong, Youngsu Jung, SeongJu Choi, Jun-Ku Lee
Journal of Musculoskeletal Trauma.2026; 39(1): 12. CrossRef - Author correction: “Does the operator's experience affect the occurrence of complications after distal radius fracture volar locking plate fixation? A comparative study of the first four years and thereafter”
Kee-Bum Hong, Chi-Hoon Oh, Chae Kwang Lim, Sungwoo Lee, Soo-Hong Han, Jun-Ku Lee
Journal of Musculoskeletal Trauma.2025; 38(1): 40. CrossRef - Characteristics of patients with distal radius fracture requiring arthroscopic foveal repair after bone union
Min Jung Park, Cheungsoo Ha, Hyun Tak Kang, Yong Hyun Yoon, Jun-Ku Lee, Soo-Hong Han
Arthroscopy and Orthopedic Sports Medicine.2025; 12(2): 70. CrossRef
- Epidemiological changes and surgical trends of distal radius fractures in adults over 50 years during the COVID-19 pandemic in Korea: a nationwide repeated cross-sectional study
- 4,322 View
- 56 Download
- 3 Crossref
- Primary Open Reduction and Plate Fixation in Open Comminuted Intra-Articular Distal Radius Fracture
- Jun-Ku Lee, Soonchul Lee, Weon Min Cho, Minkyu Kil, Soo-Hong Han
- J Korean Fract Soc 2021;34(1):16-22. Published online January 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.1.16
-
Abstract
PDF
- Purpose
There are no standard surgical treatments for open distal radius fractures (DRFs), and the fracture fixator is chosen by the surgeon’s own experience. This study compared the outcomes of open reduction and volar locking plating (OR VLP) between closed and open AO-OTA type C3 DRFs. Materials and Methods: Patient data were retrospectively collected between January 2010 and December 2018. Only patients aged >18 years with AO-OTA C3 DRFs were included. After further exclusion, the patients with DRFs were divided into two groups: 13 patients with open DRFs in Group 1 and 203 patients with closed DRFs in Group 2. Data on the patient characteristics and treatment-related factors were further investigated. For the radiological evaluation, the radial height, volar height, and volar titling were measured based on the final plain radiography, and the union time was measured. The wrist range of motion (ROM), pain visual analogue scale score, and modified Mayo wrist score for function were measured at the final outpatient follow-up. Finally, the complications associated with OR VLP fixa-tion were investigated. Results: In the demographic comparison, the patients with open fractures were older (mean age, 62years) than those with closed fractures (mean age, 57 years), without a statistically significant differ-ence. The patients with open DRFs had longer antibiotic therapy and hospital stay durations. Although they presented a higher radial inclination, with statistical significance, the clinical implication was low with a mean difference of 3°. No significant differences were observed for the remaining radiological parameters, wrist ROM, and functional scores. An open DRF did not increase the complication rates,including deep infection. Conclusion: Depending on the expertise of the operating surgeon, the primary OR VLP fixation in open intra-articular comminuted DRF did not increase the incidence of deep infections and yielded similar outcomes to a closed intra-articular comminuted DRF.
- 1,677 View
- 12 Download
- Treatment of the Communited Distal Radius Fracture Using Volar Locking Plate Fixation with Allogenic Cancellous Bone Graft in the Elderly
- Je Kang Hong, Chang Hyun Shin
- J Korean Fract Soc 2015;28(1):8-16. Published online January 31, 2015
- DOI: https://doi.org/10.12671/jkfs.2015.28.1.8
-
Abstract
PDF
- PURPOSE
We studied results of the communited distal radius fracture treated with allogenic cancellous bone graft and volar locking plate in the elderly.
MATERIALS AND METHODS
We studied 29 cases of communited distal radius fracture treated with allogenic cancellous bone graft and volar locking plate from April 2009 to April 2013. Fracture was classified according to AO/OTA classification. Postoperative clinical evaluation was performed with measurement of wrist range of motion (ROM) at last follow-up, modified Mayo wrist scoring system (MMWS), and visual analogue pain scale (VAS). Radiologic evaluation was performed with measurement of radial length on immediate postoperation and last follow-up, radial inclination, volar tilt and ulnar variance checked at the last follow-up using Sarmiento criteria.
RESULTS
Using the MMWS, 13 cases were classified as 'good', 10 'fair', and 5 'normal'. The average wrist ROM was 88.5% for flexion, 92.2% for extension, 90.5% for adduction, and 94.0% for abduction. The average VAS was 1.7. On the last follow-up, average radius length, radial inclination and volar tilt did not show statistically significant improvement (p>0.05) compared to immediate post operation measurements, and according to Sarmiento criteria, 5 cases were classified as 'good', 14 'fair', and 7 'normal'.
CONCLUSION
Treatment of severe communited distal radius fracture accompanied by bone defect with volar locking plate and allogenic cancellous bone graft is a satisfying and effective treatment method in the elderly.
- 1,310 View
- 5 Download
- Treatment of Fractures of the Distal Radius Using Variable-Angle Volar Locking Plate
- Jae Cheon Sim, Sung Sik Ha, Ki Do Hong, Tae Ho Kim, Min Chul Sung
- J Korean Fract Soc 2015;28(1):46-52. Published online January 31, 2015
- DOI: https://doi.org/10.12671/jkfs.2015.28.1.46
-
Abstract
PDF
- PURPOSE
The purpose of this study is to evaluate outcome of variable-angle volar locking plate for treatment of distal radius fractures.
MATERIALS AND METHODS
We retrospectively analyzed the results in 45 cases treated by variable-angle volar locking plate. We evaluated the clinical results according to the Mayo wrist performance scoring system and radiographic results.
RESULTS
All cases had bony union. The mean Mayo wrist performance scoring system was 84.8. Between preoperative and immediate postoperative radiographic measurement, the mean radial length improved from 8.4 to 11.8 mm, radial inclination from 14.2degrees to 22.4degrees, volar tilt from -4.5degrees to 9.6degrees, and intraarticular step-off from 1.8 to 0.3 mm (p<0.05). Between immediate postoperative and latest follow-up radiographic measurements, the mean loss of radial length measured 0.8 mm, radial inclination 0.4degrees, and volar tilt 0.9degrees (p>0.05). All cases showed bone union with no evidence of malunion, nonunion, or metal failure.
CONCLUSION
Treatment of distal radius fractures using variable angle volar locking plate showed satisfactory outcomes. It is a good option to obtain stable fixation without significant loss of reduction.
- 874 View
- 6 Download
- The Surgical Outcome of Unstable Distal Clavicle Fractures Treated with 2.4 mm Volar Distal Radius Locking Plate
- Suk Kyu Choo, Ji Ho Nam, Youngwoo Kim, Hyoung Keun Oh
- J Korean Fract Soc 2015;28(1):38-45. Published online January 31, 2015
- DOI: https://doi.org/10.12671/jkfs.2015.28.1.38
-
Abstract
PDF
- PURPOSE
This study evaluated the surgical outcomes of unstable distal clavicular fractures treated with a 2.4 mm volar distal radius locking plate.
MATERIALS AND METHODS
From August 2009 to August 2012, 16 patients with distal clavicle fractures underwent surgical treatment. Mean age was 36 years (18-62 years) and mean follow-up period was 12.9 months (6-32 months). Two cases were Neer type I, six cases IIa, three cases IIb, three cases III, and two cases V. For the radiologic assessment, union time and metal failure were evaluated, and coracoidiologic assessment, union time and metal failure were evaluatethe acromioclavicular joint. The clinical results were evaluated by range of motion, postoperative complication, and University of California at Los Angeles (UCLA) score.
RESULTS
Mean time to fracture union was 7.4 weeks (6-14 weeks) in all cases. No statistical difference in coracoid-clavicle distance was observed between immediate post-operation group and contra-lateral group (p=0.6), but an increase of 2.1 mm was observed in the last follow up group compared with the contra-lateral group (p<0.01). The UCLA scoring system showed excellent results in 15 cases and good results in one case. Acromial-clavicle instability occurred in one case so that metal removal and distal clavicle resection were performed.
CONCLUSION
A 2.4 mm volar distal radius locking plate can provide rigid fixation through several screw fixation in the short distal fragment and lead to satisfactory clinical outcomes in unstable distal clavicular fractures. -
Citations
Citations to this article as recorded by- Estudo retrospectivo da placa anterior superior como tratamento para fraturas instáveis da clavícula distal (tipo 2 de Neer)
Syed Ibrahim, Jimmy Joseph Meleppuram
Revista Brasileira de Ortopedia.2018; 53(3): 306. CrossRef - Retrospective study of superior anterior plate as a treatment for unstable (Neer type 2) distal clavicle fractures
Syed Ibrahim, Jimmy Joseph Meleppuram
Revista Brasileira de Ortopedia (English Edition).2018; 53(3): 306. CrossRef
- Estudo retrospectivo da placa anterior superior como tratamento para fraturas instáveis da clavícula distal (tipo 2 de Neer)
- 1,021 View
- 1 Download
- 2 Crossref
- The Fate of Pronator Quadratus Muscle after Volar Locking Plating of Unstable Distal Radius Fractures
- Chae Hyun Lim, Heun Guyn Jung, Ju Yeong Heo, Young Jae Jang, Yong Soo Choi
- J Korean Fract Soc 2014;27(3):191-197. Published online July 31, 2014
- DOI: https://doi.org/10.12671/jkfs.2014.27.3.191
-
Abstract
PDF
- PURPOSE
The purpose of this study is to evaluate the pronator quadrates muscle in patients who underwent internal fixation with a volar locking plate for unstable distal radius fractures.
MATERIALS AND METHODS
Forty patients who underwent internal fixation with a volar locking plate for unstable distal radius fracture were enrolled. We evaluated the clinical results according to the Mayo wrist score, the wrist range of motion, and the grip strength at the last follow-up. Using ultrasonography, muscle thickness of the pronator quadrates was compared between injured and uninjured arm.
RESULTS
Bone union was achieved in all cases. The mean Mayo wrist score was 82.79 points. The grip strength of the injured arm was decreased to 89.1% of the uninjured side. The decrease of pronation range of the injured wrist motions was significant (82.3degrees, p=0.004). There was significant atrophy of the pronator quadrates muscle on the injured side (injured side: 3.19 mm, uninjured side: 4.72 mm, p=0.001); and the decrement of muscle thickness in pronator quadrates showed an association with the Mayo wrist score (r=-0.35, p=0.042).
CONCLUSION
These results suggest that continuity of the muscle is maintained after use of the volar locking plating for unstable distal radius fractures with repair of pronator quadrates; however, there is atrophy of pronator quadrates muscle and limitation of pronation in the injured wrist.
- 789 View
- 1 Download
- Clinical Assessment after the Volar Locking Plate Removal of Distal Radius Fracture
- Hee Chul Gwak, Joo Yong Kim, Gyu Min Kong, Jung Won Kim, Jae Yong Kwak, Dong Gyun Kim
- J Korean Fract Soc 2014;27(1):23-28. Published online January 31, 2014
- DOI: https://doi.org/10.12671/jkfs.2014.27.1.23
-
Abstract
PDF
- PURPOSE
The purpose of this study is to evaluate the clinical outcomes after removing the volar locking plate for distal radius fracture.
MATERIALS AND METHODS
We reviewed retrospectively the medical records of 34 patients, 36 cases after removing the plates among 150 patients, with 162 cases that underwent open reduction and internal fixation using the volar locking plate between January 2006 and May 2011. We performed preoperative and postoperative clinical assessments using the quick-disabilities of the arm, shoulder and hand (Q-DASH), the visual analog scale (VAS) score, and the range of motion on wrist, grip and pinch power.
RESULTS
The major reason for plate removal was the time to remove the plate according to the fracture union and the patient's demand without other specific complaints (28 cases). The mean preoperative VAS score was 1.78 and the mean postoperative VAS score 1.81 (p=0.64). The mean preoperative Q-DASH score was 30.02 and the mean postoperative Q-DASH score 38.46 (p<0.001). The mean preoperative grip and pinch power were 18.14 kg and 7.67 kg. The mean postoperative grip and pinch power were 15.27 kg and 6.94 kg (p=0.23).
CONCLUSION
The removal of the volar locking plate for distal radius fracture should be decided by considering the patient's clinical and socioeconomic conditions carefully.
- 1,230 View
- 0 Download
Case Report
- Rupture of the Extensor Pollicis Longus Tendon at the Proximal Screw of Volar Plate Fixation for Distal Radius Fracture: A Case Report
- Dong Ju Shin, Seung Oh Nam, Hun Sik Cho
- J Korean Fract Soc 2013;26(4):338-342. Published online October 31, 2013
- DOI: https://doi.org/10.12671/jkfs.2013.26.4.338
-
Abstract
PDF
- As volar plate fixation of distal radius fracture becomes more common, reports of ruptured extensor pollicis longus tendon by a protruding distal screw tip are also increasing steadily. Authors have experienced a rare case of ruptured extensor pollicis longus tendon at the prominent proximal screw of fixed volar plate for distal radius fracture, and we report it herein with a review of the literature.
- 831 View
- 1 Download
Original Articles
- Comparative Analysis of the Results of Fixed-angle versus Variable-angle Volar Locking Plate for Distal Radius Fracture Fixation
- Seung Do Cha, Jai Hyung Park, Hyung Soo Kim, Soo Tae Chung, Jeong Hyun Yoo, Joo Hak Kim, Jung Hwan Park
- J Korean Fract Soc 2012;25(3):197-202. Published online July 31, 2012
- DOI: https://doi.org/10.12671/jkfs.2012.25.3.197
-
Abstract
PDF
- PURPOSE
To compare the outcomes of distal radius fractures in a fixed-angle volar locking plate group and variable-angle volar locking plate group.
MATERIALS AND METHODS
Forty-one patients observed at least 6 months after surgery were included in this retrospective study. We used the range of motion, visual analogue scale score, Disabilities of the Arm, Shoulder and Hand Questionnaire score, and radiologic findings to measure the clinical results.
RESULTS
No differences in clinical results or radiologic results were noted between the fixed-angle volar locking plate group and variable-angle volar locking plate group.
CONCLUSION
We believe that it is important to minimize complications by using appropriate screws and plates according to the fracture type, though no differences in the surgical outcome were noted between the fixed-angle volar locking plate group and variable-angle volar locking plate group with distal radius fracture. -
Citations
Citations to this article as recorded by- Volar locking plate fixation for distal radius fractures: did variable-angle plates make difference?
Mohamed Abdel-Wahed, Ahmed Abdel-Zaher Khater, Mahmoud Ahmed El-Desouky
International Orthopaedics.2022; 46(9): 2165. CrossRef - Treatment of Fractures of the Distal Radius Using Variable-Angle Volar Locking Plate
Jae-Cheon Sim, Sung-Sik Ha, Ki-Do Hong, Tae-Ho Kim, Min-Chul Sung
Journal of the Korean Fracture Society.2015; 28(1): 46. CrossRef - Functional Outcomes of Percutaneous K-Wire Fixation for Distal Radius Fractures with or without Osteoporosis
Ki-Chan An, Gyu-Min Kong, Jang-Seok Choi, Hi-Chul Gwak, Joo-Yong Kim, Sung-Yub Jin
Journal of the Korean Fracture Society.2013; 26(4): 248. CrossRef
- Volar locking plate fixation for distal radius fractures: did variable-angle plates make difference?
- 1,252 View
- 16 Download
- 3 Crossref
- Comparison of Operative Management in Distal Radius Fractures Using 3.5 mm Versus 2.4 mm Volar Locking Compression Plates
- Sung Sik Ha, Tae Ho Kim, Ki Do Hong, Jae Chun Sim, Jong Hyun Kim
- J Korean Fract Soc 2011;24(2):156-162. Published online April 30, 2011
- DOI: https://doi.org/10.12671/jkfs.2011.24.2.156
-
Abstract
PDF
- PURPOSE
To evaluate clinical and radiological results using 3.5 mm & 2.4 mm volar locking compression plate (LCP) in distal radius fractures.
MATERIALS AND METHODS
This study reviewed the results of 115 cases of distal radius fractures treated with 3.5 mm volar LCP (73 cases) & 2.4 mm volar LCP (42 cases) from September 2003 to June 2009. The radiographic results were evaluated by radiographic assessment, and the clinical results were evaluated by Knirk and Jupiter's criteria, Modified Mayo wrist scoring system and DASH score.
RESULTS
Radiological evaluation of the radial length, radial inclination, volar tilt and intraarticular step off were improved both 3.5 mm volar LCP and 2.4 mm volar LCP. Nine cases of arthritis occured in 3.5 mm volar LCP and 7 cases in 2.4 mm volar by using the Knirk and Jupiter's criteria. The mean score evaluated by Modified Mayo was 86.7 in 3.5 mm volar LCP and 84.8 in 2.4 mm volar LCP. DASH score was 11.2 point in 3.5 mm volar LCP, 10.9 point in 2.4 mm volar LCP. All cases showed bone union showing no evidence of malunion, nounion, nor metal failure.
CONCLUSION
Distal radius fractures treated with 3.5 mm volar LCP and 2.4 mm volar LCP show satisfying radiological and clinical outcome. -
Citations
Citations to this article as recorded by- Treatment of Fractures of the Distal Radius Using Variable-Angle Volar Locking Plate
Jae-Cheon Sim, Sung-Sik Ha, Ki-Do Hong, Tae-Ho Kim, Min-Chul Sung
Journal of the Korean Fracture Society.2015; 28(1): 46. CrossRef - Functional Outcomes of Percutaneous K-Wire Fixation for Distal Radius Fractures with or without Osteoporosis
Ki-Chan An, Gyu-Min Kong, Jang-Seok Choi, Hi-Chul Gwak, Joo-Yong Kim, Sung-Yub Jin
Journal of the Korean Fracture Society.2013; 26(4): 248. CrossRef
- Treatment of Fractures of the Distal Radius Using Variable-Angle Volar Locking Plate
- 1,078 View
- 2 Download
- 2 Crossref
- 2.4 mm Volar Locking Compression Plate for Treatment of Unstable Distal Radius Fractures
- Sung Jin Kim, Chul Hyun Cho
- J Korean Fract Soc 2011;24(2):151-155. Published online April 30, 2011
- DOI: https://doi.org/10.12671/jkfs.2011.24.2.151
-
Abstract
PDF
- PURPOSE
To evaluate outcomes 2.4 mm volar locking compression plate for treatment of unstable distal radius fractures.
MATERIALS AND METHODS
We retrospectively analyzed the results in 22 cases, which were treated by 2.4 mm volar locking compression plate. We evaluated the clinical results according to the Mayo wrist performance scoring system and radiographic results.
RESULTS
All cases had bony union. The mean Mayo wrist performance score was 85.23. Between preoperative and immediate postoperative radiographic measurements, the mean radial length was improved from 6.04 mm to 9.68 mm, radial inclination from 15.61degrees to 19.61degrees, volar tilt from -13.73degrees to 7.66degrees and intraarticular step-off from 0.79 mm to 0.33 mm (p<0.05). Between immediate postoperative and latest follow-up radiographic measurements, the mean loss of radial length measured 0.86 mm, radial inclination 0.41degrees, volar tilt 0.54degrees and intraarticular step-off 0.02 mm (p>0.05). Postoperative complication included that flexor pollicis longus and 2nd flexor digitorum profundus were ruptured in 1 case.
CONCLUSION
Treatment of unstable distal radius fractures using a 2.4 mm volar locking compression plate showed satisfactory outcomes. It is a good option to obtain stable fixation without significant loss of reduction. -
Citations
Citations to this article as recorded by- Is dorsal cortex drilling necessary for distal radius fractures treated with a volar locking plate? A comparative study of near-cortex-only and far-cortex drilling
Chul Hong Kim, Sung Yoon Jung, Hyeon Jun Kim, Si-Hyun Park
Journal of Trauma and Injury.2025; 38(3): 248. CrossRef - Treatment of the Communited Distal Radius Fracture Using Volar Locking Plate Fixation with Allogenic Cancellous Bone Graft in the Elderly
Je Kang Hong, Chang Hyun Shin
Journal of the Korean Fracture Society.2015; 28(1): 8. CrossRef
- Is dorsal cortex drilling necessary for distal radius fractures treated with a volar locking plate? A comparative study of near-cortex-only and far-cortex drilling
- 1,117 View
- 2 Download
- 2 Crossref
- Short Term Results of Operative Management with 2.4 mm Volar Locking Compression Plates in Distal Radius Fractures
- Ki Chul Park, Chang Hun Lee
- J Korean Fract Soc 2009;22(4):264-269. Published online October 31, 2009
- DOI: https://doi.org/10.12671/jkfs.2009.22.4.264
-
Abstract
PDF
- PURPOSE
To evaluate the short term outcome of internal fixation using 2.4 mm volar locking compression plate for the treatment of unstable distal radius fractures. MATERIALS AND METHODS: We retrospectively analyzed the results in 22 cases, which were treated with 2.4 mm volar locking compression plate. We evaluated the radiologic results and the clinical results according to Disabilities of the Arm, Shoulder and Hand (DASH) score and visual analogue scale. RESULTS: At final follow up, the mean VAS was 1.2 and mean DASH score was 10. Average loss of reduction from initial postoperative to final follow up radiographs was 0.36 mm of radial length, 0.2degrees of radial inclination, 0.6degrees of volar tilt. CONCLUSION: Fixation of unstable dorsally displaced distal radius fractures with a 2.4 mm volar locking compression plate provides sufficient stability with minimal loss of reduction and good enough clinical outcomes with less complications. -
Citations
Citations to this article as recorded by- Treatment of Fractures of the Distal Radius Using Variable-Angle Volar Locking Plate
Jae-Cheon Sim, Sung-Sik Ha, Ki-Do Hong, Tae-Ho Kim, Min-Chul Sung
Journal of the Korean Fracture Society.2015; 28(1): 46. CrossRef - 2.4 mm Volar Locking Compression Plate for Treatment of Unstable Distal Radius Fractures
Sung-Jin Kim, Chul-Hyun Cho
Journal of the Korean Fracture Society.2011; 24(2): 151. CrossRef
- Treatment of Fractures of the Distal Radius Using Variable-Angle Volar Locking Plate
- 1,101 View
- 1 Download
- 2 Crossref
- Volar Percutaneous Cannulated Screw Fixation for Subacute Scaphoid Wasit Fracture
- Jae Kwang Kim, Jong Oh Kim, Seung Yup Lee, Nam Hoon Do
- J Korean Fract Soc 2009;22(2):104-109. Published online April 30, 2009
- DOI: https://doi.org/10.12671/jkfs.2009.22.2.104
-
Abstract
PDF
- PURPOSE
To report the surgical results of volar percutaneous cannulated compression screw fixation in subacute scaphoid fracture.
MATERIALS AND METHODS
Between January 2004 and January 2007, eight consecutive patients with subacute scaphoid waist fracture, who sought medical attention between 4 weeks to 6 months after injury, were included in this study. All patients were male of an average age 29.2 years (range, 19 to 44). Mean duration of injury was 10.3+/-4.1 weeks. An acutrak cannulated screw (Acumed, Hillsboro, OR) was introduced volarly under image intensifier guidance in all patients. We performed radiological evaluation preoperatively and postoperatively. And we performed 12 months postoperatively using grip strength, range of motion (ROM) of the wrist, Mayo Modified Wrist Score (MMWS) and Disabilities of the Arm, Shoulder and the Hand (DASH) score for functional evaluation.
RESULTS
Preoperative radiography showed minimal sclerosis line in three patients and a bone resorption around fracture sites in two patients. However, no patient had dorsal intercalated segment instability or more than 35 degrees of lateral intrascaphoid angle. Fractures united successfully at 11.6+/-2.1 weeks postoperatively without any requirement for a further procedure. At 12 months follow-up evaluations, ROM of the injured wrist was 93% of the uninjured wrist and grip strength of the injured wrist was 95% of the injured wrist. The mean MMWS was 93+/-6.6 and the mean DASH score was 4.8+/-1.2.
CONCLUSION
We believe that volar percutaneous cannulated screw fixation is a reliable method in case of subacute scaphoid waist fracture without scaphoid deformity or carpal instability. -
Citations
Citations to this article as recorded by- Surgical Outcome of Stable Scaphoid Nonunion without Bone Graft
Eun Sun Moon, Myung Sun Kim, Il Kyu Kong, Min Sun Choi
Journal of the Korean Fracture Society.2010; 23(1): 69. CrossRef
- Surgical Outcome of Stable Scaphoid Nonunion without Bone Graft
- 1,079 View
- 5 Download
- 1 Crossref
Review Article
- Volar Plating of Distal Radius Fractures
- Kwang Hyun Lee
- J Korean Fract Soc 2008;21(4):325-333. Published online October 31, 2008
- DOI: https://doi.org/10.12671/jkfs.2008.21.4.325
-
Abstract
PDF
- Volar plating seems to indicate that many surgeons believe it leads to superior results, and is attractive because of the ease of the operative approach and the soft tissue sleeve to protect digital and wrist tendons. And also it have a locking mechanism to produce the fixed angle device with a low profile and may be thought to be a new era in the surgical treatment of dorsally displaced distal radius fractures even in the face of comminuted or osteoporotic bone. Locked volar plating allows direct fracture reduction, stable fixation and provides stability enough to allow early mobilization and function. The results with volar locking or fixed angle fixation for the general treatment of unstable distal radius fractures in elderly patients has been favorable. Volar plating has fewer complications than external fixation and dorsal plating and allow for earlier return to function. The current indications, technical aspects, clinical results, and complications of the volar plating are being reviewed.
-
Citations
Citations to this article as recorded by- Ultrasonographic Assessment of the Pronator Quadratus Muscle after Surgical Treatment for Distal Radius Fractures
Dong Hyuk Choi, Hyun Kyun Chung, Ji Won Lee, Cheol Hwan Kim, Yong Soo Choi
Journal of the Korean Fracture Society.2017; 30(2): 69. CrossRef - The Fate of Pronator Quadratus Muscle after Volar Locking Plating of Unstable Distal Radius Fractures
Chae-Hyun Lim, Heun-Guyn Jung, Ju-Yeong Heo, Young-Jae Jang, Yong-Soo Choi
Journal of the Korean Fracture Society.2014; 27(3): 191. CrossRef - Comparison of Operative Management in Distal Radius Fractures Using 3.5 mm Versus 2.4 mm Volar Locking Compression Plates
Sung-Sik Ha, Tae-Ho Kim, Ki-Do Hong, Jae-Chun Sim, Jong Hyun Kim
Journal of the Korean Fracture Society.2011; 24(2): 156. CrossRef - Treatment for Unstable Distal Radius Fracture with Osteoporosis -Internal Fixation versus External Fixation-
Jin Rok Oh, Tae Yean Cho, Sung Min Kwan
Journal of the Korean Fracture Society.2010; 23(1): 76. CrossRef - Short Term Results of Operative Management with 2.4 mm Volar Locking Compression Plates in Distal Radius Fractures
Ki-Chul Park, Chang-Hun Lee
Journal of the Korean Fracture Society.2009; 22(4): 264. CrossRef
- Ultrasonographic Assessment of the Pronator Quadratus Muscle after Surgical Treatment for Distal Radius Fractures
- 1,100 View
- 1 Download
- 5 Crossref
Original Articles
- Volar T-Locking Compression Plate for Treatment of Unstable Distal Radius Fractures
- Chul Hyun Cho, Ki Choer Bae, Doo Hyun Kwon
- J Korean Fract Soc 2008;21(3):220-224. Published online July 31, 2008
- DOI: https://doi.org/10.12671/jkfs.2008.21.3.220
-
Abstract
PDF
- PURPOSE
To evaluate outcomes volar T-locking compression plate for treatment of unstable distal radius fractures.
MATERIALS AND METHODS
We retrospectively analysed the results in 35 cases, which were treated by volar plating with T-LCP. We evaluated the clinical results according to the Mayo wrist scoring system and radiographic results.
RESULTS
The mean score was 83.86 respectively. Between preoperative and immediate postoperative radiographic measurements, averaged radial length was improved from 5.75 mm to 11.53 mm, radial inclination from 12.86 degrees to 22.56 degrees, volar tilt from -3.64 degrees to 9.90 degrees and intraarticular step-off from 1.48 mm to 0.42 mm. Between immediate postoperative and latest follow-up radiographic measurements, mean loss of radial length measured 0.43 mm, radial inclination 0.46 degrees, volar tilt 0.89 degrees.
CONCLUSION
Treatment of unstable distal radius fractures using a volar T-LCP showed satisfactory outcomes. We think that it is good surgical option to allow return to daily living, result in early postsurgical wrist motion. -
Citations
Citations to this article as recorded by- Treatment of Fractures of the Distal Radius Using Variable-Angle Volar Locking Plate
Jae-Cheon Sim, Sung-Sik Ha, Ki-Do Hong, Tae-Ho Kim, Min-Chul Sung
Journal of the Korean Fracture Society.2015; 28(1): 46. CrossRef - The Fate of Pronator Quadratus Muscle after Volar Locking Plating of Unstable Distal Radius Fractures
Chae-Hyun Lim, Heun-Guyn Jung, Ju-Yeong Heo, Young-Jae Jang, Yong-Soo Choi
Journal of the Korean Fracture Society.2014; 27(3): 191. CrossRef - 2.4 mm Volar Locking Compression Plate for Treatment of Unstable Distal Radius Fractures
Sung-Jin Kim, Chul-Hyun Cho
Journal of the Korean Fracture Society.2011; 24(2): 151. CrossRef - Short Term Results of Operative Management with 2.4 mm Volar Locking Compression Plates in Distal Radius Fractures
Ki-Chul Park, Chang-Hun Lee
Journal of the Korean Fracture Society.2009; 22(4): 264. CrossRef - Plate Fixation of AO Type C3 Fractures of the Distal Radius
Eun-Sun Moon, Myung-Sun Kim, Hyeong-Won Park, Min-Sun Choi
Journal of the Korean Fracture Society.2009; 22(3): 172. CrossRef - Biosorption of Mercury (II) from Aqueous Solutions by Zygnema fanicum Algae
Gh. Shams Khoramabad, A. Jafari, J. Hasanvand Jamshidi
Journal of Applied Sciences.2008; 8(11): 2168. CrossRef - Volar Plating of Distal Radius Fractures
Kwang-Hyun Lee
Journal of the Korean Fracture Society.2008; 21(4): 325. CrossRef
- Treatment of Fractures of the Distal Radius Using Variable-Angle Volar Locking Plate
- 1,136 View
- 1 Download
- 7 Crossref
- A Comparison of LCPlate versus Conventional T-plate Fixation about the Reduction Loss in the Treatment of Distal Radial Fracture
- Jin Soo Suh, Chang Soo Lee, Kook Hyun Wang
- J Korean Fract Soc 2008;21(2):135-139. Published online April 30, 2008
- DOI: https://doi.org/10.12671/jkfs.2008.21.2.135
-
Abstract
PDF
- PURPOSE
The purpose of this study was to evaluate and compare the clinical & radiological outcome between LCP and conventional T-plate fixation in the treatment of distal radial fracture.
MATERIALS AND METHODS
From January 2000 to October 2006, 26 patients were treated by LCP fixation and 20 patients were treated by conventional T-plate fixation for distal radial fracture. We used the X-ray to calculate the radial inclination, radial length and volar tilting, then compared the loss of correction after the operation between both groups. We also evaluated the clinical functional outcome by Mayo wrist score.
RESULTS
The average follow-up since operation was ten months in both LCP and conventional T-plate fixation group. According to Frykmann classification, there were 1 case of type 1 (4%), 2 of type 2 (8%), 5 of type 3 (19%), 14 of type 4 (54%), 1 of type 5 (4%), 2 of type 7 (8%), 1 of type 8 (4%), and to AO classification, 4 of type A (15%), 22 of type C (85%) in LCP group. In conventional T-plate group, according to Frykmann classification, there were 12 cases of type 3 (60%), 4 of type 4 (20%), 3 of type 7 (15%), 1 of type 8 (5%), and to AO classification, 6 of type B (30%), 14 of type C (70%). In LCP group, the loss of correction between immediate post-operation and last follow-up was about 1.03 degrees in radial inclination, -1.09 mm in radial length, -2.08 degrees in volar tilting at each, and in conventional T-plate group, 2.4 degrees in radial inclination, -0.82 mm in radial length, -2.11 degrees in volar tilting at each. There was no statistical significance (p>0.05) in two groups. In the clinical functional outcome (according to Mayo wrist score), 92% of patient showed above good result in LCP group and 85% of patient showed above good result in conventional T-plate group. There was no infection, delayed union.
CONCLUSION
Treatment by Interposition of fragments and shortening in the intractable nonunion of humerus with a bony defect can achieve not only good functional result, shortened bone union time and improved in shoulder and elbow motion.
- 620 View
- 0 Download
Case Report
- Anterior Dislocation of Distal Radio-Ulnar Joint: A Case Report
- Shin Kun Kim, Sang Bong Ko, Seung Bum Chae
- J Korean Fract Soc 2008;21(1):66-69. Published online January 31, 2008
- DOI: https://doi.org/10.12671/jkfs.2008.21.1.66
-
Abstract
PDF
- There are variable types in wrist joint injury. Most common case is simple distal radius fracture. And ulnar head dislocation associated with disruption of distal radioulnar ligament is unusual. Among thease injury types. volar dislocation of ulnar head in the distal radioulnar joint is not common and it is misdiagnosis frequently. So it needs to surgical operation frequently. The author reviews this injury with the relevant literature.
- 841 View
- 6 Download
Original Articles
- Treatment of Fractures of the Distal Radius using Locking Compression Plate
- Jae Cheon Sim, Nam Sik Chung, Ki Do Hong, Sung Sik Ha, Ji Hoon Kang
- J Korean Fract Soc 2005;18(2):100-104. Published online April 30, 2005
- DOI: https://doi.org/10.12671/jkfs.2005.18.2.100
-
Abstract
PDF
- PURPOSE
To evaluate the usefulness of locking compression plate (LCP) and volar plating through anterior approach for distal radius fracture.
MATERIALS AND METHODS
We retrospectively analysed that 15 distal radius fracture, which would not be reduced by closed reduction or too comminuated to maintain reduction or articular surface inconguency, were treated by open reduction through anterior approach and volar plating using LCP. The results were evaluated by preoperative and postoperative radiographs. Functional results were analysed using the Modified Mayo Wrist Scoring System.
RESULTS
All cases achieved anatomical articular surface reduction postoperatively. In terms of radiologic analysis, mean radial length (9.0 mm vs. 11.8 mm), radial inclination (14.7degrees vs. 20.9degrees ), volar tilt (-6.3degrees vs. 8.3degrees ) and articular step-off (1.4 mm vs. 0.3 mm) were improved. The average Modified Wrist Score was 89. Nonunion or malunion was not occurred.
CONCLUSION
Open reduction through anterior approach and volar plating using LCP is a useful method that provides excellent results with few complications in the treatment of fracture of the distal radius. -
Citations
Citations to this article as recorded by- Periprosthetic Fracture after Locked Plating in the Osteoporotic Long Bone Fracture
Ki-Chul Park, Hong-Sik Kim, Jeong-Han Oh
Journal of the Korean Orthopaedic Association.2012; 47(3): 222. CrossRef - 2.4 mm Volar Locking Compression Plate for Treatment of Unstable Distal Radius Fractures
Sung-Jin Kim, Chul-Hyun Cho
Journal of the Korean Fracture Society.2011; 24(2): 151. CrossRef - Treatment of Femur Supracondylar Fracture with Locking Compression Plate
Seong Ho Bae, Seung Han Cha, Jeung Tak Suh
Journal of the Korean Fracture Society.2010; 23(3): 282. CrossRef - Comparison of Outcomes for Unstable Distal Radius Intraarticular Fractures - T-locking Compression Plate versus External Fixator -
Chul-Hyun Cho, Su-Won Jung, Sung-Won Sohn, Chul Hyung Kang, Ki-Cheor Bae, Kyung-Jae Lee
Journal of the Korean Fracture Society.2008; 21(1): 51. CrossRef - Basic Principle of the Locking Compression Plate
Keun Bae Lee
Journal of the Korean Fracture Society.2008; 21(3): 261. CrossRef - Volar T-Locking Compression Plate for Treatment of Unstable Distal Radius Fractures
Chul Hyun Cho, Ki Choer Bae, Doo Hyun Kwon
Journal of the Korean Fracture Society.2008; 21(3): 220. CrossRef
- Periprosthetic Fracture after Locked Plating in the Osteoporotic Long Bone Fracture
- 1,092 View
- 2 Download
- 6 Crossref
- Treatment of Post-traumatic Dislocation of Metacarpophalangeal Joints of the Hand
- Seung Koo Rhee, Seok Whan Song, Joo Yup Lee, Chang Youn Moon, Jae Chan Oh
- J Korean Soc Fract 2003;16(2):253-261. Published online April 30, 2003
- DOI: https://doi.org/10.12671/jksf.2003.16.2.253
-
Abstract
PDF
- PURPOSE
To analyse the obstacles to prevent the reduction for dislocation of the metacarpophalangeal (MP) joints of the hand and evaluate the relationship between the sex and dislocation type in closed reduction case.
MATERIALS AND METHODS
Total 27 cases of MP joint dislocation of the hand (11 cases of thumb, and 14 index and 2 little finger) were reviewed retrospectively. The anatomical structures to prevent the reduction were confirmed at operation and the cases which were reduced immediately were also analysed for their ages and differences of damaged structures, and finally their complications or outcome were reviewed for average 7 months after reduction.
RESULTS
In 11 cases of thumb MP joint dislocations, the complex dorsal dislocations in which the protruded metacarpal neck was caught by buttonhole of torn anterior joint capsule, volar plate and FPB were reduced by open method in 8 cases, and closed reduction was done in 2 cases but one old case required arthrodesis. In other finger MP joint dislocations, the Kaplan's concept to prevent the reduction was confirmed. But reduction of torn volar plate and incision of transverse metacarpal ligament were sufficient to reduce the dislocation with gentle longitudinal traction during the operation. In two cases of little finger MP joint dislocation, the ruptured radial collateral ligaments were noted after open reduction and it must the repaired to prevent the finger instability later. Their overall end results were good without any significant restriction of MP joints motions and finger instabilities.
CONCLUSION
One or two times of closed reduction with proper local anesthesia could be tried, but simple reducible dislocation can be converted to complex irreducible ones by the inappropriate traction method, and so proper reduction technique by closed or even in open way is important with the knowledge of anatomical obstacles to prevent the reduction of the metacarpophalangeal joints.
- 758 View
- 0 Download
- Anterior Approach and Volar T-plate fixation of Distal Radius Fracture
- Woo Sung Choi, Weon Yoo Kim, Dong Won Choi, Yun Hack Shin, Jin Young Kim
- J Korean Soc Fract 2003;16(2):244-252. Published online April 30, 2003
- DOI: https://doi.org/10.12671/jksf.2003.16.2.244
-
Abstract
PDF
- PURPOSE
To analyze the radiologic and clinical results of open reduction and volar plating through anterior approach for distal radius fracture.
MATERIALS AND METHODS
We retrospectively analysed that 19 distal radius fracture, which would not be reduced by closed reduction or too comminuted to maintain reduction or articular surface incongruency, were treated by open reduction and volar plating through anterior approach. The results were evaluated by preoperative and immediate postoperative radiographics and clinical results were analysed using Green and O'Brien scoring system at final follow up.
RESULTS
All cases achieved anatomical articular surface reduction postoperatively. In terms of radiologic analysis, mean radial length (8.8 mm +/-4.8 mm vs. 11 mm +/-3 mm), radial inclination (15 degrees+/-5.7 degreesvs. 20degrees+/-5degrees), volar tilt (-11 degrees+/-13 degrees vs. 7 degrees+/-4 degrees) and ulnar plus variant (4 mm+/-3 mm vs. 0 mm+/-1 mm) were improved. The clinical evaluation revealed 9 excellent cases, 7 good cases, 2 fair cases and 1 poor case. The reduction loss and flexor pollicis longus rupture was occurred in one patient, who had severely displaced comminute fracture in initial injury.
CONCLUSION
Using volar plating, authors gain good radiologic and clinical results. But, additional external fixation is recommended to prevent further collapse in severly comminuted fractures. -
Citations
Citations to this article as recorded by- Is dorsal cortex drilling necessary for distal radius fractures treated with a volar locking plate? A comparative study of near-cortex-only and far-cortex drilling
Chul Hong Kim, Sung Yoon Jung, Hyeon Jun Kim, Si-Hyun Park
Journal of Trauma and Injury.2025; 38(3): 248. CrossRef - Treatment of Fractures of the Distal Radius Using Variable-Angle Volar Locking Plate
Jae-Cheon Sim, Sung-Sik Ha, Ki-Do Hong, Tae-Ho Kim, Min-Chul Sung
Journal of the Korean Fracture Society.2015; 28(1): 46. CrossRef
- Is dorsal cortex drilling necessary for distal radius fractures treated with a volar locking plate? A comparative study of near-cortex-only and far-cortex drilling
- 947 View
- 2 Download
- 2 Crossref
- Volar Perilunate Dislocation: A case report
- Sung Soo Kim, Sung Keun Sohn, Dae Hee Lee
- J Korean Soc Fract 1999;12(2):440-445. Published online April 30, 1999
- DOI: https://doi.org/10.12671/jksf.1999.12.2.440
-
Abstract
PDF
- Perilunar dislocation is not a common injury. When it occurs it is usually dorsal. Only a few isolated cases have been reported of volar perilunar dislocation, in which the capitate is displaced volar to the palmar flexed lunate. Like its more common dorsal counterpart, volar perilunate dislocation usually requires either a concomitant fracture of the scaphoid or scapholunate dissociation. Many authors have been proposed the mechanism of injury, forced hyperflexion, hyperextension with supination of the forearm and violent trauma with extensor tendon rupture. The diagnosis is most easily made on the lateral view. Closed reduction using finger-trap traction should be the initial step in management. Although successful treatment has been reported with a closed reduction alone, open reduction is probably indicated in most cases to align and stabilize the bones. We are reporting on a patient of volar perilunar dislocation without a fracture of the scaphoid or scapholunate dissociation of the right hand associated with extensor tendon rupture.
-
Citations
Citations to this article as recorded by- Combined Lunate and Triquetrum Fracture: A Case Report
Joo-Hak Kim, Hyung-Soo Kim, Soo-Tae Chung, Jeong-Hyun Yoo, Seung-Do Cha, Joong-Hyo Lee, Jai-Hyung Park
Journal of the Korean Fracture Society.2008; 21(4): 320. CrossRef
- Combined Lunate and Triquetrum Fracture: A Case Report
- 910 View
- 4 Download
- 1 Crossref
- Displaced fracture of the base of the second metacarpal into velar side
- Yerl Bo Sung, Sung Soo Kim
- J Korean Soc Fract 1997;10(4):945-948. Published online October 31, 1997
- DOI: https://doi.org/10.12671/jksf.1997.10.4.945
-
Abstract
PDF
- Fracture of the base of the second metacarpal bone is usually undisplaced or minimallly displaced. There were some reports of traumatic avulsion fracture of the extensor carpi radialis longus from the base of the second metacarpal. In most cases, the fragments were displaced into dorsal side However, there is noreport uf displaced fracture of the base of the second metacarpal into volar side in English papers. We are reporting a case in which the fragment was displaced into volar side.
- 645 View
- 1 Download
 First
First Prev
Prev

