 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 34(2); 2021 > Article
- Review Article Pediatric Fractures around the Wrist
- Gihun Kim, Kun-Bo Park
-
Journal of Musculoskeletal Trauma 2021;34(2):80-86.
DOI: https://doi.org/10.12671/jkfs.2021.34.2.80
Published online: April 30, 2021
Division of Pediatric Orthopedic Surgery, Severance Children’s Hospital, Yonsei University College of Medicine, Seoul, Korea
- 2,134 Views
- 49 Download
- 0 Crossref
- 0 Scopus
Abstract
Fractures around the wrist are the third most common fracture among all pediatric fractures. Furthermore, distal radius fractures, a type of wrist fracture, are the most common fractures in children. Understanding pediatric fractures around the wrist is very important considering their prevalence. There is a specific belief that pediatric fractures can heal easily because of remodeling, but not all fractures can heal without proper treatment. Complications such as growth problems, nonunion can occur if the fracture is not treated properly. This paper reviewed recent articles about distal radius fractures, Galeazzi-equivalent fractures, and carpal bone fractures, including scaphoid fractures in children and adolescents. Successful treatment can be achieved without complications when an accurate diagnosis and proper non-surgical or surgical treatment are performed based on this article.
J Korean Fract Soc. 2021 Apr;34(2):80-86. Korean.
Published online Apr 23, 2021.
https://doi.org/10.12671/jkfs.2021.34.2.80
Published online Apr 23, 2021.
https://doi.org/10.12671/jkfs.2021.34.2.80
Copyright © 2021 The Korean Fracture Society. All rights reserved.
Review
Pediatric Fractures around the Wrist
Gihun Kim , M.D.
and Kun-Bo Park, M.D.
, M.D.
and Kun-Bo Park, M.D.
, M.D.
and Kun-Bo Park, M.D.
Abstract
Fractures around the wrist are the third most common fracture among all pediatric fractures. Furthermore, distal radius fractures, a type of wrist fracture, are the most common fractures in children. Understanding pediatric fractures around the wrist is very important considering their prevalence. There is a specific belief that pediatric fractures can heal easily because of remodeling, but not all fractures can heal without proper treatment. Complications such as growth problems, nonunion can occur if the fracture is not treated properly. This paper reviewed recent articles about distal radius fractures, Galeazzi-equivalent fractures, and carpal bone fractures, including scaphoid fractures in children and adolescents. Successful treatment can be achieved without complications when an accurate diagnosis and proper non-surgical or surgical treatment are performed based on this article.
Keywords
Wrist fracture, Distal radius fracture, Galeazzi-equivalent fracture, Scaphoid fracture, Nonunion, Physeal arrest
Figures

Fig. 1
Manual reduction of a displaced distal radius fracture (A → B → C → D). The dorsally displaced distal bone fragment was extended and pulled until the distal bone fragment's dorsal fracture surface contacted the dorsal fracture surface of the proximal bone fragment and was then bent to the palmar side to reduce.

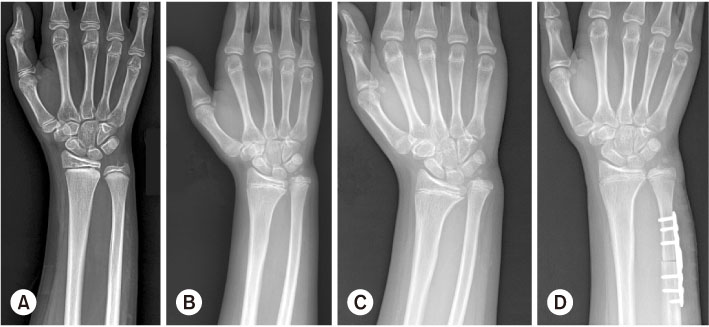
Fig. 3
(A) Distal radius physeal fracture swith Salter–Harris type I. (B) After eight months, the physeal gap was narrowed, and physeal arrest is suspected. (C) After one year nine months, the ulnar was longer than the radius due to physeal arrest of the distal radius physis (ulnar impaction). (D) Ulnar shortening was performed. The residual growth of the distal ulnar bone was expected to be about 1 cm. Complete epiphysiodesis of the distal radial and ulnar growth plate was performed to prevent further deformity.

Fig. 4
Galeazzi fracture (A, B) and Galeazzi-equivalent fracture (C, D). Unlike a Galeazzi fracture-dislocation, the distal radio-ulnar joint is preserved in the Galeazzi-equivalent fracture.

Fig. 5
A 15-year-old boy's scaphoid fracture (A) was treated by percutaneous screw fixation (B). The scaphoid nonunion (C) was observed six months after surgery. There was no evidence of bony sclerosis, necrosis, or cyst on magnetic resonance imaging (D), and the subtle bony union was noted on the medial side. Additional cast fixation was performed for six weeks, and then complete healing (E) was observed.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Randsborg PH, Gulbrandsen P, Saltytė Benth J, et al. Fractures in children: epidemiology and activity-specific fracture rates. J Bone Joint Surg Am 2013;95:e42.
-
-
Naranje SM, Erali RA, Warner WC Jr, Sawyer JR, Kelly DM. Epidemiology of pediatric fractures presenting to emergency departments in the United States. J Pediatr Orthop 2016;36:e45–e48.
-
-
Khosla S, Melton LJ 3rd, Dekutoski MB, Achenbach SJ, Oberg AL, Riggs BL. Incidence of childhood distal forearm fractures over 30 years: a population-based study. JAMA 2003;290:1479–1485.
-
-
Williams AA, Lochner HV. Pediatric hand and wrist injuries. Curr Rev Musculoskelet Med 2013;6:18–25.
-
-
Miller BS, Taylor B, Widmann RF, Bae DS, Snyder BD, Waters PM. Cast immobilization versus percutaneous pin fixation of displaced distal radius fractures in children: a prospective, randomized study. J Pediatr Orthop 2005;25:490–494.
-
-
McQuinn AG, Jaarsma RL. Risk factors for redisplacement of pediatric distal forearm and distal radius fractures. J Pediatr Orthop 2012;32:687–692.
-
-
Chia B, Kozin SH, Herman MJ, Safier S, Abzug JM. Complications of pediatric distal radius and forearm fractures. Instr Course Lect 2015;64:499–507.
-
-
Nellans KW, Kowalski E, Chung KC. The epidemiology of distal radius fractures. Hand Clin 2012;28:113–125.
-
-
Faulkner RA, Davison KS, Bailey DA, Mirwald RL, Baxter-Jones AD. Size-corrected BMD decreases during peak linear growth: implications for fracture incidence during adolescence. J Bone Miner Res 2006;21:1864–1870.
-
-
Shah NS, Buzas D, Zinberg EM. Epidemiologic dynamics contributing to pediatric wrist fractures in the United States. Hand(NY) 2015;10:266–271.
-
-
Schoenecker JG, Bae DS. Fractures of the distal radius and ulna. In: Flynn JM, Skaggs DL, Waters PM, editors. Rockwood and Wilkins' fractures in children. 8th ed. Philadelphia: Wolters Kluwer Health; 2015. pp. 349-412.
-
-
Bae DS, Waters PM. Pediatric distal radius fractures and triangular fibrocartilage complex injuries. Hand Clin 2006;22:43–53.
-
-
Egol KA, Koval KJ, Zuckerman JD. In: Handbook of fractures. 4th ed. Philadelphia: Lippincott, Williams & Wilkins; 2010.
-
-
Bae DS, Howard AW. Distal radius fractures: what is the evidence? J Pediatr Orthop 2012 32 Suppl 2:S128–S130.
-
-
Hang JR, Hutchinson AF, Hau RC. Risk factors associated with loss of position after closed reduction of distal radial fractures in children. J Pediatr Orthop 2011;31:501–506.
-
-
Luther G, Miller P, Waters PM, Bae DS. Radiographic evaluation during treatment of pediatric forearm fractures: implications on clinical care and cost. J Pediatr Orthop 2016;36:465–471.
-
-
Valverde JA, Albiñana J, Certucha JA. Early posttraumatic physeal arrest in distal radius after a compression injury. J Pediatr Orthop B 1996;5:57–60.
-
-
Waters PM, Bae DS, Montgomery KD. Surgical management of posttraumatic distal radial growth arrest in adolescents. J Pediatr Orthop 2002;22:717–724.
-
-
Eberl R, Singer G, Schalamon J, Petnehazy T, Hoellwarth ME. Galeazzi lesions in children and adolescents: treatment and outcome. Clin Orthop Relat Res 2008;466:1705–1709.
-
-
Voigt C, Lill H. [Combined injuries of the forearm - Monteggia, Galeazzi and Essex-Lopresti lesions]. Aktuelle Traumatol 2004;34:270–277.
-
-
Walsh HP, McLaren CA, Owen R. Galeazzi fractures in children. J Bone Joint Surg Br 1987;69:730–733.
-
-
Rodríguez-Merchán EC. Pediatric fractures of the forearm. Clin Orthop Relat Res 2005;(432):65–72.
-
-
Imatani J, Hashizume H, Nishida K, Morito Y, Inoue H. The Galeazzi-equivalent lesion in children revisited. J Hand Surg Br 1996;21:455–457.
-
-
Mitsui Y, Yagi M, Gotoh M, Inoue H, Nagata K. Irreducible Galeazzi-equivalent fracture in a child: an unusual case. J Orthop Trauma 2009;23:76–79.
-
-
Christodoulou AG, Colton CL. Scaphoid fractures in children. J Pediatr Orthop 1986;6:37–39.
-
-
Brudvik C, Hove LM. Childhood fractures in Bergen, Norway: identifying high-risk groups and activities. J Pediatr Orthop 2003;23:629–634.
-
-
Gholson JJ, Bae DS, Zurakowski D, Waters PM. Scaphoid fractures in children and adolescents: contemporary injury patterns and factors influencing time to union. J Bone Joint Surg Am 2011;93:1210–1219.
-
-
Evenski AJ, Adamczyk MJ, Steiner RP, Morscher MA, Riley PM. Clinically suspected scaphoid fractures in children. J Pediatr Orthop 2009;29:352–355.
-
-
Cook PA, Yu JS, Wiand W, Cook AJ 2nd, Coleman CR, Cook AJ. Suspected scaphoid fractures in skeletally immature patients: application of MRI. J Comput Assist Tomogr 1997;21:511–515.
-
-
Goodell PB, Bauer A. Problematic pediatric hand and wrist fractures. JBJS Rev 2016;4:01874474-201605000-00003
-
-
Chloros GD, Themistocleous GS, Wiesler ER, Benetos IS, Efstathopoulos DG, Soucacos PN. Pediatric scaphoid nonunion. J Hand Surg Am 2007;32:172–176.
-
-
Toh S, Miura H, Arai K, Yasumura M, Wada M, Tsubo K. Scaphoid fractures in children: problems and treatment. J Pediatr Orthop 2003;23:216–221.
-
-
Oestreich K, Jacomel TUY, Hassan S, Horwitz MD, Lindau TR. Pediatric scaphoid nonunions: a case series, review of the literature, and evidence-based guidelines. J Wrist Surg 2020;9:2–12.
-
-
Kadar A, Morsy M, Sur YJ, Akdag O, Moran SL. Capitate fractures: a review of 53 patients. J Hand Surg Am 2016;41:e359–e366.
-
-
Goddard N. Carpal fractures in children. Clin Orthop Relat Res 2005;(432):73–76.
-
 Cite
Cite- Related articles

