 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Review Articles
- Definitive fixation for traumatic pelvic ring injuries: a dynamically informed, posterior-referenced framework
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(2):73-82. Published online March 24, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00045
-
 Abstract
Abstract
 PDF
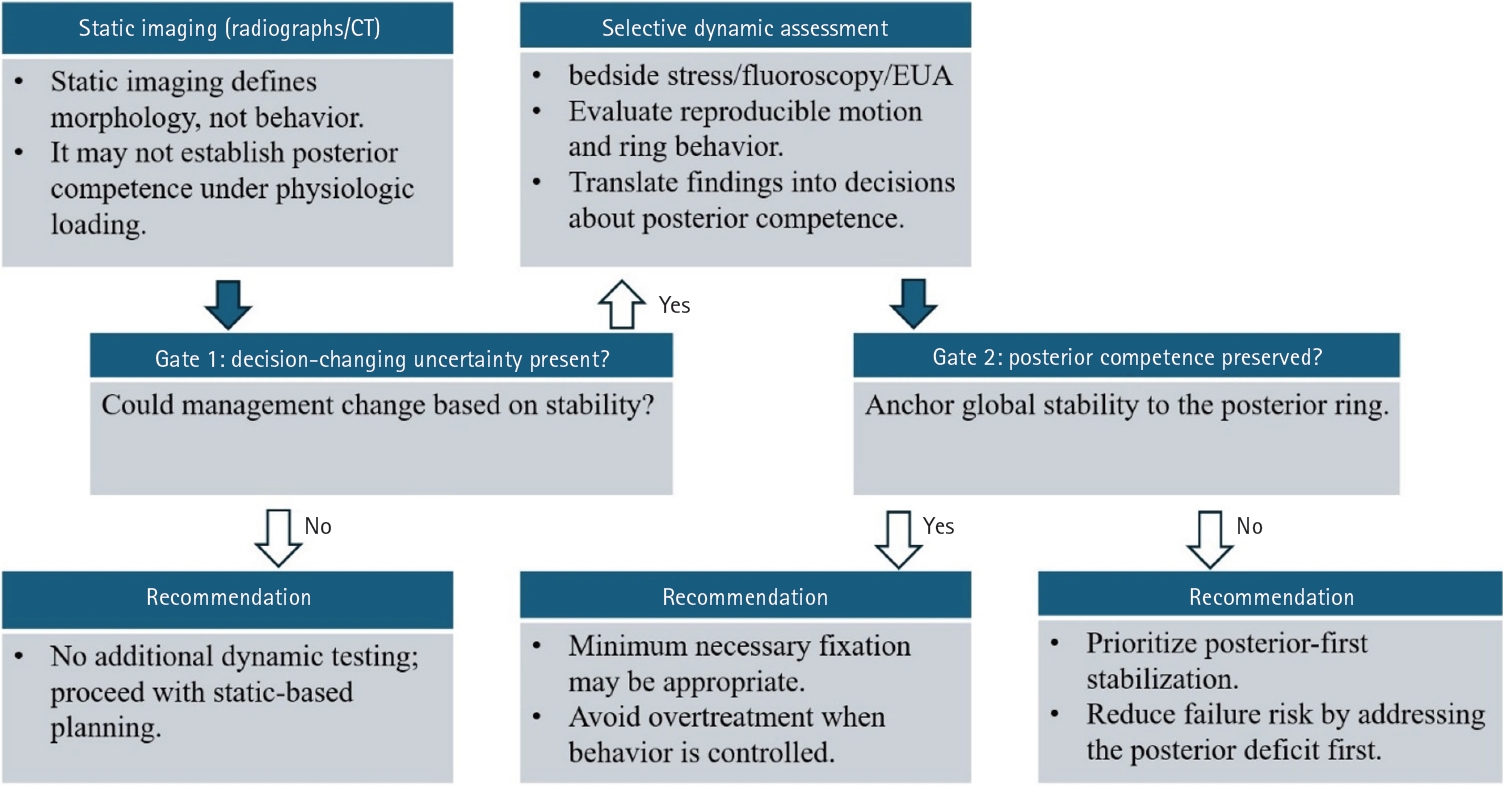
PDF - Optimal definitive fixation for traumatic pelvic ring injuries remains challenging because static radiographs and computed tomography, although essential for defining morphology, do not consistently predict load-dependent behavior during early mobilization. This uncertainty contributes to substantial practice variation and continued reliance on simplified displacement thresholds, such as the 2.5 cm rule. Such rules can misclassify instability by underrepresenting posterior competence and by privileging static measurements over functional behavior. In this narrative review, we propose a dynamically informed, posterior- referenced framework composed of three linked elements: (1) decision-linked terminology that explicitly distinguishes dynamic instability, radiographic change, and clinical failure; (2) selective stress-based assessment when uncertainty is likely to alter management; and (3) escalation along a fixation continuum that weighs incremental stability against operative burden. When static imaging cannot establish posterior competence with confidence, we outline selective stress-based approaches to assess pelvic ring behavior and to translate demonstrated instability into fixation selection along a defined continuum. Across all steps, the framework emphasizes minimum necessary fixation and explicitly incorporates the cost of selection as a primary decision variable. The operative question, therefore, shifts from gap width alone to clinically relevant motion and preservation of posterior competence. In doing so, this approach aims to reduce both undertreatment and overtreatment and to improve the consistency and defensibility of definitive fixation strategies across diverse practice environments.
- 454 View
- 21 Download

- Avulsion fractures around the hip joint and pelvis
- Won-Sik Choy, Yonghan Cha, Jung-Taek Kim, Jun-Il Yoo, Jin-Woo Kim
- J Musculoskelet Trauma 2025;38(2):53-62. Published online March 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00010
-
Abstract
PDF
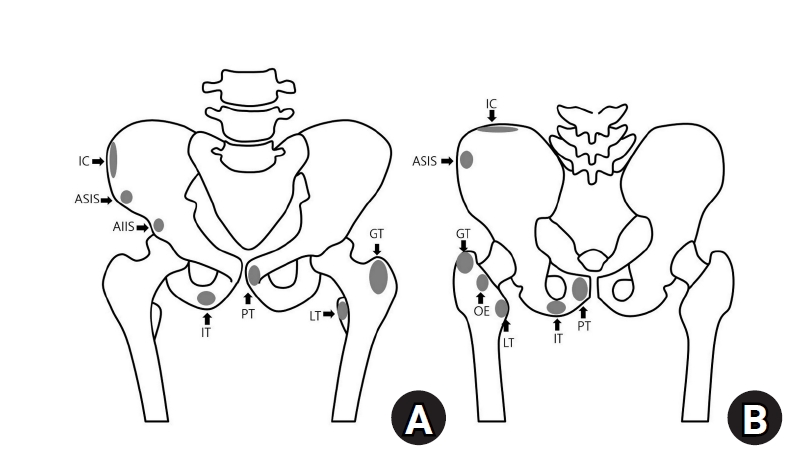
- Avulsion fractures occur when tendons or ligaments are subjected to forces greater than they can withstand at the apophysis or enthesis, regardless of fusion status. The pelvis and hip joint are vulnerable to these injuries due to the diverse muscular structures in these structures, which serve as origins for multiple muscles leading to the lower extremities. Pelvic avulsion fractures commonly affect young athletes, but can also occur in adults. The diagnosis typically involves assessing trauma history, a clinical examination, and radiographic imaging. If the diagnosis is unclear, additional tests such as computed tomography and magnetic resonance imaging may assist in the diagnosis and provide useful information for treatment decisions. While most avulsion fractures respond well to conservative treatment, surgical intervention may be preferred in severe displacements, cases of significant retraction in active athletes, or when a faster recovery is necessary. Chronic or neglected injuries may lead to excessive osseous formation around the pelvis, causing impingement syndromes. Recognizing characteristic radiological findings based on pelvic anatomy helps to make an accurate diagnosis, as chronic injuries can mimic tumors or infectious conditions, necessitating a careful differential diagnosis.
-
Citations
Citations to this article as recorded by
- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
Dawid Bartosik, Bartlomiej Cwikla, Anna Kowalczyk, Michalina Loson-Kawalec, Anna Palka-Szymaniec, Bartosz Starzynski, Alina Keska, Jakub Szkuta, Klaudia Wojcik
Cureus.2026;[Epub] CrossRef - Outcomes of Conservative Versus Surgical Treatment of Adolescent Pelvic and Hip Avulsion Fractures: A Systematic Review and Meta-Analysis
Lindsey L. Molina, Andrew M. Block, Sasha Carsen, Allison E. Crepeau, Tyler J. Stavinoha, Michael M. Chau, Jeffrey J. Nepple
Journal of Pediatric Orthopaedics.2026;[Epub] CrossRef
- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
- 13,591 View
- 178 Download
- 2 Crossref
- Easily missed nondisplaced fractures accompanying complete fractures in the lower extremity and pelvis: a narrative review
- Young-Chang Park
- J Musculoskelet Trauma 2025;38(1):5-12. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00017

-
Abstract
PDF
- Nondisplaced fractures accompanying complete fractures are often difficult to detect on plain radiographs or computed tomography scans, posing a diagnostic challenge. The diagnosis of these frequently overlooked injuries can be delayed, potentially leading to suboptimal patient outcomes. This review discusses four commonly missed fracture patterns in the lower extremity and pelvis, including posterior involvement in fragility fractures of the pelvis, intertrochanteric extensions in isolated greater trochanter fractures, ipsilateral femoral neck fractures in high energy femoral shaft fractures, and posterior malleolar fractures in distal spiral tibial shaft fractures. An accurate diagnosis of these accompanying nondisplaced fractures is critical for optimizing surgical outcomes. Surgeons should incorporate thorough preoperative evaluations into their clinical practice to facilitate early detection and appropriate treatment strategies. Prompt identification and comprehensive management remain essential for improving patient outcomes.
-
Citations
Citations to this article as recorded by- Selective Anterior Fixation for Rami Fractures in Anteroposterior Compression-Type Pelvic Ring Injuries: Impact of Posterior Stability
Jeong-Hyun Koh, Sumin Lim, Won-Tae Cho, Seungyeob Sakong, Wan-Sun Choi, Daehyun Han, Hyung Keun Song
Journal of Clinical Medicine.2026; 15(10): 3773. CrossRef
- Selective Anterior Fixation for Rami Fractures in Anteroposterior Compression-Type Pelvic Ring Injuries: Impact of Posterior Stability
- 2,245 View
- 59 Download
- 1 Crossref
- Avulsion Fractures around the Hip Joint and Pelvis
- Ha-Yong Kim, Hajun Jang, Jung-Taek Kim, Jin-Woo Kim, Jun-Il Yoo, Won-Sik Choy, Yonghan Cha
- J Korean Fract Soc 2024;37(3):150-157. Published online July 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.3.150
-
Abstract
PDF
- Avulsion fractures occur when tendons or ligaments are subjected to forces greater than they can withstand at the apophysis or enthesis, regardless of the fusion status. Given the diverse muscular structures around the pelvis and hip joint, which serve as origins for multiple muscles leading to the lower extremities, these areas are vulnerable to such injuries. Pelvic avulsion fractures commonly af-fect young athletes, but they can also occur in adults. Diagnosis typically involves assessing the trauma history, clinical examination, and radiographic imaging. In cases of unclear diagnosis, additional tests, such as computed tomography or magnetic resonance imaging, may assist in treatment decisions and diagnosis. Although most avulsion fractures respond well to conservative treatment, surgical interven-tion may be preferred in severe displacements, significant retraction in active athletes, or when a faster recovery is necessary. Chronic or neglected injuries may lead to excessive osseous formation around the pelvis, causing impingement syndromes. Recognizing the characteristic radiological findings based on the pelvic anatomy aids in accurate diagnosis because chronic injuries might mimic tumors or infectious conditions, necessitating a careful differential diagnosis.
- 2,112 View
- 49 Download
- Fragility Fractures of the Pelvis and Sacrum
- Se-Won Lee, Ju-Yeong Kim
- J Korean Fract Soc 2023;36(1):29-38. Published online January 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.1.29
-
Abstract
PDF
- The incidence of fragility fractures of the pelvis (FFP) has increased significantly due to the aging popu-lation and improved diagnostic modalities. The evaluation and treatment of these patients differ from that of high-energy pelvic ring injuries typically seen in younger patients. Therefore, it is important to classify the FFP by patterns of the classification system to standardize optimal treatment criteria and appropriate treatment strategy. However, some cases are not classifiable according to the FFP classifi-cation. A newly proposed classification that can be verified by comparing existing FFP classifications is needed to overcome the weak points. Non-operative treatment is usually considered first and should focus on early mobilization. Operative fixation should focus on stabilizing the minimally invasive pelvic ring than the reduction of fractures to facilitate early mobilization and avoid complications that can arise from comorbidities associated with immobility.
- 2,477 View
- 44 Download
- Fixation Options of Unstable Posterior Pelvic Ring Disruption: Ilio-Sacral Screw Fixation, S2AI Fixation, Posterior Tension Band Plate Fixation, and Spino-Pelvic Fixation
- Dong Hee Kim, Jae Hoon Jang, Myungji Shin, Gu Hee Jung
- J Korean Fract Soc 2019;32(4):240-247. Published online October 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.4.240
-
Abstract
PDF
- The fixation methods that can be used for unstable posterior pelvic ring injuries have undergone many innovative changes due to the recent development of surgical and imaging techniques. After understanding the appropriate indications of first and second sacroiliac screw fixation and spinopelvic fixation, innovative methods, including the trans-sacral screw fixation, posterior tension-band plate fixation, and the S2AI screw, would be chosen and applied. Considering the anatomical complexity and proximity to the surrounding vessels and nerves in the posterior fixation, the safe zone according to the fixation options should be well understood in preoperative planning. Moreover, the functional reduction of the posterior pelvic ring through the reduction and fixation of the anterior lesion should be achieved before placing the implant to reduce the number of malposition-related complications.
-
Citations
Citations to this article as recorded by- Clinical Research through Computational Anatomy and Virtual Fixation
Ju Yeong Kim, Dong-Geun Kang, Gu-Hee Jung
Journal of the Korean Orthopaedic Association.2023; 58(4): 299. CrossRef
- Clinical Research through Computational Anatomy and Virtual Fixation
- 1,450 View
- 19 Download
- 1 Crossref
- Pelvis/Acetabular Fractures in the Elderly: When and How to Fix?
- Kyeong Hyeon Park, Chang Wug Oh, Joon Woo Kim
- J Korean Fract Soc 2018;31(3):102-113. Published online July 31, 2018
- DOI: https://doi.org/10.12671/jkfs.2018.31.3.102
-
Abstract
PDF
- Owing to the increase in life expectancy, the incidence of osteoporotic fracture of the pelvis and acetabulum is increasing. Fractures in the elderly population is different from those in younger patients. Pelvic ring and acetabular fractures in geriatric patients are more likely the result of low-energy trauma, but the outcomes are generally poorer than those of the younger population. Multiple management options are available, but no intervention has become the standard of care for these fractures in the elderly. A treatment strategy should be established depending on the state of the individual patient. Regardless of whether nonsurgical or surgical treatment is selected, early ambulation should be considered to avoid the complications associated with prolonged immobilization.
-
Citations
Citations to this article as recorded by- Effect of Korean Medicine Treatments for Pain Reduction in Patients with Hip Fracture : A Retrospective Observational Study
Nam Hoon Kim, Min Seok Oh
Journal of Physiology & Pathology in Korean Medicine.2020; 34(5): 263. CrossRef
- Effect of Korean Medicine Treatments for Pain Reduction in Patients with Hip Fracture : A Retrospective Observational Study
- 737 View
- 6 Download
- 1 Crossref
Original Articles
- Clinical Features and Outcomes of Pelvic Insufficiency Fractures
- Yong Min Seo, Young Chang Kim, Ji Wan Kim
- J Korean Fract Soc 2017;30(4):186-191. Published online October 31, 2017
- DOI: https://doi.org/10.12671/jkfs.2017.30.4.186
-
Abstract
PDF
- PURPOSE
The purpose of this study was to investigate the radiological and epidemiological characteristics, as well as the clinical course of pelvic insufficiency fractures in the elderly population.
MATERIALS AND METHODS
At a Haeundae Paik Hospital, we retrospectively reviewed patients with pelvic insufficiency fractures between March 2010 and May 2017. The demographic data of patients were analyzed, and bone mineral density and bone turnover markers were evaluated to estimate the metabolic status of the bone. The radiological characteristics were evaluated by comparing the simple x-ray images with the computed tomography images, and the types of fractures were classified via computed tomography images. For clinical course evaluation, we investigated comorbid complications, and compared the walking ability scale before and 6 months after the fracture.
RESULTS
A total of 42 patients were included, with an average age of 76.5 years. All were female except one case. In 5 cases where the initial medical examination was from another institution, the fracture was not found in 3 cases. All cases received conservative treatment. After the diagnosis of pelvic bone fracture using a simple x-ray imaging, additional fractures were found in 81.0% of the study population using a computed tomography. Initiation of gait occurred at an average of 2.8 weeks, and every case except 1 (97.6%) fully recovered their gait ability.
CONCLUSION
We concluded that there was a limitation with diagnosing pelvic insufficiency fracture using only a simple x-ray imaging technique. In general, cases in this study showed conservative treatment yielded favorable clinical outcome with relatively less critical complications.
- 728 View
- 1 Download
- Usefulness of Spring Plate for Acetabular Posterior Wall Fracture Including Small Fragment
- Jeong Hoon Kang, Sang Hong Lee, Hyeon Jun Lee
- J Korean Fract Soc 2016;29(1):19-25. Published online January 31, 2016
- DOI: https://doi.org/10.12671/jkfs.2016.29.1.19
-
Abstract
PDF
- PURPOSE
We applied internal fixation using a spring plate against an acetabular posterior wall fracture including small fragments and then evaluated the clinical and radiological results and want to understand the usefulness of the spring plate.
MATERIALS AND METHODS
Fifteen patients in whom fixation was difficult using leg screws or a metal plate because of a small bone fragment, in patients with posterior wall acetabular fractures who presented in our hospital since August of 2011 to March of 2014 were enrolled. The mean age was 42.6 years (range 24-54 years) with relatively young patients, and they were followed-up for at least one year. We analyzed the rate of reduction after surgery using the classification of Matta in radiographs, and the classification of Borrelli in 3-dimensional computed tomography (CT) and clinical results were evaluated using the clinical grading system.
RESULTS
There were five cases of anatomical reduction, 9 cases of imperfect reduction, and 1 case of unsatisfactory reduction according to the classification of Matta. Except for one case during the follow-up period, the union of bone was successful without failure of fixation and the clinical results were 6 cases of excellence, 8 cases of good, and 1 case of failure. Articular displacement was also evaluated in postoperative CT scan according to Borrelli's criteria. The mean of gap and step off was 2.04 mm, 1.3 mm.
CONCLUSION
Use of leg screw fixation and so on in posterior wall fractures including a small fragment of the acetabular rim is not easy. However the method using spring plate fixation enables relatively accurate reduction and fixation for a small fragment and the clinical outcome showed satisfactory results. -
Citations
Citations to this article as recorded by- Biomechanical Comparison of Fixation Methods for Posterior Wall Fractures of the Acetabulum: Conventional Reconstruction Plate vs. Spring Plate vs. Variable Angle Locking Compression Plate
HoeJeong Chung, Hoon-Sang Sohn, Jong-Keon Oh, Sangho Lee, DooSup Kim
Medicina.2024; 60(6): 882. CrossRef
- Biomechanical Comparison of Fixation Methods for Posterior Wall Fractures of the Acetabulum: Conventional Reconstruction Plate vs. Spring Plate vs. Variable Angle Locking Compression Plate
- 919 View
- 6 Download
- 1 Crossref
Review Article
- Surgical Treatment of Malunion and Nonunion after Pelvic Bone Fracture
- Byung Woo Min, Kyung Jae Lee
- J Korean Fract Soc 2015;28(4):266-272. Published online October 31, 2015
- DOI: https://doi.org/10.12671/jkfs.2015.28.4.266
-
Abstract
PDF
- Regardless of the efforts of several treatments after pelvic bone fracture, as many as 5% of all pelvic fractures result in malunion or nonunion of the pelvis. These complications can cause disabling symptoms, including pain, instability, and gait disturbance, which can decrease life quality of patients and increase socioeconomic problems. Therefore concerns regarding the treatment of malunion and nonunion after pelvic bone fracture are increasing. We report our experience and surgical management for pelvic malunion and nonunion.
- 1,009 View
- 11 Download
Original Articles
- Neurologic Injury within Pelvic Ring Injuries
- Ji Wan Kim, Dong Hoon Baek, Jae Hyun Kim, Young Chang Kim
- J Korean Fract Soc 2014;27(1):17-22. Published online January 31, 2014
- DOI: https://doi.org/10.12671/jkfs.2014.27.1.17
-
Abstract
PDF
- PURPOSE
To evaluate the incidence of neurologic injury in pelvic ring injuries and to assess the risk factors for neurologic injury related to pelvic fractures.
MATERIALS AND METHODS
Sixty-two patients with the pelvic ring injury were enrolled in the study from March 2010 to May 2013. When the neurologic injury was suspected clinically, the electro-diagnostic tests were performed. Combined injuries, fracture types, and longitudinal displacements were examined for correlations with the neurologic injury.
RESULTS
There were 7 cases of AO/OTA type A, 37 cases of type B, and 18 cases of type C. Among them, 25 patients (40%) had combined spine fractures, and the average of longitudinal displacement was 7 mm (1-50 mm). Of the 62 patients, 13 (21%) had neurologic injury related with pelvic fractures; 5 with lumbosacral plexus injury, 5 with L5 or S1 nerve injury, 2 with obturator nerve injury, and 1 case of lateral femoral cutaneous nerve injury. There were no relationships between the neurologic injuries and fracture types (p=0.192), but the longitudinal displacements of posterior ring and combined spine fractures were related to the neurologic injury within pelvic ring injury (p=0.006, p=0.048).
CONCLUSION
The incidence of neurologic injury in pelvis fracture was 21%. In this study, the longitudinal displacements of posterior ring and combined spine fractures were risk factors for neurological injury in pelvic ring injury. -
Citations
Citations to this article as recorded by- Surgical Outcome of Posterior Pelvic Fixation Using S1, S2 Screws in Vertically Unstable Pelvic Ring Injury
Kwang Hee Yeo, Nam Hoon Moon, Jae Min Ahn, Jae Yoon Jeong, Jae Hoon Jang
Journal of the Korean Fracture Society.2018; 31(1): 9. CrossRef
- Surgical Outcome of Posterior Pelvic Fixation Using S1, S2 Screws in Vertically Unstable Pelvic Ring Injury
- 884 View
- 6 Download
- 1 Crossref
- Anatomical Study of Symphysis Pubis Using 3 Dimensional Computed Tomography in Koreans
- Ji Wan Kim, Jung Min Park, Jae Suk Chang
- J Korean Fract Soc 2013;26(1):32-36. Published online January 31, 2013
- DOI: https://doi.org/10.12671/jkfs.2013.26.1.32
-
Abstract
PDF
- PURPOSE
To acquire anatomical data for the normal pelvic bone structure using three-dimensional computed tomography (3D CT) and to propose the most appropriate angle and screw length for safe screw insertion during symphysis pubis plating.
MATERIALS AND METHODS
We performed 3D CT analysis in 52 patients who required plating and selected a medial and lateral insertion point between the symphysis pubis and the pubic tubercle. Using a three-dimensional medical image analysis program, we evaluated the appropriate screw length, sagittal angle, and oblique angle at each point in this cohort.
RESULTS
At the medial point, the sagittal angle was determined to be 49.1degrees with an average screw length of 49.4 mm. At the lateral point, we calculated an average screw length of 49.1 mm, oblique angle of 23.2degrees, and sagittal angle of 45.7degrees. The screw length was longer in men than in women (4.6 mm and 7.3 mm, respectively) at the medial and lateral point.
CONCLUSION
At the symphysis pubis diastasis, we can insert the screw caudally at 49degrees with a minimal length of 37 mm at the medial point. We can insert the screw caudally at 46degrees, medially at 23degrees, with a minimal 34 mm length at the lateral point.
- 757 View
- 3 Download
- The Incidence of Venous Thromboembolism in Trauma Patients with Pelvic or Acetabular Fracture
- Ji Wan Kim, Hyun Wook Chung, Young Chang Kim
- J Korean Fract Soc 2012;25(4):250-256. Published online October 31, 2012
- DOI: https://doi.org/10.12671/jkfs.2012.25.4.250
-
Abstract
PDF
- PURPOSE
To evaluate the incidence of venous thromboembolism (VTE) in trauma patients with pelvic or acetabular fracture and determine high risk factors.
MATERIALS AND METHODS
Twenty-three patients who had a pelvic or acetabular fracture were enrolled between March 2011 and February 2012. All patients had mechanical and chemical prophylaxis and underwent deep vein thrombosis (DVT) computed tomography around 2 weeks after injury for evaluation of VTE. The relationships between VTE and each of sex, age, body mass index, injury severity score, intensive care unit stay, transfusion, operation time, coagulopathy, and associated injury were analyzed.
RESULTS
A total of 8 patients developed VTE (34.8%), of which 5 had DVT, 2 had pulmonary embolism (PE), and one had both DVT and PE. The group with a VTE risk score of 14 or more had a significantly higher incidence of VTE.
CONCLUSION
Careful attention is needed in management of patients with pelvic or acetabular fracture. -
Citations
Citations to this article as recorded by- Knowledge, Health Belief, and Preventive Behavioral Intention related to Venous Thromboembolism (VTE) of the Patients with Lower Limb Musculoskeletal System Disorders
Hye Jin Yang, Hee-Young Kang
The Journal of Korean Academic Society of Nursing Education.2013; 19(4): 531. CrossRef
- Knowledge, Health Belief, and Preventive Behavioral Intention related to Venous Thromboembolism (VTE) of the Patients with Lower Limb Musculoskeletal System Disorders
- 1,304 View
- 6 Download
- 1 Crossref
Case Report
- Bowel Entrapment by Fragments of Acetabular Fracture: A Case Report
- Ji Wan Kim, Jung Jae Kim, Suk Kyung Hong, Kyu Hyuk Kyung, Jin Hee Kim
- J Korean Fract Soc 2010;23(4):373-376. Published online October 31, 2010
- DOI: https://doi.org/10.12671/jkfs.2010.23.4.373
-
Abstract
PDF
- Abdominal injuries are common in patients with pelvic or acetabular fracture. However intestinal entrapment or perforation caused by fragments of a pelvic or acetabular fracture is rare and to date there has been no report of this occurring in Korea so far. As it is difficult to diagnose intestinal entrapment caused by fragments of pelvic or acetabular fracture, the entrapment therefore results in intestinal perforation, sepsis, and a high mortality rate in the absence of early detection. We present a case of intestinal entrapment and perforation caused by fragments of acetabular fracture as well as a literature review.
- 514 View
- 0 Download
Original Articles
- Separation of the Symphysis Pubis during Childbirth
- Dong Ju Shin, Young Soo Byun, Se Ang Chang, Ok Rang Park, Shin Yoon Kim, Dae Hee Hwang, Sung Rak Lee, Dong Young Kim
- J Korean Fract Soc 2006;19(4):412-417. Published online October 31, 2006
- DOI: https://doi.org/10.12671/jkfs.2006.19.4.412
-
Abstract
- PURPOSE
To evaluate the clinical features and incidence of separation of the symphysis pubis during childbirth, and to evaluate the risk factors of the lesion and the outcome of treatment.
MATERIALS AND METHODS
Seventy two cases of separation of symphysis pubis among 66,721 delivery between January 1992 and December 2004 was selected. The control group was composed of 498 cases without separation of symphysis pubis during childbirth. Several factors increasing the risk of this lesion were assessed using χ
- 512 View
- 0 Download
- Prognosis of early internal fixation in unstable pelvic fractures
- Jang Yeol Lee, Do Hun Moon, Gun Beom Kim
- J Korean Soc Fract 2000;13(4):741-748. Published online October 31, 2000
- DOI: https://doi.org/10.12671/jksf.2000.13.4.741
-
Abstract
PDF
- PURPOSE
This study was conducted to analyze the clinical prognosis of early internal fixation in unstable pelvic fracture. MATERIAL AND METHOD: We analyzed the sixteen patients. The average age of the patients was 34 years(range, 21-64 years). They were followed up for average 21 months. The sixteen pelves were classified by Tile ; Type B 3 cases, Type C 13 cases. Nine patients(56%) had the associated injuries. In 13 patients(81%), internal fixation were performed within 3 weeks after the injury. Fixation was accomplished by the plates and screws. We assessed the functional, radiological results and postoperative complications.
RESULTS
Fourteen(88%) patients were fully ambulatory, had no limp, did not need assistive devices. Fifty percents of the patients had returned to the previous jobs and 31% had to change the jobs. On radiolograph, there were 14 excellent and 2 good reduction. Three postoperative complications happened ; two superficial infections and one lumbar neuropathy, which resolved spontaneously. Three patients with associated injuries, who had delayed fixation, appealed gait disturbance and chronic pain.
CONCLUSION
early internal fixation of unstable pelvic ring fractures may be expected to yield satisfactory functional success and radiologic results in the majority of patients -
Citations
Citations to this article as recorded by- Intrapelvic Anterior Plate Fixation for Crescent Fracture-Dislocation of Sacroiliac Joint
Kwang-Jun Oh, Jin-Ho Choi
Journal of the Korean Fracture Society.2013; 26(3): 184. CrossRef - Surgical Fixation of Sacroiliac Joint Complex in Unstable Pelvic Ring Injuries
Kwang-Jun Oh, Seok-Min Hwang
Hip & Pelvis.2012; 24(2): 139. CrossRef - Operative Treatment of Unstable Pelvic Ring Injury
Sang Hong Lee, Sang Ho Ha, Young Kwan Lee, Sung Won Cho, Sang Soo Park
Journal of the Korean Fracture Society.2012; 25(4): 243. CrossRef - Crescent Fracture-dislocation of Sacroiliac Joint: Affecting Factors of Operative Results
Hee-Soo Kim, Chang-Wug Oh, Poong-Taek Kim, Young-Soo Byun, Joo-Woo Kim, Byung-Chul Park, Woo-Kie Min, Hyun-Joo Lee
Journal of the Korean Fracture Society.2009; 22(2): 71. CrossRef
- Intrapelvic Anterior Plate Fixation for Crescent Fracture-Dislocation of Sacroiliac Joint
- 857 View
- 0 Download
- 4 Crossref
- Posterior stabilization of the Unstable Pelvic Ring Fracture
- Soon Taek Jeong, Ji Yeon Kim, Se Hyun Cho
- J Korean Soc Fract 1996;9(3):513-517. Published online July 31, 1996
- DOI: https://doi.org/10.12671/jksf.1996.9.3.513
-
Abstract
PDF
- Stable pelvis fracture is easily treated by conservative treatment with little complication. Unstable pelvic ring fracture, however, is difficult to manage due to various problems. Conservative treatment is rarely indicated because prolonged traction and immobilization often lead to life-threatening complications. The malunion produces pain, limb length discrepancy and eventually poor life quality, Surgical stabilization can help easy care of patients, early mobilization and diminish the morbidity. This study is to present the clinical results of two kinds of metal fixations using seven transiliac bars and four percutaneous sacral screws for the surgical stabilization of the unstable pelvic ring fractures. Total eleven cases had been operated by the authors at Geyong-Sang national hospital from August 1991 to April 1994. They were eight male and three female patients of average forty one years in age(range, eighteen to sixty two years). The average duration of follow-up was thirty one months(range, twenty to fifty three months). All cases of sacral screw fixations revealed satisfactory results both at clinical and radiological aspects. Out of seven cases of transiliac bar fixation, there were two cases of minor infection and three cases of painful and palpable hardware requiring removal, especially in thin patients. The results confirm that sacral screw is better tolerated by thin patients in spite of risk of temporary entrapment of sacral cutaneous nerves.
- 570 View
- 1 Download
 First
First Prev
Prev

