 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 29(1); 2016 > Article
-
Original Article
- Usefulness of Spring Plate for Acetabular Posterior Wall Fracture Including Small Fragment
- Jeong Hoon Kang, M.D., Sang Hong Lee, M.D., Hyeon Jun Lee, M.D.
-
Journal of the Korean Fracture Society 2016;29(1):19-25.
DOI: https://doi.org/10.12671/jkfs.2016.29.1.19
Published online: January 19, 2016
Department of Orthopaedic Surgery, Chosun University School of Medicine, Gwangju, Korea.
- Address reprint requests to: Sang Hong Lee, M.D. Department of Orthopaedic Surgery, Chosun University Hospital, 365 Pilmun-daero, Dong-gu, Gwangju 61453, Korea. Tel: 82-62-220-3147, Fax: 82-62-226-3379, shalee@chosun.ac.kr
• Received: June 19, 2015 • Revised: September 13, 2015 • Accepted: November 12, 2015
Copyright © 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,127 Views
- 8 Download
- 1 Crossref
Abstract
-
Purpose
- We applied internal fixation using a spring plate against an acetabular posterior wall fracture including small fragments and then evaluated the clinical and radiological results and want to understand the usefulness of the spring plate.
-
Materials and Methods
- Fifteen patients in whom fixation was difficult using leg screws or a metal plate because of a small bone fragment, in patients with posterior wall acetabular fractures who presented in our hospital since August of 2011 to March of 2014 were enrolled. The mean age was 42.6 years (range 24-54 years) with relatively young patients, and they were followed-up for at least one year. We analyzed the rate of reduction after surgery using the classification of Matta in radiographs, and the classification of Borrelli in 3-dimensional computed tomography (CT) and clinical results were evaluated using the clinical grading system.
-
Results
- There were five cases of anatomical reduction, 9 cases of imperfect reduction, and 1 case of unsatisfactory reduction according to the classification of Matta. Except for one case during the follow-up period, the union of bone was successful without failure of fixation and the clinical results were 6 cases of excellence, 8 cases of good, and 1 case of failure. Articular displacement was also evaluated in postoperative CT scan according to Borrelli's criteria. The mean of gap and step off was 2.04 mm, 1.3 mm.
-
Conclusion
- Use of leg screw fixation and so on in posterior wall fractures including a small fragment of the acetabular rim is not easy. However the method using spring plate fixation enables relatively accurate reduction and fixation for a small fragment and the clinical outcome showed satisfactory results.
- 1. Baumgaertner MR. Fractures of the posterior wall of the acetabulum. J Am Acad Orthop Surg, 1999;7:54-65.Article
- 2. Letournel E. Acetabulum fractures: classification and management. Clin Orthop Relat Res, 1980;151:81-106.Article
- 3. Letournel EJR. Fracture of acetabulum. 2nd ed. New York: Springer-Verlag; 1993. p. 535-563.
- 4. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am, 1996;78:1632-1645.
- 5. Moed BR, Carr SE, Watson JT. Open reduction and internal fixation of posterior wall fractures of the acetabulum. Clin Orthop Relat Res, 2000;377:57-67.Article
- 6. Pantazopoulos T, Nicolopoulos CS, Babis GC, Theodoropoulos T. Surgical treatment of acetabular posterior wall fractures. Injury, 1993;24:319-323.Article
- 7. Eichenholtz SN, Stark RM. Central acetabular fractures; a review of thirty-five cases. J Bone Joint Surg Am, 1964;46:695-714.
- 8. Knight RA, Smith H. Central fractures of the acetabulum. J Bone Joint Surg Am, 1958;40:1 passim-16 passim.Article
- 9. Borrelli J Jr, Ricci WM, Steger-May K, Totty WG, Goldfarb C. Postoperative radiographic assessment of acetabular fractures: a comparison of plain radiographs and CT scans. J Orthop Trauma, 2005;19:299-304.
- 10. Lee SH. Conservative treatment of acetabular fracture. J Korean Hip Soc, 2004;16:291-295.
- 11. Olson SA, Bay BK, Pollak AN, Sharkey NA, Lee T. The effect of variable size posterior wall acetabular fractures on contact characteristics of the hip joint. J Orthop Trauma, 1996;10:395-402.Article
- 12. Matta JM, Anderson LM, Epstein HC, Hendricks P. Fractures of the acetabulum. A retrospective analysis. Clin Orthop Relat Res, 1986;205:230-240.
- 13. Magu NK, Gogna P, Singh A, et al. Long term results after surgical management of posterior wall acetabular fractures. J Orthop Traumatol, 2014;15:173-179.ArticlePDF
- 14. Mast J, Jakob R, Ganz R. Planning and reduction technique in fracture surgery. New York, NY: Springerverlag; 1989.
- 15. Goulet JA, Rouleau JP, Mason DJ, Goldstein SA. Comminuted fractures of the posterior wall of the acetabulum. A biomechanical evaluation of fixation methods. J Bone Joint Surg Am, 1994;76:1457-1463.Article
- 16. Richter H, Hutson JJ, Zych G. The use of spring plates in the internal fixation of acetabular fractures. J Orthop Trauma, 2004;18:179-181.Article
- 17. Han SB, Park SW, Lee SH, Chung JW, Choi GW. The use of spring plates in management of acetabular posterior wall fractures. J Korean Hip Soc, 2005;17:217-222.
- 18. Briffa N, Pearce R, Hill AM, Bircher M. Outcomes of acetabular fracture fixation with ten years' follow-up. J Bone Joint Surg Br, 2011;93:229-236.ArticlePDF
REFERENCES
Fig. 1
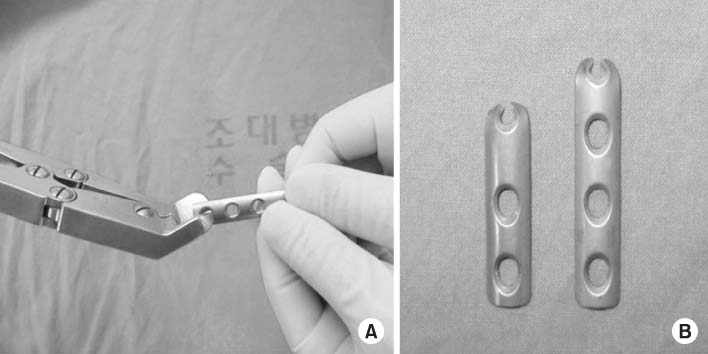
(A) Making a spring plate. The tip of the plate is cut to make the hook shape. (B) Photograph of the spring plate.
Fig. 2
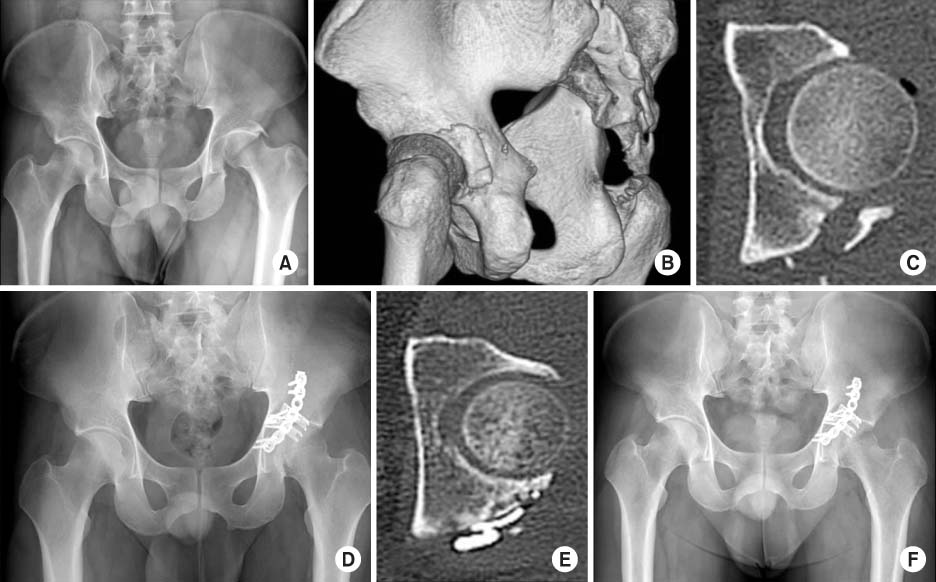
A 37-year-old male with a left hip fracutre and dislocation with an acetabular posteior wall fracture. (A) Preoperative anterioposterior radiograph of the pelvis. (B) Preoperative three dimensional computed tomography scan. (C) The small bony fragment is observed in the acetabular posterior wall. (D) Postoperative anterioposterior radiograph of the pelvis. Applying the reconstruction plate and spring plate against the fracture site for reduction. (E) Postoperative computed tomography scan shows configuration of the spring plate. (F) The anterioposterior raidograph of the pelvis after 1 year.
Table 1
![jkfs-29-19-i001.jpg]()
Patient Demographics
Table 2
![jkfs-29-19-i002.jpg]()
Quality of Reduction and Clinical Grading System (CGS)
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Biomechanical Comparison of Fixation Methods for Posterior Wall Fractures of the Acetabulum: Conventional Reconstruction Plate vs. Spring Plate vs. Variable Angle Locking Compression Plate
HoeJeong Chung, Hoon-Sang Sohn, Jong-Keon Oh, Sangho Lee, DooSup Kim
Medicina.2024; 60(6): 882. CrossRef
 Cite
CiteUsefulness of Spring Plate for Acetabular Posterior Wall Fracture Including Small Fragment
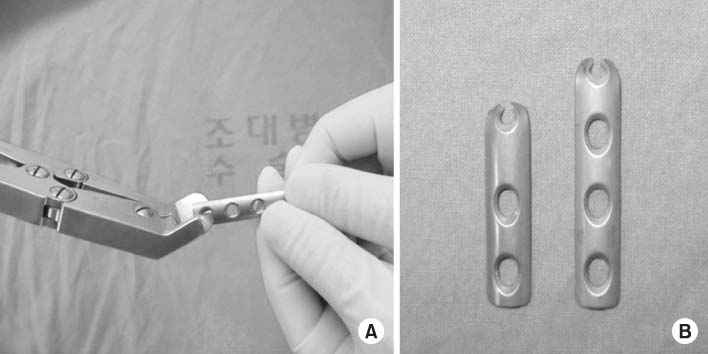
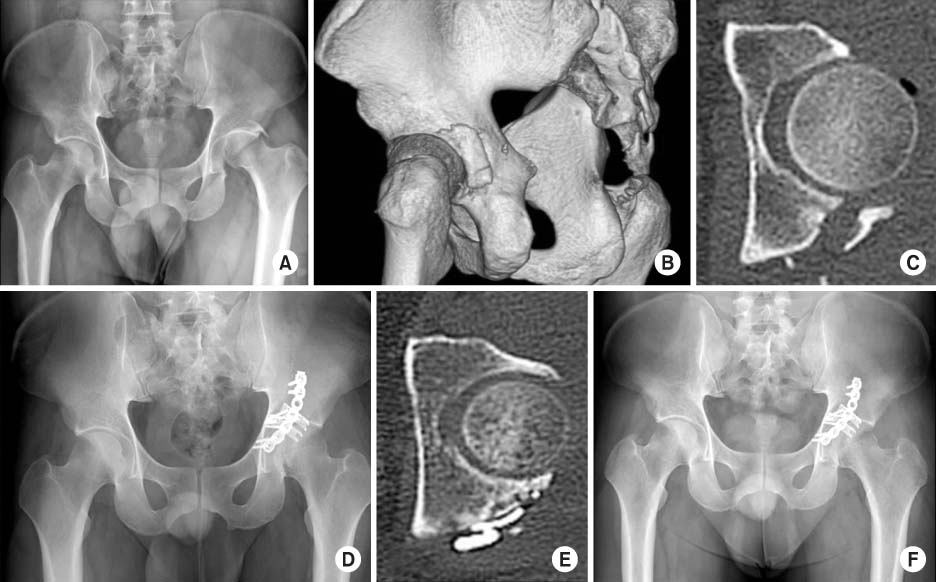
Fig. 1
(A) Making a spring plate. The tip of the plate is cut to make the hook shape. (B) Photograph of the spring plate.
Fig. 2
A 37-year-old male with a left hip fracutre and dislocation with an acetabular posteior wall fracture. (A) Preoperative anterioposterior radiograph of the pelvis. (B) Preoperative three dimensional computed tomography scan. (C) The small bony fragment is observed in the acetabular posterior wall. (D) Postoperative anterioposterior radiograph of the pelvis. Applying the reconstruction plate and spring plate against the fracture site for reduction. (E) Postoperative computed tomography scan shows configuration of the spring plate. (F) The anterioposterior raidograph of the pelvis after 1 year.
Fig. 1
Fig. 2
Usefulness of Spring Plate for Acetabular Posterior Wall Fracture Including Small Fragment
Patient Demographics
| Case No. | Age (yr)/sex | Injury mechanism | Type* | Dislocation† | Comminution |
|---|---|---|---|---|---|
| 1 | 26/male | MVA | G | III | + |
| 2 | 31/female | MVA | A | II | – |
| 3 | 48/male | MVA | F | - | + |
| 4 | 54/male | MVA | G | - | + |
| 5 | 37/male | MVA | A | II | – |
| 6 | 54/male | MVA | F | III | + |
| 7 | 53/male | MVA | A | III | + |
| 8 | 55/female | MVA | A | III | + |
| 9 | 28/male | MVA | A | - | – |
| 10 | 24/male | F/D | A | - | – |
| 11 | 55/male | PA | F | - | + |
| 12 | 41/male | F/D | A | III | + |
| 13 | 40/female | PA | A | - | – |
| 14 | 52/male | MVA | A | II | – |
| 15 | 46/male | F/D | A | II | – |
*Classification according to the standard of Judet and Letournel.
†Classification according to the standard of Thompson and Epstein. MVA: Motor vehicle accident, F/D: Fall down, PA: Pedestrian accident.
Quality of Reduction and Clinical Grading System (CGS)
| Case No. | Fixation | Duration of union | Reduction | Displacement* | CGS | Complication |
|---|---|---|---|---|---|---|
| 1 | Spring plate | 16 | Imperfect | 5.5/1.7 | Excellent | - |
| 3 cannulated screw | ||||||
| 2 | Spring plate | 12 | Anatomical | 0/0 | Excellent | - |
| 2 cancellous screw | ||||||
| 3 | Spring & reconstruction plate | 23 | Imperfect | 2.8/2.9 | Good | - |
| Cannulated screw | ||||||
| 4 | Spring & reconstruction plate | 20 | Imperfect | 0/0 | Excellent | - |
| 5 | 2 spring & reconstruction plate | 20 | Imperfect | 0.5/0.5 | Good | - |
| 6 | Spring & reconstruction plate | 18 | Imperfect | 2.6/1.6 | Excellent | - |
| Cannulated screw | ||||||
| 7 | Spring & reconstruction plate | - | Poor | 6/3 | Poor | Redislocation |
| Sciatic nerve palsy | ||||||
| 8 | Spring & reconstruction plate | 21 | Anatomical | 0.8/1.5 | Good | - |
| Cannulated screw | ||||||
| 9 | Spring & reconstruction plate | 12 | Anatomical | 0.6/1.3 | Good | - |
| 10 | Spring plate | 12 | Anatomical | 0/0 | Excellent | - |
| 11 | Spring & reconstruction plate | 18 | Imperfect | 2.5/1.9 | Good | - |
| Cannulated screw | ||||||
| 12 | Spring & reconstruction plate | 20 | Imperfect | 2/1.5 | Good | - |
| 13 | Spring & reconstruction plate | 13 | Anatomical | 0.9/0 | Excellent | - |
| 14 | Spring & reconstruction plate | 16 | Imperfect | 1.7/1 | Good | - |
| 15 | Spring & reconstruction plate | 15 | Imperfect | 2.6/2 | Good | - |
| Cannulated screw |
*Step off/gap.
Correlation between Congruency of Fracture and Functional Score*
| Mean±standard deviation | t | p-value | |
|---|---|---|---|
| Anatomical | 17.600±0.547 | 3.080 | 0.010 |
| Excellent | 15.66±1.322 |
*t-test.
Table 1
Patient Demographics
*Classification according to the standard of Judet and Letournel. †Classification according to the standard of Thompson and Epstein. MVA: Motor vehicle accident, F/D: Fall down, PA: Pedestrian accident.
Table 2
Quality of Reduction and Clinical Grading System (CGS)
*Step off/gap.
Table 3
Correlation between Congruency of Fracture and Functional Score*
*t-test.

