 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 29(3); 2016 > Article
-
Review Article
- Fracture of the Talus
- Tae Jung Bang, M.D., Sun-Kyu Kim, M.D., Hyung-Jin Chung, M.D.
-
Journal of the Korean Fracture Society 2016;29(3):213-220.
DOI: https://doi.org/10.12671/jkfs.2016.29.3.213
Published online: July 21, 2016
Department of Orthopedic Surgery, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- Address reprint requests to: Hyung-Jin Chung, M.D. Department of Orthopedic Surgery, Inje University Sanggye Paik Hospital, 1342 Dongil-ro, Nowon-gu, Seoul 01757, Korea. Tel: 82-2-950-1399, Fax: 82-2-950-1398, orthoman@paik.ac.kr
Copyright © 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,654 Views
- 27 Download
Abstract
- Although talus fractures are uncommon, proper management is important because they are often associated with severe complications. Talar neck and body fractures occupy most of the talar fractures. It remains controversial whether talar neck fractures require emergent or elective treatment. Elective definitive fixation, however, may reduce risks of wound complications. Many surgeons recommend dual surgical approaches—anteromedial and anterolateral—to allow accurate visualization and anatomic reduction. Although there are various methods of fixation, the use of plates is necessary in comminuted talar fractures. Outcomes may vary and will be dependent on the degree of the initial fracture displacement. It is necessary to restore articular congruency and axial alignment for normalizing hindfoot function. Common complications include posttraumatic arthritis, avascular necrosis, malunion, and nonunion.
- 1. Abdelgaid SM, Ezzat FF. Percutaneous reduction and screw fixation of fracture neck talus. Foot Ankle Surg, 2012;18:219-228.Article
- 2. Peterson L, Goldie IF. The arterial supply of the talus. A study on the relationship to experimental talar fractures. Acta Orthop Scand, 1975;46:1026-1034.Article
- 3. Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J. Fractures of the talus: experience of two level 1 trauma centers. Foot Ankle Int, 2000;21:1023-1029.ArticlePDF
- 4. Lin S, Hak DJ. Management of talar neck fractures. Orthopedics, 2011;34:715-721.Article
- 5. Hawkins LG. Fractures of the neck of the talus. J Bone Joint Surg Am, 1970;52:991-1002.Article
- 6. Canale ST. Fractures of the neck of the talus. Orthopedics, 1990;13:1105-1115.Article
- 7. Ahmad J, Raikin SM. Current concepts review: talar fractures. Foot Ankle Int, 2006;27:475-482.ArticlePDF
- 8. Inokuchi S, Ogawa K, Usami N. Classification of fractures of the talus: clear differentiation between neck and body fractures. Foot Ankle Int, 1996;17:748-750.ArticlePDF
- 9. Vallier HA, Nork SE, Benirschke SK, Sangeorzan BJ. Surgical treatment of talar body fractures. J Bone Joint Surg Am, 2003;85:1716-1724.Article
- 10. Sneppen O, Christensen SB, Krogsoe O, Lorentzen J. Fracture of the body of the talus. Acta Orthop Scand, 1977;48:317-324.Article
- 11. Fortin PT, Balazsy JE. Talus fractures: evaluation and treatment. J Am Acad Orthop Surg, 2001;9:114-127.Article
- 12. Vallier HA, Reichard SG, Boyd AJ, Moore TA. A new look at the Hawkins classification for talar neck fractures: which features of injury and treatment are predictive of osteonecrosis? J Bone Joint Surg Am, 2014;96:192-197.Article
- 13. Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: results and outcomes. J Bone Joint Surg Am, 2004;86:1616-1624.Article
- 14. Lindvall E, Haidukewych G, DiPasquale T, Herscovici D Jr, Sanders R. Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am, 2004;86:2229-2234.Article
- 15. Fournier A, Barba N, Steiger V, et al. Total talar fracture: long-term results of internal fixation of talar fractures. A multicentric study of 114 cases. Orthop Traumatol Surg Res, 2012;98:S48-S55.Article
- 16. Xue Y, Zhang H, Pei F, et al. Treatment of displaced talar neck fractures using delayed procedures of plate fixation through dual approaches. Int Orthop, 2014;38:149-154.ArticlePDF
- 17. Rush SM, Jennings M, Hamilton GA. Talus fractures: surgical principles. Clin Podiatr Med Surg, 2009;26:91-103.Article
- 18. Mullen M, Pillai A, Fogg QA, Kumar CS. The anterior approach for the fixation of displaced talar neck fractures: a cadaveric study. Foot (Edinb), 2013;23:70-73.Article
- 19. Swanson TV, Bray TJ, Holmes GB Jr. Fractures of the talar neck. A mechanical study of fixation. J Bone Joint Surg Am, 1992;74:544-551.Article
- 20. Abdelkafy A, Imam MA, Sokkar S, Hirschmann M. Antegrade-retrograde opposing lag screws for internal fixation of simple displaced talar neck fractures. J Foot Ankle Surg, 2015;54:23-28.Article
- 21. Charlson MD, Parks BG, Weber TG, Guyton GP. Comparison of plate and screw fixation and screw fixation alone in a comminuted talar neck fracture model. Foot Ankle Int, 2006;27:340-343.ArticlePDF
- 22. Fleuriau Chateau PB, Brokaw DS, Jelen BA, Scheid DK, Weber TG. Plate fixation of talar neck fractures: preliminary review of a new technique in twenty-three patients. J Orthop Trauma, 2002;16:213-219.Article
- 23. Migues A, Solari G, Carrasco NM, González Della Valle A. Repair of talar neck nonunion with indirect corticocancellous graft technique: a case report and review of the literature. Foot Ankle Int, 1996;17:690-694.ArticlePDF
- 24. Sangeorzan BJ, Wagner UA, Harrington RM, Tencer AF. Contact characteristics of the subtalar joint: the effect of talar neck misalignment. J Orthop Res, 1992;10:544-551.Article
- 25. Canale ST, Kelly FB Jr. Fractures of the neck of the talus. Long-term evaluation of seventy-one cases. J Bone Joint Surg Am, 1978;60:143-156.Article
- 26. Bellamy JL, Keeling JJ, Wenke J, Hsu JR. Does a longer delay in fixation of talus fractures cause osteonecrosis? J Surg Orthop Adv, 2011;20:34-37.
- 27. Thordarson DB, Triffon MJ, Terk MR. Magnetic resonance imaging to detect avascular necrosis after open reduction and internal fixation of talar neck fractures. Foot Ankle Int, 1996;17:742-747.ArticlePDF
- 28. Sanders R. Fractures and fracture dislocations of the talus. In: Coughlin MJ, Mann RA, editors. Surgery of the foot and ankle. 7th ed. St. Louis: Mosby; 1999. p. 1465-1518.
REFERENCES


Fig. 3

(A, B) Preopertive radiographs show a comminuted talar neck and body fracture (A: anteroposterior view; B: lateral view). (C, D) Postoperative radiographs show a fixation using multiple screws and lateral plate with dual (anteromedial & anterolateral) surgical exposures and medial malleolar osteotomy (C: anteroposterior view; D: lateral view).
Fig. 4

(A, B) Preopertive radiographs show a comminuted talar neck fracture with subtalar joint subluxation (A: anteroposterior view; B: lateral view). (C, D) Postoperative radiographs show fixation using one anteroposterior screw, one posteroanterior screw, and one lateral plate with screws (C: anteroposterior view; D: lateral view).
Fig. 5

(A) Postoperative radiograph shows a subcondral sclerosis ten weeks after screw fixation of comminuted talar neck fracture. Hawkins sign is absent. (B, C) These T2-weighted magnetic resonance imaging scans were obtained ten weeks after a talar neck fracture and demonstrate focal osteonecrosis of talar body (B: coronal section; C: sagittal section).
Table 1
![jkfs-29-213-i001.jpg]()
Hawkins Classification of Talar Neck Fractures6)
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteFracture of the Talus
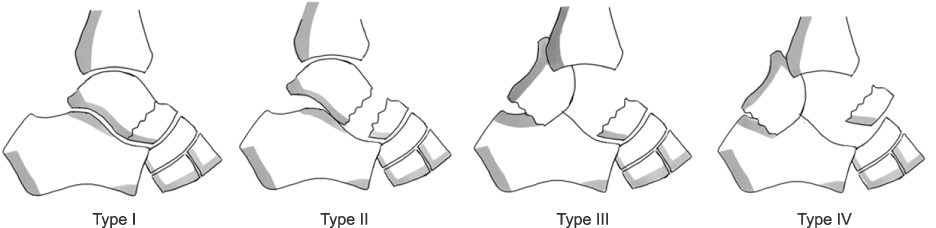
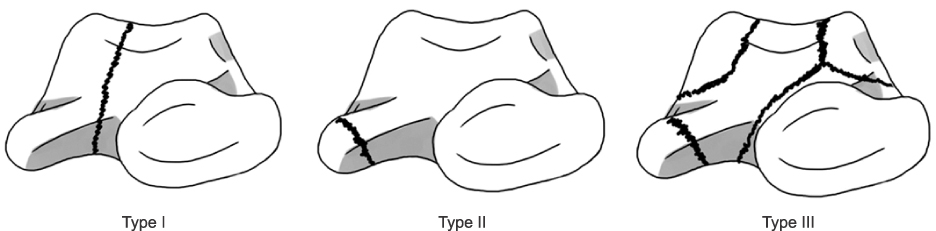


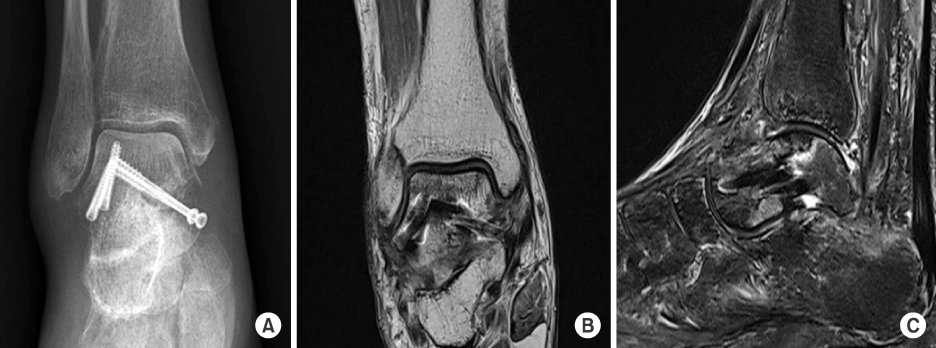
Fig. 1
Hawkins classification of talar neck fractures.6)
Fig. 2
Classification of talar body fractures.11)
Fig. 3
(A, B) Preopertive radiographs show a comminuted talar neck and body fracture (A: anteroposterior view; B: lateral view). (C, D) Postoperative radiographs show a fixation using multiple screws and lateral plate with dual (anteromedial & anterolateral) surgical exposures and medial malleolar osteotomy (C: anteroposterior view; D: lateral view).
Fig. 4
(A, B) Preopertive radiographs show a comminuted talar neck fracture with subtalar joint subluxation (A: anteroposterior view; B: lateral view). (C, D) Postoperative radiographs show fixation using one anteroposterior screw, one posteroanterior screw, and one lateral plate with screws (C: anteroposterior view; D: lateral view).
Fig. 5
(A) Postoperative radiograph shows a subcondral sclerosis ten weeks after screw fixation of comminuted talar neck fracture. Hawkins sign is absent. (B, C) These T2-weighted magnetic resonance imaging scans were obtained ten weeks after a talar neck fracture and demonstrate focal osteonecrosis of talar body (B: coronal section; C: sagittal section).
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fracture of the Talus
Hawkins Classification of Talar Neck Fractures6)
| Type I: nondisplaced fracture without subluxation; risk of avascular necrosis 0% to 13% |
| Type II: displaced vertical talar neck fracture with subtalar joint; risk of avascular necrosis 20% to 50% |
| Type III: displaced vertical talar neck fracture with subluxation of the subtalar and tibiotalar joint; risk of avascular necrosis 75% to 100% |
| Type IV: displaced vertical talar neck fracture with subluxation of the subtalar, ankle, and talonavicular joint; risk of avascular necrosis 100% |
Table 1
Hawkins Classification of Talar Neck Fractures6)

