 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 26(4); 2013 > Article
-
Original Article
- Results of Treatment for Medial Condyle Fracture of the Distal Humerus in Children
- Jeong Han Kang, M.D., Seung Hyeon Yang, M.S., Kuk Pil Lim, M.D., Hui Taek Kim, M.D.
-
Journal of the Korean Fracture Society 2013;26(4):261-267.
DOI: https://doi.org/10.12671/jkfs.2013.26.4.261
Published online: October 18, 2013
Department of Orthopaedic Surgery, Pusan National University Hospital, Busan, Korea.
*School of Medicine, Pusan National University, Yangsan, Korea.
- Address reprint requests to: Hui Taek Kim, M.D. Department of Orthopaedic Surgery, Pusan National University Hospital, 179 Gudeok-ro, Seo-gu, Busan 602-739, Korea. Tel: 82-51-240-7248, Fax: 82-51-247-8395, kimht@pusan.ac.kr
• Received: April 12, 2013 • Revised: June 7, 2013 • Accepted: July 24, 2013
Copyright © 2013 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 829 Views
- 5 Download
Abstract
-
Purpose
- We evaluated outcomes of treatment in medial condyle fracture of the distal humerus in children.
-
Materials and Methods
- Seven patients (4 females, 3 males) who were treated at the Pusan National University Hospital and followed-up until skeletal maturity after treatment were included. The average age at the time of fracture was 4.6 years (range, 2 to 10 years). Treatment was performed from 1 day to 6 months after the fracture: 4 patients underwent a surgical treatment for 17 days, 2 months, 2 months and 6 months after fracture, respectively. All fractures were Milch type 1. Five patients had Kilfoyle type 3, and two patients had type 2 fractures. Final outcomes were evaluated by the Mayo elbow performance score and carrying angle.
-
Results
- There were 3 excellent, 3 good and 1 fair result at the final follow-up. There was no elbow pain in any of the patients. One of the four patients who underwent a late surgical treatment received corrective osteotomy due to cubitus varus. All four patients had a limitation of elbow motion. The other three patients who had accurate diagnosis and treatment had a full range of motion.
-
Conclusion
- Diagnosis of medial condyle fracture of the distal humerus based on plain radiograph is difficult in children due to its cartilaginous structures. When a patient shows pain, tenderness and swelling on the medial side of the elbow, an additional examination with magnetic resonance imaging may be required even if no fracture line is found in the radiograph. Accurate diagnosis and early treatment is important for good results.
- 1. Bensahel H, Csukonyi Z, Badelon O, Badaoui S. Fractures of the medial condyle of the humerus in children. J Pediatr Orthop, 1986;6:430-433.Article
- 2. Chacha PB. Fracture of the medical condyle of the humerus with rotational displacement. Report of two cases. J Bone Joint Surg Am, 1970;52:1453-1458.
- 3. De Boeck H, Casteleyn PP, Opdecam P. Fracture of the medial humeral condyle. Report of a case in an infant. J Bone Joint Surg Am, 1987;69:1442-1444.Article
- 4. Fowles JV, Kassab MT. Displaced fractures of the medial humeral condyle in children. J Bone Joint Surg Am, 1980;62:1159-1163.Article
- 5. Ghawabi MH. Fracture of the medial condyle of the humerus. J Bone Joint Surg Am, 1975;57:677-680.Article
- 6. Gogola GR. Pediatric humeral condyle fractures. Hand Clin, 2006;22:77-85.Article
- 7. Hanspal RS. Injury to the medial humeral condyle in a child reviewed after 18 years. Report of a case. J Bone Joint Surg Br, 1985;67:638-639.ArticlePDF
- 8. Haraldsson S. On osteochondrosis deformas juvenilis capituli humeri including investigation of intra-osseous vasculature in distal humerus. Acta Orthop Scand Suppl, 1959;38:1-232.
- 9. Ingersoll RE. Fractures of the humeral condyles in children. Clin Orthop Relat Res, 1965;41:32-42.Article
- 10. Ippolito E, Tudisco C, Farsetti P, Caterini R. Fracture of the humeral condyles in children: 49 cases evaluated after 18-45 years. Acta Orthop Scand, 1996;67:173-178.Article
- 11. Kilfoyle RM. Fractures of the medial condyle and epicondyle of the elbow in children. Clin Orthop Relat Res, 1965;41:43-50.Article
- 12. Leet AI, Young C, Hoffer MM. Medial condyle fractures of the humerus in children. J Pediatr Orthop, 2002;22:2-7.Article
- 13. Lins RE, Simovitch RW, Waters PM. Pediatric elbow trauma. Orthop Clin North Am, 1999;30:119-132.Article
- 14. Milch H. Fractures and fracture dislocations of the humeral condyles. J Trauma, 1964;4:592-607.Article
- 15. Oppenheim WL, Clader TJ, Smith C, Bayer M. Supracondylar humeral osteotomy for traumatic childhood cubitus varus deformity. Clin Orthop Relat Res, 1984;(188):34-39.Article
- 16. Papavasiliou V, Nenopoulos S, Venturis T. Fractures of the medial condyle of the humerus in childhood. J Pediatr Orthop, 1987;7:421-423.Article
- 17. Ryu K, Nagaoka M, Ryu J. Osteosynthesis for nonunion of the medial humeral condyle in an adolescent: a case report. J Shoulder Elbow Surg, 2007;16:e8-e12.Article
REFERENCES
Fig. 1
(A) A 3-year-old girl had trauma in the left elbow which was misdiagnosed as a sprain, and was treated with a splint (Case 2).
(B) However, a radiograph taken 17 days after the trauma revealed a medial condyle fracture of the distal humerus (white arrow: scattered calcification in the medial condyle).
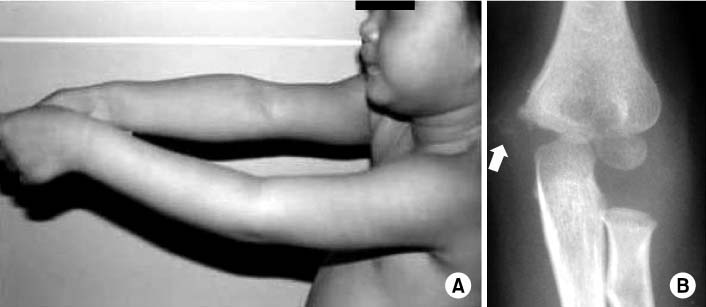
Fig. 2Magnetic resonance imaging showed a displaced medial condyle fracture (white arrow) with rotation (Kilfoyle type 3).


Fig. 4Reduction of the fragment and internal fixation with K-wire was performed with a careful dissection of soft tissues from the fragment to preserve blood supply from flexor muscle group. Anteroposterior radiograph taken 3 months after surgery showed an irregular margin of medial side of the distal humerus with an ossification center of medial epicondyle.

Fig. 5Anteroposterior radiographs of both elbows taken 4 years after surgery (when the patient was 7 years old) showed deformity of the distal humerus in the left elbow.

Fig. 6Anteroposterior radiographs of both elbows taken 13 years after surgery (when the patient was 16 years old) showed undergrowth of trochlea on the affected side. At the latest follow-up, her elbow performance score in the left side was 94 (excellent) with a slight limitation of motion (0-130°). Five degrees difference of carrying angle from the normal side was noticed.

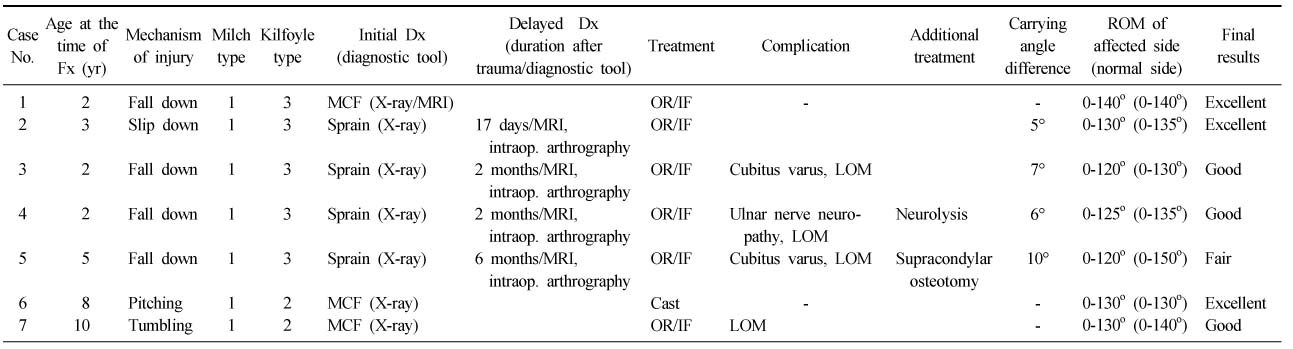
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteResults of Treatment for Medial Condyle Fracture of the Distal Humerus in Children
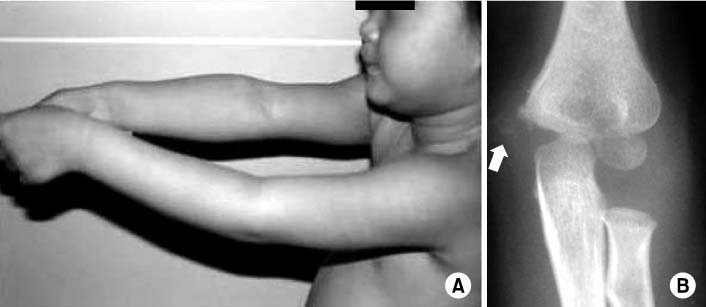





Fig. 1
(A) A 3-year-old girl had trauma in the left elbow which was misdiagnosed as a sprain, and was treated with a splint (Case 2).
(B) However, a radiograph taken 17 days after the trauma revealed a medial condyle fracture of the distal humerus (white arrow: scattered calcification in the medial condyle).
Fig. 2
Magnetic resonance imaging showed a displaced medial condyle fracture (white arrow) with rotation (Kilfoyle type 3).
Fig. 3
Arthrogram confirmed a medial condyle fracture (white arrow) with rotation (Kilfoyle type 3).
Fig. 4
Reduction of the fragment and internal fixation with K-wire was performed with a careful dissection of soft tissues from the fragment to preserve blood supply from flexor muscle group. Anteroposterior radiograph taken 3 months after surgery showed an irregular margin of medial side of the distal humerus with an ossification center of medial epicondyle.
Fig. 5
Anteroposterior radiographs of both elbows taken 4 years after surgery (when the patient was 7 years old) showed deformity of the distal humerus in the left elbow.
Fig. 6
Anteroposterior radiographs of both elbows taken 13 years after surgery (when the patient was 16 years old) showed undergrowth of trochlea on the affected side. At the latest follow-up, her elbow performance score in the left side was 94 (excellent) with a slight limitation of motion (0-130°). Five degrees difference of carrying angle from the normal side was noticed.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Results of Treatment for Medial Condyle Fracture of the Distal Humerus in Children
Patient Data
Fx: Fracture, Dx: Diagnosis, MCF: Medial condyle fracture, MRI: Magnetic resonance imaging, Intraop.: Intraoperative, OR/IF: Open reduction and internal fixation, LOM: Limitation of motion, ROM: Range of motion.
Table 1
Patient Data
Fx: Fracture, Dx: Diagnosis, MCF: Medial condyle fracture, MRI: Magnetic resonance imaging, Intraop.: Intraoperative, OR/IF: Open reduction and internal fixation, LOM: Limitation of motion, ROM: Range of motion.

