 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 26(4); 2013 > Article
-
Original Article
- Augmentative Locking Plate Fixation for the Treatment of Femoral Nonunion after Intramedullary Nailing
- Ki-Chul Park, M.D., Chul-Woong Kim, M.D., Kyu-Tae Hwang, M.D., Ye-Soo Park, M.D.
-
Journal of the Korean Fracture Society 2013;26(4):268-274.
DOI: https://doi.org/10.12671/jkfs.2013.26.4.268
Published online: October 18, 2013
Department of Orthopedic Surgery, Hanyang University College of Medicine, Seoul, Korea.
- Address reprint requests to: Ki-Chul Park, M.D. Department of Orthopedic Surgery, Hanyang University Guri Hospital, 153 Gyeongchun-ro, Guri 471-701, Korea. Tel: 82-31-560-2318, Fax: 82-31-557-8781, kcpark@hanyang.ac.kr
• Received: April 4, 2013 • Revised: June 1, 2013 • Accepted: July 31, 2013
Copyright © 2013 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 884 Views
- 3 Download
Abstract
-
Purpose
- To evaluate the efficacy of the augmentative locking compression plate fixation in the treatment of femoral shaft nonunion occurring after intramedullary nailing.
-
Materials and Methods
- Between July 2004 and September 2012, a total of 17 patients (twelve men, five women, average age 52.5 years) who had femoral nonunions after primary intramedullary nailing for femoral shaft fractures were reviewed. The mean period of nonunion after primary nailing was 18.5 months. Leaving the nail in situ, an augmentative locking plate was applied to the nonunion site with simultaneous autogenous bone grafting, except for five hypertrophic nonunions. We followed up all patients with plain radiograph and evaluated clinical status to determine bone union.
-
Results
- All patients demonstrated evidence of fracture union with an average follow-up time of 5.0 (range 2 to 9) months. The time of operation was an average of 115 (range 45 to 160) minutes, and mean blood loss was 345.9 (range 150 to 700) ml. Two patients noted discomfort at the distal portion of plate, and one noted discomfort of donor site, but functional limitation was not observed in all patients.
-
Conclusion
- Augmentative locking plate fixation for diaphyseal femoral nonunion after intramedullary nailing is a reasonable treatment option with increased stability.
- 1. Brinker MR, O'Connor DP. Exchange nailing of ununited fractures. J Bone Joint Surg Am, 2007;89:177-188.Article
- 2. Brumback RJ, Uwagie-Ero S, Lakatos RP, Poka A, Bathon GH, Burgess AR. Intramedullary nailing of femoral shaft fractures. Part II: fracture-healing with static interlocking fixation. J Bone Joint Surg Am, 1988;70:1453-1462.Article
- 3. Choi YS, Kim KS. Plate augmentation leaving the nail in situ and bone grafting for non-union of femoral shaft fractures. Int Orthop, 2005;29:287-290.ArticlePDF
- 4. Furlong AJ, Giannoudis PV, DeBoer P, Matthews SJ, MacDonald DA, Smith RM. Exchange nailing for femoral shaft aseptic non-union. Injury, 1999;30:245-249.Article
- 5. Hak DJ, Lee SS, Goulet JA. Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma, 2000;14:178-182.Article
- 6. Hakeos WM, Richards JE, Obremskey WT. Plate fixation of femoral nonunions over an intramedullary nail with autogenous bone grafting. J Orthop Trauma, 2011;25:84-89.Article
- 7. Jung HG, Kim DJ, Kim BH, Chung YY. Treatment of the femoral shaft nonunion occurred after intramedullary nailing. J Korean Orthop Assoc, 2007;42:653-658.Article
- 8. Kuntscher G. Intrmedullary surgical technique and its place in orthopaedic surgery. my present concept. J Bone Joint Surg Am, 1965;47:809-818.
- 9. Lin CJ, Chiang CC, Wu PK, et al. Effectiveness of plate augmentation for femoral shaft nonunion after nailing. J Chin Med Assoc, 2012;75:396-401.Article
- 10. Nadkarni B, Srivastav S, Mittal V, Agarwal S. Use of locking compression plates for long bone nonunions without removing existing intramedullary nail: review of literature and our experience. J Trauma, 2008;65:482-486.Article
- 11. Niedźwiedzki T, Brudnicki J, Niedźwiedzki Ł. Treatment of femoral shaft union disturbances with intramedullary nailing. Treatment failure. Ortop Traumatol Rehabil, 2007;9:377-383.
- 12. Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br, 2002;84:1093-1110.
- 13. Pihlajamäki HK, Salminen ST, Böstman OM. The treatment of nonunions following intramedullary nailing of femoral shaft fractures. J Orthop Trauma, 2002;16:394-402.Article
- 14. Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R. Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma, 2001;15:161-169.Article
- 15. Ring D, Jupiter J. Humerus nonunion after intramedullary rod fixation: locking compression plating without removing the nail. Tech Orthop, 2003;18:356-359.
- 16. Shin YW, Sung YB, Choi JY, Kim M. Analysis of risk factors for nonunion after intramedullary nailing of femoral shaft fracture in adult. J Korean Fract Soc, 2011;24:313-320.Article
- 17. Smith WR, Morgan SJ. Failure of internal fixation of the femoral shaft. Tech Orthop, 2002;17:448-457.Article
- 18. Taitsman LA, Lynch JR, Agel J, Barei DP, Nork SE. Risk factors for femoral nonunion after femoral shaft fracture. J Trauma, 2009;67:1389-1392.Article
- 19. Ueng SW, Chao EK, Lee SS, Shih CH. Augmentative plate fixation for the management of femoral nonunion after intramedullary nailing. J Trauma, 1997;43:640-644.Article
- 20. Webb LX, Winquist RA, Hansen ST. Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft. A report of 105 consecutive cases. Clin Orthop Relat Res, 1986;(212):133-141.
- 21. Weresh MJ, Hakanson R, Stover MD, Sims SH, Kellam JF, Bosse MJ. Failure of exchange reamed intramedullary nails for ununited femoral shaft fractures. J Orthop Trauma, 2000;14:335-338.Article
- 22. Winquist RA, Hansen ST Jr, Clawson DK. Closed intramedullary nailing of femoral fractures. A report of five hundred and twenty cases. J Bone Joint Surg Am, 1984;66:529-539.Article
- 23. Ye J, Zheng Q. Augmentative locking compression plate fixation for the management of long bone nonunion after intramedullary nailing. Arch Orthop Trauma Surg, 2012;132:937-940.ArticlePDF
REFERENCES
Fig. 1
(A) Forty-three-year-old man with segmental femoral shaft fracture (AO-OTA classification 32-C2).
(B) Eight months after application of intramedullary nail and circlage wire, showing atrophic nonunion of middle third of femur.
(C) Immediate postoperative X-ray after application of locking compression plate along with bone grafting.
(D) Five months after surgery, a solid union was achieved.
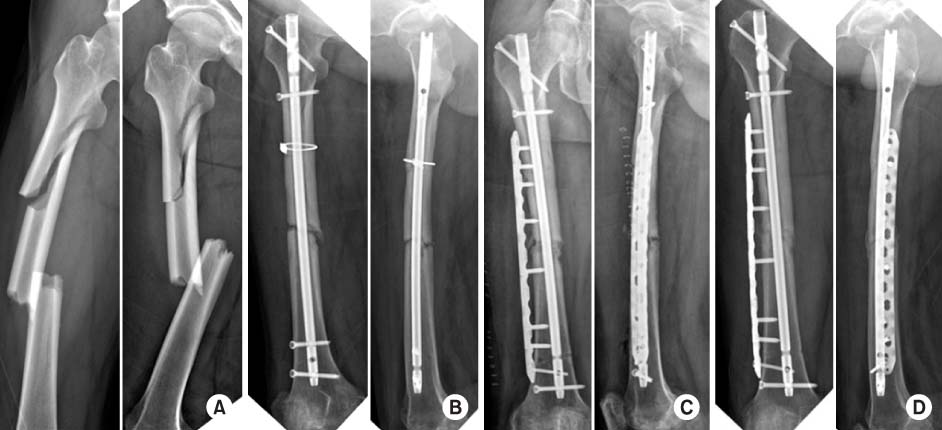
Fig. 2
(A) Forty-five-year-old man with segmental femoral shaft fracture (AO-OTA classification 32-C2).
(B) One year after application of intramedullary nail and circlage wire, showing hypertrophic nonunion of distal third of femur.
(C) Immediate postoperative X-ray after application of locking compression plate without bone grafting.
(D) Solid union was achieved at nine months after surgery, and then implant was removed.

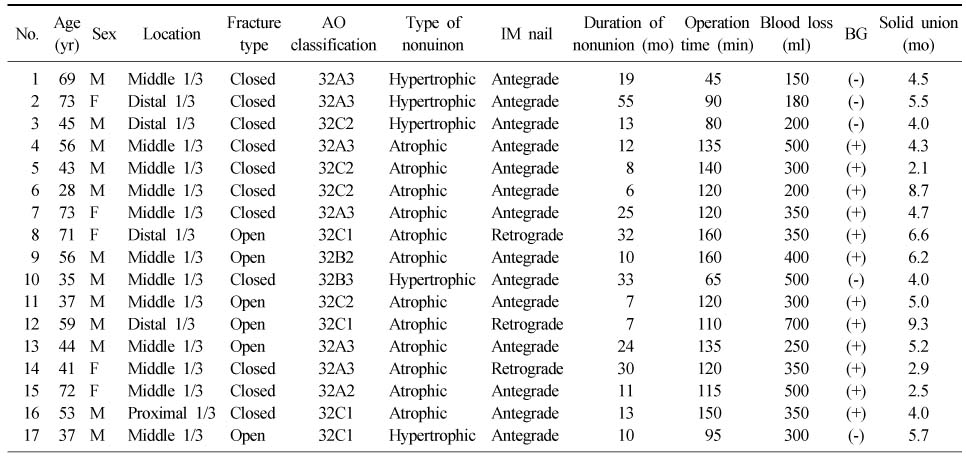
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteAugmentative Locking Plate Fixation for the Treatment of Femoral Nonunion after Intramedullary Nailing
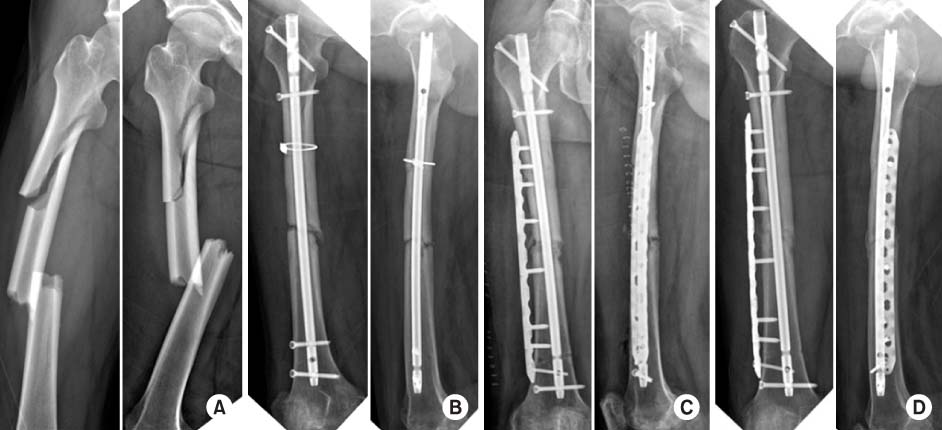

Fig. 1
(A) Forty-three-year-old man with segmental femoral shaft fracture (AO-OTA classification 32-C2).
(B) Eight months after application of intramedullary nail and circlage wire, showing atrophic nonunion of middle third of femur.
(C) Immediate postoperative X-ray after application of locking compression plate along with bone grafting.
(D) Five months after surgery, a solid union was achieved.
Fig. 2
(A) Forty-five-year-old man with segmental femoral shaft fracture (AO-OTA classification 32-C2).
(B) One year after application of intramedullary nail and circlage wire, showing hypertrophic nonunion of distal third of femur.
(C) Immediate postoperative X-ray after application of locking compression plate without bone grafting.
(D) Solid union was achieved at nine months after surgery, and then implant was removed.
Fig. 1
Fig. 2
Augmentative Locking Plate Fixation for the Treatment of Femoral Nonunion after Intramedullary Nailing
Clinical Details of the Nonunion of Femoral Shaft Fracture after Intramedullary Nailing
IM: Intramedullary, BG: Bone graft, M: Male, F: Female.
Table 1
Clinical Details of the Nonunion of Femoral Shaft Fracture after Intramedullary Nailing
IM: Intramedullary, BG: Bone graft, M: Male, F: Female.

