 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 28(4); 2015 > Article
-
Original Article
- Clinical Outcomes of Fasciotomy for Acute Compartment Syndrome
- Ji Yong Park, M.D., Young Chang Kim, M.D., Ph.D., Ji Wan Kim, M.D., Ph.D.
-
Journal of the Korean Fracture Society 2015;28(4):223-229.
DOI: https://doi.org/10.12671/jkfs.2015.28.4.223
Published online: October 19, 2015
Department of Orthopedic Surgery, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- Address reprint requests to: Ji Wan Kim, M.D., Ph.D. Department of Orthopedic Surgery, Inje University Haeundae Paik Hospital, 875 Haeun-daero, Haeundae-gu, Busan 48108, Korea. Tel: 82-51-797-0668, Fax: 82-51-797-0669, H00106@paik.ac.kr
• Received: July 1, 2015 • Revised: July 20, 2015 • Accepted: July 20, 2015
Copyright © 2015 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,121 Views
- 10 Download
Abstract
-
Purpose
- The purpose of this study is to evaluate clinical outcomes and complications after fasciotomy in acute compartment syndrome.
-
Materials and Methods
- Seventeen cases diagnosed as compartment syndrome and underwent fasciotomy from January 2011 to February 2015 were evaluated retrospectively. We investigated the causes and regions of acute compartment syndrome, the methods of wound management, the necessity of skin graft, and the complications including amputation and infection.
-
Results
- According to the causes of acute compartment syndrome, there were 7 fractures, 1 traumatic hematoma, 6 reperfusion injury, and 3 rhabdomyolysis. The regions of acute compartment syndrome were 3 cases of thigh, 10 cases of leg, and 3 cases of foot. One case had acute compartment syndrome involving thigh, leg, and foot. Of 17 cases, 3 cases died due to reperfusion injury and one case with severe necrosis of soft tissues underwent amputation. Among the 13 cases excluding 4 cases with death or amputation, 3 cases underwent split thickness skin graft. Shoelace technique and/or vacuum-assisted closure (VAC) was used for 9 cases, and wound closure without skin graft was achieved in all except one case, while 2 cases required skin graft among 4 cases without shoelace technique or VAC. There were 2 cases of infection.
-
Conclusion
- Acute compartment syndrome caused by reperfusion injury had poor outcomes. Shoelace technique and/or VAC were useful for management of wound after fasciotomy.
- 1. Oh CW, Lee HJ. Acute compartment syndrome after trauma. J Korean Fract Soc, 2010;23:399-403.Article
- 2. Elliott KGB, Johnstone AJ. Review article: diagnosing acute compartment syndrome. J Bone Joint Surg Br, 2003;85:625-632.PubMed
- 3. Fulkerson E, Razi A, Tejwani N. Review: acute compartment syndrome of the foot. Foot Ankle Int, 2003;24:180-187.ArticlePubMedPDF
- 4. Frink M, Hildebrand F, Krettek C, Brand J, Hankemeier S. Compartment syndrome of the lower leg and foot. Clin Orthop Relat Res, 2010;468:940-950.ArticlePubMed
- 5. Chae SU. Acute compartment syndrome of the lower leg and foot. J Korean Foot Ankle Soc, 2013;17:165-173.
- 6. Daniels M, Reichman J, Brezis M. Mannitol treatment for acute compartment syndrome. Nephron, 1998;79:492-493.ArticlePubMedPDF
- 7. Lee KB, Lee SH. Diagnosis and management of acute compartment syndrome. J Korean Fract Soc, 2015;28:93-101.Article
- 8. Vo A. Closing the fasciotomy wound following compartment syndrome. UOJM, 2013;3:38-41.
- 9. McQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome. Who is at risk. J Bone Joint Surg Br, 2000;82:200-203.PubMed
- 10. Stark E, Stucken C, Trainer G, Tornetta P 3rd. Compartment syndrome in Schatzker type VI plateau fractures and medial condylar fracture-dislocations treated with temporary external fixation. J Orthop Trauma, 2009;23:502-506.ArticlePubMed
- 11. Volanska M, Zavacky P, Bober J. Ischaemic-reperfusion damage of tissue and critical limb ischaemia. Bratisl Lek Listy, 2006;107:264-268.PubMed
- 12. Ganie FA, Lone H, Wani ML, Ahmad Dar F, Wani NU, Wani SN. Role of liberal primary fasciotomy in traumatic vascular injury. Trauma Mon, 2012;17:287-290.Article
- 13. Kronja G, Misović S, Tomić A. Indications and results of fasciotomy in vascular injuries of the lower extremities. Vojnosanit Pregl, 2000;57:271-276.PubMed
- 14. Shon OJ, Kim GB, Park CH. Acute compartment syndrome of the thigh caused by contusion: 4 cases report. J Korean Fract Soc, 2012;25:215-218.Article
- 15. Rööser B, Bengtson S, Hägglund G. Acute compartment syndrome from anterior thigh muscle contusion: a report of eight cases. J Orthop Trauma, 1991;5:57-59.PubMed
- 16. Weaver MJ, Owen TM, Morgan JH, Harris MB. Delayed primary closure of fasciotomy incisions in the lower leg: do we need to change our strategy. J Orthop Trauma, 2015;29:308-311.PubMed
- 17. Kakagia D, Karadimas EJ, Drosos G, Ververidis A, Trypsiannis G, Verettas D. Wound closure of leg fasciotomy: comparison of vacuum-assisted closure versus shoelace technique. A randomised study. Injury, 2014;45:890-893.ArticlePubMed
- 18. Saziye K, Mustafa C, Ilker U, Afksendyios K. Comparison of vacuum-assisted closure device and conservative treatment for fasciotomy wound healing in ischaemia-reperfusion syndrome: preliminary results. Int Wound J, 2011;8:229-236.ArticlePubMedPMC
- 19. Zorrilla P, Marín A, Gómez LA, Salido JA. Shoelace technique for gradual closure of fasciotomy wounds. J Trauma, 2005;59:1515-1517.ArticlePubMed
REFERENCES
Fig. 1
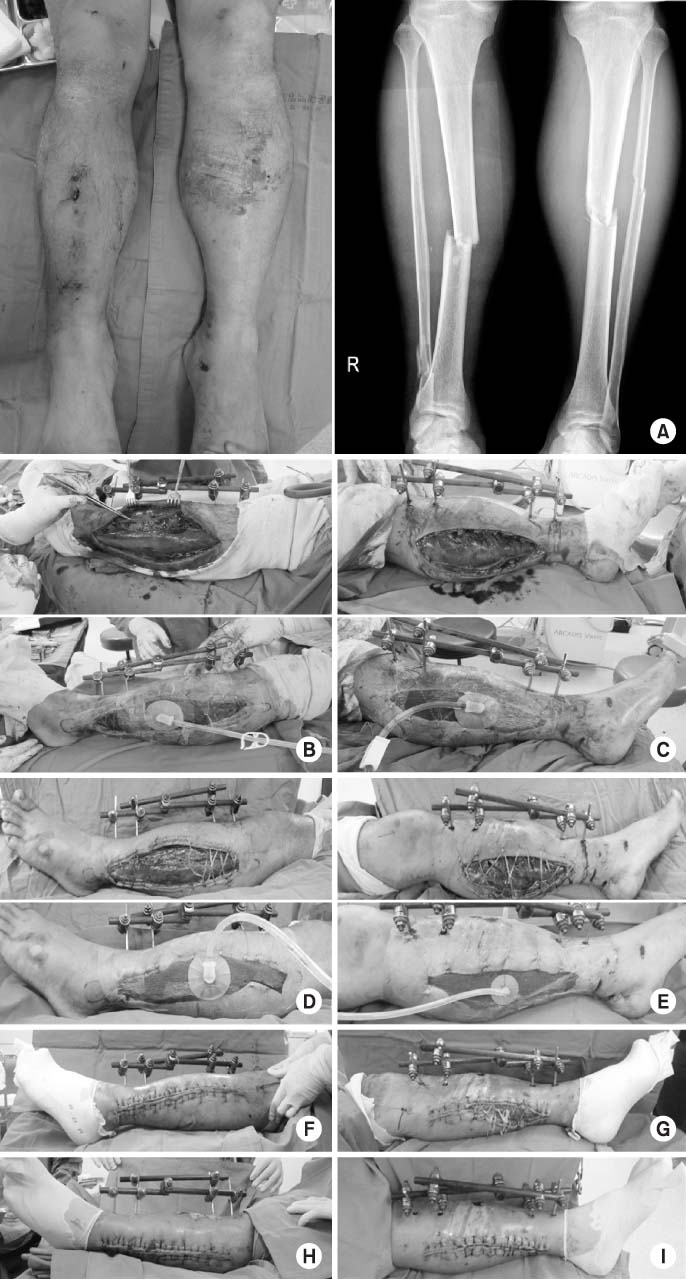
(A) A 41-year-old male had both a tibia shaft fracture and severe swelling on the left leg with pain. Emergency fasciotomy was performed with a double incision on lateral (B) and medial (C). A photograph at 4 days after injury shows that shoelace technique and negative pressure wound dressing was applied on lateral (D) and medial (E). Progressive wound closure was performed using shoelace technique and negative pressure wound dressing on the lateral side (F) and medial side (G). (H, I) At 16 days after injury, complete wound closure was possible without skin graft.
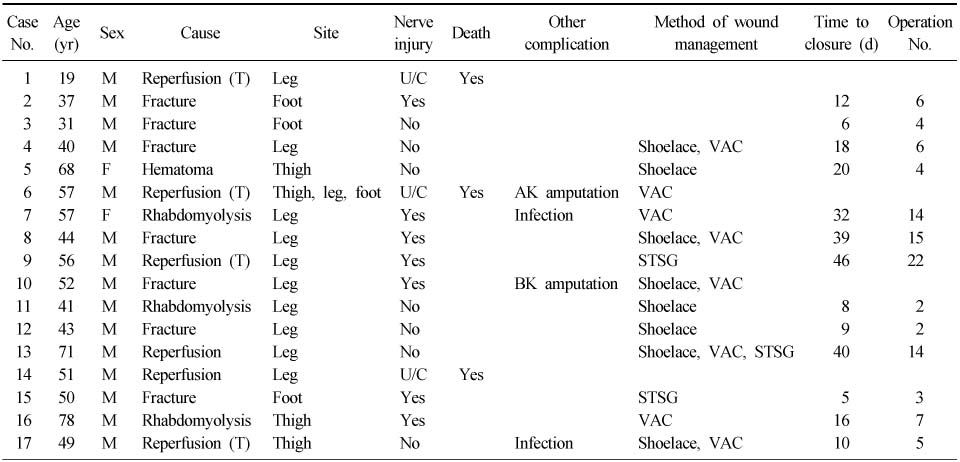
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteClinical Outcomes of Fasciotomy for Acute Compartment Syndrome
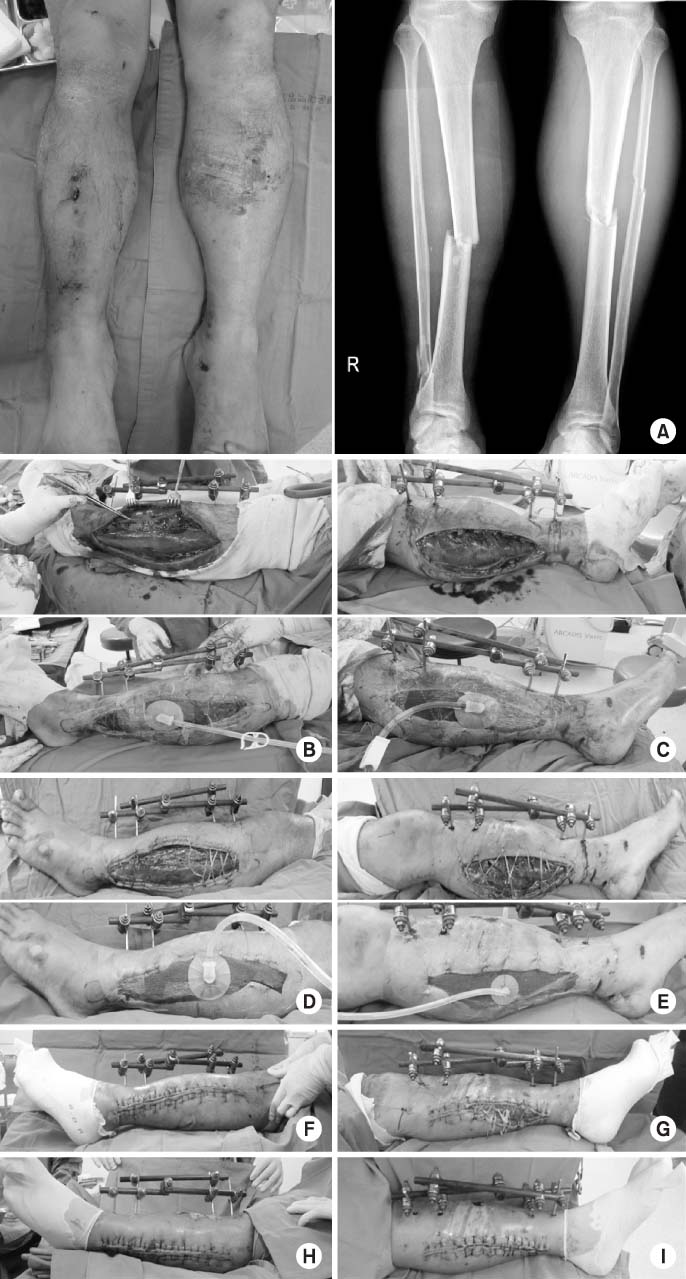
Fig. 1
(A) A 41-year-old male had both a tibia shaft fracture and severe swelling on the left leg with pain. Emergency fasciotomy was performed with a double incision on lateral (B) and medial (C). A photograph at 4 days after injury shows that shoelace technique and negative pressure wound dressing was applied on lateral (D) and medial (E). Progressive wound closure was performed using shoelace technique and negative pressure wound dressing on the lateral side (F) and medial side (G). (H, I) At 16 days after injury, complete wound closure was possible without skin graft.
Fig. 1
Clinical Outcomes of Fasciotomy for Acute Compartment Syndrome
Summary of Clinical Course in 17 Patients
M: Male, F: Female, T: Traumatic, U/C: Uncheckable, AK: Above knee, BK: Below knee, VAC: Vacuum-assisted closure, STSG: Split thickness skin graft.
Table 1
Summary of Clinical Course in 17 Patients
M: Male, F: Female, T: Traumatic, U/C: Uncheckable, AK: Above knee, BK: Below knee, VAC: Vacuum-assisted closure, STSG: Split thickness skin graft.

