 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 29(3); 2016 > Article
-
Original Article
- Surgical Treatment for Stable 2-Part Intertrochanteric Femur Fracture Using Dynamic Hip Screw with 2-Hole Side Plate in Elderly Patients
- Kyung-Hoon Lee, M.D., Suk Ku Han, M.D., Seung-Jae Chung, M.D., Jongho Noh, M.D., Kee-Haeng Lee, M.D.
-
Journal of the Korean Fracture Society 2016;29(3):192-199.
DOI: https://doi.org/10.12671/jkfs.2016.29.3.192
Published online: July 21, 2016
Department of Orthopedic Surgery, School of Medicine, The Catholic University of Korea, Seoul, Korea.
- Address reprint requests to: Kee-Haeng Lee, M.D. Department of Orthopedic Surgery, The Catholic University of Korea, Bucheon St. Mary's Hospital, 327 Sosa-ro, Wonmi-gu, Bucheon 14647, Korea. Tel: 82-32-340-2260, Fax: 82-32-340-2671, keeleehip@gmail.com
• Received: March 23, 2016 • Revised: April 15, 2016 • Accepted: June 8, 2016
Copyright © 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 781 Views
- 0 Download
Abstract
-
Purpose
- The purpose of this study is to evaluate the postoperative outcomes of elderly patients with stable 2-part intertrochanteric femur fractures surgically treated using dynamic hip screw with 2-hole side plate.
-
Materials and Methods
- From February 2008 to January 2014, 50 patients older than the age of 65 years, who had been followed-up for more than 6 months after the operation at The Catholic University of Korea, Bucheon St. Mary's Hospital were enrolled. A clinical evaluation of the skin incision length, operating time, and ambulatory status, using Clawson's Ambulation Capacity Classification, was performed, and a radiologic evaluation of Fogagnolo reduction quality, tip-apex distance (TAD), Cleveland index, sliding extent of lag screws, time duration till bony union, and complications was also done.
-
Results
- The mean skin incision length was 9.8 cm (range, 8-13 cm), the mean operating time was 41.4 minutes (range, 30-60 minutes), and 32 patients recovered their ambulatory function. Forty-eight patients gained bony union, and the time lapsed till union was average 10.6 weeks (range, 8-16 weeks). The evaluation of postoperative radiologic images showed the following reduction statuses by the Fogagnolo classification: 46 cases of "Good", 3 cases of "Acceptable," and 1 case of "Poor." Moreover, the mean TAD was 18.9 mm (range, 9.0-24.9 mm). While 45 cases fit into the zone 5 of the Cleveland index, other 3 were within zone 8 and the other 2 were within zone 6. The mean sliding length of the lag screws were 4.9 mm (range, 0.1-19.4 mm). There were a case of nonunion and a case of periprosthetic infection with nonunion as complications.
-
Conclusion
- Using dynamic hip screws with 2-hole side plate for stable 2-part intertrochanteric femur fractures in elderly patients showed satisfactory results with respect to the recovery of ambulatory functions and bony union.
- 1. Haentjens P, Casteleyn PP, Opdecam P. Primary bipolar arthroplasty or total hip arthroplasty for the treatment of unstable intertrochanteric and subtrochanteric fractures in elderly patients. Acta Orthop Belg, 1994;60:Suppl 1. 124-128.
- 2. Kaplan K, Miyamoto R, Levine BR, Egol KA, Zuckerman JD. Surgical management of hip fractures: an evidence-based review of the literature. II: intertrochanteric fractures. J Am Acad Orthop Surg, 2008;16:665-673.Article
- 3. Lorich DG, Geller DS, Nielson JH. Osteoporotic pertrochanteric hip fractures: management and current controversies. Instr Course Lect, 2004;53:441-454.
- 4. Rodop O, Kiral A, Kaplan H, Akmaz I. Primary bipolar hemiprosthesis for unstable intertrochanteric fractures. Int Orthop, 2002;26:233-237.ArticlePDF
- 5. Clawson DK. Trochanteric fractures treated by the sliding screw plate fixation method. J Trauma, 1964;4:737-752.Article
- 6. Rao JP, Banzon MT, Weiss AB, Rayhack J. Treatment of unstable intertrochanteric fractures with anatomic reduction and compression hip screw fixation. Clin Orthop Relat Res, 1983;175:65-71.Article
- 7. Bolhofner BR, Russo PR, Carmen B. Results of intertrochanteric femur fractures treated with a 135-degree sliding screw with a two-hole side plate. J Orthop Trauma, 1999;13:5-8.Article
- 8. Verhofstad MH, van der Werken C. DHS osteosynthesis for stable pertrochanteric femur fractures with a two-hole side plate. Injury, 2004;35:999-1002.Article
- 9. Yian EH, Banerji I, Matthews LS. Optimal side plate fixation for unstable intertrochanteric hip fractures. J Orthop Trauma, 1997;11:254-259.Article
- 10. McLoughlin SW, Wheeler DL, Rider J, Bolhofner B. Biomechanical evaluation of the dynamic hip screw with two- and four-hole side plates. J Orthop Trauma, 2000;14:318-323.Article
- 11. Clawson DK. Intertrochanteric fracture of the hip. Am J Surg, 1957;93:580-587.Article
- 12. Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am, 1995;77:1058-1064.Article
- 13. Cleveland M, Bosworth DM, Thompson FR, Wilson HJ Jr, Ishizuka T. A ten-year analysis of intertrochanteric fractures of the femur. J Bone Joint Surg Am, 1959;41:1399-1408.Article
- 14. Fogagnolo F, Kfuri M Jr, Paccola CA. Intramedullary fixation of pertrochanteric hip fractures with the short AO-ASIF proximal femoral nail. Arch Orthop Trauma Surg, 2004;124:31-37.ArticlePDF
- 15. Doppelt SH. The sliding compression screw: today's best answer for stabilization of intertrochanteric hip fractures. Orthop Clin North Am, 1980;11:507-523.Article
- 16. Mitkovic M, Milenkovic S, Micic I, Mladenovic D, Mitkovic M. Results of the femur fractures treated with the new selfdynamisable internal fixator (SIF). Eur J Trauma Emerg Surg, 2012;38:191-200.Article
- 17. Davis TR, Sher JL, Horsman A, Simpson M, Porter BB, Checketts RG. Intertrochanteric femoral fractures. Mechanical failure after internal fixation. J Bone Joint Surg Br, 1990;72:26-31.ArticlePDF
- 18. Den Hartog BD, Bartal E, Cooke F. Treatment of the unstable intertrochanteric fracture. Effect of the placement of the screw, its angle of insertion, and osteotomy. J Bone Joint Surg Am, 1991;73:726-773.Article
- 19. Mainds CC, Newman RJ. Implant failures in patients with proximal fractures of the femur treated with a sliding screw device. Injury, 1989;20:98-100.Article
- 20. Parker MJ. Cutting-out of the dynamic hip screw related to its position. J Bone Joint Surg Br, 1992;74:625. ArticlePDF
- 21. Steinberg GG, Desai SS, Kornwitz NA, Sullivan TJ. The intertrochanteric hip fracture. A retrospective analysis. Orthopedics, 1988;11:265-273.Article
- 22. Laohapoonrungsee A, Arpornchayanon O, Phornputkul C. Two-hole side-plate DHS in the treatment of intertrochanteric fracture: results and complications. Injury, 2005;36:1355-1360.Article
- 23. Koval KJ, Skovron ML, Aharonoff GB, Meadows SE, Zuckerman JD. Ambulatory ability after hip fracture. A prospective study in geriatric patients. Clin Orthop Relat Res, 1995;(310):150-159.
- 24. Baird RP, O'Brien P, Cruickshank D. Comparison of stable and unstable pertrochanteric femur fractures managed with 2- and 4-hole side plates. Can J Surg, 2014;57:327-330.Article
- 25. Zhao C, Liu DY, Guo JJ, et al. Comparison of proximal femoral nail and dynamic hip screw for treating intertrochanteric fractures. Zhongguo Gu Shang, 2009;22:535-537.
- 26. Zhang K, Zhang S, Yang J, et al. Proximal femoral nail vs. dynamic hip screw in treatment of intertrochanteric fractures: a meta-analysis. Med Sci Monit, 2014;20:1628-1633.Article
REFERENCES
Fig. 1

(A) Preoperative X-ray. (B) X-ray taken immediately after the operation. An excessive lag screw telescope is observed due to a reduction loss. (C) X-ray taken 6 months after the operation. Varus collapse occurred due to non-union and breakage of distal cortical screw. (D) Conversion to hip replacement arthroplasty.
Fig. 2

(A) Preoperative X-ray. (B) X-ray taken immediately after the operation. (C) X-ray taken 7 months after the operation. Breakage of the lag screw, non-union of the fracture site, and radio-lucent shadow around the hardware are observed. The patient complained of systemic femur with right hip pain. (D) Girdlestone operation with antibiotic-loaded cement insertion was done. However, the patient expired due to sepsis.
Table 1
![jkfs-29-192-i001.jpg]()
Demographic Characteristics of Enrolled Patients
Table 2
![jkfs-29-192-i002.jpg]()
Clawson's Ambulation Capacity Classification11)
| Class I | Wheelchair ambulation |
| Class II | Crutch, two cane |
| Class III | One cane or simple brace |
| Class IV | Self ambulation |
Table 3
![jkfs-29-192-i003.jpg]()
Clinical Results of Enrolled Patients
Table 4
![jkfs-29-192-i004.jpg]()
Radiologic Results of Enrolled Patients
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteSurgical Treatment for Stable 2-Part Intertrochanteric Femur Fracture Using Dynamic Hip Screw with 2-Hole Side Plate in Elderly Patients

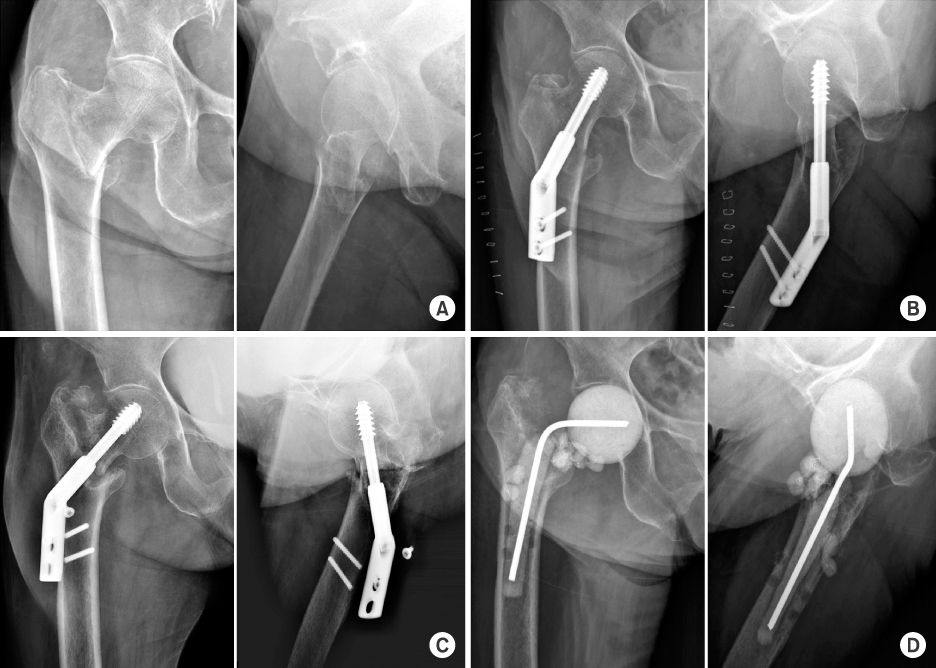
Fig. 1
(A) Preoperative X-ray. (B) X-ray taken immediately after the operation. An excessive lag screw telescope is observed due to a reduction loss. (C) X-ray taken 6 months after the operation. Varus collapse occurred due to non-union and breakage of distal cortical screw. (D) Conversion to hip replacement arthroplasty.
Fig. 2
(A) Preoperative X-ray. (B) X-ray taken immediately after the operation. (C) X-ray taken 7 months after the operation. Breakage of the lag screw, non-union of the fracture site, and radio-lucent shadow around the hardware are observed. The patient complained of systemic femur with right hip pain. (D) Girdlestone operation with antibiotic-loaded cement insertion was done. However, the patient expired due to sepsis.
Fig. 1
Fig. 2
Surgical Treatment for Stable 2-Part Intertrochanteric Femur Fracture Using Dynamic Hip Screw with 2-Hole Side Plate in Elderly Patients
Demographic Characteristics of Enrolled Patients
| Characteristic | Value |
|---|---|
| Sex (male:female) | 50 (17:33) |
| Age (yr) | 77.8±8.6 (65-101) |
| Follow-up period (mo) | 14.3±10.4 (6-60) |
| BMD (T-score) | −3.0±1.5 (−5.6 to −0.3) |
| Cormobidities | |
| Diabetes mellitus | 18 |
| Hypertension | 24 |
| Cerebrovascular accident | 9 |
| COPD | 2 |
| ASA physical status classification | |
| Class I | 9 |
| Class II | 21 |
| Class III | 16 |
| Class IV | 4 |
| AO classification of fracture | |
| 31-A1.1 | 41 |
| 31-A1.2 | 9 |
Values are presented as number (%), mean±standard deviation (range), or number only. BMD: Bone mineral density, COPD: Chronic obstructive pulmonary disease, ASA: American Society of Anesthesiologists.
Clawson's Ambulation Capacity Classification11)
| Class I | Wheelchair ambulation |
| Class II | Crutch, two cane |
| Class III | One cane or simple brace |
| Class IV | Self ambulation |
Clinical Results of Enrolled Patients
| Variable | Value |
|---|---|
| Length of skin incision (cm) | 9.8±1.1 (8-13) |
| Operation time (min) | 41.4±6.6 (30-60) |
| Ambulation capacity recovery rate before trauma by Clawson classification | |
| Class I | 100 (2/2) |
| Class II | 50.0 (2/4) |
| Class III | 50.0 (5/10) |
| Class IV | 67.6 (23/34) |
Values are presented as mean±standard deviation (range) or percent (number/total number).
Radiologic Results of Enrolled Patients
| Variable | Value |
|---|---|
| Bone union rate | 96.0 (48/50) |
| Bone union time (wk) | 10.6±1.7 (8-16) |
| Reduction status by Fogagnolo classification | |
| Good | 46 |
| Acceptable | 3 |
| Poor | 1 |
| Tip apex distance (mm) | 18.9±4.0 (9.0-24.9) |
| Cleveland index | |
| Zone 5 | 45 |
| Zone 6 | 2 |
| Zone 8 | 3 |
| Telescope length of lag screw (mm) | 4.9±5.1 (0.1-19.4) |
Values are presented as percent (number/total number), mean±standard deviation (range), number only.
Table 1
Demographic Characteristics of Enrolled Patients
Values are presented as number (%), mean±standard deviation (range), or number only. BMD: Bone mineral density, COPD: Chronic obstructive pulmonary disease, ASA: American Society of Anesthesiologists.
Table 2
Clawson's Ambulation Capacity Classification11)
Table 3
Clinical Results of Enrolled Patients
Values are presented as mean±standard deviation (range) or percent (number/total number).
Table 4
Radiologic Results of Enrolled Patients
Values are presented as percent (number/total number), mean±standard deviation (range), number only.

