 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(2); 2011 > Article
-
Review Article from Symposium
- Treatment of Peri-prosthetic Fracture about Total Knee Replacement
- Sang-Hyup Yoon, M.D., Chang-Wug Oh, M.D.
-
Journal of the Korean Fracture Society 2011;24(2):206-211.
DOI: https://doi.org/10.12671/jkfs.2011.24.2.206
Published online: April 13, 2011
Department of Orthopaedic Surgery, Kyungpook National University Hospital, Daegu, Korea.
- Address reprint requests to: Chang-Wug Oh, M.D. Department of Orthopaedic Surgery, Kyungpook National University Hospital, 50, Samdeok 2-ga, Jung-gu, Daegu 700-721, Korea. Tel: 82-53-420-5630, Fax: 82-53-422-6605, cwoh@knu.ac.kr
Copyright © 2011 The Korean Fracture Society
- 1,939 Views
- 53 Download
- 1. Berry DJ. Epidemiology: hip and knee. Orthop Clin North Am, 1999;30:183-190.PubMed
- 2. Felix NA, Stuart MJ, Hanssen AD. Periprosthetic fractures of the tibia associated with total knee arthroplasty. Clin Orthop Relat Res, 1997;345:113-124.Article
- 3. Lesh ML, Schneider DJ, Deol G, Davis B, Jacobs CR, Pellegrini VD Jr. The consequences of anterior femoral notching in total knee arthroplasty. A biomechanical study. J Bone Joint Surg Am, 2000;82:1096-1101.
- 4. Lewis PL, Rorabeck CH, Angliss RD. Fractures of the femur, tibia, and patella after total knee arthroplasty: Decision making and principles of management. Instr Course Lect, 1998;47:449-460.PubMed
- 5. Oh CW, Oh JK, Kyung HS, et al. Double plating of unstable proximal tibial fractures using minimally invasive percutaneous osteosynthesis technique. Acta Orthop, 2006;77:524-530.ArticlePubMed
- 6. Peters CL, Hennessey R, Barden RM, Galante JO, Rosenberg AG. Revision total knee arthroplasty with a cemented posterior-stabilized or constrained condylar prosthesis: a minimum 3-year and average 5-year follow-up study. J Arthroplasty, 1997;12:896-903.
- 7. Petersen MM, Lauritzen JB, Pedersen JG, Lund B. Decreased bone density of the distal femur after uncemented knee arthroplasty. A 1-year follow-up of 29 knees. Acta Orthop Scand, 1996;67:339-344.Article
- 8. Ricci WM, Borrelli J Jr. Operative management of periprosthetic femur fractures in the elderly using biological fracture reduction and fixation techniques. Injury, 2007;38:Suppl 3. S53-S58.Article
- 9. Schütz M, Müller M, Krettek C, et al. Minimally invasive fracture stabilization of distal femoral fractures with the LISS: a prospective multicenter study. Results of a clinical study with special emphasis on difficult cases. Injury, 2001;32:3 Suppl. SC48-SC54.
- 10. Sharkey PF, Hozack WJ, Callaghan JJ, et al. Acetabular fracture associated with cementless acetabular component insertion: a report of 13 cases. J Arthroplasty, 1999;14:426-431.
- 11. Su ET, DeWal H, Di Cesare PE. Periprosthetic femoral fractures above total knee replacements. J Am Acad Orthop Surg, 2004;12:12-20.Article
- 12. Thompson NW, McAlinden MG, Breslin E, Crone MD, Kernohan WG, Beverland DE. Periprosthetic tibial fractures after cementless low contact stress total knee arthroplasty. J Arthroplasty, 2001;16:984-990.Article
- 13. Wang CJ, Wang JW, Weng LH, Hsu CC, Huang CC, Chen HS. The effect of alendronate on bone mineral density in the distal part of the femur and proximal part of the tibia after total knee arthroplasty. J Bone Joint Surg Am, 2003;85:2121-2126.Article
REFERENCES
Fig. 1Lewis and Rorabeck classification of supracondylar periprosthetic femoral fracture classification. Type I: Undisplaced fracture, prosthesis stable. Type II: Displaced fracture, prosthesis stable. Type III: Unstable prosthesis with or without fracture displacement.
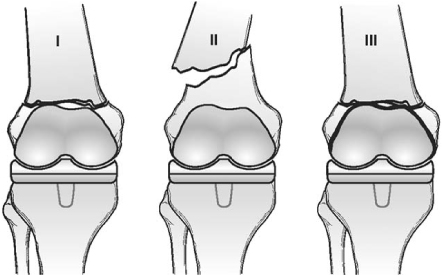
Fig. 2Anteroposterior and lateral views of supracondylar periprosthetic femoral fracture classification by Su et al. Type I: Fracture proximal to femoral knee component. Type II: Fracture originating at the proximal aspect of the femoral knee component and extending proximally. Type III: Any part of the fracture line is distal to the upper edge of the anterior flange of the femoral knee component.
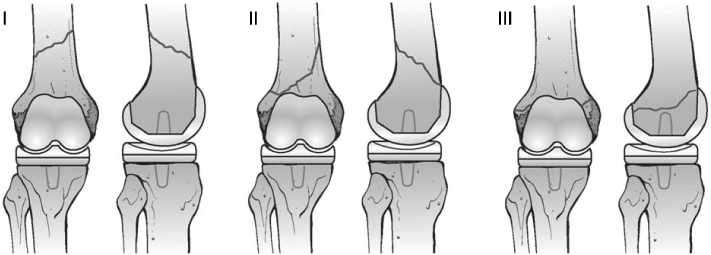
Fig. 3Classification for periprosthetic fractures of the tibia associated with total knee arthroplasty. There are four types, subclassified as A (prosthesis radiographically well fixed), B (loose), and C (intraoperative). Type I fracture involves the tibial plateau, type II fracture is adjacent to the prosthetic stem, type III fracture is distal to the stem, and type IV fracture involves the tibial tubercle.
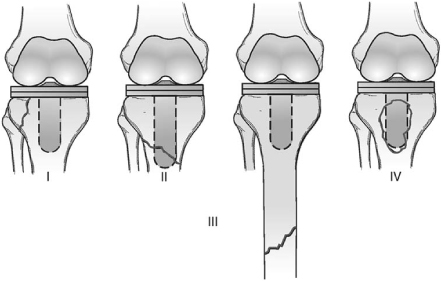
Fig. 4
(A) Initial anteroposterior radiograph shows a type II periprosthetic supracondylar femoral fracture.
(B) MIPO procedure was performed with a precontoured locking plate application.
(C) Immediate postoperative AP view.
(D) AP and lateral radiographs show a good healing at the final follow-up.
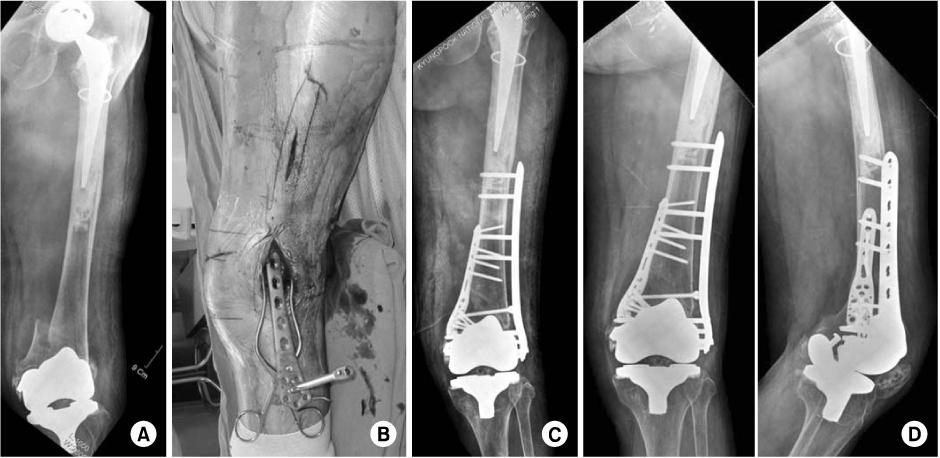
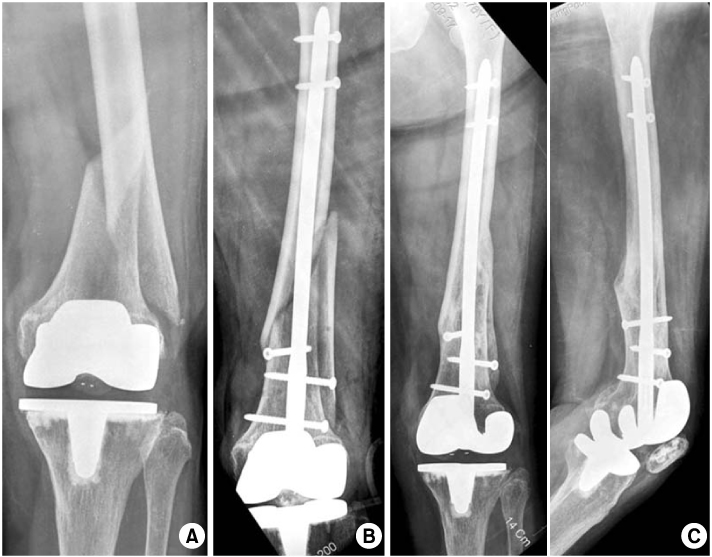
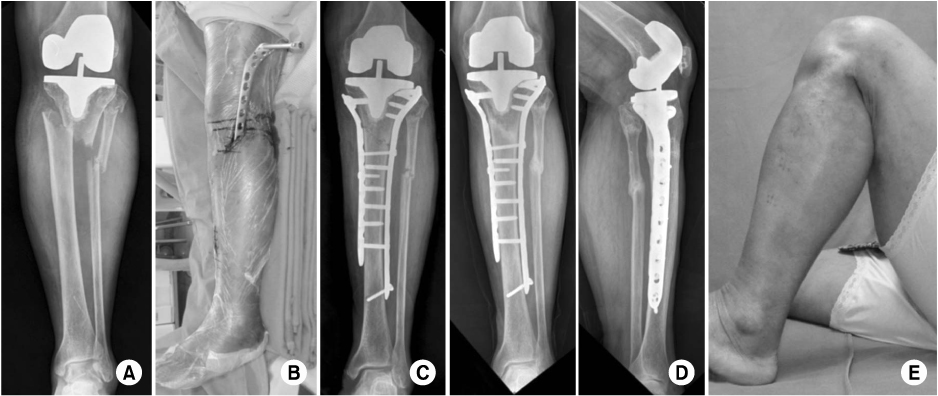
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteTreatment of Peri-prosthetic Fracture about Total Knee Replacement
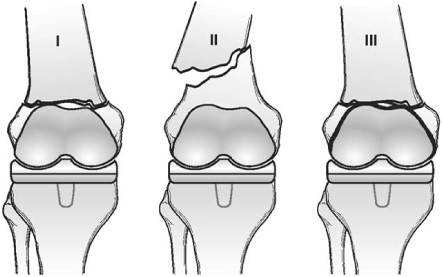
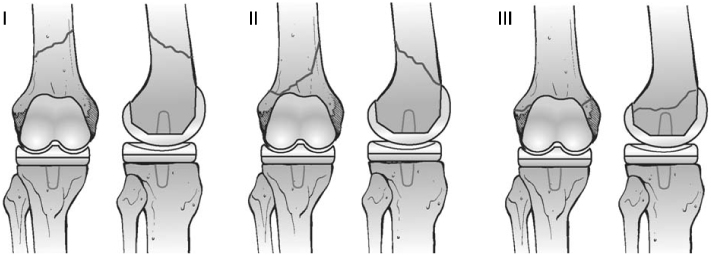
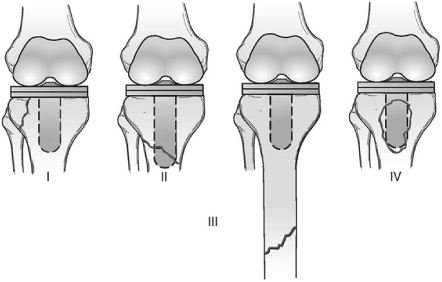
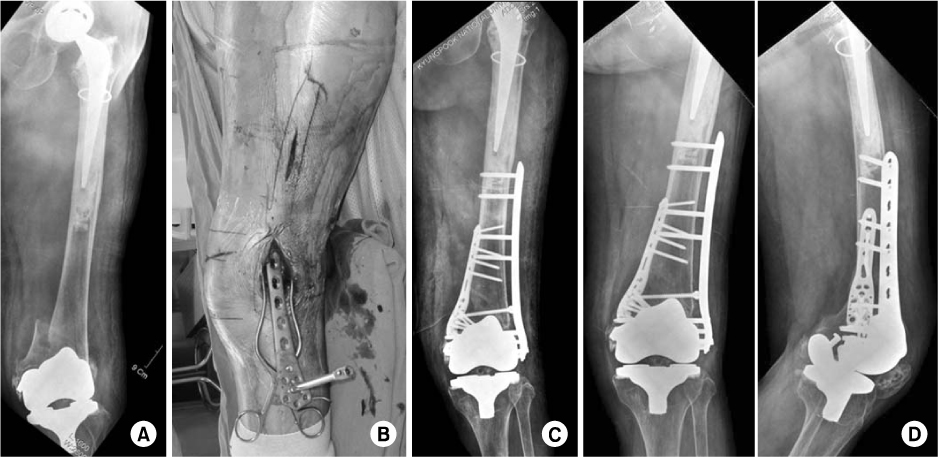
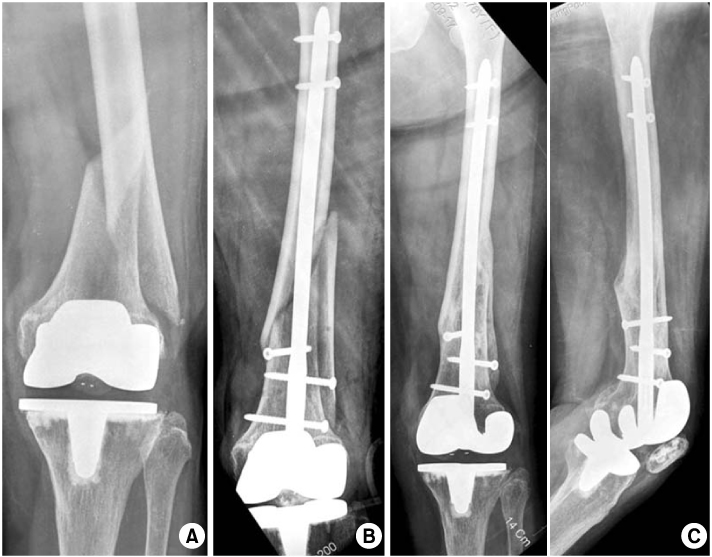

Fig. 1
Lewis and Rorabeck classification of supracondylar periprosthetic femoral fracture classification. Type I: Undisplaced fracture, prosthesis stable. Type II: Displaced fracture, prosthesis stable. Type III: Unstable prosthesis with or without fracture displacement.
Fig. 2
Anteroposterior and lateral views of supracondylar periprosthetic femoral fracture classification by Su et al. Type I: Fracture proximal to femoral knee component. Type II: Fracture originating at the proximal aspect of the femoral knee component and extending proximally. Type III: Any part of the fracture line is distal to the upper edge of the anterior flange of the femoral knee component.
Fig. 3
Classification for periprosthetic fractures of the tibia associated with total knee arthroplasty. There are four types, subclassified as A (prosthesis radiographically well fixed), B (loose), and C (intraoperative). Type I fracture involves the tibial plateau, type II fracture is adjacent to the prosthetic stem, type III fracture is distal to the stem, and type IV fracture involves the tibial tubercle.
Fig. 4
(A) Initial anteroposterior radiograph shows a type II periprosthetic supracondylar femoral fracture.
(B) MIPO procedure was performed with a precontoured locking plate application.
(C) Immediate postoperative AP view.
(D) AP and lateral radiographs show a good healing at the final follow-up.
Fig. 5
(A) Anteroposterior radiograph shows a periprosthetic fracture starting proximal to the femoral component.
(B) Closed reduction and fixation was performed using a retrograde nail.
(C) Fracture was healed uneventfully at 10 month postoperatively.
Fig. 6
(A) Type III periprosthetic tibia fracture in a 67 year-old lady with rheumatoid arthritis.
(B, C) Bilateral locking plate was applied using minimally invasive plate osteosynthesis (MIPO) technique.
(D, E) The fracture was united with good function.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Treatment of Peri-prosthetic Fracture about Total Knee Replacement

