 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 28(3); 2015 > Article
-
Review Article
- Management of Long Bone Fractures with Severe Bone Defect
- Jae-Woo Cho, M.D., Jinil Kim, M.D., Han-Ju Kim, M.D., Jong-Keon Oh, M.D.
-
Journal of the Korean Fracture Society 2015;28(3):205-214.
DOI: https://doi.org/10.12671/jkfs.2015.28.3.205
Published online: July 22, 2015
Department of Orthopedic Surgery, Korea University Guro Hospital, Seoul, Korea.
- Address reprint requests to: Jong-Keon Oh, M.D. Department of Orthopedic Surgery, Korea University Guro Hospital, 148 Gurodong-ro, Guro-gu, Seoul 152-703, Korea. Tel: 82-2-2626-3088, Fax: 82-2-2626-1163, jkoh@korea.ac.kr
Copyright © 2015 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,340 Views
- 23 Download
- 1 Crossref
- 1. Mauffrey C, Barlow BT, Smith W. Management of Segmental Bone Defects. J Am Acad Orthop Surg, 2015;23:143-153.Article
- 2. Keating JF, Simpson AH, Robinson CM. The management of fractures with bone loss. J Bone Joint Surg Br, 2005;87:142-150.ArticlePDF
- 3. Gouron R, Deroussen F, Plancq MC, Collet LM. Bone defect reconstruction in children using the induced membrane technique: a series of 14 cases. Orthop Traumatol Surg Res, 2013;99:837-843.Article
- 4. Uzel AP, Lemonne F, Casoli V. Tibial segmental bone defect reconstruction by Ilizarov type bone transport in an induced membrane. Orthop Traumatol Surg Res, 2010;96:194-198.Article
- 5. Karger C, Kishi T, Schneider L, Fitoussi F, Masquelet AC. French Society of Orthopaedic Surgery and Traumatology (SoFCOT). Treatment of posttraumatic bone defects by the induced membrane technique. Orthop Traumatol Surg Res, 2012;98:97-102.Article
- 6. Zhen P, Hu YY, Luo ZJ, Liu XY, Lu H, Li XS. One-stage treatment and reconstruction of Gustilo Type III open tibial shaft fractures with a vascularized fibular osteoseptocutaneous flap graft. J Orthop Trauma, 2010;24:745-751.Article
- 7. Lasanianos NG, Kanakaris NK, Giannoudis PV. Current management of long bone large segmental defects. Orthop Trauma, 2010;24:149-163.Article
- 8. El-Rosasy MA. Acute shortening and re-lengthening in the management of bone and soft-tissue loss in complicated fractures of the tibia. J Bone Joint Surg Br, 2007;89:80-88.ArticlePDF
- 9. DeCoster TA, Gehlert RJ, Mikola EA, Pirela-Cruz MA. Management of posttraumatic segmental bone defects. J Am Acad Orthop Surg, 2004;12:28-38.Article
- 10. Bosse MJ, MacKenzie EJ, Kellam JF, et al. A prospective evaluation of the clinical utility of the lower- extremity injury-severity scores. J Bone Joint Surg Am, 2001;83:3-14.Article
- 11. Masquelet AC, Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop Clin North Am, 2010;41:27-37.Article
REFERENCES
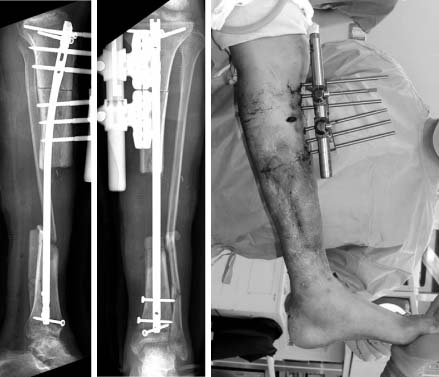
Fig. 1

Plain radiographs and clinical photo of AO type 42-C3, open fracture G-A type IIIb in a 44-year-old female patient.
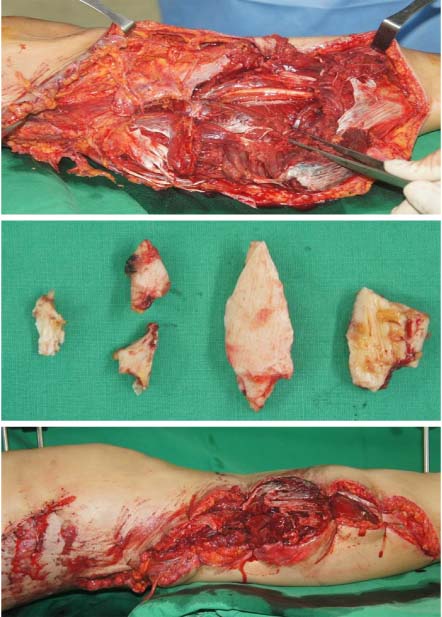
Fig. 3

Bone defect was filled with an antibiotic loaded polymethyl methacrylate spacer. A temporary external fixator and vacuum assisted closure system were applied.
Fig. 4

'Fix and Flap' internal fixation was performed using an interlocking intramedullary nail and soft tissue defect was reconstructed by anterolateral thigh flap.


Fig. 7

Plain radiographs and clinical photo of AO type 33-C3, open fracture G-A type II in a 23-year-old female patient.
Fig. 8
Clinical photos and serial anteroposterior and lateral radiographs of the right femur. (A) 1st stage: debridement, antibiotic loaded polymethyl methacrylate spacer insertion and bridging external fixator application. (B) 2nd stage: secondary debridement, cement change, and articular reconstruction. (C) 3rd stage: convert to internal fixation using a pre-contoured locking plate.
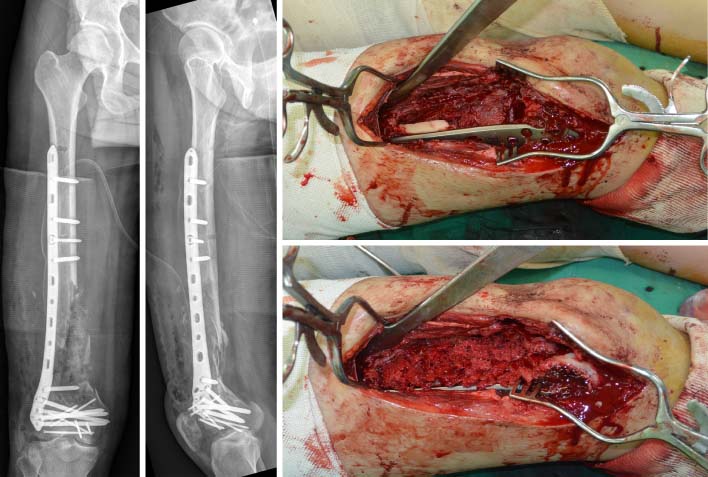

Fig. 11
Plain radiographs and clinical photo of AO type 42-B2, open fracture G-A type IIIb in a 25-year-old male patient. A contaminated and devitalized bony wedge remained with wire.
Fig. 12

Systemized radical debridement was performed and the defect was filled with antibiotic loaded cement beads.
Fig. 13

Intramedullary nailing was performed and the soft tissue defect was reconstructed with Lattismus dorsi flap.
Fig. 14
Osteotomy was performed at the level of the proximal tibia and a mono external fixator was applied for distraction osteogenesis.
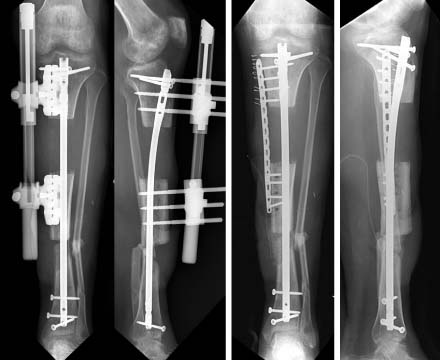

Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Treatment Strategy of Infected Nonunion
Hyoung-Keun Oh
Journal of the Korean Fracture Society.2017; 30(1): 52. CrossRef
 Cite
CiteManagement of Long Bone Fractures with Severe Bone Defect

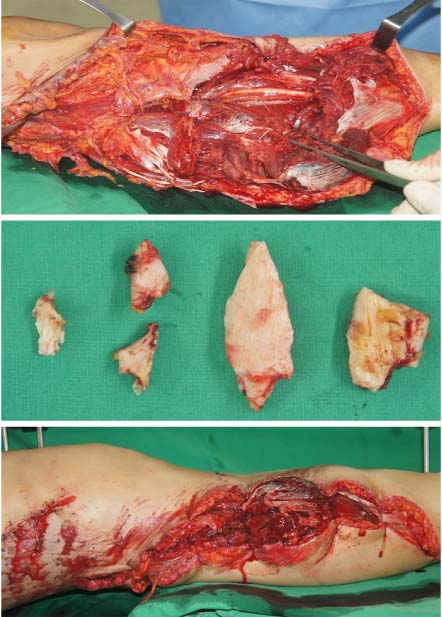


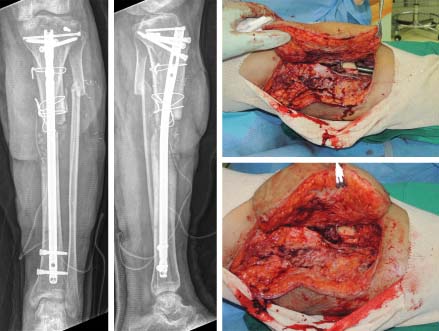


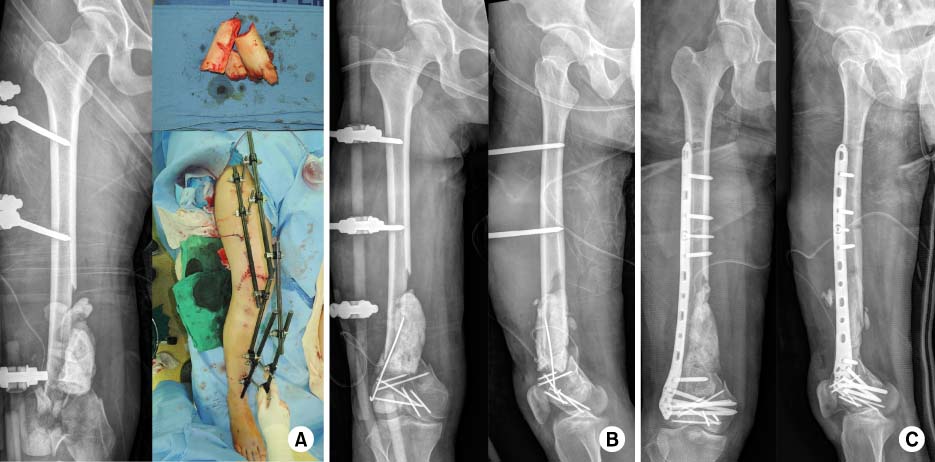
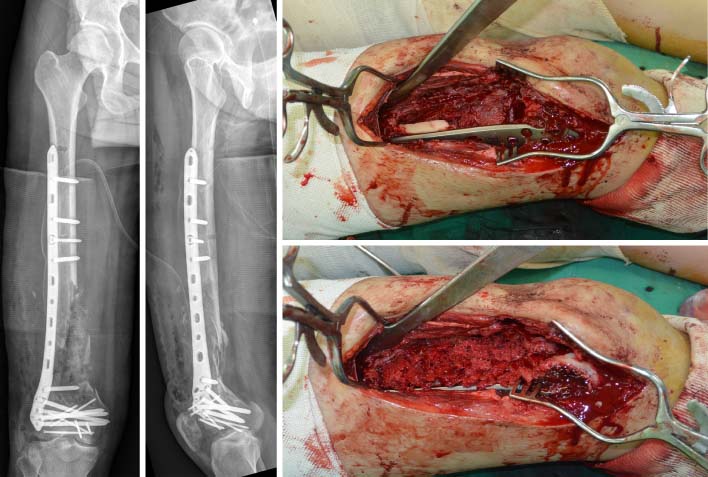

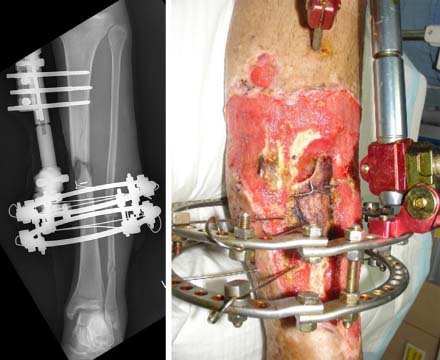


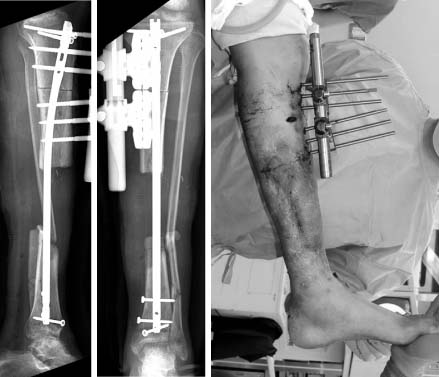


Fig. 1
Plain radiographs and clinical photo of AO type 42-C3, open fracture G-A type IIIb in a 44-year-old female patient.
Fig. 2
Systemic debridement was performed and devitalized wedges were removed.
Fig. 3
Bone defect was filled with an antibiotic loaded polymethyl methacrylate spacer. A temporary external fixator and vacuum assisted closure system were applied.
Fig. 4
'Fix and Flap' internal fixation was performed using an interlocking intramedullary nail and soft tissue defect was reconstructed by anterolateral thigh flap.
Fig. 5
Autogenous bone graft was performed using an induced membrane technique.
Fig. 6
Bony consolidation was achieved without complications.
Fig. 7
Plain radiographs and clinical photo of AO type 33-C3, open fracture G-A type II in a 23-year-old female patient.
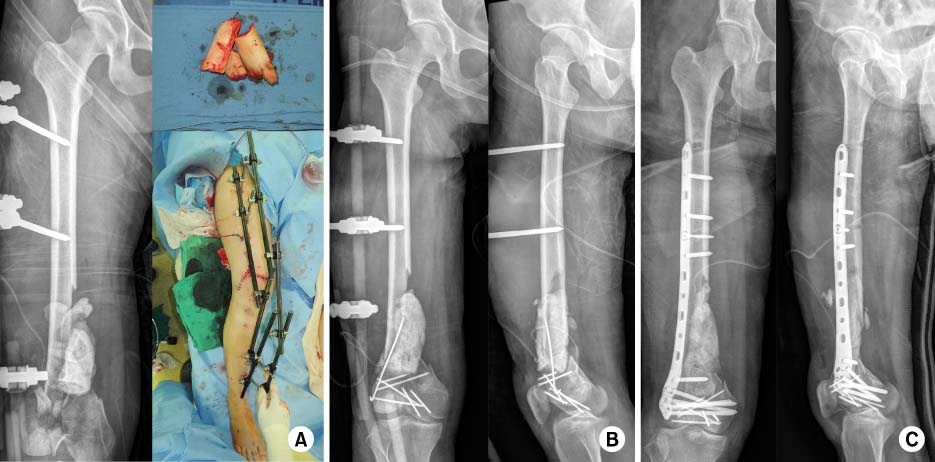
Fig. 8
Clinical photos and serial anteroposterior and lateral radiographs of the right femur. (A) 1st stage: debridement, antibiotic loaded polymethyl methacrylate spacer insertion and bridging external fixator application. (B) 2nd stage: secondary debridement, cement change, and articular reconstruction. (C) 3rd stage: convert to internal fixation using a pre-contoured locking plate.
Fig. 9
Autogenous bone graft was performed using an induced membrane technique.
Fig. 10
Follow-up at 4 months, bony consolidation was achieved without complications.
Fig. 11
Plain radiographs and clinical photo of AO type 42-B2, open fracture G-A type IIIb in a 25-year-old male patient. A contaminated and devitalized bony wedge remained with wire.
Fig. 12
Systemized radical debridement was performed and the defect was filled with antibiotic loaded cement beads.
Fig. 13
Intramedullary nailing was performed and the soft tissue defect was reconstructed with Lattismus dorsi flap.
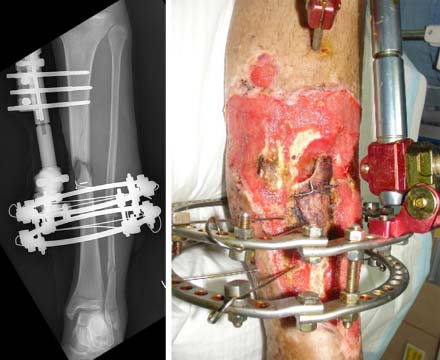
Fig. 14
Osteotomy was performed at the level of the proximal tibia and a mono external fixator was applied for distraction osteogenesis.
Fig. 15
After 3 months, the distraction fragment was docked at the distal fragment. Plate augmentation was performed using the minimally invasive plate osteosynthesis technique. Autogenous bone graft was performed at the docking site.
Fig. 16
Bony consolidation was achieved without complications.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Fig. 9
Fig. 10
Fig. 11
Fig. 12
Fig. 13
Fig. 14
Fig. 15
Fig. 16
Management of Long Bone Fractures with Severe Bone Defect

