 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 20(1); 2007 > Article
-
Original Article
- Treatment for the Supracondylar Fractures of the Distal Humerus with Cannulated Screw
- Jin Soo Park, M.D., Young Khee Chung, M.D., Jung Han Yoo, M.D., Kyu Cheol Noh, M.D., Kook Jin Chung, M.D., Dong Nyoung Lee, M.D.
-
Journal of the Korean Fracture Society 2007;20(1):58-63.
DOI: https://doi.org/10.12671/jkfs.2007.20.1.58
Published online: June 14, 2016
Department of Orthopaedic Surgery, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea.
- Address reprint requests to: Jin Soo Park, M.D. Department of Orthopaedic Surgery, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, 948-1, Daerim 1-dong, Yeongdeungpo-gu, Seoul 150-950, Korea. Tel: 82-2-829-5313, Fax: 82-2-834-1728, nyjspark@yahoo.co.kr
Copyright © The Korean Fracture Society. All rights reserved
- 1,319 Views
- 27 Download
Abstract
-
Purpose
- To evaluate the results of the treatment of the supracondylar fractures of the humerus according to the fixation methods with cannulated screw.
-
Materials and Methods
- Eight patients, aged 49 to 82 years (average, 65 years), were reviewed after a mean follow-up of 16 months (range, 12~24 months). According to AO classification all fractures were classified as type A2 (simple transverse supracondylar fracture). All patients underwent closed reduction. Percutaneous fixation with cannulated screws was performed in 8 patients. Three of 8 patients had associated medical problems and one patient had distal radius fracture. The functional results were assessed by the Mayo Elbow Performance Score.
-
Results
- Mean operation time was 59 minutes (45~75) and all the patients with cannulated screw fixation had bony union and were able to early ROM exercise. Mean ranges of motion was 5~120 degrees with excellent functional results. Functional evaluation of elbow joint by Mayo method showed mean value of 88 (75~95).
-
Conclusion
- The cannulated screw fixation of supracondylar fracture of humerus, especially in the elderly aged group with medical disease had excellent functional results (rigid fixation & early ROM exercise) due to shortening of surgery time and anesthesic time, combined with decreased technical difficulties of the surgical procedure.
- 1. Aitken GK, Rorabeck CH. Distal humeral fractures in the adult. Clin Orthop Relat Res, 1986;207:191-197.Article
- 2. Cassebaum WH. Operative treatment of T and Y fractures of the lower end of humerus. Am J Surg, 1952;83:265-270.
- 3. Chadwick CJ. The treatment of nonunion to the distal humerus by means of a transcondylar rod: a report of 3 cases. J Shoulder Elbow Surg, 2000;9:244-247.
- 4. Choi KH, Kang CN, Wang JM, Jang HJ. Clinical review of comminuted fracture of distal humerus in adult. J Korean Orthop Assoc, 1983;18:869-873.ArticlePDF
- 5. Eralp L, Kocaoglu M, Sar C, Atalar AC. Surgical treatment of distal intraarticular humeral fractures in adults. Int Orthop, 2001;25:46-50.ArticlePDF
- 6. Figgie MP, Inglis AE, Mow CS, Figgie HE 3rd. Salvage of non-union of supracondylar fracture of the humerus by total elbow arthroplasty. J Bone Joint Surg Am, 1989;71:1058-1065.Article
- 7. Gabel GT, Hanson G, Bennett JB, Noble PC, Tullos HS. Intraarticular fractures of the distal humerus in the adult. Clin Orthop Relat Res, 1987;216:99-108.Article
- 8. Gupta R. Intercondylar fractures of the distal humerus in adults. Injury, 1996;27:569-572.Article
- 9. Gupta R. Intercondylar fractures of the distal humerus in adults: a critical analysis of 55 cases. Injury, 2002;33:511-515.Article
- 10. Helfet DL, Schmeling GJ. Bicondylar intraarticular fractures of the distal humerus in adults. Clin Orthop Relat Res, 1993;292:26-36.Article
- 11. Horne G. Supracondylar fractures of the humerus in adults. J Trauma, 1980;20:71-74.Article
- 12. Jacobson SR, Glisson RR, Urbaniak JR. Comparison of distal humerus fracture fixation: a biomechanical study. J South Orthop Assoc, 1997;6:241-249.
- 13. Jupiter JB. Complex fractures of the distal part of the humerus and associated complications. Instr Course Lect, 1995;44:187-198.Article
- 14. Jupiter JB, Neff U, Holzach P, Allgower M. Intercondylar fractures of the humerus. An operative approach. J Bone Joint Surg Am, 1985;67:226-239.Article
- 15. Kang CS, Pyen YS, Son SW, Keon YC. Treatment of comminuted fracture of distal humerus in adult. J Korean Orthop Assoc, 1984;19:373-381.ArticlePDF
- 16. Kinik H, Atalar H, Mergen E. Management of distal humerus fractures in adults. Arch Orthop Trauma Surg, 1999;119:467-469.ArticlePDF
- 17. Low CK, Wong DH, Toh CL, Wong HP, Low YP. A retrospective study on elbow function after internal fixation of intercondylar fracture of adult humerus. Ann Acad Med Singapore, 1997;26:168-171.
- 18. McKee MD, Kim J, Kebaish K, Stephen DJ, Kreder HJ, Schemitsch EH. Functional outcome after open supracondylar fractures of the humerus. The effect of the surgical approach. J Bone Joint Surg Br, 2000;82:646-651.
- 19. McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR. Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am, 2000;82:1701-1707.Article
- 20. Moritomo H. Tricortical bone-block grafting for comminuted supracondylar and intercondylar fracture of the elbow in an elderly woman: case report. J Trauma, 2001;51:784-787.Article
- 21. Morrey BF. Functional evaluation of the elbow. In: Morrey BF, editor. The elbow and its disorders. 2nd ed. Philadelphia: WB Saunders Co; 1993. p. 112-115.
- 22. O'Driscoll SW. The triceps-reflecting anconeus pedicle (TRAP) approach for distal humeral fractures and nonunions. Orthop Clin North Am, 2000;31:91-101.Article
- 23. Pajarinen J, Bjorkenheim JM. Operative treatment of type C intercondylar fractures of the distal humerus: results after a mean follow-up of 2 years in a series of 18 patients. J Shoulder Elbow Surg, 2002;11:48-52.Article
- 24. Palvanen M, Kannus P, Niemi S, Parkkari J. Secular trends in the osteoporotic fractures of the distal humerus in elderly women. Eur J Epidemiol, 1998;14:159-164.ArticlePDF
- 25. Park SR, Kim HS, Kang JS, Lee WH, Lee JH, Park SJ. The treatment of comminuted fractures of distal humerus with rigid internal fixation and early motion. J Korean Fract Soc, 1998;11:28-33.Article
- 26. Ring D, Jupiter JB. Fractures of the distal humerus. Orthop Clin North Am, 2000;31:103-113.Article
REFERENCES
Fig. 1
(B) K-wires should be parallel to each other and the portion of the K-wires in the distal fragment should be located in the circular part (black dotted line) of the tear drop in lateral radiograph of the elbow in order not to encroach either into the trochlear fossa or olecranon fossa.
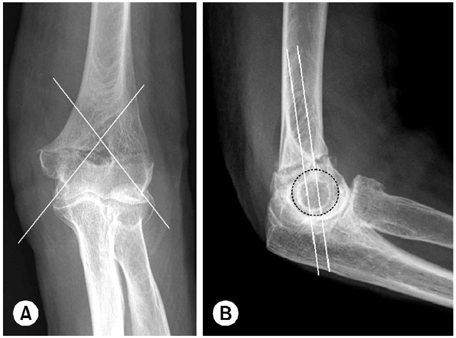
(A) Preliminary K-wires are inserted from the lowest point of each condyle across the fracture site thereby purchasing bone masses as much as possible.
Fig. 2
(B) Closed reduction and percutaneous fixation with full threaded cannulated screws was performed.
(C) Sixteen months postoperatively, stable bony union with nearly full range of motion was possible.

(A) A 80 year old woman sustained a A2 type fracture of left distal humerus.
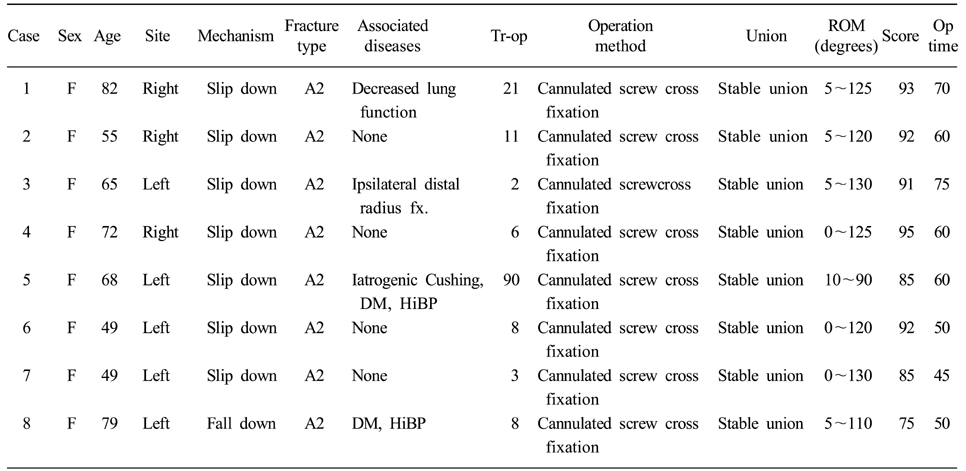

Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteTreatment for the Supracondylar Fractures of the Distal Humerus with Cannulated Screw
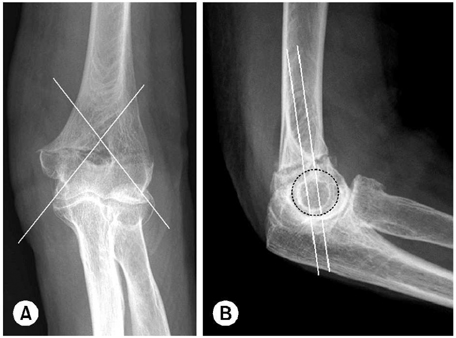

Fig. 1
(A) Preliminary K-wires are inserted from the lowest point of each condyle across the fracture site thereby purchasing bone masses as much as possible.
(B) K-wires should be parallel to each other and the portion of the K-wires in the distal fragment should be located in the circular part (black dotted line) of the tear drop in lateral radiograph of the elbow in order not to encroach either into the trochlear fossa or olecranon fossa.
Fig. 2
(A) A 80 year old woman sustained a A2 type fracture of left distal humerus.
(B) Closed reduction and percutaneous fixation with full threaded cannulated screws was performed.
(C) Sixteen months postoperatively, stable bony union with nearly full range of motion was possible.
Fig. 1
Fig. 2
Treatment for the Supracondylar Fractures of the Distal Humerus with Cannulated Screw
Patient data
Tr-op: Time interval between trauma and operation (days), ROM: Range of motion, Score: Mayo elbow performance score.
Mayo elbow performance score
Classification; Excellent: 90, Good: 75~89, Fair: 60~74, Poor: <60.
Table 1
Patient data
Tr-op: Time interval between trauma and operation (days), ROM: Range of motion, Score: Mayo elbow performance score.
Table 2
Mayo elbow performance score
Classification; Excellent: 90, Good: 75~89, Fair: 60~74, Poor: <60.

