 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Current issue
- Page Path
- HOME > Browse articles > Current issue
- Volume 39(3); July 2026
-


Review Articles
- How do we know a fracture has healed? A narrative review of radiographic bone union definitions and assessment methods
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(3):185-194. Published online May 20, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00150

-
 Abstract
Abstract
 PDF
PDF Supplementary Material
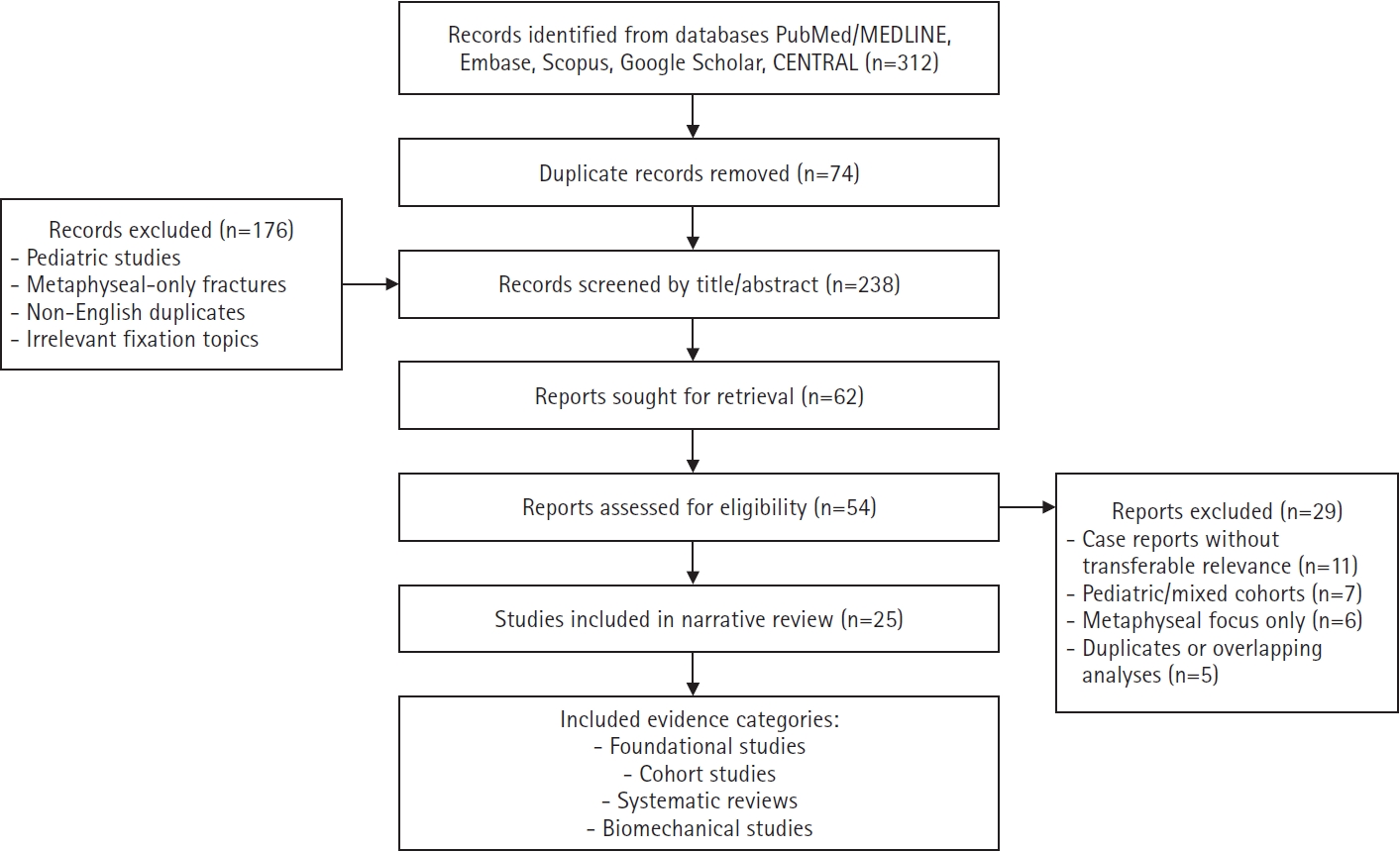
Supplementary Material - Bone union is the most commonly reported primary outcome in fracture treatment trials, yet no universally accepted radiographic definition exists. The widely taught criterion of “bridging callus on 3 of 4 cortices on anteroposterior and lateral radiographs” has no clearly identifiable primary source in the indexed literature. This narrative review traces the historical origins of radiographic bone union assessment, documents the heterogeneity of definitions used in clinical studies, and provides a comparative analysis of the standardized scoring systems developed to address this problem. A systematic PubMed search using six prespecified strategies, from database inception to March 2026, supplemented by hand-searching and citation tracking, identified 2,380 records. After screening, 359 articles on long-bone fractures were included. The “3 of 4 cortices” criterion appears most plausibly to derive from Panjabi’s 1985 finding that cortical continuity was the strongest radiographic predictor of fracture strength (r=0.80), but no traceable validation study was identified despite citation tracking through successive Cochrane reviews (CD008579, pub2‒pub4). In their 2008 study, Corrales and colleagues documented 11 different radiographic criteria across 123 studies, finding that ‘3 cortices’ was used in only 27%. Five standardized scoring systems (Radiographic Union Score for Tibial fractures [RUST], modified RUST [mRUST], Radiographic Union Score for Hip [RUSH], Radiographic Union Score for Humeral fractures [RUSHU], and Radiographic Humerus Union Measurement [RHUM]) have improved interobserver reliability within specific anatomical settings but remain fragmented by site and limited to secondary bone healing. A 2024 analysis by Bax et al. further illustrated that this inconsistency is not limited to fractures, documenting 13 different criteria and nine classification systems within the osteotomy literature. The most widely used radiographic union criterion likely emerged through clinical teaching rather than formal validation. A minimum reporting framework is proposed to improve standardization in future studies. Consensus definitions, cross-site validation, and more objective assessment strategies are needed to resolve this four-decade-old problem.
- 1,383 View
- 11 Download

- Spine OpenSim models: a narrative review of the literature
- Mohammad Taghi Karimi
- J Musculoskelet Trauma 2026;39(3):195-204. Published online July 7, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00171
-
Abstract
PDF
- The human spine is affected by various traumatic and pathological conditions that can impair function during daily activities. Several software programs have been developed to assess the risk of spinal injury, and OpenSim is one platform used for this purpose. Various OpenSim spine models have been developed to analyze parameters such as range of motion, moments applied to the vertebrae, muscle forces, and joint contact forces. This review aimed to compile the available OpenSim models that can be used to study the spine under normal and pathological conditions. Published studies using spine models in OpenSim were reviewed, and information on model outputs, availability, and validity was extracted. Keywords such as “spine models,” “lumbar models,” “musculoskeletal modeling,” and “trunk models” were used in combination with “OpenSim.” Eighty papers on spine models in OpenSim were identified, of which 23 were selected for final analysis. The available OpenSim models were classified as specific spine models (17 models) or full-body models (six models) that include the spine as a component. The available models can be used to assess injury risk, muscle forces, and joint contact forces in the cervical and lumbar spine. Full-body models allow examination of kinematics and joint contact forces at L5/S1, although only a limited number of muscles are represented in these models. Output validity has been evaluated in only a few models.
- 206 View
- 11 Download
- Current concepts and applications of internal fixation for forearm diaphyseal fractures
- Sung Yoon Jung, Min Kyun Cho, Dong-hee Kim, Sang Hyun Lee
- J Musculoskelet Trauma 2026;39(3):205-215. Published online July 3, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00087
-
Abstract
PDF
- Adult diaphyseal fractures of the forearm functionally behave as intra-articular injuries because forearm rotation depends on accurate restoration of length, axial alignment, rotation, and the native radial bow. This narrative review summarizes contemporary surgical options for adult forearm shaft fractures, including 3.5-mm plate osteosynthesis, dual mini-plate fixation, interlocking intramedullary nailing, and minimally invasive plate osteosynthesis (MIPO). Compression plating with 3.5-mm plates remains the reference standard for most fracture patterns, whereas other techniques should be regarded as selective, emerging, or salvage options according to their indication spectrum and evidence base. Mini-fragment dual plating may be useful for short segments or thin soft-tissue envelopes, although the supporting clinical evidence remains limited and meticulous biomechanical execution is essential. Interlocking intramedullary nailing is a viable alternative for carefully selected simple fracture patterns or soft-tissue-compromised situations, offering less invasive exposure but a narrower indication spectrum. MIPO may be considered for selected comminuted or soft-tissue-compromised diaphyseal fractures; however, its use in adult forearm fractures remains constrained by the high functional requirement for precise restoration of length, rotation, and the radial bow. To improve transparency, this review explicitly distinguishes established, evidence-supported methods from techniques supported mainly by limited retrospective data or institutional experience. A pattern-based pragmatic algorithm and expanded comparison table are provided to guide fixation selection according to the bone involved, fracture location, fracture morphology, soft-tissue condition, and evidence tier while minimizing complications such as nonunion, infection, nerve injury, refracture after plate removal, and radioulnar synostosis.
- 235 View
- 6 Download
Original Articles
- Postoperative sagittal alignment and reoperation predict late outcomes after plate fixation of AO/OTA 33C distal femur fractures: a retrospective cohort study
- Hee Gon Park
- J Musculoskelet Trauma 2026;39(3):216-226. Published online July 24, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00073
-
Abstract
PDF
- Background
Intra-articular distal femoral fractures are associated with high complication rates and variable late outcomes. Although the AO Foundation/Orthopaedic Trauma Association (AO/OTA) classification system is useful for describing injury severity and anticipating complications, whether fracture subtype alone determines clinically relevant late outcomes remains unclear. This study aimed to evaluate postoperative complications and late outcomes following plate fixation of intra-articular distal femoral fractures and to identify factors independently associated with final clinical outcomes.
Methods
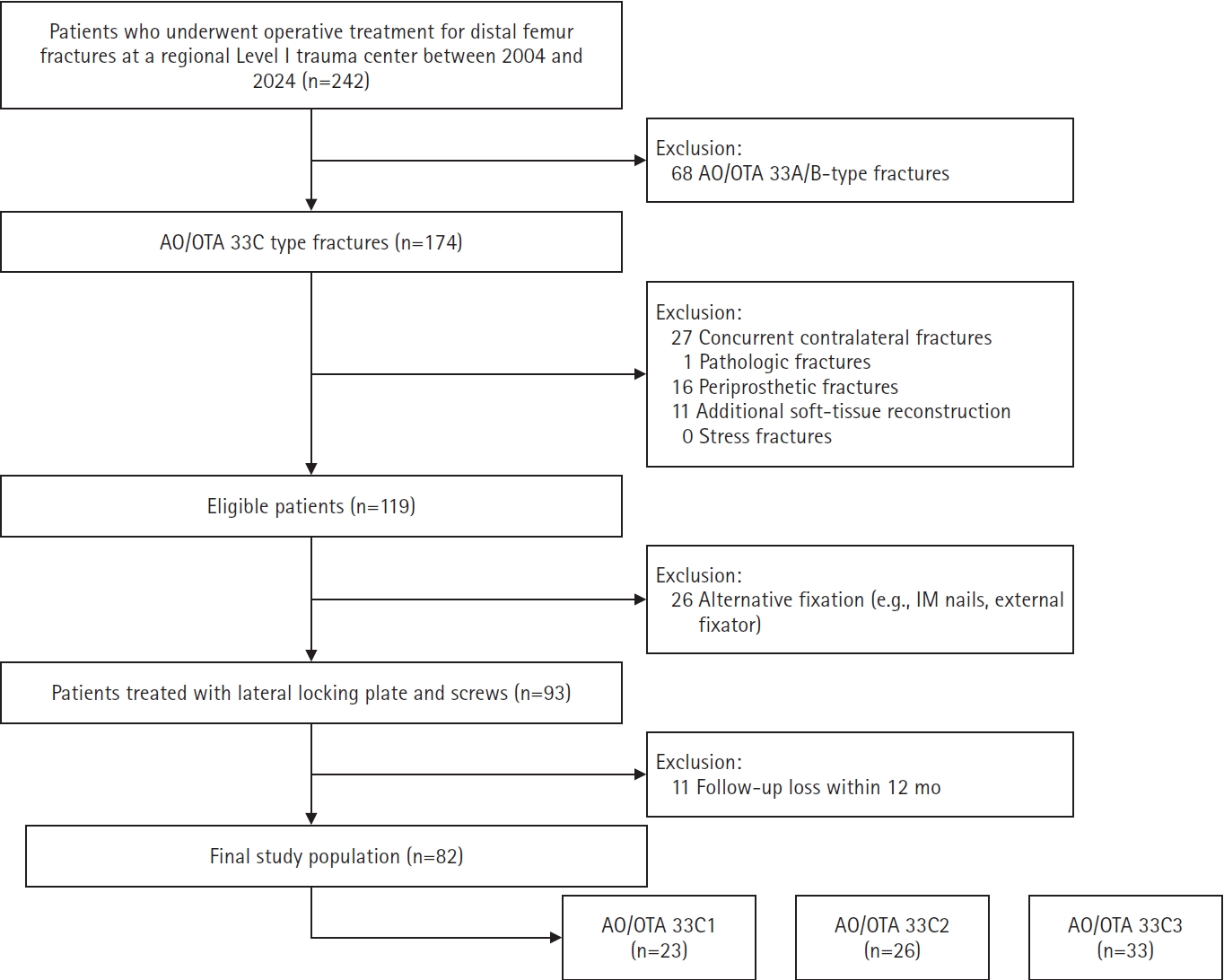
This retrospective cohort study was conducted at a regional Level I trauma center. Patients with AO/OTA 33C intra-articular distal femoral fractures who underwent plate fixation and were followed for at least 12 months were included. Radiographic parameters reflecting coronal and sagittal alignment were assessed using standardized measurement methods. Postoperative complications and reoperation were recorded as intermediate events. Clinically relevant late outcomes included final knee range of motion (ROM), leg length discrepancy, and radiographic osteoarthritis severity, assessed as the difference in Kellgren-Lawrence grade. Multivariable linear regression analyses were performed to identify factors independently associated with late outcomes.
Results
The 33C3 group (n=33) had significantly higher rates of open fracture (54.5%), nonunion (39.4%), and reoperation (45.5%) than the 33C1–2 group (n=49). At the final follow-up, 33C3 fractures were associated with lower mean ROM (P<0.001) and greater osteoarthritis progression (P<0.001). However, multivariable analysis showed that sagittal malalignment (Δ anatomical posterior distal femoral angle: β=−2.35, P=0.001) and reoperation (β=−17.5, P=0.001), rather than AO/OTA subtype itself, were independent predictors of final ROM.
Conclusions
Although fracture subtype according to the AO/OTA classification was associated with predictable complication patterns, clinically relevant late outcomes following intra-articular distal femoral fractures were more closely associated with postoperative alignment quality and the treatment course than with fracture classification alone. These findings highlight the importance of optimizing radiographic alignment and preventing complications that lead to reoperation to improve long-term outcomes after plate fixation. Level of evidence: III.
- 92 View
- 6 Download
- Open reduction and internal fixation for distal humerus fractures in older adults: a retrospective comparative study by osteoporosis status
- Tong Joo Lee, Hee Beom Shin, Yongseok Lee
- J Musculoskelet Trauma 2026;39(3):227-235. Published online July 15, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00101
-
Abstract
PDF
- Background
Distal humerus fractures in older patients, particularly those with osteoporosis, pose substantial treatment challenges because of increased fracture complexity and compromised bone stock. Open reduction and internal fixation (ORIF) is the preferred treatment but may be complicated by fixation failure. This study investigated the outcomes of ORIF in older osteoporotic and nonosteoporotic patients with complete articular distal humerus fractures.
Methods
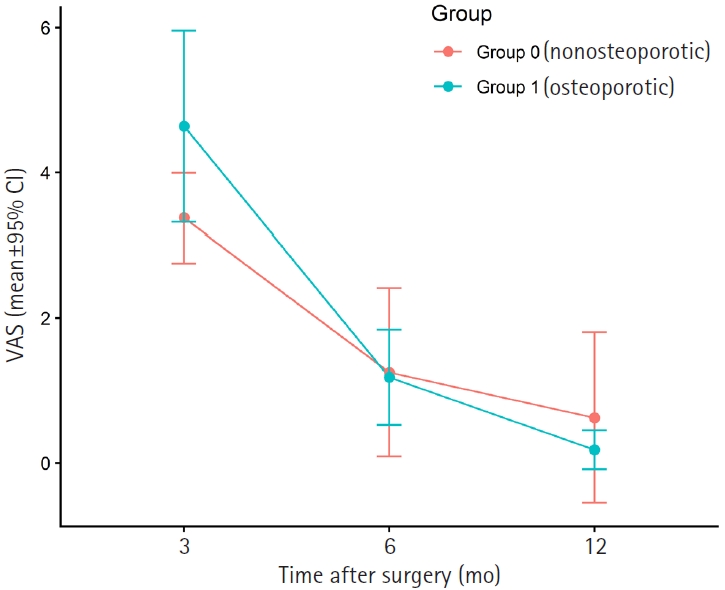
This retrospective study included 19 patients with Arbeitsgemeinschaft für Osteosynthesefragen/ Orthopaedic Trauma Association (AO/OTA) 13C distal humerus fractures who underwent surgical treatment between 2012 and 2024. The mean patient age was 79.1 years. Patients were divided into osteoporotic (n=11) and nonosteoporotic (n=8) groups based on the lowest recorded dual-energy X-ray absorptiometry T-score at the femoral neck or lumbar spine. Osteoporosis was defined as a T-score of −2.5 or lower, and the nonosteoporotic group included patients with osteopenia. All fractures were treated with ORIF using bicolumnar plating. All included patients completed 12 months of clinical follow-up for visual analog scale (VAS) and Mayo Elbow Performance Score (MEPS) assessments. Radiographic follow-up was recorded separately and continued until union was confirmed; imaging follow-up extended to 12 months or longer in 14 patients and was limited to 6 months in five asymptomatic patients after confirmed union.
Results
Both groups showed significant within-group improvement in pain, as assessed using the VAS, and function, as assessed using the MEPS, over time. Between-group comparisons at each follow-up time point showed no statistically significant differences in VAS or MEPS. No radiographic nonunion was observed during the available imaging follow- up, and complications were limited to one case of screw pullout/loosening and one case of postoperative stiffness.
Conclusions
ORIF provides reliable outcomes for older patients with complex distal humerus fractures, regardless of osteoporosis status, when stable reconstruction is achievable. These findings suggest that ORIF remains a viable treatment option, with satisfactory functional recovery and low complication rates in this population. Level of evidence: III.
- 175 View
- 7 Download
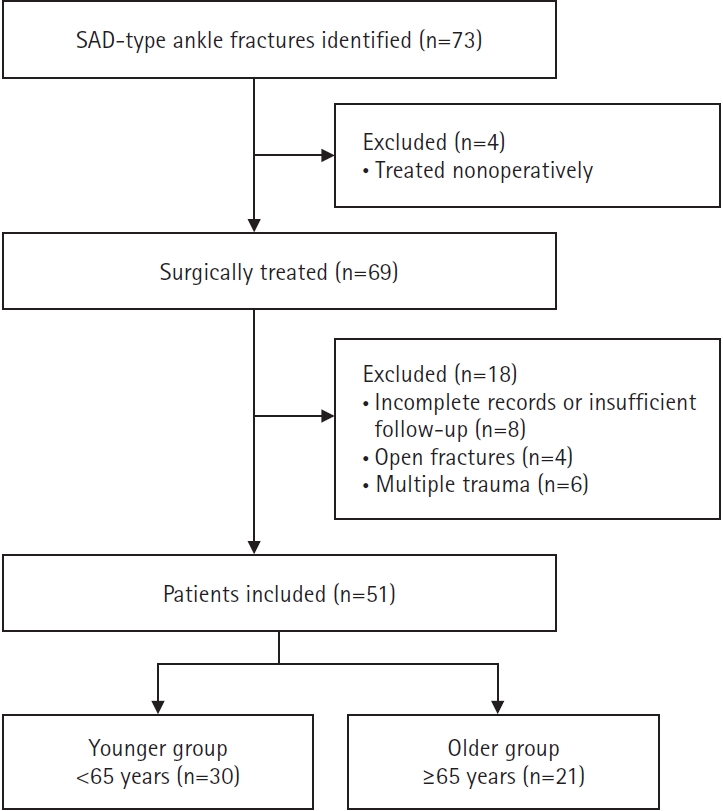
- Clinical and radiographic outcomes after surgical treatment of supination-adduction type ankle fractures in older (≥65 years) and younger (<65 years) patients: a retrospective single-center comparative study in Korea
- JungHo Lee, Bawoo Ko, Hongik Choi, Jun-young Lee
- J Musculoskelet Trauma 2026;39(3):236-244. Published online July 24, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00374
-
Abstract
PDF
- Background
Supination-adduction (SAD) ankle fractures involve a vertical medial malleolar fracture and potential tibial plafond impaction, but pattern-specific evidence in older patients remains limited. We compared postoperative complications and clinical/radiographic outcomes between older and younger patients and explored complication-associated factors within the older group.
Methods
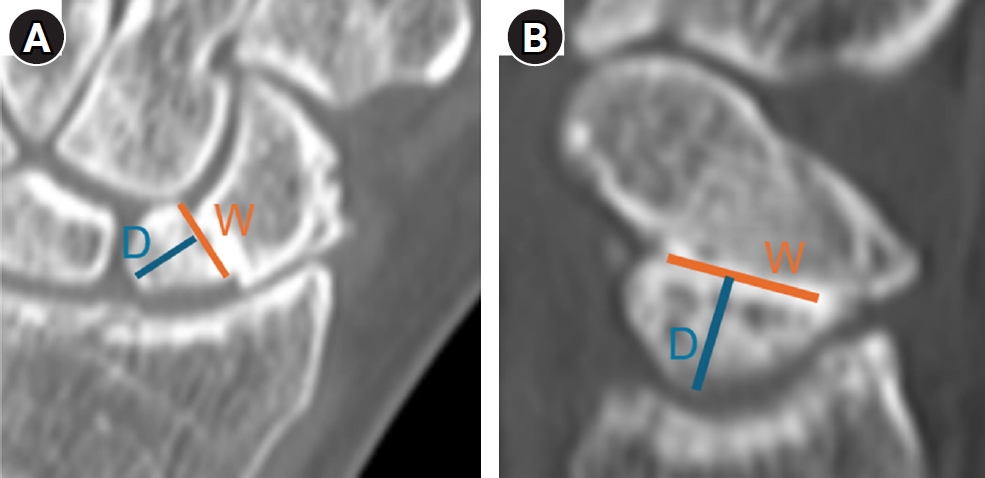
We retrospectively reviewed 51 patients who underwent surgery for SAD-type ankle fractures (2010–2020): 30 younger (<65 years) and 21 older (≥65 years). The primary outcome was a composite of surgical site infection, loss of reduction, or delayed union. Functional recovery was assessed using Olerud-Molander Ankle Score (OMAS) and American Orthopaedic Foot & Ankle Society (AOFAS) scores through 12 months. Union and posttraumatic osteoarthritis were assessed radiographically at ≥18 months. Preoperative dual- energy X-ray absorptiometry was performed in older patients for exploratory analyses.
Results
Postoperative complications were higher in the older group (38.1% vs. 10.0%, P=0.035). In older patients, diabetes mellitus was associated with complications (odds ratio [OR], 9.17; 95% confidence interval [CI], 1.15–73.24; P=0.037); smoking was not (OR, 5.50; 95% CI, 0.71–42.60; P=0.103). At 12 months, OMAS and AOFAS scores did not differ significantly. One older patient developed nonunion, and posttraumatic osteoarthritis occurred in one patient per group. Lower T-scores (mean, −2.3±0.5) correlated with greater tibial plafond impaction depth (3.1±1.2 mm; ρ=−0.46, P=0.036) and showed a borderline significant correlation with articular step-off (2.0±0.8 mm; ρ=−0.43, P=0.052).
Conclusions
Older patients had higher postoperative complication rates than younger patients, although 12-month functional and late radiographic outcomes were comparable. Diabetes was associated with complications, though the small sample warrants cautious interpretation. Findings support careful perioperative optimization and individualized fixation based on fracture morphology and bone quality in older patients, especially those with diabetes. Level of evidence: III.
- 105 View
- 4 Download
Case Reports
- Successful reconstruction and functional recovery of a pediatric medial malleolus defect in an 8-year-old girl using autologous iliac crest bone grafting in Korea: a case report
- Sung Yoon Jung, Dong-hee Kim, Sang Hyun Lee, Ki-Hun Kim
- J Musculoskelet Trauma 2026;39(3):245-251. Published online April 8, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00059

-
Abstract
PDF
- An 8-year-old girl presented after a traffic accident with a severe crush and degloving injury of the medial right ankle and foot, a distal tibiofibular fracture, and medial midfoot bone defects. After staged irrigation and debridement with temporary external fixation, definitive reconstruction was performed on August 6, 2016. The medial malleolar defect (2.5×2.0 cm) was reconstructed using a contoured autologous iliac crest bone graft secured with internal fixation, and medial stability was augmented using harvested gluteal fascia as a deltoid ligament substitute fixed with suture anchors. A bone-cement spacer was placed adjacent to the injured physis to mitigate physeal bridging, and the extensive soft-tissue defect was covered with a free anterolateral thigh flap and skin graft. During follow-up, progressive varus deformity and contracture were managed with corrective osteotomy and plating, Achilles tendon lengthening, Z-plasty, and Ilizarov fixation. At the final follow-up (March 6, 2025), the limb-length discrepancy was 5 mm, active ankle dorsiflexion was 0° (passive dorsiflexion 5°), and the patient was pain-free with full participation in daily activities, including hiking and dancing. This case emphasizes the value of an integrated staged strategy that combines bony reconstruction, medial stabilization, physeal management, and durable soft-tissue coverage during skeletal growth. Level of evidence: V.
- 773 View
- 12 Download
- Fixation with two headless compression screws and a distal-radius bone graft for proximal scaphoid nonunion with dorsal intercalated segment instability deformity: a report of three cases
- Seonjeong Lee, Won Sun Lee, Jae Kwang Kim
- J Musculoskelet Trauma 2026;39(3):252-261. Published online July 7, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00136
-
Abstract
PDF
- Proximal scaphoid nonunion is difficult to treat because the proximal fragment is small and biologically compromised. Secure fixation can be especially challenging when dorsal intercalated segment instability (DISI) is present and requires correction. We report three male patients with proximal scaphoid nonunion and DISI deformity who underwent volar fixation with two 2.4-mm headless compression screws and cancellous bone graft harvested from the distal radius at the Lister tubercle. Preoperative computed tomography confirmed a proximal nonunion line and proximal fragment dimensions considered sufficient for dual-screw fixation, and magnetic resonance imaging showed no definite avascular necrosis. Early postoperative computed tomography showed maintained fixation and alignment in all three patients. Although CT-confirmed union at final follow-up was not uniformly available, radiographic union defined on plain radiographs was achieved in all cases without loss of alignment or carpal collapse. Carpal alignment improved in two patients, but DISI persisted in one. One patient underwent secondary removal of a preexisting loose body and one screw. This small case series suggests that dual-screw fixation with cancellous grafting may be technically feasible in selected proximal scaphoid nonunions with concomitant DISI. Level of evidence: V.
- 177 View
- 6 Download
- Open distal radius fracture with ulnar neurovascular injury treated with dorsal spanning plate fixation and vein interposition grafting: a case report
- Kyeong-Eon Kim, Ho-Yong Lee, Shin-Woo Lee, Ji-Sup Kim
- J Musculoskelet Trauma 2026;39(3):262-268. Published online July 20, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00164

-
Abstract
PDF
- Open comminuted intra-articular distal radius fractures with associated ulnar neurovascular injury are rare; furthermore, these injuries are challenging because skeletal stabilization, arterial reconstruction, nerve assessment, and soft-tissue coverage must be coordinated. We report the case of an 80-year-old female patient who presented after a fall from stairway with a severe open distal radius fracture and a volar-ulnar distal forearm wound. She reported numbness and tingling in the ring and small fingers, with a cold sensation and delayed capillary refill. Imaging showed a severely comminuted intra-articular distal radius fracture (AO/OTA type 23-C3). Emergency surgery was performed within 6 hours. First, a dorsal spanning plate was applied, and the small volar lunate facet fragment was fixed with a volar lunate facet plate. After debridement of the injured ulnar artery, a segmental defect remained and was reconstructed using a reversed basilic vein interposition graft harvested from the ipsilateral proximal forearm. The contused but continuous ulnar nerve was treated with neurolysis. The soft-tissue defect was managed with an acellular dermal matrix and negative-pressure wound therapy, followed by staged full-thickness skin grafting 1 week later. At 1 year postoperatively, bony union was achieved, and the functional outcomes were satisfactory. Level of evidence: V.
- 100 View
- 7 Download
- Radiocarpal subluxation after volar plating due to an insufficiently supported dorsal key fragment: a case report
- Yeongyoon Koh, Kanghun Yu, Jong Woong Park, In Cheul Choi
- J Musculoskelet Trauma 2026;39(3):269-274. Published online July 3, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00185

-
Abstract
PDF
- Distal radius fractures are commonly managed using volar locking plate fixation, which provides stable fixation in most cases. However, certain fracture patterns involving dorsal key fragments may not be adequately stabilized with a volar approach alone, even when intraoperative reduction appears satisfactory. We report the case of a 58-year-old male patient with a complex intra-articular distal radius fracture involving a dorsoulnar corner (DUC) fragment. Preoperative computed tomography revealed a dorsal fragment associated with subtle dorsal radiocarpal subluxation. Despite this finding, the fragment was considered amenable to fixation through a volar approach because it was relatively large. Although satisfactory reduction was achieved intraoperatively, early postoperative imaging demonstrated progressive dorsal radiocarpal subluxation due to displacement of the DUC fragment, while overall alignment parameters remained preserved. Revision surgery with additional dorsal buttress fixation successfully restored stability. This case highlights the critical importance of recognizing dorsal key fragments and achieving adequate dorsal support during fixation, as failure to provide sufficient support may result in delayed instability despite acceptable initial reduction. Level of evidence: V.
- 212 View
- 7 Download
 First
First Prev
Prev

