 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Case report
- Radiocarpal subluxation after volar plating due to an insufficiently supported dorsal key fragment: a case report
- Yeongyoon Koh, Kanghun Yu, Jong Woong Park, In Cheul Choi
- Received April 28, 2026 Accepted May 13, 2026 Published online July 3, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00185 [Epub ahead of print]
-
 Abstract
Abstract
 PDF
PDF - Distal radius fractures are commonly managed using volar locking plate fixation, which provides stable fixation in most cases. However, certain fracture patterns involving dorsal key fragments may not be adequately stabilized with a volar approach alone, even when intraoperative reduction appears satisfactory. We report the case of a 58-year-old male patient with a complex intra-articular distal radius fracture involving a dorsoulnar corner (DUC) fragment. Preoperative computed tomography revealed a dorsal fragment associated with subtle dorsal radiocarpal subluxation. Despite this finding, the fragment was considered amenable to fixation through a volar approach because it was relatively large. Although satisfactory reduction was achieved intraoperatively, early postoperative imaging demonstrated progressive dorsal radiocarpal subluxation due to displacement of the DUC fragment, while overall alignment parameters remained preserved. Revision surgery with additional dorsal buttress fixation successfully restored stability. This case highlights the critical importance of recognizing dorsal key fragments and achieving adequate dorsal support during fixation, as failure to provide sufficient support may result in delayed instability despite acceptable initial reduction.
- 69 View
- 2 Download

Review Article
- Definitive fixation for traumatic pelvic ring injuries: a dynamically informed, posterior-referenced framework
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(2):73-82. Published online March 24, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00045
-
Abstract
PDF
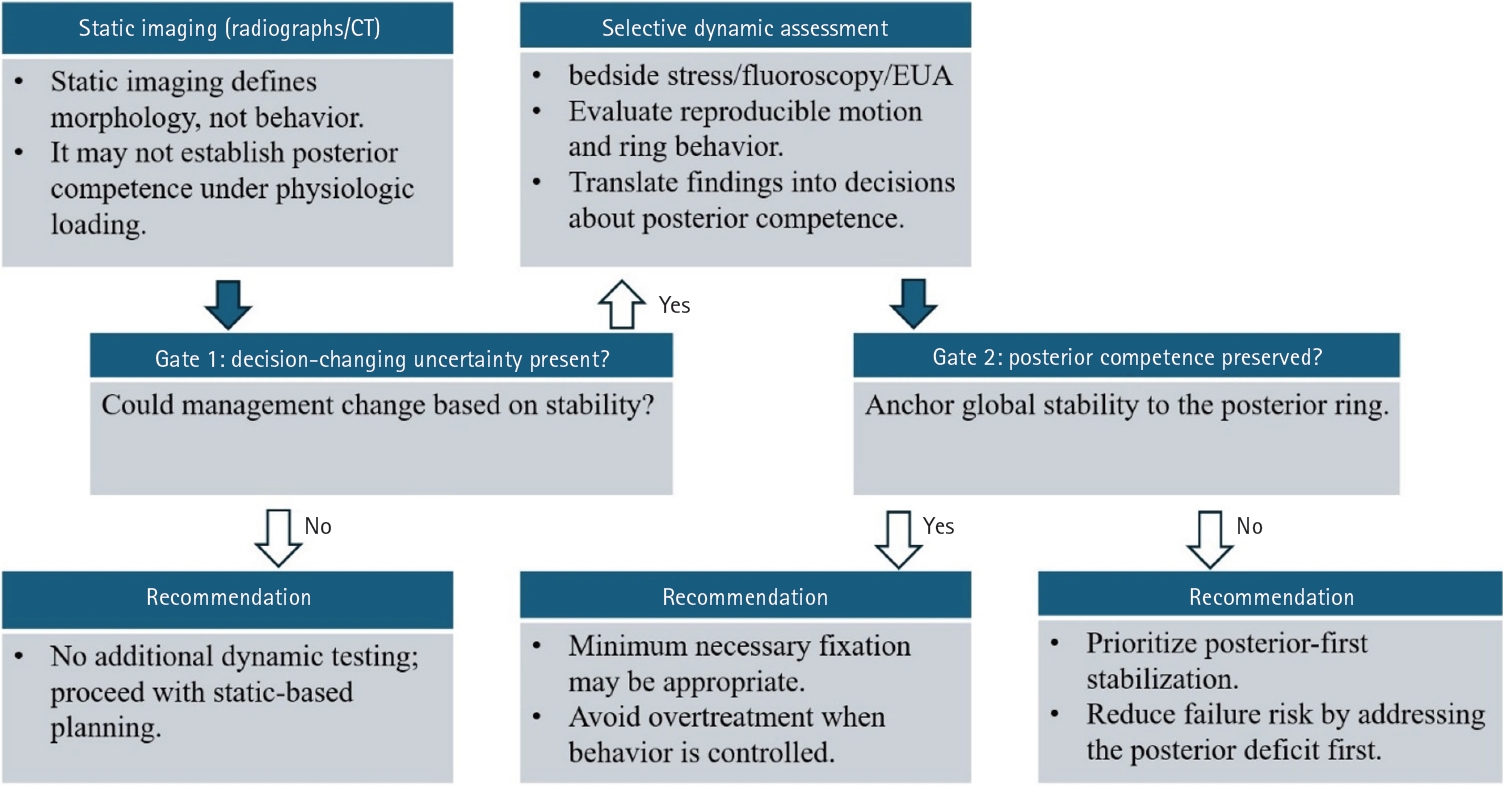
- Optimal definitive fixation for traumatic pelvic ring injuries remains challenging because static radiographs and computed tomography, although essential for defining morphology, do not consistently predict load-dependent behavior during early mobilization. This uncertainty contributes to substantial practice variation and continued reliance on simplified displacement thresholds, such as the 2.5 cm rule. Such rules can misclassify instability by underrepresenting posterior competence and by privileging static measurements over functional behavior. In this narrative review, we propose a dynamically informed, posterior- referenced framework composed of three linked elements: (1) decision-linked terminology that explicitly distinguishes dynamic instability, radiographic change, and clinical failure; (2) selective stress-based assessment when uncertainty is likely to alter management; and (3) escalation along a fixation continuum that weighs incremental stability against operative burden. When static imaging cannot establish posterior competence with confidence, we outline selective stress-based approaches to assess pelvic ring behavior and to translate demonstrated instability into fixation selection along a defined continuum. Across all steps, the framework emphasizes minimum necessary fixation and explicitly incorporates the cost of selection as a primary decision variable. The operative question, therefore, shifts from gap width alone to clinically relevant motion and preservation of posterior competence. In doing so, this approach aims to reduce both undertreatment and overtreatment and to improve the consistency and defensibility of definitive fixation strategies across diverse practice environments.
- 1,459 View
- 35 Download
Original Articles
- Reverse V step-cut osteotomy for the correction of cubitus varus in adults: a retrospective study
- Jinyoung Bang, Hyung Jun Koo
- J Musculoskelet Trauma 2025;38(2):102-108. Published online April 25, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00045

-
Abstract
PDF
- Background
Cubitus varus deformity in adults most commonly occurs as a late complication resulting from malunion of distal humeral fractures sustained during childhood. This deformity can cause cosmetic problems and anatomical deformities that hinder normal sports activities and potentially lead to long-term complications. Although various surgical techniques exist for correcting cubitus varus, this study investigated the clinical and functional outcomes of reverse V step-cut osteotomy.
Methods
In total, 15 patients underwent surgical treatment with reverse V step-cut osteotomy between 2012 and 2023. The mean age of the patients at the time of surgery was 46.3 years (range, 20–65 years). The preoperative carrying angle was ‒11.09° of varus, which was corrected to +12.81° of valgus postoperatively. The mean preoperative lateral prominence index (LPI) was ‒10.03, and the mean postoperative LPI improved to ‒4.48. A comparison to the unaffected side showed a P-value of 0.978, indicating similarity.
Results
Preoperatively, eight patients exhibited signs of posterolateral rotatory instability, and among them, three underwent concomitant lateral ulnar collateral ligament reconstruction. Seven patients reported ulnar nerve symptoms, and all underwent concurrent ulnar nerve release. Postoperatively, improvements in elbow pain, instability, and ulnar nerve symptoms were observed. One patient required reoperation due to malunion and insufficient correction, but no other complications were noted.
Conclusions
These outcomes demonstrate that reverse V step-cut osteotomy can be an effective treatment method for cubitus varus deformity in adults. Level of evidence: IV.
- 3,898 View
- 93 Download
- Effect of Fracture Gap on Biomechanical Stability of Compression Bone-Plate Fixation System after Bone Fracture Augmentation
- Duk Young Jung, Sung Jae Lee, Seon Chil Kim, Jong Keon Oh
- J Korean Fract Soc 2010;23(2):220-226. Published online April 30, 2010
- DOI: https://doi.org/10.12671/jkfs.2010.23.2.220
-
Abstract
PDF
- PURPOSE
The goal of this study using the biomechanical test was to evaluate the mechanical stability of the bone-plate fixation system according to changes of the fracture gap sizes and widths.
MATERIALS AND METHODS
For mechanical test, four types with different fracture models simulating the clinical situations were constructed depending on the gap size (FGS, mm) and the gap width (FGW, %) at the fracture site: 0 mm/0%, 1 mm/100%, 4 mm/100%, 4 mm/50%. For analyzing the effects of fracture gap on the biomechanical stability of the bone-plate fixation system, 4-point bending test was performed under all same conditions.
RESULTS
It was found that the fracture gap sizes of 1 and 4 mm decreased mechanical stiffness by about 50~60% or more. Furthermore, even without fracture gap size, 50% or more fracture gap width considerably decreased mechanical stiffness and suggested the possibility of plate damage through strain results.
CONCLUSION
Our findings suggested that at least 50% contact of the fracture faces in a fracture surgery would be maintained to increase the mechanical stability of the bone-plate fixation system.
- 1,235 View
- 5 Download
- A Finite Element Analysis of Biomechanical Stability of Compression Plate Fixation System in according to Existing of Fracture Gap after Bone Fracture Augmentation
- Duk Young Jung, Bong Ju Kim, Jong Keon Oh
- J Korean Fract Soc 2010;23(1):83-89. Published online January 31, 2010
- DOI: https://doi.org/10.12671/jkfs.2010.23.1.83
-
Abstract
PDF
- PURPOSE
This study using the finite element analysis (FEA) focused on evaluating the biomechanical stability of the LC-DCP in accordance with existing of the fracture gap at the facture site after bone fracture augmentation.
MATERIALS AND METHODS
For FEM analysis, total eleven types with different fracture models considering clinical fracture cases were constructed according to the fracture gap sizes (0, 1, 4 mm)/widths (0, 25, 50, 75, 100%). Limited contact dynamic compression plate (LC-DCP) fixation system was used in this FEM analysis, and three types of load were applied to the bone-plate fixation system: compressive, torsional, bending load.
RESULTS
The results in FEM analysis showed that the 1, 4 mm fracture gap sizes and 75% or more fracture gap widths increased considerably the peak von Mises stress (PVMS) both the plate and the screw under all loading conditions. PVMS were concentrated on the center of the LC-DCP bone-plate, and around the necks of screws.
CONCLUSION
Based on the our findings, we recommend at least 50% contact of the fracture faces in a fracture surgery using the compression bone-plate system. Moreover, if x-ray observation after surgery finds 100% fracture gap or 50% or more fracture gap width, supplementary measures to improve biomechanical stability must be taken, such as restriction of walking of the patient or plastering. -
Citations
Citations to this article as recorded by
- Application of Patient-Specific 3D-Printed Orthopedic Splint for Bone Fracture in Small Breed Dogs
Kwangsik Jang, Eun Joo Jang, Yo Han Min, Kyung Mi Shim, Chunsik Bae, Seong Soo Kang, Se Eun Kim
Journal of Veterinary Clinics.2023; 40(4): 268. CrossRef
- Application of Patient-Specific 3D-Printed Orthopedic Splint for Bone Fracture in Small Breed Dogs
- 1,126 View
- 3 Download
- 1 Crossref
- Result of Early Active Range of Motion Exercise after Bankart Repair of Traumatic Anterior Instability
- Haeng Kee Noh, Jong Woong Park, Jung Il Lee, Jung Ho Park
- J Korean Fract Soc 2007;20(1):53-57. Published online January 31, 2007
- DOI: https://doi.org/10.12671/jkfs.2007.20.1.53
-
Abstract
PDF
- PURPOSE
To evaluate prospectively the results of early active exercise after open Bankart repair of traumatic anterior shoulder instability.
MATERIALS AND METHODS
From January, 2001 to June, 2003, 26 patients who were followed up at least 1 year after open Bankart repair for traumatic anterior shoulder instability were evaluated. Average age was 23.9 years old (range, 19~43) with 24 males and 2 females. We evaluated them using the functional shoulder scores (modified Rowe score, ASES score), range of motion, VAS pain scale, patient's subjective satisfaction and return to unlimited daily living activity.
RESULTS
The shoulder functional scores increased significantly. At last follow up, the final range of motion were flexion in average 5° deficit in comparison to normal side, external rotation in average 10o deficit, and internal rotation in T9. The patient's subjective satisfaction was good in 2l patients (81%). Return to unlimited daily activity was possible in 23 patients (88.5%), and 19 patients (73%) rejoined to sports activity before injury. There were complications including anterior recurrent subluxation in 1 case, weakness of subscapularis muscle in 1 case.
CONCLUSION
In traumatic anterior shoulder instability, early active range of motion exercise after open Bankart repair does not decrease shoulder stability. Early exercise can be useful for returning to previous level of sports activity in young active patients.
- 898 View
- 5 Download
- Instability of Knee Associated with Ipsilateral Femoral and Tibial Shaft Fractures
- Whan Yong Chung, Woo Suk Lee, Woo Sik Kim, Yong Chan Kim, Taek Soo Jeon, Sun Hong Kim, Ji Hyuk Lim, Young Su Lim
- J Korean Fract Soc 2005;18(2):136-143. Published online April 30, 2005
- DOI: https://doi.org/10.12671/jkfs.2005.18.2.136
-
Abstract
PDF
- PURPOSE
To establish the incidence, type and significance of knee instability in patients with ipsilateral femoral and tibial shaft fracture, comparing with the patients with femoral shaft or tibial shaft fracture alone.
MATERIALS AND METHODS
Two hundreds and seventy-nine consecutive patients were retrospectively reviewed from February 2000 to April 2004. They were composed of 80 patients with femoral shaft fracture alone, 176 patients with tibial shaft fracture alone and 23 patient with ipsilateral femoral and tibial shaft fracture. We evaluate the instability of knee based on physical examinations, plain stress films and MRI. We analyze incidence and period to diagnosis of instability, period to complete bony union and Hospital for Special Surgery (HSS) knee score respectively.
RESULTS
There were 6.3% of knee instability in femoral shaft fracture alone, 9.7% in tibial shaft fracture alone and 30.4% in ipsilateral femoral and tibial shaft fracture. The average period to diagnosis of instability, average period to complete bony union and average HSS knee score were 9.2 months, 4.7 months and 65 points in femoral shaft fracture alone, 9.1 months, 4.2 months and 69 points in tibial shaft fracture alone, 8.7 months, 5.3 months (femur), 4.7 months (tibia) and 57 points in ipsilateral femoral and tibial shaft fracture respectively.
CONCLUSION
We should consider MRI to evaluate the knee instability in patient with ipsilateral femoral and tibial shaft fracture at the time of injury and make a plan early about the treatment of knee instability.
- 635 View
- 2 Download
- Assessment of the Stability of the Isolated Lateral Malleolar Fracture
- Woo Chun Lee, Hyun Soo Park, Young Kil Han, Jang Woon Rim, Jong Deuk Rha
- J Korean Soc Fract 1998;11(4):873-879. Published online October 31, 1998
- DOI: https://doi.org/10.12671/jksf.1998.11.4.873
-
Abstract
PDF
- Recent advances in the understnading of the biomechanics of the ankle have given rise to the clinical uncertainty about the indications for the operative treament of isolated fractures of the lateral malleolus. If deltoid ligament injury is associated, it may be unstable and operation may be indicated. This study was done to determine if we are able to assess the stability of the isolated lateral malleolus fracture based on the fracture patterns seen on radiographs and clinical findings. 37 patients with malleolar fracture of the ankle were treated at Hanil General Hospital by open reduction and internal fixation from Dec. 1996 to Jan. 1998. Lauge-Hansen classification was tried in all cases to determine if it could be applied. Stress test under anesthesia on 10 isolated lateral malleolar fracture patients with clinical findings of injury on the deltoid ligament area, whose medial clear space were normal or widened less than 2 mm on initial film. Exploration of the deltoid ligament was performed in 6 of above 10 patients There were 21 supination-external rotation type injuries, 2 supination-adduction injuries, 1 pronation-abduction injury and 13 fractures could not be clearly categorized into specific group. In 6 among 13 unclear cases, there were short oblique fracture lime indicating pronation injury, but direction of the fracture line could not be clearly determined. In 4 cases, direction of the fracture lime indicated pronation injury, but the length of the fracture line was too long. In 3 cases, both the direction and length of the fracture line was indeterminate. The stress test on 10 isolated lateral malleolar fraactures with clinical findings of deltoid injury revealed less than 2 mm widening in 7 cases, more than 2 mm widening in 3 cases. In 3 cases with less than 2 mm widening, tearing of anterior third of superficial deltoid was confirmed by exploration. In 3 cases with more than 3 mm widening, partial rupture of the deep deltoid was observed in 2 cases and anterior third of superficial deltoid was torn in 1 case. We suggest that we cannot clearly assess the stability of isolated lateral malleolar fracture either by fracture patterns or clinical findings, so stress test can be considered in determining the stability.
- 676 View
- 0 Download
- Biomechanical Evaluation on Hooks Pattern of the Posterior Constructs in an Unstable Burst Fracture Model
- Jae Won You, Tae Hong Lim
- J Korean Soc Fract 1998;11(2):337-344. Published online April 30, 1998
- DOI: https://doi.org/10.12671/jksf.1998.11.2.337
-
Abstract
PDF
- We prefer the posterior instrumentation system for the surgical treatment of the unstable burst fractures of the thoracolumbar spine. We are usually using a hooks pattern with posterior instrumentation, when we can not use a pedicle screw instrumentation in the case of an one stage operation of anterior decompression and posterior stabilization or injury of osteoporotic spine. The purpose of this study was designed to compare biomechanical flexibilities of posterior instrumentation constructs provided by hooks pattern in an unstable calf spine model. Ten fresh frozen calf spines (T10-L4) were used for this study with an anterior and middle column defect and loaded with pure unconstrained moments in flexion, extension, axial rotation, and lateral bending directions. Testing was performed on intact specimens first and then each specimens after laminar hooks insertion and ISOLA posterior implants and any kind of graft materials or transfixation devices were not used to make the worst possible case of instability of an injured spine. Three different fixation methods were instrumented. These included: (1) 2 hooks 2 levels above and 2 levels below corpectomy site in distraction modes bilaterally, (2) 2 levels above and 2 levels below hooks with one rod in distraction and the another rod in compression modes, (3) 2 levels above and 2 levels below hooks with claw hook configuration bilaterally. The results were as follows; 1. At the level of corpectomy site, the group I significantly reduced the motion in flexion and lateral bending (p<0.001), but not in extension as compared to the intact specimen. The group I provided significantly less stabilization than other fixation methods in all motions (p<0.01). The group II and III significantly reduced the motions in flexion, extension, and lateral bending as compared to the intact specimen (p<0.001). Axial rotational motions of all fixation constructs were significantly larger than the intact specimens (p<0.001), and the group I showed greater axial rotational motion than the groups II and III (p<0.001). 2. At the level below corpectomy site, all fixation methods showed the reduced motion significantly in all loading modes and the stabilization was similar with each other. 3. At the level above corpectomy site, all tested fixation methods did not improve the axial rotational stability beyond the intact case, but reduced flexion, extension, and lateral bending motions significantly(p<0.001). In conclusion, the hooks pattern construct in distraction modes is least stable at the corpectomy and above corpectomy sites. It was showed similar stabilizing effect between the claw and compression-distraction configuration. when using hooks, the hooks should be placed in either the claw or compression-distraction configuration.
- 499 View
- 0 Download
- Surgical Treatment of Avulsion Fracture of the Fibular Head Associated with Lateral Instability of the Knee
- Min Young Chung, Won Suck Lee, Soo Myung Lee, Won Cheul Song, Chang Woo Kim, Kwang Min Jung
- J Korean Soc Fract 1997;10(3):597-603. Published online July 31, 1997
- DOI: https://doi.org/10.12671/jksf.1997.10.3.597
-
Abstract
PDF
- Though avulsion fracture of the fibular head rarely occurs, it frequently associates with lateral compartment injury of the knee which resulls in lateral instability. Some authors preferred to internally fixing avulsion fracture of the fibular head to prevent and restore lateral instability of the knee. Our purpose was to suggest that lateral instability of the knee be restored by internal fixation of the fibular head in these cases. We reviewed 6 cases of avulsion fracture of the fibular head associated with lateral instability of the knee which were treated surgically from January, 1993 to December, 1994 with average 2-year-over follow-up. We evaluated each cases using the Knee Ligament Standard Evaluation Form proposed by International Knee Documentation Committee. The results were as follows. The average displacement of the fibular head was 8.4mm. The activity level and overall grade were A(normal) in 4 cases, B(nearly normal) in 1 case, D(severe abnormal) in 1 case. Lateral instability of the knee was satisfactorily restored by internal fixation of the fibular head and repair of ligamentous injuries in cases of avulsion fracture of the fibular head associated with lateral instability of the knee.
-
Citations
Citations to this article as recorded by- Establishment of Classification of Tibial Plateau Fracture Associated with Proximal Fibular Fracture
Zhan‐le Zheng, Yi‐yang Yu, Heng‐rui Chang, Huan Liu, Hui‐lin Zhou, Ying‐ze Zhang
Orthopaedic Surgery.2019; 11(1): 97. CrossRef
- Establishment of Classification of Tibial Plateau Fracture Associated with Proximal Fibular Fracture
- 1,058 View
- 11 Download
- 1 Crossref
- Effect of Unreduced Lesser Trochanteric Fracture on Stability in Intertrochanteric Fracture of Femur
- Seung Woo Suh, Jeong Ho Park, Jong Kun Oh, Kyung Wook Nah, Tae Hyeon Kim, Woo Nam Moon
- J Korean Soc Fract 1997;10(3):529-533. Published online July 31, 1997
- DOI: https://doi.org/10.12671/jksf.1997.10.3.529
-
Abstract
PDF
- Unstable intertrochanteric hip fractures are characterized by comminution of the posteromedial cortex, resulting in a fragment of variable size containing the lesser trochanter. Stability can be provided by transfixion of the lesser trochanteric fracture fragment with a screw. However, fixation of lesser trochanteric fragment is difficult, time-consuming, and often unsuccessful. Controversy exists as to whether it is necessary to perform reduction and fixation of this fragment. A radiological review of 61 intertrochanteric fractures treated with compression screw was made to study the effect of unreduced lesser trochanteric fracture on fracture healing and stability in unstable intertrochanteric fractures accompanied by lessor trochanteric fracture. Analysis were made on terms of rate of bone union, maintenance of reduction by comparing between anatomically reduced group with/without lesser trochanteric fracture and malreduced group with lesser trochanteric fracture. Anatomically reduced groups with/without lessel trochanteric fracture showed similar rates of bone union(88.3% in average) and degree of sliding of lag screw(3.74mm in average) regardless of fixation of lesser trochanter. On the other hand, unreduced group had 33.3% of bone union rates and 9.80mm of sliding of lag screw representing importance of anatomical reduction rather than fixation of lesser trochanteric fracture. In conclusion, it is suggested that unstable intertrochanteric fractures accompanied by large lesser trochanteric fracture fragment can be treated without fixation of lesser trochanteric fragment avoiding major complicatioins such as loosening of implant or collapse of fracture fragment.
- 655 View
- 2 Download
- Clinical Application of Halo-Vest Apparatus in Cervical Spine Lesions
- Yung Tae Kim, Yong Jung Kim, Ho Seung Lee
- J Korean Soc Fract 1995;8(1):262-268. Published online January 31, 1995
- DOI: https://doi.org/10.12671/jksf.1995.8.1.262
-
Abstract
PDF
- Halo-vest apparatus has the mechanical advantages that provides immediate cervical stabilization and can afford the diagnostic work-up for the acute cervical spine injuried patients, and does not interfere with MRI test. Furthermore, we can take the reduction of the dislocation by controlling it in any plane. Especially it is effective in conseuative treatment in upper cervical lesion without neurologic deficit or patient with high risk of operation. We put on the Halo-vest apparatus in seventeen patients with cervical spine lesion. There were fifteen cases of fracture-dislocation, one case of pathologic fracture, and one case of tuberculous spondylitis. The lesion site were upper ceuical in ten cases and others were lower cervical lesion. Three cases were undergone surgical intervention and were fixed with Halo-vest apparstus for further stabilization. We could get the external fixation for the unstable cervical lesion after several segment fusion. Initial immobilization were undertaken with Gardner well tong, Halter or Halo treation for 1.6 weeks in average. They were changed to Halo-vest apparatus for further immobilization and concomitant ambulation. Halo-vest apparatus were put on for 10.2 weeks to get solid bony union. After then other conventional brace were worn such as neck collar,S.0.M.I., four-poster or Philadelphia brace. The complications were one case of pin loosening, and three cases of pin tract infection.
- 678 View
- 1 Download
 First
First Prev
Prev

