 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Review Article
- Combined acetabular and pelvic ring injuries: a reference-frame algorithm for definitive fixation sequencing
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(2):83-92. Published online April 9, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00031
-
 Abstract
Abstract
 PDF
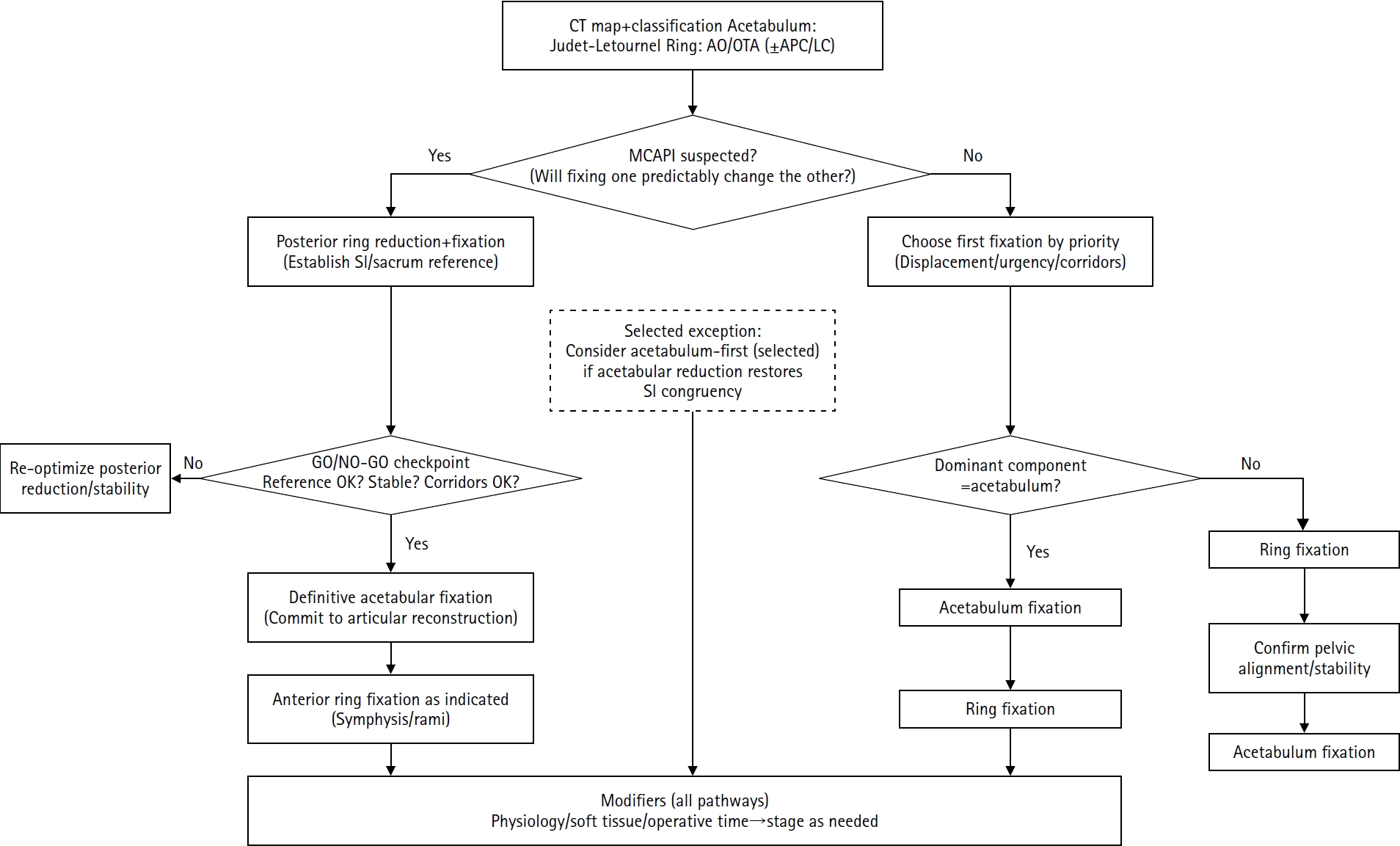
PDF - Combined acetabular and pelvic ring injuries are not simply “two fractures in one patient.” Reduction and fixation of one component can alter the alignment and reducibility of the other, rendering operative sequencing a primary decision variable rather than a secondary consideration. These injuries typically result from high-energy trauma, frequently occur in patients with polytrauma, and are further influenced by physiological tolerance and the feasibility of available operative corridors. The existing evidence base remains constrained by retrospective study designs, inconsistent definitions, variable classification systems, and heterogeneous outcome reporting, all of which limit the strength of comparative recommendations. This state-of-the-art review presents a surgeon-facing, algorithmic approach grounded in a reference-frame mindset. We emphasize computed tomography (CT)-based mapping and the use of consistent terminology to characterize acetabular morphology, pelvic ring instability, deformity vectors, suspicion of mechanical coupling, and feasible operative corridors. Mechanically connected acetabular and pelvic ring injuries (MCAPI) are introduced as a working framework for identifying patterns in which reduction or fixation of one injury predictably influences the other. In cases of suspected MCAPI, a posterior ring-based sequence is generally preferred, typically consisting of posterior ring reduction and fixation, definitive acetabular reconstruction, and subsequent anterior ring fixation. We propose an explicit intraoperative “GO/NO-GO” checkpoint (reference acceptable, stable, corridors feasible) to prevent acetabular reconstruction on a moving target. Acetabulum-first strategies may be appropriate only in selected anteroposterior compression- type configurations in which acetabular fixation plausibly restores sacroiliac congruency and posterior stabilization remains technically feasible. We summarize key outcome domains and complication patterns, highlighting hip dislocation as an important risk factor associated with both neurologic deficits and overall complications. Standardized CTbased definitions and outcome instruments, together with multicenter cohorts employing predefined decision pathways, are required to test sequencing strategies and to determine whether improved radiographic reduction translates into durable functional benefit.
- 2,598 View
- 37 Download

Case Reports
- Latent Superior Gluteal Artery Injury by Entrapment between the Fragments in Transverse Acetabular Fracture - A Case Report -
- Hyuk Jin Choi, Byung Chul Kim, Hoon Kwon, Jae Hoon Jang
- J Korean Fract Soc 2021;34(1):30-33. Published online January 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.1.30
-
Abstract
PDF
- The superior gluteal artery is branched from the internal iliac artery and is located outside the pelvis through a greater sciatic notch. This anatomical characteristic makes the artery vulnerable to injury when pelvic fracture involves the sciatic notch. In the case of a superior gluteal artery injury, hemodynamic instability can occur, and appropriate evaluation and management are mandatory in the acute phase. On the other hand, if the initial detection of the injury is neglected due to a masked pattern, it can cause massive bleeding during surgery, resulting in difficult hemostasis. This paper reports an experience of a latent superior gluteal artery injury by entrapment between the fragments of a transverse acetabular fracture.
-
Citations
Citations to this article as recorded by
- Superior gluteal artery injury in pelvic ring injury and acetabular fracture: Single center observational study
Hoon Kwon, Jae Hoon Jang, Nam Hoon Moon, Seung Joon Rhee, Dong Yeon Ryu, Tae Young Ahn
Journal of Orthopaedic Science.2024; 29(6): 1483. CrossRef
- Superior gluteal artery injury in pelvic ring injury and acetabular fracture: Single center observational study
- 1,376 View
- 6 Download
- 1 Crossref
- Sclerotherapy Using Abnobaviscum for the Extensive Recurrent Chronic Morel-Lavallée Lesions - A Case Report -
- Joon-Kuk Kim, Ji-Won Jung, Ki-Chul Park
- J Korean Fract Soc 2020;33(4):222-226. Published online October 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.4.222
-
Abstract
PDF
- The Morel-Lavallée lesion (MLL) is a closed soft-tissue degloving injury, resulting in characteristic hemo-lymphatic fluid collection between the fascia and subcutaneous layers. The MLL was managed routinely with drainage and compression bandages, but sclerotherapy can be used in patients with chronic lesions refractory to first-line therapy. This paper presents a case of extensive recurrent chronic MLL treated with sclerotherapy using Abnobaviscum, which has been used to treat adhesion in malignant pleural effusion.
-
Citations
Citations to this article as recorded by- Seroma prevention with topical Abnobaviscum sclerotherapy following excision of giant cervical lipoma
Jun Ho Choi, Seung Yeon Choi, Jae Ha Hwang, Kwang Seog Kim, Sam Yong Lee
Archives of Craniofacial Surgery.2023; 24(1): 10. CrossRef
- Seroma prevention with topical Abnobaviscum sclerotherapy following excision of giant cervical lipoma
- 1,340 View
- 14 Download
- 1 Crossref
Review Article
- Fixation Options of Unstable Posterior Pelvic Ring Disruption: Ilio-Sacral Screw Fixation, S2AI Fixation, Posterior Tension Band Plate Fixation, and Spino-Pelvic Fixation
- Dong Hee Kim, Jae Hoon Jang, Myungji Shin, Gu Hee Jung
- J Korean Fract Soc 2019;32(4):240-247. Published online October 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.4.240
-
Abstract
PDF
- The fixation methods that can be used for unstable posterior pelvic ring injuries have undergone many innovative changes due to the recent development of surgical and imaging techniques. After understanding the appropriate indications of first and second sacroiliac screw fixation and spinopelvic fixation, innovative methods, including the trans-sacral screw fixation, posterior tension-band plate fixation, and the S2AI screw, would be chosen and applied. Considering the anatomical complexity and proximity to the surrounding vessels and nerves in the posterior fixation, the safe zone according to the fixation options should be well understood in preoperative planning. Moreover, the functional reduction of the posterior pelvic ring through the reduction and fixation of the anterior lesion should be achieved before placing the implant to reduce the number of malposition-related complications.
-
Citations
Citations to this article as recorded by- Clinical Research through Computational Anatomy and Virtual Fixation
Ju Yeong Kim, Dong-Geun Kang, Gu-Hee Jung
Journal of the Korean Orthopaedic Association.2023; 58(4): 299. CrossRef
- Clinical Research through Computational Anatomy and Virtual Fixation
- 1,898 View
- 19 Download
- 1 Crossref
Case Reports
- Bilateral Gluteal Necrosis and Deep Infection after Transarterial Embolization for Pelvic Ring Injury in Patient with Hemodynamic Instability: A Case Report
- Sung Jin Park, Chang Ho Jeon, Nam Hoon Moon, Yong Geon Park, Jae Hoon Jang
- J Korean Fract Soc 2019;32(1):56-60. Published online January 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.1.56
-
Abstract
PDF
- Transarterial embolization is accepted as effective and safe for the acute management in hemodynamically unstable patients with pelvic ring injury. However, transarterial embolization has potential complications, such as gluteal muscle/skin necrosis, deep infection, surgical wound breakdown, and internal organ infarction, which are caused by blocked blood flow to surrounding tissues and organs, and many studies on the complications have been reported. Here, we report an experience of the management of gluteal necrosis and infection that occurred after transarterial embolization, with a review of the relevant literature.
- 1,382 View
- 0 Download
- Spino-Pelvic Fixation in Unstable Sacral Fracture: A Case Report
- Jung Hwan Choi, Kyu Tae Hwang, Seung Gun Lee, Chang Nam Kang
- J Korean Fract Soc 2018;31(4):145-148. Published online October 31, 2018
- DOI: https://doi.org/10.12671/jkfs.2018.31.4.145
-
Abstract
PDF
- A 22-year-old female patient visited the emergency room (ER) after a pedestrian traffic accident in a drunken state. An examination at the ER revealed fractures at the right side of the sacral ala, sacral foramina, left anterior acetabulum, right inferior ramus, and right superior articular process of S1. She underwent spino-pelvic fixation and iliosacral (IS) screw fixation. One year later, bone union was completed and implant removal was performed and the treatment was completed without complications. The authors recommend spino-pelvic fixation and IS screw fixation for unstable sacral fractures as one of the excellent methods for obtaining posterior stability of the pelvis among the various treatments of unstable sacral fractures.
- 633 View
- 5 Download
Review Article
- Pelvis/Acetabular Fractures in the Elderly: When and How to Fix?
- Kyeong Hyeon Park, Chang Wug Oh, Joon Woo Kim
- J Korean Fract Soc 2018;31(3):102-113. Published online July 31, 2018
- DOI: https://doi.org/10.12671/jkfs.2018.31.3.102
-
Abstract
PDF
- Owing to the increase in life expectancy, the incidence of osteoporotic fracture of the pelvis and acetabulum is increasing. Fractures in the elderly population is different from those in younger patients. Pelvic ring and acetabular fractures in geriatric patients are more likely the result of low-energy trauma, but the outcomes are generally poorer than those of the younger population. Multiple management options are available, but no intervention has become the standard of care for these fractures in the elderly. A treatment strategy should be established depending on the state of the individual patient. Regardless of whether nonsurgical or surgical treatment is selected, early ambulation should be considered to avoid the complications associated with prolonged immobilization.
-
Citations
Citations to this article as recorded by- Effect of Korean Medicine Treatments for Pain Reduction in Patients with Hip Fracture : A Retrospective Observational Study
Nam Hoon Kim, Min Seok Oh
Journal of Physiology & Pathology in Korean Medicine.2020; 34(5): 263. CrossRef
- Effect of Korean Medicine Treatments for Pain Reduction in Patients with Hip Fracture : A Retrospective Observational Study
- 982 View
- 7 Download
- 1 Crossref
Original Article
- Surgical Outcome of Posterior Pelvic Fixation Using S1, S2 Screws in Vertically Unstable Pelvic Ring Injury
- Kwang Hee Yeo, Nam Hoon Moon, Jae Min Ahn, Jae Yoon Jeong, Jae Hoon Jang
- J Korean Fract Soc 2018;31(1):9-17. Published online January 31, 2018
- DOI: https://doi.org/10.12671/jkfs.2018.31.1.9
-
Abstract
PDF
- PURPOSE
Iliosacral screw fixation is an effective and less invasive method that is used widely for the definitive treatment of unstable pelvic ring injuries. On the other hand, fixation failures after iliosacral screw fixation have been reported in vertically unstable pelvic ring injuries. This study examined the surgical outcomes of posterior pelvic fixation using S1 and S2 screws in vertically unstable pelvic ring injuries.
MATERIALS AND METHODS
Between January 2011 and April 2016, 17 patients with vertically unstable pelvic ring injuries who met the minimum 1 year follow-up criteria were treated with internal fixation using posterior pelvic S1 and S2 screws. Their mean age was 43.9 years. According to the AO/OTA classification, 10 patients had C1, 6 had C2, and 1 had C3 injuries. Surgical treatments of single or multiple steps, where necessary, were performed by two surgeons. The clinical and radiologic outcomes were assessed retrospectively using radiographs and medical records.
RESULTS
Overall, 16 patients had bone healing without screw loosening; however, one patient could not maintain anterior pelvic fixation because of an open fracture and deep infection in the anterior pelvic ring. Of five patients who complained of neurological symptoms after injury, three had partially recovered from their neurological deficit. At the last follow-up, the clinical outcomes according to the Majeed score were excellent in 5, good in 6, fair in 4, and poor in 2 patients. The postoperative radiologic outcomes by Matta and Tornetta's method were excellent in 5, good in 8, and fair in 4 patients. Malposition of the S2 screw was identified in one case. The mean time to union was 14.6 weeks after surgery.
CONCLUSION
S1 and S2 screw fixation can be an effective treatment option for posterior pelvic stabilization in vertically unstable pelvic ring injuries when considering the surgical outcomes, such as screw loosening and loss of reduction. -
Citations
Citations to this article as recorded by- Fixation Options of Unstable Posterior Pelvic Ring Disruption: Ilio-Sacral Screw Fixation, S2AI Fixation, Posterior Tension Band Plate Fixation, and Spino-Pelvic Fixation
Dong-Hee Kim, Jae Hoon Jang, Myungji Shin, Gu-Hee Jung
Journal of the Korean Fracture Society.2019; 32(4): 240. CrossRef
- Fixation Options of Unstable Posterior Pelvic Ring Disruption: Ilio-Sacral Screw Fixation, S2AI Fixation, Posterior Tension Band Plate Fixation, and Spino-Pelvic Fixation
- 1,038 View
- 3 Download
- 1 Crossref
Case Reports
- Intrapelvic Penetration of Lag Screw in Proximal Femoral Nailing: A Case Report
- Jung Woo Lee, Hong Man Cho, Jae Woong Seo
- J Korean Fract Soc 2017;30(4):203-208. Published online October 31, 2017
- DOI: https://doi.org/10.12671/jkfs.2017.30.4.203
-
Abstract
PDF
- Hip fractures are common among elderly individuals. Internal fixation with the intramedullary system has been widely used to treat intertrochanteric femur fractures. The Gamma 3 nail is a useful device for fixating trochanteric fractures of the proximal femur. We report a rare complication of medial pelvic penetration of the lag screw of a Gamma 3 nail two months after surgery. There was a complete separation between the nail body and lag screw, and the lag screw penetrated through the acetabulum into the pelvis. We report a case of unstable intertrochanteric fracture with intrapelvic penetration after surgical treatment with proximal femoral nailing and a case followed by fatal results.
-
Citations
Citations to this article as recorded by- Medial lag screw migration in an intramedullary nail combination
Zac Dragan, Ryan J Campbell, Terence R Moopanar
BMJ Case Reports.2025; 18(3): e262436. CrossRef - Slipped hip acetabular cortical screw: Laparoscopy to the rescue
Nidhi Paswan, Lovenish Bains, Soukat Ali Khan, Anubhav Vindal, Lalit Maini
Journal of Minimal Access Surgery.2025;[Epub] CrossRef - Endovascular assisted removal of intrapelvic lag screw after intramedullary proximal femoral nail: A case report and literature review
Zakaria Mousati, Mathias Van Den Broek, Joren Callaert, Jan Gielis, Kris Govaers
Trauma Case Reports.2023; 46: 100873. CrossRef - Intrapelvic migration of the lag screw in intramedullary nailing after intertrochanteric fracture fixation: A case report
Aymen Ben Fredj, Hedi Rbai, Fourat Farhat, Marouen Berriri
Clinical Case Reports.2022;[Epub] CrossRef - Intramedullary nailing confers an increased risk of medial migration compared to dynamic hip screw fixation in unstable intertrochanteric hip fractures
Gin Way LAW, Yoke Rung WONG, Antony GARDNER, Yau Hong NG
Injury.2021; 52(11): 3440. CrossRef - Medial migration in cephalomedullary nail fixation of pertrochanteric hip fractures
G. W. Law, Y. R. Wong, A. K-S. Yew, A. C. T. Choh, J. S. B. Koh, T. S. Howe
Bone & Joint Research.2019; 8(7): 313. CrossRef - Intrapelvic Migration of the Lag Screw with Wedge Wing from Dyna Locking Trochanteric Nail: A Case Report and Literature Review
Yong-Woo Kim, Weon-Yoo Kim, Kyong-Jun Kim, Se-Won Lee
Hip & Pelvis.2019; 31(2): 110. CrossRef
- Medial lag screw migration in an intramedullary nail combination
- 2,458 View
- 17 Download
- 7 Crossref
- Surgical Correction and Osteosynthesis for Cranial Displaced Pelvic Nonunion: Technical Note and Two Cases Report Regarding Anterior Correction and Osteosynthesis Following Posterior Release
- Kwang Cheon Choi, Ji Yoon Ha, Weon Yoo Kim
- J Korean Fract Soc 2014;27(2):151-156. Published online April 30, 2014
- DOI: https://doi.org/10.12671/jkfs.2014.27.2.151
-
Abstract
PDF
- Nonunion of an unstable pelvic fracture with cranial displacement pelvic surgery is technically difficult due to a large amount of bleeding and the risk of nerve damage. In addition, surgical correction of leg length discrepancy by reduction of a dislocated sacroiliac joint is in high demand. Nevertheless, when a patient is strongly disabled by a pelvic deformity, surgical correction may be necessary. Two patients with pelvic deformity were treated successfully by surgical correction and osteosynthesis.
- 687 View
- 0 Download
Original Articles
- Neurologic Injury within Pelvic Ring Injuries
- Ji Wan Kim, Dong Hoon Baek, Jae Hyun Kim, Young Chang Kim
- J Korean Fract Soc 2014;27(1):17-22. Published online January 31, 2014
- DOI: https://doi.org/10.12671/jkfs.2014.27.1.17
-
Abstract
PDF
- PURPOSE
To evaluate the incidence of neurologic injury in pelvic ring injuries and to assess the risk factors for neurologic injury related to pelvic fractures.
MATERIALS AND METHODS
Sixty-two patients with the pelvic ring injury were enrolled in the study from March 2010 to May 2013. When the neurologic injury was suspected clinically, the electro-diagnostic tests were performed. Combined injuries, fracture types, and longitudinal displacements were examined for correlations with the neurologic injury.
RESULTS
There were 7 cases of AO/OTA type A, 37 cases of type B, and 18 cases of type C. Among them, 25 patients (40%) had combined spine fractures, and the average of longitudinal displacement was 7 mm (1-50 mm). Of the 62 patients, 13 (21%) had neurologic injury related with pelvic fractures; 5 with lumbosacral plexus injury, 5 with L5 or S1 nerve injury, 2 with obturator nerve injury, and 1 case of lateral femoral cutaneous nerve injury. There were no relationships between the neurologic injuries and fracture types (p=0.192), but the longitudinal displacements of posterior ring and combined spine fractures were related to the neurologic injury within pelvic ring injury (p=0.006, p=0.048).
CONCLUSION
The incidence of neurologic injury in pelvis fracture was 21%. In this study, the longitudinal displacements of posterior ring and combined spine fractures were risk factors for neurological injury in pelvic ring injury. -
Citations
Citations to this article as recorded by- Surgical Outcome of Posterior Pelvic Fixation Using S1, S2 Screws in Vertically Unstable Pelvic Ring Injury
Kwang Hee Yeo, Nam Hoon Moon, Jae Min Ahn, Jae Yoon Jeong, Jae Hoon Jang
Journal of the Korean Fracture Society.2018; 31(1): 9. CrossRef
- Surgical Outcome of Posterior Pelvic Fixation Using S1, S2 Screws in Vertically Unstable Pelvic Ring Injury
- 1,282 View
- 8 Download
- 1 Crossref
- Treatment of Unstable Sacral Fractures Related to Spino-Pelvic Dissociations
- Hong Sik Kim, Jung Hwan Lee, Ki Chul Park, Ye Soo Park
- J Korean Fract Soc 2013;26(3):178-183. Published online July 31, 2013
- DOI: https://doi.org/10.12671/jkfs.2013.26.3.178
-
Abstract
PDF
- PURPOSE
To evaluate the outcomes of surgical treatment modality in unstable sacral fractures combined with spinal and pelvic ring injury depending on the presence of spino-pelvic dissociations.
MATERIALS AND METHODS
The subjects were 16 patients, with unstable sacral fractures combined with spinal and pelvic ring injuries, were operated from July 2004 to January 2011. The patients were divided into 2 groups depending on the presence of spino-pelvic dissociations: those with dissociations were group 1, and those without dissociations were group 2. Group 1 was treated with spino-pelvic fixations using iliac screw, while group 2 was treated with percutaneous iliosacral screw fixations. The availability of the radiological bony union with its application periods, and clinical results using visual analogue scale (VAS) and oswestry disability index (ODI) were evaluated, retrospectively.
RESULTS
Out of 16 patients, 8 patients in group 1 were treated with spino-pelvic fixation using iliac screw, and 8 patients in group 2 were treated with percutaneous iliosacral screw fixation. The mean bony union period was 17.4 weeks in group 1, and 19.6 weeks in group 2. The Mean VAS and ODI scores on the last follow-up were 2.5 points and 15.6 points in group 1, 2 points and 18.8 points in group 2, respectively. Both groups had favorable clinical results at the last follow-up.
CONCLUSION
For surgical treatments of unstable sacral fractures, spino-pelvic fixation using iliac screws is advised for cases with combined spino-pelvic dissociation, while percutaneous iliosacral screw fixation is advised for cases without combined dissociation. -
Citations
Citations to this article as recorded by- Integrative Korean Medicine Treatment for Sacral Fracture: Two Clinical Cases
Yeon Soo Kang, Pil Je Park, So Jeong Kim, Hyun Jin Jang, Min Ju Kim, Hyeon Kyu Choi, Jeong Kyo Jeong, Ju Hyun Jeon, Young Il Kim
Journal of Acupuncture Research.2023; 40(3): 281. CrossRef - Spino-Pelvic Fixation in Unstable Sacral Fracture: A Case Report
Jung-Hwan Choi, Kyu-Tae Hwang, Seung Gun Lee, Chang-Nam Kang
Journal of the Korean Fracture Society.2018; 31(4): 145. CrossRef
- Integrative Korean Medicine Treatment for Sacral Fracture: Two Clinical Cases
- 1,179 View
- 1 Download
- 2 Crossref
- Anatomical Study of Symphysis Pubis Using 3 Dimensional Computed Tomography in Koreans
- Ji Wan Kim, Jung Min Park, Jae Suk Chang
- J Korean Fract Soc 2013;26(1):32-36. Published online January 31, 2013
- DOI: https://doi.org/10.12671/jkfs.2013.26.1.32
-
Abstract
PDF
- PURPOSE
To acquire anatomical data for the normal pelvic bone structure using three-dimensional computed tomography (3D CT) and to propose the most appropriate angle and screw length for safe screw insertion during symphysis pubis plating.
MATERIALS AND METHODS
We performed 3D CT analysis in 52 patients who required plating and selected a medial and lateral insertion point between the symphysis pubis and the pubic tubercle. Using a three-dimensional medical image analysis program, we evaluated the appropriate screw length, sagittal angle, and oblique angle at each point in this cohort.
RESULTS
At the medial point, the sagittal angle was determined to be 49.1degrees with an average screw length of 49.4 mm. At the lateral point, we calculated an average screw length of 49.1 mm, oblique angle of 23.2degrees, and sagittal angle of 45.7degrees. The screw length was longer in men than in women (4.6 mm and 7.3 mm, respectively) at the medial and lateral point.
CONCLUSION
At the symphysis pubis diastasis, we can insert the screw caudally at 49degrees with a minimal length of 37 mm at the medial point. We can insert the screw caudally at 46degrees, medially at 23degrees, with a minimal 34 mm length at the lateral point.
- 1,179 View
- 3 Download
- Operative Treatment of Unstable Pelvic Ring Injury
- Sang Hong Lee, Sang Ho Ha, Young Kwan Lee, Sung Won Cho, Sang Soo Park
- J Korean Fract Soc 2012;25(4):243-249. Published online October 31, 2012
- DOI: https://doi.org/10.12671/jkfs.2012.25.4.243
-
Abstract
PDF
- PURPOSE
To analyze the clinical and radiological results of the different fixation methods according to the type and displacement of unstable pelvic ring injuries.
MATERIALS AND METHODS
Twenty-three patients with unstable pelvic ring injuries from January 2005 to December 2009 were classified according to the AO/OTA classification system. When patients had been diagnosed with unstable pelvic ring injuries with partial instability, they were treated by anterior fixation with a plate and posterior percutaneous iliosacral screw fixation. When patients had been diagnosed with unstable pelvic ring injuries with complete instability, they were treated by open reduction and anterior to posterior fixation with a plate through the ilioinguinal approach. The radiological results were evaluated using Matta and Saucedo's method, and the clinical results were evaluated using Rommens and Hessmann's method.
RESULTS
The outcomes from the radiological evaluation were that the displacement of the posterior pelvic ring were improved by about 6.65 mm in unstable pelvic ring injuries with partial instability. The displacement of the posterior pelvic ring were improved by about 7.8 mm in unstable pelvic ring injuries with complete instability. The clinical results were excellent in 13 cases and good in 6 cases on latest follow-up.
CONCLUSION
Good results can be achieved by selecting the treatment method according to the type of unstable pelvic ring injurie and displacement. -
Citations
Citations to this article as recorded by- Displacement of an anterior pelvic ring fracture after L5, S1, and iliac screw fixation: a case report
Euijin Cho, Joonghyuk Kim, Hyeongyu Lim, Kyeol Han, Yonghun Pee, Junhong Min, Il-Tae Jang, Jeesoo Jang
Journal of Korean Society of Geriatric Neurosurgery.2025; 21(1): 24. CrossRef - Functional outcomes in pelvic fractures and the factors affecting them– A short term, prospective observational study at a tertiary care hospital
Subhajit Ghosh, Sameer Aggarwal, Prasoon Kumar, Vishal Kumar
Journal of Clinical Orthopaedics and Trauma.2019; 10(5): 896. CrossRef - Outcome of Surgical Treatment of AO Type C Pelvic Ring Injury
Do Hyeon Moon, Nam Ki Kim, Jun Sung Won, Jang Seok Choi, Dong Hyun Kim
Hip & Pelvis.2014; 26(4): 269. CrossRef - Minimally Invasive Plate Osteosynthesis for Humeral Proximal or Distal Shaft Fractures Using a 3.5/5.0 Metaphyseal Locking Plate
Hyoung Keun Oh, Suk Kyu Choo, Jung Il Lee, Dong Hyun Seo
Journal of the Korean Fracture Society.2012; 25(4): 305. CrossRef
- Displacement of an anterior pelvic ring fracture after L5, S1, and iliac screw fixation: a case report
- 1,672 View
- 11 Download
- 4 Crossref
- Crescent Fracture-dislocation of Sacroiliac Joint: Affecting Factors of Operative Results
- Hee Soo Kim, Chang Wug Oh, Poong Taek Kim, Young Soo Byun, Joo Woo Kim, Byung Chul Park, Woo Kie Min, Hyun Joo Lee
- J Korean Fract Soc 2009;22(2):71-78. Published online April 30, 2009
- DOI: https://doi.org/10.12671/jkfs.2009.22.2.71
-
Abstract
PDF
- PURPOSE
To assess the affecting factors of results after the operation of Crescent fracture-dislocation in sacro-iliac joint.
MATERIALS AND METHODS
In 19 patients (mean age, 47.4 year-old) of open reduction and internal fixation for Crescent fracture-dislocation, there were seven type I, 9 type II, and 3 type III fractures according to Day's classification. We assessed affecting factors of radiological and functional results, such as patients' ages, surgical approaches, the fixation extent of pelvic ring, and fracture patterns.
RESULTS
Seventeen of 19 cases united at 14.5 weeks in average, and 2 non-unions occurred with the fixation failure of posterior ring. Satisfactory results were 14 and 15 in radiological and functional evaluation, respectively. In complications, three cases of leg length discrepancy were from an imperfect reduction and two fixation failures. Surgical approach did not show any difference of results, but all cases of unsatisfactory reduction occurred from posterior ring fixation through the anterior approach. Fixation of both rings seemed to have satisfactory results, comparing to posterior ring only. Older patients over 60 year-old had more complications and a tendency to show an unsatisfactory result.
CONCLUSION
In operative treatment of Crescent fracture-dislocation of sacro-iliac joint, it is better to fix both anterior and posterior rings. But, caution is needed to prevent complications in old-aged patients. -
Citations
Citations to this article as recorded by
- 2,039 View
- 78 Download
- 2 Crossref
Case Reports
- Vertically Unstable Fracture of the Pelvis Combined with Anterior Dislocation of the Hip Joint: A Case Report
- Kap Jung Kim, Ha Yong Kim, Dae Suk Yang, Won Sik Choy
- J Korean Fract Soc 2007;20(3):272-276. Published online July 31, 2007
- DOI: https://doi.org/10.12671/jkfs.2007.20.3.272
-
Abstract
PDF
- Pelvic fractures result from high energy trauma and often associated with concomitant injuries. But, vertically unstable pelvic fractures combined with anterior dislocation of the hip is far less common. The traumatic dislocation of the hip is a true orthopedic emergency and it should be considered that a femoral head can be exposed to deteriorized vascularity. We report a case of vertically unstable pelvic fractures combined with traumatic anterior dislocation of the hip joint with the review of the literature.
- 774 View
- 1 Download
- Testicular Necrosis after Ilioinguinal Approach for Pelvic Nonunion: A Case Report
- Sang Eun Park, Young Yul Kim, Jong Hun Ji, Chang Whan Han, Weon Yoo Kim
- J Korean Fract Soc 2006;19(4):490-493. Published online October 31, 2006
- DOI: https://doi.org/10.12671/jkfs.2006.19.4.490
-
Abstract
- Pelvic nonunion is very difficult to treat. According to the nonunion site, anterior or posterior surgical approach should be used selectively. And if the nonunion site is located in both anterior and posterior, both anterior and posterior surgical approach should be used. We report a case of testicular necrosis after ilioinguinal approach used as a anterior approach to pelvis to treat pelvic nonunion developed as a result of unstable pelvic ring injury.
-
Citations
Citations to this article as recorded by- Anatomical Study of Symphysis Pubis Using 3 Dimensional Computed Tomography in Koreans
Ji Wan Kim, Jung Min Park, Jae Suk Chang
Journal of the Korean Fracture Society.2013; 26(1): 32. CrossRef
- Anatomical Study of Symphysis Pubis Using 3 Dimensional Computed Tomography in Koreans
- 993 View
- 0 Download
- 1 Crossref
- Complete Rupture of Sciatic Nerve by Protruded Kuncher Nail in Pelvic Bone Fracture: A Case Report
- Yong Sik Kim, Nam Yong Choi, Suk Ku Han
- J Korean Fract Soc 2006;19(4):486-489. Published online October 31, 2006
- DOI: https://doi.org/10.12671/jkfs.2006.19.4.486
-
Abstract
- Rupture of sciatic nerve is a rare injury in minimally displaced pelvic bone fracture. We report one case of complete rupture of sciatic nerve that were resulted from the extremely protruded Kuncher nail inserted before accident and the preexisting heterotopic ossification with a review of the relevant literature.
- 653 View
- 0 Download
Original Articles
- Problems of Anterior External Fixation in Unstable Pelvic Ring Injury
- Jun Dong Chang, Young Jin Seo, Yong Hyuck Choi
- J Korean Fract Soc 2005;18(4):394-398. Published online October 31, 2005
- DOI: https://doi.org/10.12671/jkfs.2005.18.4.394
-
Abstract
PDF
- PURPOSE
To determine the problems of anterior external fixators in unstable pelvic ring injuries.
MATERIALS AND METHODS
We reviewed 25 patients with an unstable pelvic ring injuries who had been treated with only anterior external fixator over one year follow-up. By Tile's classification, type B 14, type C 11 and the radiological results were evaluated preoperation, postoperation and bone union state. The clinical evaluation was done in termas of the residual pain, discrepency in limb length, rotational deformities, gait disturbance, neurologic deficiency.
RESULTS
In 25 patients with an unstable pelvic ring injuries, 18 (72%) patients were reducted and 3 (17%) patients of 25 were reduction failure at last follow up, they were all Tile type C. The residual pain was graded normal 3, mild 11, moderate 10, severe 1 respectively. The cases with discrepency in limb length and gait disturbance were 6 (all type C), 10 (type B 3, type C 7) respectively. The complication were 4 pin site infection, 3 pressure sore and 1 pyogenic hip arthritis.
CONCLUSION
Our results indicate that anterior external fixator should be limited to vitally unstable patients in acute resuscitative phase and cases without vertical displacement. -
Citations
Citations to this article as recorded by- Outcome of Surgical Treatment of AO Type C Pelvic Ring Injury
Do Hyeon Moon, Nam Ki Kim, Jun Sung Won, Jang Seok Choi, Dong Hyun Kim
Hip & Pelvis.2014; 26(4): 269. CrossRef - General Assessment and Initial Management of Polytrauma Patients
Hyoung Keun Oh
Journal of the Korean Fracture Society.2013; 26(3): 230. CrossRef - Damage Control and Provisional Fixation
Hyoung Keun Oh
Journal of the Korean Fracture Society.2010; 23(3): 346. CrossRef
- Outcome of Surgical Treatment of AO Type C Pelvic Ring Injury
- 969 View
- 0 Download
- 3 Crossref
- Surgical Treatment of Unstable Pelvic Bone Fracture Involving Sacroiliac Joint
- Myung Ho Kim, Hee Gon Park, Moon jib Yoo, Jin Woo An
- J Korean Soc Fract 2003;16(4):433-440. Published online October 31, 2003
- DOI: https://doi.org/10.12671/jksf.2003.16.4.433
-
Abstract
PDF
- PURPOSE
To evaluate the results of surgical method using plate and screws in the treatment of unstable pelvic bone fracture involving Sacroiliac Joint.
MATERIALS AND METHOD
Authors reviewed 21 patients treated by surgical method from 1998 to 2002. Mean follow-up period was 15 months (12~24 month). Male were 16 and female were 5. We used plate and screws in 18 cases, just screws in 3 cases. We classified the type of fracture by Tile's classification and evaluated the results with Moon's criteria that based on reduction state in simple x-ray and patient's subjective satisfaction.
RESULTS
We got the bony union in all cases. By Moon's criteria, 10 cases were good, 7 cases were fair and 4 cases were poor. In 17 cases (80.9%), we got the results over fair. Mean weight bearing exercise periods were 6.4 weeks. There were 2 infection and 2 sacroiliac arthritis after operation.
CONCLUSION
As a method of surgical treatment on unstable pelvic bone fracture involving sacroiliac joint, we recommend open reduction and internal fixation with plate and screws and it may has particular advantages in early ambulation and satisfactory functional outcome.
- 778 View
- 1 Download
- Traumatic Bladder Rupture in Pelvic Fracture - Case Report
- Soon yong Kwon, Woung Kyun Woo, Hwa Sung Lee, Jong Chul Kim, Yong Sik Kim
- J Korean Soc Fract 2002;15(1):77-81. Published online January 31, 2002
- DOI: https://doi.org/10.12671/jksf.2002.15.1.77
-
Abstract
PDF
- Pelvic fracture and bladder rupture resulted in bladder wall entrapment in the fracture site of a patient involved in a fall down accident. Although hematuria and bladder rupture are known to occur after fracture of the pelvis, our literature review showed no reports of this type injury or management. Abscess was drainaged and sepsis was managed with fluid and antibiotics treatment. Bladder extravasation was managed with primary repair and surgical extraction of catheter drainage. We report a case of a patient who presented with traumatic bladder rupture in pelvic fracture.
- 703 View
- 2 Download
- Pelvic Bone Fractures in Children
- Byoung Suck Kim, Ye Yeon Won, Weon Ik Lee, Myeong Ryeol Song, Jae In Ahn
- J Korean Soc Fract 1998;11(1):107-114. Published online January 31, 1998
- DOI: https://doi.org/10.12671/jksf.1998.11.1.107
-
Abstract
PDF
- The pelvic bone fractures in children were uncommon, except for avulsion injuries in the literature and authors had 21 cases of children's pelvic bone fracture, ranging from 1 to 15 years. The mode of injury, type of fracture, associated injuries, morbidity and mortality, and out-come were retrospectively analyzed. The majority of injuries were from automobile-pedestrian collisions (81.0%). the Torode and Zieg type IV injury had the greatest morbidity, mortality, and complications. sixteen patients had non-orthopedic, associated injuries and fourteen required blood transfusions within initial 48 hours after injury. Two of them passed away due to hematologic unstableness. Twenty patients were managed by conservative method, except for one operative case by using of an external fixation device. This study included only 13 cases had average 1 year of follow-up. One acetabular dysplasia of 5 acetabular fractures was found at 12 months after injury. The nonoperative approach for the pelvic bone injury has had a satisfactory outcome in our hospital. so, authors think that if conservative methods will be properly applied, it may be one of the methods of treatment for the children's pelvic bone fracture. Even though there is no symptoms, long-term follow-up will be inevitable for checking more severe acetabular dysplasia and leg length discrepancy.
- 713 View
- 0 Download
- Operative treatment of the Unstable Pelvic Bone Fracture
- Byung Woo Min, Kwang Soon Song, Chul Hyung Kang, Young Soo Kim
- J Korean Soc Fract 1996;9(3):518-524. Published online July 31, 1996
- DOI: https://doi.org/10.12671/jksf.1996.9.3.518
-
Abstract
PDF
- Unstable pelvic bone fracture caused by high-energy trauma that can result in life-threatening situations in which intrapelvic hemorrhage and neurovascular injury. Long-term complications are frequently present, such as leg length discrepancy, gait disturbance and chronic low-back pain. Recently it is principle that it is mandatory to restore the anatomy of pelvic ring structure and to fixistably by means of internal fixation or extemal fixation for successful outcome after unstable pelvicring injury. 26 cases of unstable pelvic bone fracture were treated operatively at the authors hospital between 1992 and 1994. We analyse the clinical and the radiological result. The following results were obtained. 1. The incidence of the unstable pelvic bone fracture was 26 cases(18.4%) of all pelvic bone fractures(141 cases). 2. By the classification of modified Tile, type B1 were 8 cases, type B2(3 cases). type C1(7 cases) and type C3(8 cases). 3. Associated organ injury were found most commonly in the acetabular fracture(8 cases), and other extremity fracture(8 cases), genitourinary system(6 cases) and hemopenitoneum(4 cases). 4. The specific fracture pattern was classified according to various anatomical locations such as transsymphysis(7 cases), transpubic(7 cases), combination of the trassymphysis and traspubic(1 cases), trassacroiliac(7 cases), transiliac(9 cases), transsacral(1 case) and sacroiliac fracture dis location(1 case). 5. According to the fracture location, following methods of stabilization were applied. For the ante rior portion of pelvic ring, plates(13 cases), external fixators(3 cases) and wirings(3 cases) were used. For the posterior portion of pelvic ring, plates(9 cases), percutaneous iliosacral screws(3 cases) and lag screw(1 case) were used. 6. The results revealed as excellent in 20 cases, good in 5 case and fair in 1 case. 7. Postoperative complications were fixation failure(2 cases), metal failure(1 case) and nerve injury(1 case).
-
Citations
Citations to this article as recorded by- Surgical Treatment of Malunion and Nonunion after Pelvic Bone Fracture
Byung-Woo Min, Kyung-Jae Lee
Journal of the Korean Fracture Society.2015; 28(4): 266. CrossRef - Clinical Results of Surgical Treatment of Acetabular Fractures according to Quality of Reduction
Sang-Hong Lee, Min-Kyu Shin, Sueng-Hwan Jo
The Journal of the Korean Orthopaedic Association.2007; 42(2): 153. CrossRef
- Surgical Treatment of Malunion and Nonunion after Pelvic Bone Fracture
- 1,010 View
- 0 Download
- 2 Crossref
- Posterior stabilization of the Unstable Pelvic Ring Fracture
- Soon Taek Jeong, Ji Yeon Kim, Se Hyun Cho
- J Korean Soc Fract 1996;9(3):513-517. Published online July 31, 1996
- DOI: https://doi.org/10.12671/jksf.1996.9.3.513
-
Abstract
PDF
- Stable pelvis fracture is easily treated by conservative treatment with little complication. Unstable pelvic ring fracture, however, is difficult to manage due to various problems. Conservative treatment is rarely indicated because prolonged traction and immobilization often lead to life-threatening complications. The malunion produces pain, limb length discrepancy and eventually poor life quality, Surgical stabilization can help easy care of patients, early mobilization and diminish the morbidity. This study is to present the clinical results of two kinds of metal fixations using seven transiliac bars and four percutaneous sacral screws for the surgical stabilization of the unstable pelvic ring fractures. Total eleven cases had been operated by the authors at Geyong-Sang national hospital from August 1991 to April 1994. They were eight male and three female patients of average forty one years in age(range, eighteen to sixty two years). The average duration of follow-up was thirty one months(range, twenty to fifty three months). All cases of sacral screw fixations revealed satisfactory results both at clinical and radiological aspects. Out of seven cases of transiliac bar fixation, there were two cases of minor infection and three cases of painful and palpable hardware requiring removal, especially in thin patients. The results confirm that sacral screw is better tolerated by thin patients in spite of risk of temporary entrapment of sacral cutaneous nerves.
- 761 View
- 1 Download
 First
First Prev
Prev

