 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 25(4); 2012 > Article
-
Original Article
- Operative Treatment of Unstable Pelvic Ring Injury
- Sang Hong Lee, M.D., Sang Ho Ha, M.D., Young Kwan Lee, M.D., Sung Won Cho, M.D., Sang Soo Park, M.D.
-
Journal of the Korean Fracture Society 2012;25(4):243-249.
DOI: https://doi.org/10.12671/jkfs.2012.25.4.243
Published online: October 19, 2012
Department of Orthopaedic Surgery, School of Medicine, Chosun University, Gwangju, Korea.
- Address reprint requests to: Sang Hong Lee, M.D. Department of Orthopaedic Surgery, Chosun University Hospital, 365, Pilmun-daero, Dong-gu, Gwangju 501-717, Korea. Tel: 82-62-220-3147, Fax: 82-62-226-3379, shalee@chosun.ac.kr
• Received: February 2, 2012 • Revised: March 10, 2012 • Accepted: July 10, 2012
Copyright © 2012 The Korean Fracture Society
- 1,750 Views
- 11 Download
- 4 Crossref
Abstract
-
Purpose
- To analyze the clinical and radiological results of the different fixation methods according to the type and displacement of unstable pelvic ring injuries.
-
Materials and Methods
- Twenty-three patients with unstable pelvic ring injuries from January 2005 to December 2009 were classified according to the AO/OTA classification system. When patients had been diagnosed with unstable pelvic ring injuries with partial instability, they were treated by anterior fixation with a plate and posterior percutaneous iliosacral screw fixation. When patients had been diagnosed with unstable pelvic ring injuries with complete instability, they were treated by open reduction and anterior to posterior fixation with a plate through the ilioinguinal approach. The radiological results were evaluated using Matta and Saucedo's method, and the clinical results were evaluated using Rommens and Hessmann's method.
-
Results
- The outcomes from the radiological evaluation were that the displacement of the posterior pelvic ring were improved by about 6.65 mm in unstable pelvic ring injuries with partial instability. The displacement of the posterior pelvic ring were improved by about 7.8 mm in unstable pelvic ring injuries with complete instability. The clinical results were excellent in 13 cases and good in 6 cases on latest follow-up.
-
Conclusion
- Good results can be achieved by selecting the treatment method according to the type of unstable pelvic ring injurie and displacement.
- 1. Atlihan D, Tekdemir I, Ateŝ Y, Elhan A. Anatomy of the anterior sacroiliac joint with reference to lumbosacral nerves. Clin Orthop Relat Res, 2000;(376):236-241.Article
- 2. Bucholz RW. The pathological anatomy of Malgaigne fracture-dislocations of the pelvis. J Bone Joint Surg Am, 1981;63:400-404.ArticlePubMed
- 3. Bucholz RW, Peters P. Assessment of pelvic stability. Instr Course Lect, 1988;37:119-127.PubMed
- 4. Burgess AR, Eastridge BJ, Young JW, et al. Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma, 1990;30:848-856.PubMed
- 5. Comstock CP, van der Meulen MC, Goodman SB. Biomechanical comparison of posterior internal fixation techniques for unstable pelvic fractures. J Orthop Trauma, 1996;10:517-522.ArticlePubMed
- 6. Griffin DR, Starr AJ, Reinert CM, Jones AL, Whitlock S. Vertically unstable pelvic fractures fixed with percutaneous iliosacral screws: does posterior injury pattern predict fixation failure? J Orthop Trauma, 2006;20:1 Suppl. S30-S36.ArticlePubMed
- 7. Keating JF, Werier J, Blachut P, Broekhuyse H, Meek RN, O'Brien PJ. Early fixation of the vertically unstable pelvis: the role of iliosacral screw fixation of the posterior lesion. J Orthop Trauma, 1999;13:107-113.ArticlePubMed
- 8. Kellam JF, McMurtry RY, Paley D, Tile M. The unstable pelvic fracture. Operative treatment. Orthop Clin North Am, 1987;18:25-41.PubMed
- 9. Kim JJ, Kim JW, Chang JS. Clinical outcome of AO type C pelvic ring injury. J Korean Orthop Assoc, 2005;40:181-187.ArticlePDF
- 10. Kim WY, Ji JH, Kwon OS, Park SE, Kim YY, Moon CY. Comparison with number and position of percutaneous iliosacral screws as treatment of unstable pelvic fracture. J Korean Orthop Assoc, 2009;44:1-7.Article
- 11. Latenser BA, Gentilello LM, Tarver AA, Thalgott JS, Batdorf JW. Improved outcome with early fixation of skeletally unstable pelvic fractures. J Trauma, 1991;31:28-31.Article
- 12. Lee JY, Moon DH, Kim GB. Prognosis of early internal fixation in unstable pelvic fractures. J Korean Soc Fract, 2000;13:741-748.Article
- 13. Matta JM, Saucedo T. Internal fixation of pelvic ring fractures. Clin Orthop Relat Res, 1989;(242):83-97.Article
- 14. Min BW, Jeon SH, Kim TY. Plate fixation for sacroiliac joint separation through the anterior approach. J Korean Orthop Assoc, 2002;37:478-482.ArticlePDF
- 15. Oh CW, Kim PT, Park BC, et al. Anterior plating and ilio-sacral screwing for unstable pelvic injury. J Korean Orthop Assoc, 2007;42:483-489.Article
- 16. Oh JK, Bae SY, Kim JO, Roh KJ, Lee JJ, Chang SY. Radiologic evaluation for the safe zone of percutaneous iliosacral screw fixation. J Korean Soc Fract, 2002;15:336-341.Article
- 17. Pennal GF, Tile M, Waddell JP, Garside H. Pelvic disruption: assessment and classification. Clin Orthop Relat Res, 1980;(151):12-21.Article
- 18. Pohlemann T, Angst M, Schneider E, Ganz R, Tscherne H. Fixation of transforaminal sacrum fractures: a biomechanical study. J Orthop Trauma, 1993;7:107-117.
- 19. Pohlemann T, Bosch U, Gänsslen A, Tscherne H. The Hannover experience in management of pelvic fractures. Clin Orthop Relat Res, 1994;(305):69-80.Article
- 20. Rommens PM, Hessmann MH. Staged reconstruction of pelvic ring disruption: differences in morbidity, mortality, radiologic results, and functional outcomes between B1, B2/B3, and C-type lesions. J Orthop Trauma, 2002;16:92-98.Article
- 21. Routt ML Jr, Kregor PJ, Simonian PT, Mayo KA. Early results of percutaneous iliosacral screws placed with the patient in the supine position. J Orthop Trauma, 1995;9:207-214.Article
- 22. Routt ML Jr, Simonian PT, Agnew SG, Mann FA. Radiographic recognition of the sacral alar slope for optimal placement of iliosacral screws: a cadaveric and clinical study. J Orthop Trauma, 1996;10:171-177.Article
- 23. Routt ML Jr, Simonian PT, Mills WJ. Iliosacral screw fixation: early complications of the percutaneous technique. J Orthop Trauma, 1997;11:584-589.Article
- 24. Simonian PT, Routt ML Jr, Harrington RM, Tencer AF. The unstable iliac fracture: a biomechanical evaluation of internal fixation. Injury, 1997;28:469-475.Article
- 25. Stocks GW, Gabel GT, Noble PC, Hanson GW, Tullos HS. Anterior and posterior internal fixation of vertical shear fractures of the pelvis. J Orthop Res, 1991;9:237-245.Article
- 26. Tile M. Pelvic ring fractures: should they be fixed? J Bone Joint Surg Br, 1988;70:1-12.ArticlePDF
- 27. Tile M. Acute pelvic fractures: I. Causation and classification. J Am Acad Orthop Surg, 1996;4:143-151.Article
- 28. Tile M. Acute pelvic fractures: II. Principles of management. J Am Acad Orthop Surg, 1996;4:152-161.Article
- 29. Tornetta P 3rd, Dickson K, Matta JM. Outcome of rotationally unstable pelvic ring injuries treated operatively. Clin Orthop Relat Res, 1996;(329):147-151.Article
- 30. Tsukushi S, Katagiri H, Nakashima H, Shido Y, Wasa J. Computed tomography-guided screw fixation of a sacroiliac joint dislocation fracture: a case report. J Orthop Sci, 2003;8:729-732.Article
- 31. Ward EF, Tomasin J, Vander Griend RA. Open reduction and internal fixation of vertical shear pelvic fractures. J Trauma, 1987;27:291-295.Article
- 32. Young JW, Burgess AR, Brumback RJ, Poka A. Pelvic fractures: value of plain radiography in early assessment and management. Radiology, 1986;160:445-451.Article
REFERENCES
Fig. 1
(A, B) A 41-year-old male patient who had an unstable pelvic fracture with symphysis pubis diastasis and sacroiliac joint disruption.
(C, D) Plate fixation on symphysis pubis and percutaneous iliosacral screw fixation on sacroiliac joint.
(E) After 30 months, he had a complete union and excellent function.
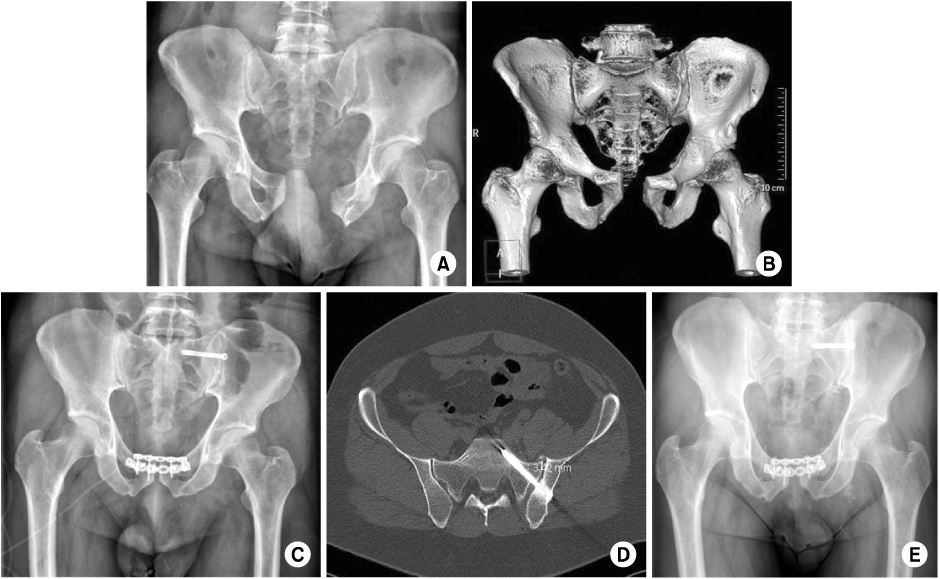
Fig. 2
(A, B) A 65-year-old female patient who had unstable pelvic fracture with superior and inferior ramus fracture and sacroiliac joint disruption.
(C, D) Through the anterior approach, anatomical reconstruction was achieved with the fixation of the anterior and posterior rings.
(E) After 53 months, she had a complete union and excellent function.
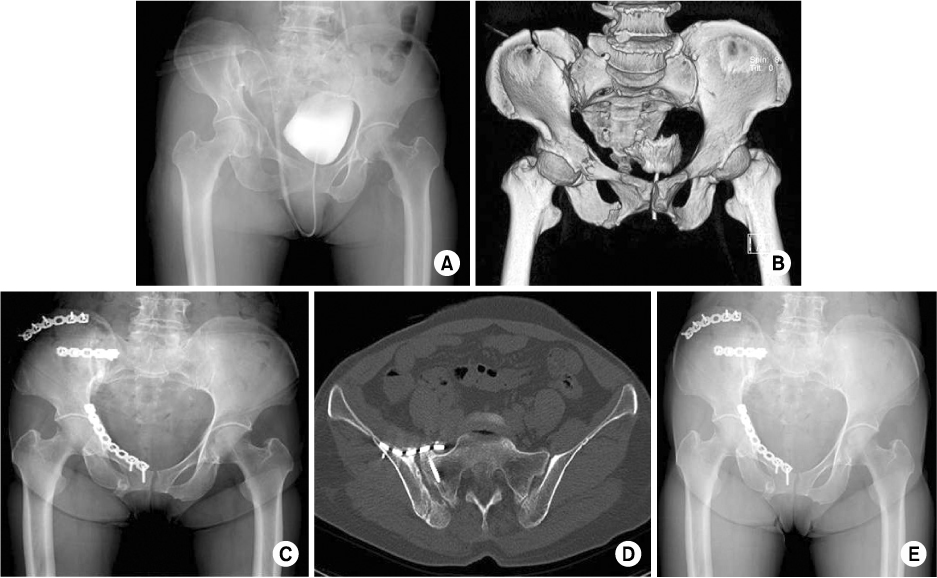
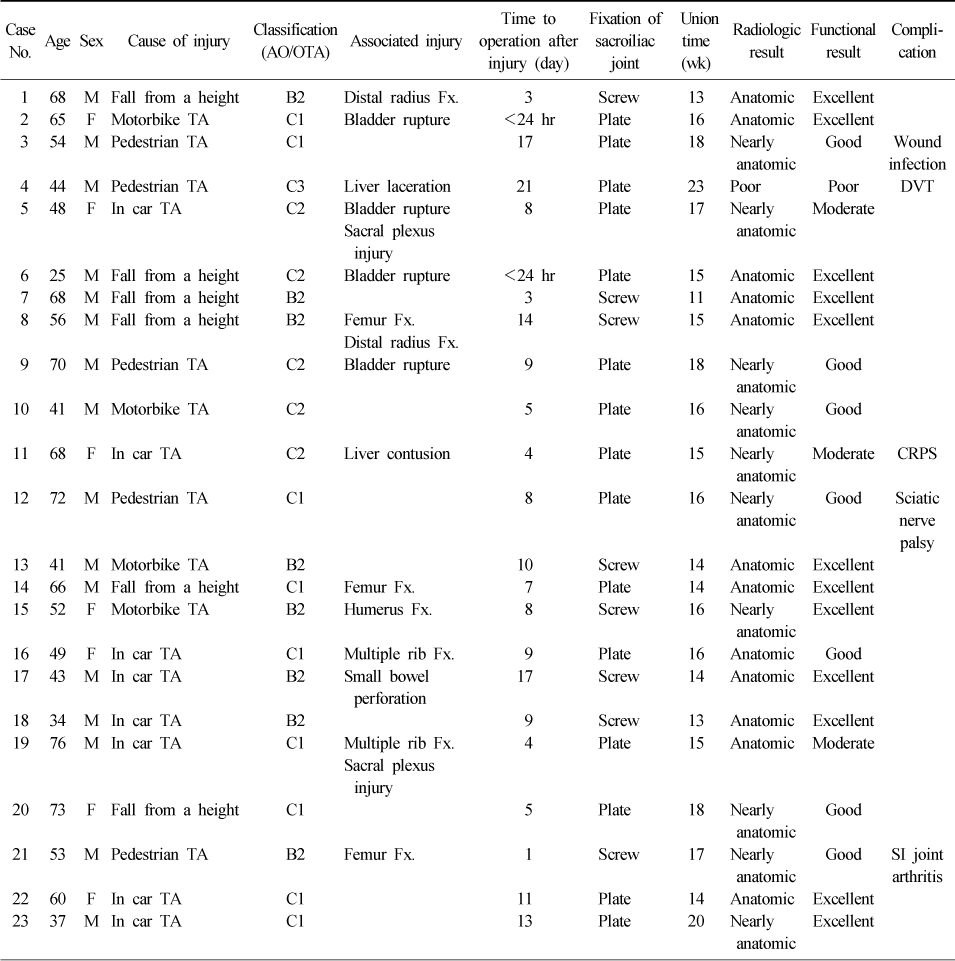
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Displacement of an anterior pelvic ring fracture after L5, S1, and iliac screw fixation: a case report
Euijin Cho, Joonghyuk Kim, Hyeongyu Lim, Kyeol Han, Yonghun Pee, Junhong Min, Il-Tae Jang, Jeesoo Jang
Journal of Korean Society of Geriatric Neurosurgery.2025; 21(1): 24. CrossRef - Functional outcomes in pelvic fractures and the factors affecting them– A short term, prospective observational study at a tertiary care hospital
Subhajit Ghosh, Sameer Aggarwal, Prasoon Kumar, Vishal Kumar
Journal of Clinical Orthopaedics and Trauma.2019; 10(5): 896. CrossRef - Outcome of Surgical Treatment of AO Type C Pelvic Ring Injury
Do Hyeon Moon, Nam Ki Kim, Jun Sung Won, Jang Seok Choi, Dong Hyun Kim
Hip & Pelvis.2014; 26(4): 269. CrossRef - Minimally Invasive Plate Osteosynthesis for Humeral Proximal or Distal Shaft Fractures Using a 3.5/5.0 Metaphyseal Locking Plate
Hyoung Keun Oh, Suk Kyu Choo, Jung Il Lee, Dong Hyun Seo
Journal of the Korean Fracture Society.2012; 25(4): 305. CrossRef
 Cite
CiteOperative Treatment of Unstable Pelvic Ring Injury
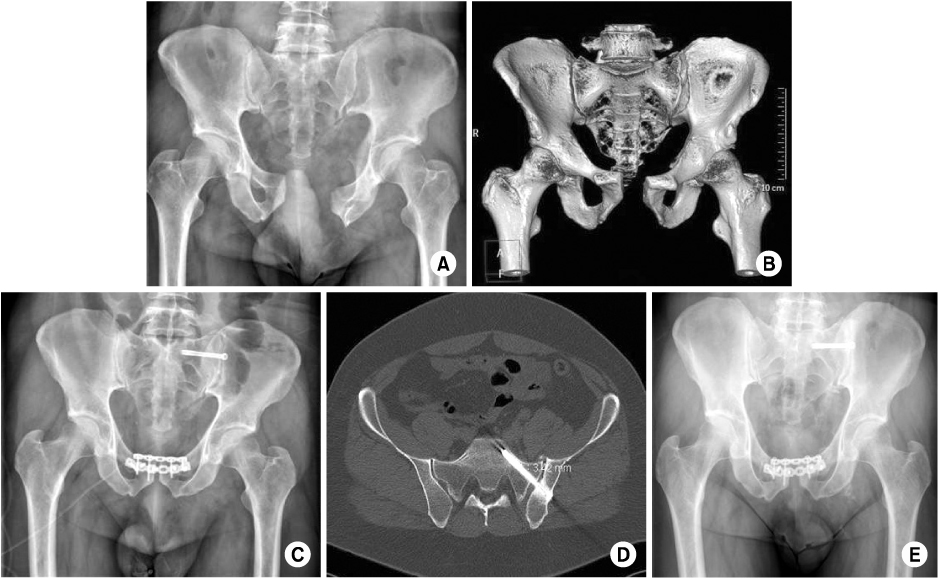
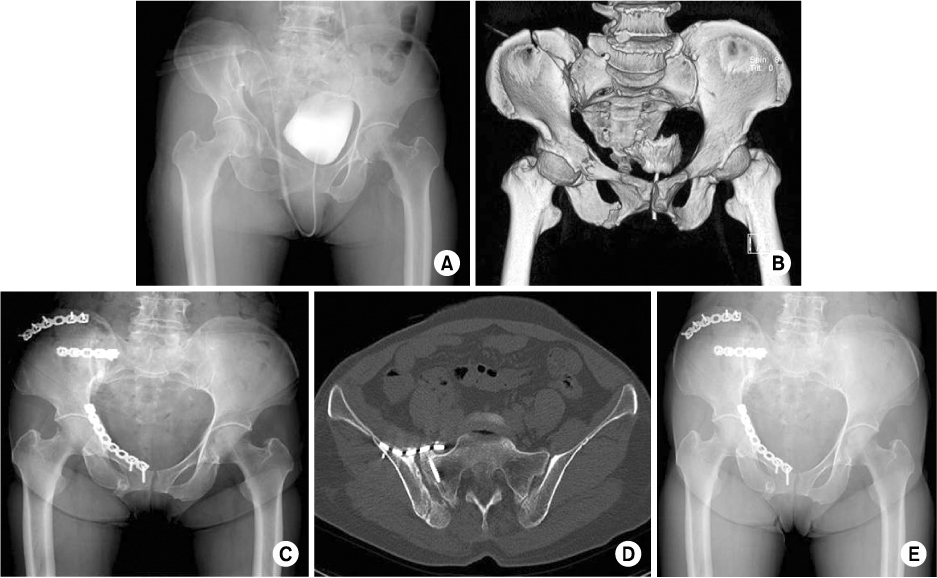
Fig. 1
(A, B) A 41-year-old male patient who had an unstable pelvic fracture with symphysis pubis diastasis and sacroiliac joint disruption.
(C, D) Plate fixation on symphysis pubis and percutaneous iliosacral screw fixation on sacroiliac joint.
(E) After 30 months, he had a complete union and excellent function.
Fig. 2
(A, B) A 65-year-old female patient who had unstable pelvic fracture with superior and inferior ramus fracture and sacroiliac joint disruption.
(C, D) Through the anterior approach, anatomical reconstruction was achieved with the fixation of the anterior and posterior rings.
(E) After 53 months, she had a complete union and excellent function.
Fig. 1
Fig. 2
Operative Treatment of Unstable Pelvic Ring Injury
Patient Data
M: Male, F: Female, TA: Traffic accident, Fx: Fracture, DVT: Deep vein thrombosis, CRPS: Complex regional pain syndrome, SI: Sacro-Iliac.
Table 1
Patient Data
M: Male, F: Female, TA: Traffic accident, Fx: Fracture, DVT: Deep vein thrombosis, CRPS: Complex regional pain syndrome, SI: Sacro-Iliac.

