 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(1); 2011 > Article
-
Original Article
- Antegrade Intramedullary Prebent K-wire Fixation for the 5th Metacarpal Neck Fracture
- Tae-Hyung Kim, M.D., Bo Hyeon Kim, M.D., In-Ho Jung, M.D., Dong-Hyun Kim, M.D.
-
Journal of the Korean Fracture Society 2011;24(1):67-72.
DOI: https://doi.org/10.12671/jkfs.2011.24.1.67
Published online: January 21, 2011
Department of Orthopedic Surgery, Cheongju St. Mary's Hospital, Cheongju, Korea.
*Department of Orthopedic Surgery, The Catholic University of Korea College of Medicine, Seoul, Korea.
- Address reprint requests to: Bo Hyeon Kim, M.D. Department of Orthopedic Surgery, Cheongju St. Mary's Hospital, 589-5, Jujung-dong, Sangdang-gu, Cheongju 360-568, Korea. Tel: 82-43-219-8140·Fax: 82-43-219-8157, ostwins@naver.com
• Received: August 2, 2010 • Revised: September 11, 2010 • Accepted: November 16, 2010
Copyright © 2011 The Korean Fracture Society
- 1,809 Views
- 20 Download
- 1 Crossref
Abstract
-
Purpose
- To evaluate radiological and clinical results of the antegrade intramedullary prebent K-wire fixation for the 5th metacarpal neck fracture.
-
Materials and Methods
- Between January, 2006 and December, 2009, 31 patients with displaced neck fracture of the fifth metacarpal who received antegrade intramedullary prebent K-wire fixation were included in this study. Radiological and clinical outcome evaluations were performed.
-
Results
- All the fractures were completely united. In the oblique radiographs, the average of preoperative angulation was corrected from 38.9° to 4.4°. The average difference between postoperative and final follow-up was 1.2°. Clinical outcomes were satisfactory except for one patient who had sustained ulnar nerve dorsal branch injury during surgery.
-
Conclusion
- Antegrade intramedullary prebent K-wire fixation may be preferentially considered as one of the best ways to fix the displaced neck fractures of the fifth metacarpal.
- 1. Ali A, Hamman J, Mass DP. The biomechanical effects of angulated boxer's fractures. J Hand Surg Am, 1999;24:835-844.ArticlePubMed
- 2. Braakman M, Oderwald EE, Haentjens MH. Functional taping of fractures of the 5th metacarpal results in a quicker recovery. Injury, 1998;29:5-9.ArticlePubMed
- 3. Choi SJ, Chang SK. Teatment method of the metacarpal bone fractures with retrograde percutaneous intramedullary K-wire fixation to decrease the injury of extensor tendon. J Korean Soc Surg Hand, 2004;9:117-122.
- 4. Ford DJ, Ali MS, Steel WM. Fractures of the fifth metacarpal neck: is reduction or immobilisation necessary? J Hand Surg Br, 1989;14:165-167.ArticlePubMedPDF
- 5. Foucher G. "Bouquet" osteosynthesis in metacarpal neck fractures: a series of 66 patients. J Hand Surg Am, 1995;20:S86-S90.ArticlePubMed
- 6. Foucher G, Chemorin C, Sibilly A. A new technic of osteosynthesis in fractures of the distal 3d of the 5th metacarpus. Nouv Presse Med, 1976;5:1139-1140.PubMed
- 7. Hunter JM, Cowen NJ. Fifth metacarpal fractures in a compensation clinic population. A report on one hundred and thirty-three cases. J Bone Joint Surg Am, 1970;52:1159-1165.PubMed
- 8. Jahss SA. Fracture of the metacarpals: a new method of reduction and immobilization. J Bone Joint Surg Am, 1938;20:178-186.
- 9. Kim BS, Cho SD, Cho YS, et al. Operative treatment of metacarpal shaft fracture. J Korean Soc Fract, 1999;12:720-726.Article
- 10. Kim MH, Yoo MJ, Kim JP, Lee JH, Lee JW. Bouquet pin intramedullary nail technique of the 5th metacarpal neck fractures. J Korean Fract Soc, 2007;20:64-69.Article
- 11. Lamraski G, Monsaert A, De Maeseneer M, Haentjens P. Reliability and validity of plain radiographs to assess angulation of small finger metacarpal neck fractures: human cadaveric study. J Orthop Res, 2006;24:37-45.ArticlePubMed
- 12. Leung YL, Beredjiklian PK, Monaghan BA, Bozentka DJ. Radiographic assessment of small finger metacarpal neck fractures. J Hand Surg Am, 2002;27:443-448.ArticlePubMed
- 13. Manueddu CA, Della Santa D. Fasciculated intramedullary pinning of metacarpal fractures. J Hand Surg Br, 1996;21:230-236.ArticlePubMedPDF
- 14. McKerrell J, Bowen V, Johnston G, Zondervan J. Boxer's fractures--conservative or operative management. J Trauma, 1987;27:486-490.ArticlePubMed
- 15. Paul AS, Kurdy N, Kay PR. Fixation of closed metacarpal shaft fractures. Transverse K-wires in 22 cases. Acta Orthop Scand, 1994;65:427-429.ArticlePubMed
- 16. Steel WM. Barton NJ. Articular fractures. In: Fractures of the hand and wrist, 1988;New York, Churchill Livingstone. 55-73.
- 17. Theeuwen GA, Lemmens JA, van Niekerk JL. Conservative treatment of boxer's fracture: a retrospective analysis. Injury, 1991;22:394-396.ArticlePubMed
- 18. Wong TC, Ip FK, Yeung SH. Comparison between percutaneous transverse fixation and intramedullary K-wires in treating closed fractures of the metacarpal neck of the little finger. J Hand Surg Br, 2006;31:61-65.ArticlePubMedPDF
REFERENCES
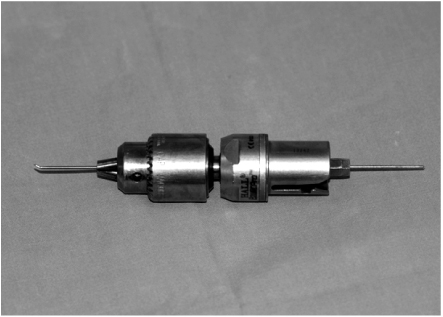
Fig. 2The wire is inserted through the ulnar cortex of the little finger metacarpal base, after 5 mm incision.

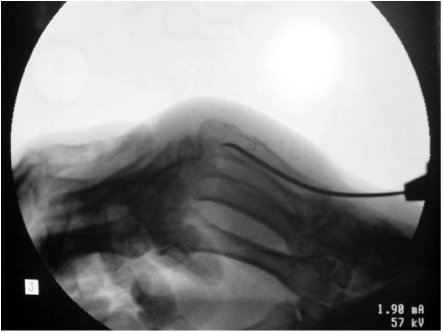
Fig. 4Prebent tip of the wire is secured at the subchondral bone of the metacarpal head after closed reduction under the C-arm.
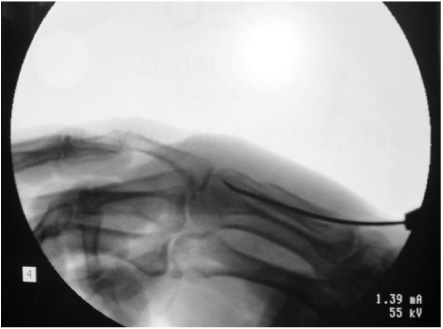
Fig. 5A 46-year old man sustains a 5th metacarpal neck fracture with 35° angulation deformity in oblique radiograph.
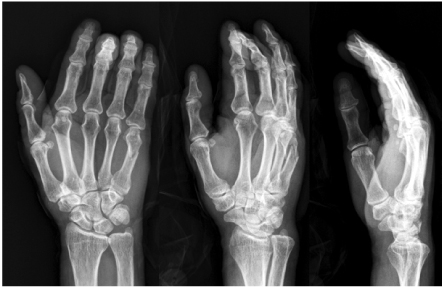


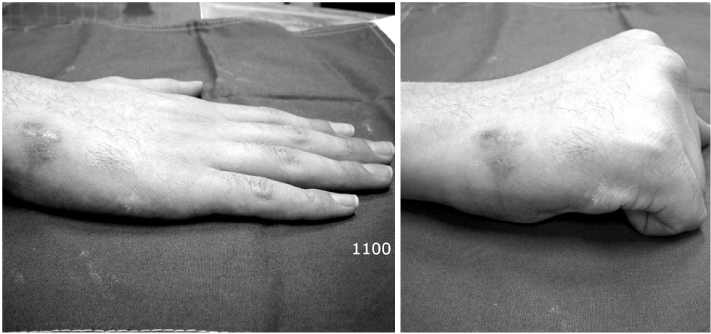


Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Clinical Outcomes of Customized Staple Fixation Using K-wire in Metacarpal Base or Neck Fractures
Hong-ki Jin, Hyoung Min Kim, Yong Seung Oh, Jihoon Kim
Journal of the Korean Fracture Society.2021; 34(1): 23. CrossRef
 Cite
CiteAntegrade Intramedullary Prebent K-wire Fixation for the 5th Metacarpal Neck Fracture
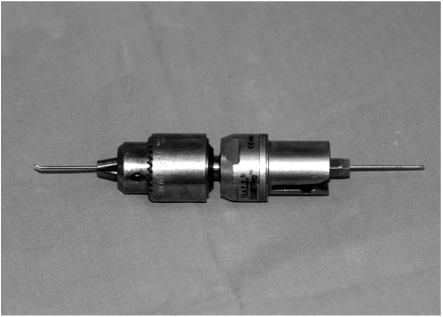
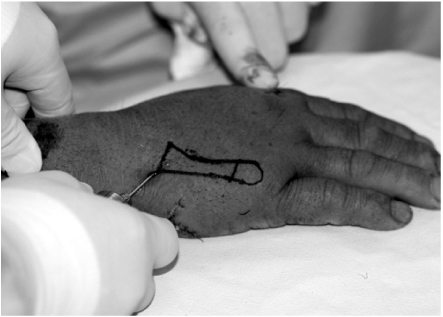
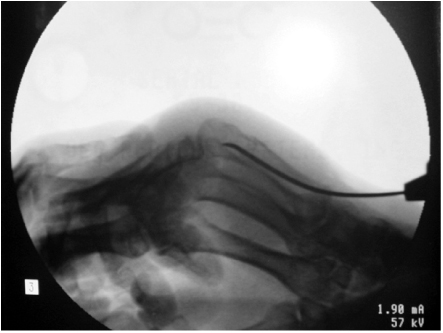
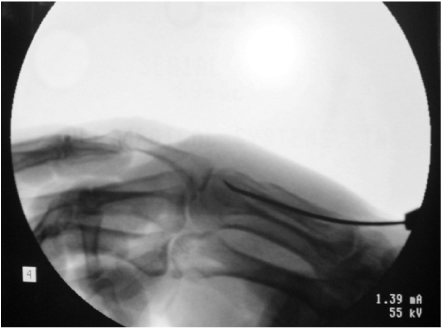
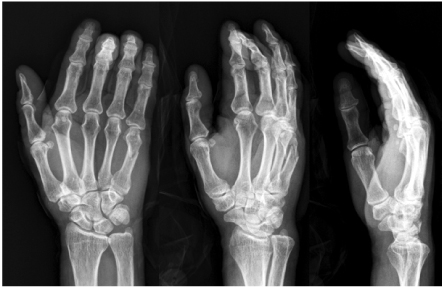




Fig. 1
The prebent wire is firmly fixed to the drill chuck.
Fig. 2
The wire is inserted through the ulnar cortex of the little finger metacarpal base, after 5 mm incision.
Fig. 3
Drive the wire into the fracture site like a guide pin of the interlocking nail system.
Fig. 4
Prebent tip of the wire is secured at the subchondral bone of the metacarpal head after closed reduction under the C-arm.
Fig. 5
A 46-year old man sustains a 5th metacarpal neck fracture with 35° angulation deformity in oblique radiograph.
Fig. 6
Postoperative radiographs show 0° residual angulation after pin fixation.
Fig. 7
Four-month postoperative radiographs show good union without any reduction loss.
Fig. 8
Phoptograhs show full range of motion.
Fig. 9
The height of the K-wire is proportionate to the bending angle. H: Thickness of K-wire+h, b: Length of prebent wire, a: Angle, h: b sin a.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Fig. 9
Antegrade Intramedullary Prebent K-wire Fixation for the 5th Metacarpal Neck Fracture
Table 1
Grading for clinical results
Excellent: 500~476, Good: 475~451, Fair: 450~426, Poor: <425. From Kim et al

