 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(1); 2011 > Article
-
Original Article
- Interposition of Periosteum in Distal Tibial Physeal Fractures of Children
- Phil Hyun Chung, M.D., Suk Kang, M.D., Jong Pil Kim, M.D., Young Sung Kim, M.D., Jae Woo Cho, M.D.
-
Journal of the Korean Fracture Society 2011;24(1):73-78.
DOI: https://doi.org/10.12671/jkfs.2011.24.1.73
Published online: January 21, 2011
Department of Orthopedic Surgery, College of Medicine, Dongguk University, Gyeonju, Korea.
- Address reprint requests to: Young Sung Kim, M.D. Department of Orthopedic Surgery, College of Medicine, Dongguk University, 1090-1, Seokjang-dong, Gyeonju 780-350, Korea. Tel: 82-54-770-8222·Fax: 82-54-770-8378, kys7374@freechal.com
• Received: September 30, 2010 • Accepted: October 27, 2010
Copyright © 2011 The Korean Fracture Society
- 1,123 Views
- 8 Download
Abstract
-
Purpose
- To evaluate the factors influencing periosteal interposition in distal tibial physeal fractures of children.
-
Materials and Methods
- 34 cases of distal tibial physeal fractures were analysed. We confirmed the presence of periosteal interposition with MRI in all cases and accessed the relationship between periosteal interposition and gender, age, cause of injury, type of fracture, degree of initial displacement and after closed reduction.
-
Results
- 9 (26.5%) of 34 fractures had interposed periosteum. There was no statistically significant correlation between periosteal interposition and gender, age, cause of injury (p>0.05). 5 (83.3%) of 6 pronation-eversion-external rotation type of fractures according to Dias-Tachjian classification had interposed periosteum and that was a statistically significant correlation (p=0.006). As Salter-Harris type was toward to high degree, there were decreasing tendency of periosteal interposition (p=0.026). There was high rate of periosteal interposition in case of displacement more than 2 mm in each initial and after closed reduction (p<0.05).
-
Conclusion
- There was high incidence of periosteal interposition in pronation-eversion-external rotation type with displacement more than 2 mm in distal tibial physeal fractures of children. But, periosteal interposition could occur in fractures with mild displacement less than 2 mm, if initial fracture displacement was more than 2 mm, the methods of treatment should be decided after confirm the presence of periosteal interposition with MRI after closed reduction.
- 1. Barmada A, Gaynor T, Mubarak SJ. Premature physeal closure following distal tibia physeal fractures: a new radiographic predictor. J Pediatr Orthop, 2003;23:733-739.
- 2. Cummings RJ. Beaty JH, Kasser JR. Distal tibial and fibular fractures. In: Rockwood and Wilkins' fracture in children, 2006;6th ed. Philadelphia, Lippincott, Williams & Wilkins. 1077-1128.
- 3. Dias LS, Tachdjian MO. Physeal injuries of the ankle in children: classification. Clin Orthop Relat Res, 1978;136:230-233.
- 4. Gruber HE, Phieffer LS, Wattenbarger JM. Physeal fractures, part II: fate of interposed periosteum in a physeal fracture. J Pediatr Orthop, 2002;22:710-716.
- 5. Hahn SH, Yang BK, Yi SR, Yoo SH. Treatment of distal tibial epiphyseal fracture salter-harris type I & II. J Korean Soc Fract, 1999;12:1065-1070.
- 6. Kim JR, Pyo SH, Hwang BY. Results of treatment for epiphyseal injuries of the ankle in children. J Korean Soc Fract, 2000;13:680-685.
- 7. Kim JR, Song KH. Factors influencing premature physeal closure following physeal injury of the ankle in children. J Korean Orthop Assoc, 2008;43:672-676.
- 8. Kim KC, Choi JY, Kim JS, Jhe YS, Yun BC. Treatment of the pediatric ankle fracture. J Korean Soc Fract, 1996;9:341-348.
- 9. Kling TF Jr, Bright RW, Hensinger RN. Distal tibial physeal fractures in children that may require open reduction. J Bone Joint Surg Am, 1984;66:647-657.
- 10. Leary JT, Handling M, Talerico M, Yong L, Bowe JA. Physeal fractures of the distal tibia: predictive factors of premature physeal closure and growth arrest. J Pediatr Orthop, 2009;29:356-361.
- 11. O'Driscoll SW, Keeley FW, Salter RB. The chondrogenic potential of free autogenous periosteal grafts for biological resurfacing of major full-thickness defects in joint surfaces under the influence of continuous passive motion. An experimental investigation in the rabbit. J Bone Joint Surg Am, 1986;68:1017-1035.
- 12. Phieffer LS, Meyer RA Jr, Gruber HE, Easley M, Wattenbarger JM. Effect of interposed periosteum in an animal physeal fracture model. Clin Orthop Relat Res, 2000;376:15-25.
- 13. Rohmiller MT, Gaynor TP, Pawelek J, Mubarak SJ. Salter-Harris I and II fractures of the distal tibia: does mechanism of injury relate to premature physeal closure? J Pediatr Orthop, 2006;26:322-328.
- 14. Salter RB, Harris WR. Injuries involving the epiphyseal plate. J Bone Joint Surg Am, 1963;45:587-622.
- 15. Schurz M, Binder H, Platzer P, Schulz M, Hajdu S, Vécsei V. Physeal injuries of the distal tibia: long-term results in 376 patients. Int Orthop, 2010;34:547-552.
- 16. Spiegel PG, Cooperman DR, Laros GS. Epiphyseal fractures of the distal ends of the tibia and fibula A retrospective study of two hundred and thirty-seven cases in children. J Bone Joint Surg Am, 1978;60:1046-1050.
- 17. Weber BG. Fibrous interposition causing valgus deformity after fracture of the upper tibial metaphysis in children. J Bone Joint Surg Br, 1977;59:290-292.
- 18. Wirth T, Byers S, Byard RW, Hopwood JJ, Foster BK. The implantation of cartilaginous and periosteal tissue into growth plate defects. Int Orthop, 1994;18:220-228.
REFERENCES
Fig. 1
A 7 year-old boy sustained physeal injury of the ankle.
(A) According to the Dias-Dachjian classification, initial radiographs show pronation-eversion-external rotation type of distal tibial physeal fracture.
(B) Post-reduction radiographs demonstrate satisfactory closed reduction. Distal tibia fracture has Thurston-Holland fragment (arrow), it representing Salter-Harris type II injury.
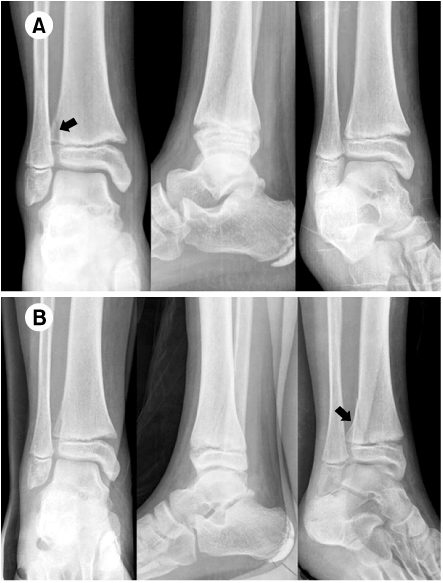
Fig. 2Coronal and sagittal T2W MRI show the interposed periosteum in antero-medial aspect of distal tibial physeal fracture (arrow).

Fig. 3
(A) Intraoperative finding gross photography shows the interposed periosteun.
(B) The probe is inserted into fractured physeal space.
(C) The interposed periosteum was extracted.
(D) The extracted periosteum was repaired with absorbable suture.
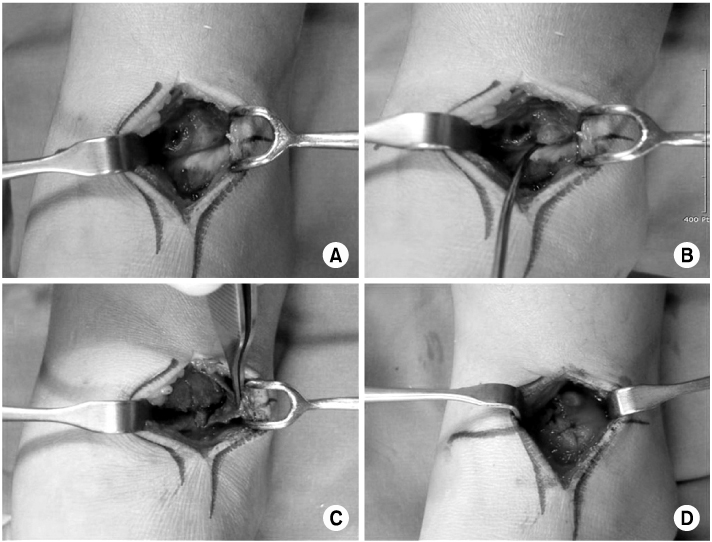
Fig. 4
(A) The distal tibial physeal fracture was fixed with 2 smooth pins.
(B) At postoperative 4 years, the radiographs show no deformity or premature physeal closure.

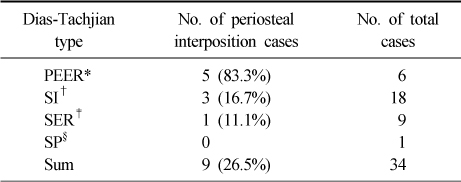
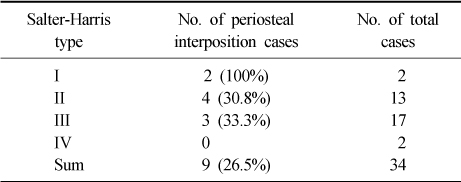
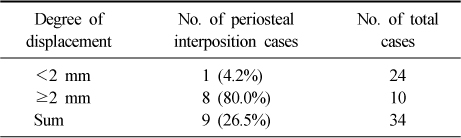
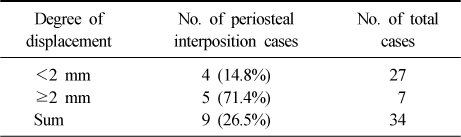
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteInterposition of Periosteum in Distal Tibial Physeal Fractures of Children
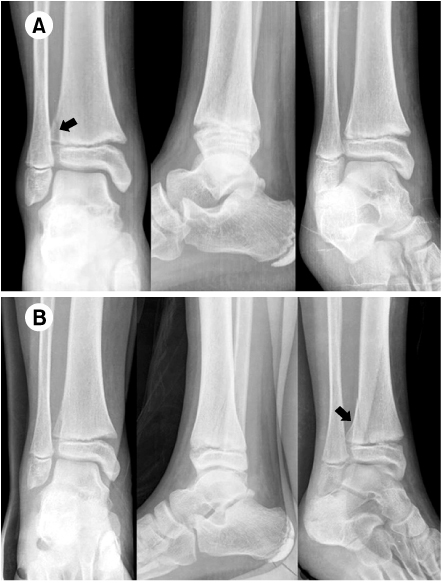

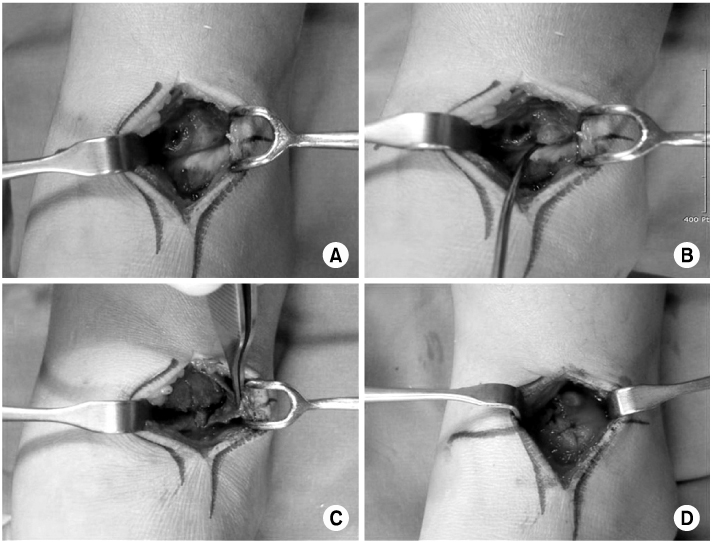
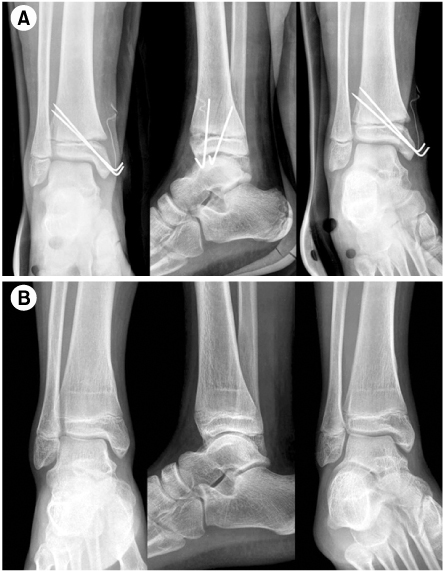
Fig. 1
A 7 year-old boy sustained physeal injury of the ankle.
(A) According to the Dias-Dachjian classification, initial radiographs show pronation-eversion-external rotation type of distal tibial physeal fracture.
(B) Post-reduction radiographs demonstrate satisfactory closed reduction. Distal tibia fracture has Thurston-Holland fragment (arrow), it representing Salter-Harris type II injury.
Fig. 2
Coronal and sagittal T2W MRI show the interposed periosteum in antero-medial aspect of distal tibial physeal fracture (arrow).
Fig. 3
(A) Intraoperative finding gross photography shows the interposed periosteun.
(B) The probe is inserted into fractured physeal space.
(C) The interposed periosteum was extracted.
(D) The extracted periosteum was repaired with absorbable suture.
Fig. 4
(A) The distal tibial physeal fracture was fixed with 2 smooth pins.
(B) At postoperative 4 years, the radiographs show no deformity or premature physeal closure.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Interposition of Periosteum in Distal Tibial Physeal Fractures of Children
Periosteal interposition in Dias-Tachjian classification (p=0.006)
*PEER: Pronation-Eversion-External Rotation, †SI: Supination-Inversion, ‡SER: Supination-External Rotation, §SP: Supination-Plantar Flexion.
Periosteal interposition in Salter-Harris classification (p=0.026)
Relationship between initial displacement and periosteal interposition (p=0.000)
Relationship between displacement after closed reduction and periosteal interposition (p=0.007)
Table 1
Periosteal interposition in Dias-Tachjian classification (p=0.006)
*PEER: Pronation-Eversion-External Rotation, †SI: Supination-Inversion, ‡SER: Supination-External Rotation, §SP: Supination-Plantar Flexion.
Table 2
Periosteal interposition in Salter-Harris classification (p=0.026)
Table 3
Relationship between initial displacement and periosteal interposition (p=0.000)
Table 4
Relationship between displacement after closed reduction and periosteal interposition (p=0.007)

