 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 33(2); 2020 > Article
- Review Article Treatment of Periprosthetic Fracture after Total Elbow Replacement Arthroplasty
- Hyunseok Seo, Jin-Hyung Im, Joo-Yup Lee
-
Journal of Musculoskeletal Trauma 2020;33(2):110-117.
DOI: https://doi.org/10.12671/jkfs.2020.33.2.110
Published online: April 30, 2020
1Department of Orthopedic Surgery, The Catholic University of Korea, Eunpyeong St. Mary’s Hospital, Seoul, Korea
2Department of Orthopedic Surgery, Gyeongsang National University Changwon Hospital, Changwon, Korea
2Department of Orthopedic Surgery, Gyeongsang National University Changwon Hospital, Changwon, Korea
- 2,050 Views
- 64 Download
- 2 Crossref
- 0 Scopus
Abstract
The indications for total elbow replacement arthroplasty (TERA) include rheumatoid arthritis, degenerative arthritis, acute fracture, nonunion, malunion, posttraumatic arthritis, tumor, and chronic instability. With the development of designs and the increasing use of TERA, more periprosthetic fractures are occurring. On the other hand, there is less data on periprosthetic fractures after TERA because TERA is a relatively rare procedure. Thus, a careful review of the previous literature and appropriate selection of surgical indications are essential for achieving a satisfactory outcome, which should be accompanied by precise surgery as planned. This article presents the causes, risk factors, classification, and principles of treatment of periprosthetic fractures after TERA.
J Korean Fract Soc. 2020 Apr;33(2):110-117. Korean.
Published online Apr 28, 2020.
https://doi.org/10.12671/jkfs.2020.33.2.110
Published online Apr 28, 2020.
https://doi.org/10.12671/jkfs.2020.33.2.110
Copyright © 2020 The Korean Fracture Society. All rights reserved.
Review
Treatment of Periprosthetic Fracture after Total Elbow Replacement Arthroplasty

Abstract
The indications for total elbow replacement arthroplasty (TERA) include rheumatoid arthritis, degenerative arthritis, acute fracture, nonunion, malunion, posttraumatic arthritis, tumor, and chronic instability. With the development of designs and the increasing use of TERA, more periprosthetic fractures are occurring. On the other hand, there is less data on periprosthetic fractures after TERA because TERA is a relatively rare procedure. Thus, a careful review of the previous literature and appropriate selection of surgical indications are essential for achieving a satisfactory outcome, which should be accompanied by precise surgery as planned. This article presents the causes, risk factors, classification, and principles of treatment of periprosthetic fractures after TERA.
Keywords
Elbow, Arthroplasty, Periprosthetic fracture
Figures
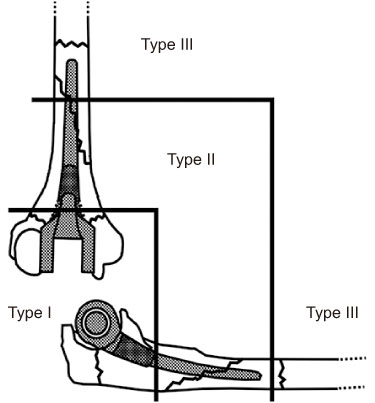
Fig. 1
Mayo classification of periprosthetic fractures after elbow arthroplasty. Type I, fracture of the humeral condyles and olecranon. Type II, humeral and ulnar shaft fracture along the length of the stem. Type III, fracture past the tip of the prosthesis.
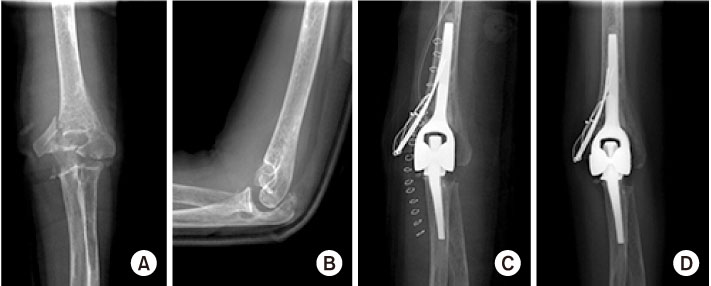
Fig. 2
(A, B) Anteriorposterior (A) and lateral (B) elbow radiographs of a 41-year-old female with rheumatoid arthritis. The comminuted intra-articular fracture of the distal humerus with the displacement of the medial condyle was found. (C) Total elbow replacement arthroplasty was performed, and tension-band wiring was simultaneously applied simultaneously to fix the medial humeral condylar fracture. (D) Anteriorposterior radiographs of 3 months postoperatively, showing bony union.
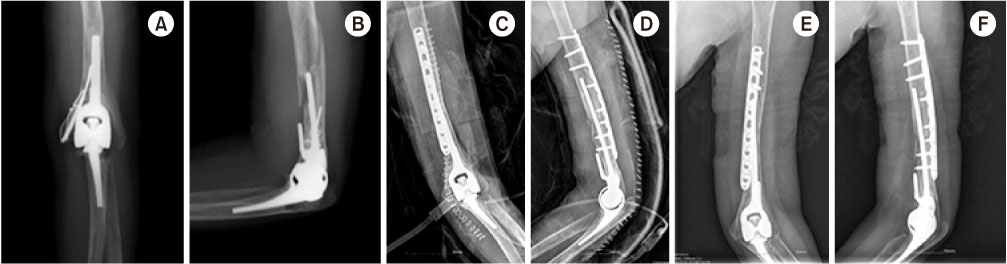
Fig. 3
(A, B) Anteriorposterior (A) and lateral (B) elbow radiographs of the same patient in Fig. 2 shows the fracture line involved proximal and distal to the tip of the prosthesis with evidence of loosening. The fracture was caused by slip down at 3 years and 7 months after the primary total elbow replacement arthroplasty. (C, D) Revision arthroplasty was done with autologous iliac bone grafting and locking compression plate fixation. (E, F) Anteriorposterior (E) and lateral (F) radiographs of 6 months postoperatively, showing bony union.

Fig. 4
(A) Anteriorposterior and lateral elbow radiographs of a 67-year-old female who had internal fixation for the distal humeral intercondylar and olecranon fracture in the other hospital three-months ago. The radiographs showed no evidence of bony union at the distal humerus. (B) Removal of hardware and total elbow replacement arthroplasty were done. The long arm splint with elbow extension was applied anteriorly after the surgery. (C) Lateral elbow radiographs 1 month postoperatively, showing refracture of the previous olecranon osteotomy site. Conservative treatment with long arm splint was planned. (D) Lateral elbow radiographs of 2 months postoperatively, showing union of the fracture.
Tables
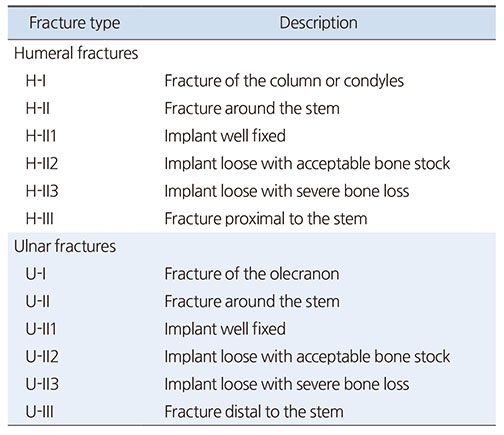
Table 1
Mayo Classification of Periprosthetic Fractures of the Elbow

Table 2
Grading Scale for Humeral Bone Loss
Notes
Financial support:None.
Conflict of interests:None.
References
-
Dee R, Sweetnam DR. Total replacement arthroplasty of the elbow joint for rheumatoid arthritis: two cases. Proc R Soc Med 1970;63:653–655.
-
-
Kozak TK, Adams RA, Morrey BF. Total elbow arthroplasty in primary osteoarthritis of the elbow. J Arthroplasty 1998;13:837–842.
-
-
Rajaee SS, Lin CA, Moon CN. Primary total elbow arthroplasty for distal humeral fractures in elderly patients: a nationwide analysis. J Shoulder Elbow Surg 2016;25:1854–1860.
-
-
Mighell MA, Dunham RC, Rommel EA, Frankle MA. Primary semi-constrained arthroplasty for chronic fracture-dislocations of the elbow. J Bone Joint Surg Br 2005;87:191–195.
-
-
Prkic A, Welsink C, The B, van den Bekerom MPJ, Eygendaal D. Why does total elbow arthroplasty fail today? A systematic review of recent literature. Arch Orthop Trauma Surg 2017;137:761–769.
-
-
DeBernardis DA, Horneff JG, Davis DE, Ramsey ML, Pontes MC, Austin LS. Revision total elbow arthroplasty failure rates: the impact of primary arthroplasty failure etiology on subsequent revisions. J Shoulder Elbow Surg 2020;29:321–328.
-
-
Yoo MC, Rhee YG, Cho YJ, Kim KI, Cho YL. Treatment of periprosthetic fracture following total elbow arthroplasty. J Korean Soc Fract 2000;13:193–199.
-
-
Suh YJ, Song SW, Rhee SK, Bae MK. Insufficiency fracture of olecranon after total elbow replacement arthroplasty in rheumatoid arthritis: report of three cases. J Korean Orthop Assoc 2005;40:89–94.
-
-
Lee SM, Park JC, Song SW, et al. Periprosthetic fractures after total elbow replacement. J Korean Soc Surg Hand 2010;15:107–111.
-
-
Kasten MD, Skinner HB. Total elbow arthroplasty. An 18-year experience. Clin Orthop Relat Res 1993;(290):177–188.
-
-
O'Driscoll SW, Morrey BF. Periprosthetic fractures about the elbow. Orthop Clin North Am 1999;30:319–325.
-
-
Hildebrand KA, Patterson SD, Regan WD, MacDermid JC, King GJ. Functional outcome of semiconstrained total elbow arthroplasty. J Bone Joint Surg Am 2000;82:1379–1386.
-
-
Geurts EJ, Viveen J, van Riet RP, Kodde IF, Eygendaal D. Outcomes after revision total elbow arthroplasty: a systematic review. J Shoulder Elbow Surg 2019;28:381–386.
-
-
Ramirez MA, Cheung EV, Murthi AM. Revision total elbow arthroplasty. J Am Acad Orthop Surg 2017;25:e166–e174.
-
-
Sanchez-Sotelo J, O'Driscoll S, Morrey BF. Periprosthetic humeral fractures after total elbow arthroplasty: treatment with implant revision and strut allograft augmentation. J Bone Joint Surg Am 2002;84:1642–1650.
-
-
Duncan CP, Masri BA. Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293–304.
-
-
Kwak JM, Koh KH, Jeon IH. Total elbow arthroplasty: clinical outcomes, complications, and revision surgery. Clin Orthop Surg 2019;11:369–379.
-
-
Cheung EV, O'Driscoll SW. Total elbow prosthesis loosening caused by ulnar component pistoning. J Bone Joint Surg Am 2007;89:1269–1274.
-
-
Kamineni S, Morrey BF. Proximal ulnar reconstruction with strut allograft in revision total elbow arthroplasty. J Bone Joint Surg Am 2004;86:1223–1229.
-
-
Ito H, Matsumoto T, Yoshitomi H, Kakinoki R, Nakamura T. The outcome of peri-operative humeral condylar fractures after total elbow replacement in patients with rheumatoid arthritis. J Bone Joint Surg Br 2007;89:62–65.
-
-
Kim JM, Mudgal CS, Konopka JF, Jupiter JB. Complications of total elbow arthroplasty. J Am Acad Orthop Surg 2011;19:328–339.
-
-
Fang C, Yan CH, Yee D, Lau TW, Wong TM, Leung F. Restoration of humeral bone stock two years after internal fixation of a periprosthetic fracture with a loose stem: a report of two cases. JBJS Case Connect 2017;7:e17
-
-
Mavrogenis AF, Angelini A, Guerra E, Rotini R. Humeral fracture between a total elbow and total shoulder arthroplasty. Orthopedics 2011;34:315.
-
-
Yanagisawa Y, Hara Y, Nozawa D, Yamazaki M. Treatment of periprosthetic humeral shaft fracture after total elbow arthroplasty in an osteoporotic patient, using the ilizarov external ring fixator: a case report. J Orthop Case Rep 2018;8:82–85.
-
-
Torbert JT, Fox EJ, Hosalkar HS, Ogilvie CM, Lackman RD. Endoprosthetic reconstructions: results of long-term followup of 139 patients. Clin Orthop Relat Res 2005;438:51–59.
-
-
Kawano Y, Okazaki M, Ikegami H, Sato K, Nakamura T, Toyama Y. The “docking” method for periprosthetic humeral fracture after total elbow arthroplasty: a case report. J Bone Joint Surg Am 2010;92:1988–1991.
-
-
Peach CA, Salama A, Stanley D. Humeral windows in revision total elbow arthroplasty. Shoulder Elbow 2016;8:130–133.
-
-
Foruria AM, Sanchez-Sotelo J, Oh LS, Adams RA, Morrey BF. The surgical treatment of periprosthetic elbow fractures around the ulnar stem following semiconstrained total elbow arthroplasty. J Bone Joint Surg Am 2011;93:1399–1407.
-
-
Tokunaga D, Hojo T, Ohashi S, et al. Periprosthetic ulnar fracture after loosening of total elbow arthroplasty treated by twostage implant revision: a case report. J Shoulder Elbow Surg 2006;15:e23–e26.
-
-
Kim JT, Jeong HJ, Lee SJ, Kim HJ, Yoo JJ. Adjuvant teriparatide therapy for surgical treatment of femoral fractures; does it work? Hip Pelvis 2016;28:148–156.
-
-
Capone A, Ennas F, Podda D. Periprosthetic femoral fractures: risk factors and current options to treatment. Aging Clin Exp Res 2011;23 2 Suppl:33–35.
-
 Cite
Cite
