 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 33(2); 2020 > Article
- Case Report Intraspinal Extradural Cyst Subsequent to a Vertebral Compression Fracture - A Case Report -
- Byeong Yeol Choi, Jong Eon Choi
-
Journal of Musculoskeletal Trauma 2020;33(2):105-109.
DOI: https://doi.org/10.12671/jkfs.2020.33.2.105
Published online: April 30, 2020
Department of Orthopaedic Surgery, St. Carollo Hospital, Suncheon, Korea
- 788 Views
- 0 Download
- 0 Crossref
- 0 Scopus
Abstract
Although a rare entity, intraspinal extradural cyst can cause severe deficit via neural compression. After reviewing available literature, the authors report a rare case of cord compression by intraspinal extradural cystic mass that developed after an osteoporotic vertebral compression fracture. An 80-year-old female patient had undergone vertebroplasty for osteoporotic vertebral compression fracture of T12, subsequent to a minor fall. However, the patient complained about sustained pain and progressive weakness of lower extremities even after the procedure. Follow-up magnetic resonance imaging revealed an intraspinal extradural cystic lesion compressing the spinal cord, and the patient had to undergo a surgical intervention via the posterior approach. Symptoms were relieved postoperatively, with no recurrence during the 1-year follow-up.
J Korean Fract Soc. 2020 Apr;33(2):105-109. Korean.
Published online Apr 28, 2020.
https://doi.org/10.12671/jkfs.2020.33.2.105
Published online Apr 28, 2020.
https://doi.org/10.12671/jkfs.2020.33.2.105
Copyright © 2020 The Korean Fracture Society. All rights reserved.
Case Report
Intraspinal Extradural Cyst Subsequent to a Vertebral Compression Fracture: A Case Report
Byeong Yeol Choi , M.D.,
and Jong Eon Choi, M.D.
, M.D.,
and Jong Eon Choi, M.D.
, M.D.,
and Jong Eon Choi, M.D.
Abstract
Although a rare entity, intraspinal extradural cyst can cause severe deficit via neural compression. After reviewing available literature, the authors report a rare case of cord compression by intraspinal extradural cystic mass that developed after an osteoporotic vertebral compression fracture. An 80-year-old female patient had undergone vertebroplasty for osteoporotic vertebral compression fracture of T12, subsequent to a minor fall. However, the patient complained about sustained pain and progressive weakness of lower extremities even after the procedure. Follow-up magnetic resonance imaging revealed an intraspinal extradural cystic lesion compressing the spinal cord, and the patient had to undergo a surgical intervention via the posterior approach. Symptoms were relieved postoperatively, with no recurrence during the 1-year follow-up.
Keywords
Extradural cyst, Osteoporotic compression fracture
Figures
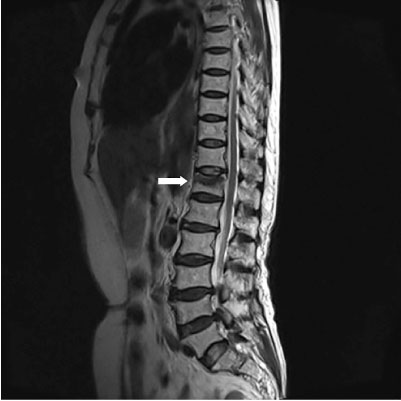
Fig. 1
T2-weighted sagittal magnetic resonance image shows acute compression fracture at T12 (arrow).

Fig. 2
Lumbar lateral radiograph showing augmented T12 vertebra with bone cement (arrow).
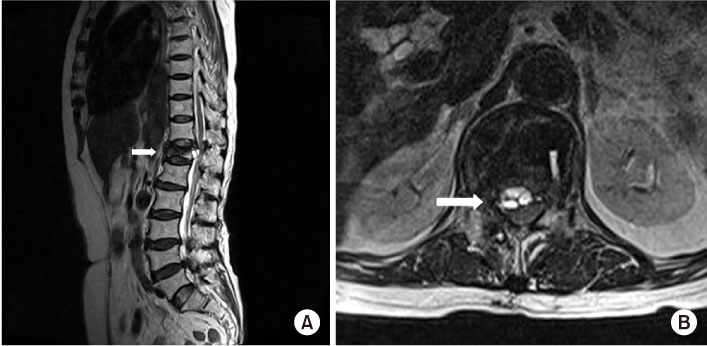
Fig. 3
T2-weighted sagittal (A) and axial (B) magnetic resonance images reveal a large septated cystic mass in the anterior extradural space (arrows).

Fig. 4
Postmyelography computed tomography scan demonstrate that the cyst is not communicating with dural sac.

Fig. 5
An intraoperative image showing the cyst (arrow) at the ventral side of the dural sac.
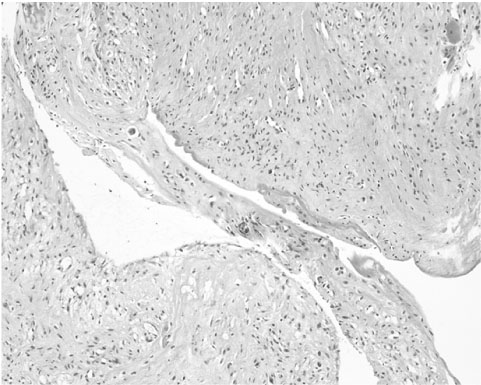
Fig. 6
Histologic image shows reactive fibrous connective tissue without epithelial lining cells, compatible with pseudomembrane (H&E, × 100).
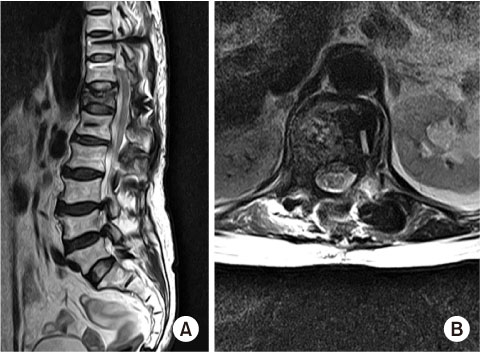
Fig. 7
Follow-up T2-weighted sagittal (A) and axial (B) magnetic resonance images at 1-year after surgery show complete removal of cyst and no recurrence.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Ito Y, Hasegawa Y, Toda K, Nakahara S. Pathogenesis and diagnosis of delayed vertebral collapse resulting from osteoporotic spinal fracture. Spine J 2002;2:101–106.
-
-
Baba H, Maezawa Y, Kamitani K, Furusawa N, Imura S, Tomita K. Osteoporotic vertebral collapse with late neurological complications. Paraplegia 1995;33:281–289.
-
-
Mao HQ, Yang HL, Geng DC, Bao ZH, Tang TS. Spinal extradural arachnoid cyst following percutaneous vertebroplasty. Eur Spine J 2011;20 Suppl 2:S206–S210.
-
-
Lee JH, Kim KT, Suk KS, et al. Extradural cyst causing spinal cord compression in osteoporotic compression fracture. J Neurosurg Spine 2013;19:133–137.
-
-
Liu SS, Williams KD, Drayer BP, Spetzler RF, Sonntag VK. Synovial cysts of the lumbosacral spine: diagnosis by MR imaging. AJNR Am J Neuroradiol 1989;10:1239–1242.
-
-
Acosta FL Jr, Quinones-Hinojosa A, Schmidt MH, Weinstein PR. Diagnosis and management of sacral Tarlov cysts. Case report and review of the literature. Neurosurg Focus 2003;15:E15
-
-
Chiba K, Toyama Y, Matsumoto M, Maruiwa H, Watanabe M, Nishizawa T. Intraspinal cyst communicating with the intervertebral disc in the lumbar spine: discal cyst. Spine (Phila Pa 1976) 2001;26:2112–2118.
-
-
Toyama Y, Kamata N, Matsumoto M, et al. Pathogenesis and diagnostic title of intraspinal cyst communicating with intervertebral disc in the lumbar spine. Rinsho Seikei Geka 1997;32:393–400.
-
-
Koga H, Yone K, Yamamoto T, Komiya S. Percutaneous CTguided puncture and steroid injection for the treatment of lumbar discal cyst: a case report. Spine (Phila Pa 1976) 2003;28:E212–E216.
-
 Cite
Cite
