 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Korean Fract Soc > Volume 37(1); 2024 > Article
- Review Article Osteoporotic Hip Fracture: How We Make Better Results?
- Byung-Chan Choi, Kyung-Jae Lee
-
Journal of The Korean Orthopaedic Trauma Association 2024;37(1):52-59.
DOI: https://doi.org/10.12671/jkfs.2024.37.1.52
Published online: January 31, 2024
Department of Orthopaedic Surgery, Keimyung University Dongsan Hospital, Keimyung University School of Medicine, Daegu, Korea
- 1,131 Views
- 33 Download
- 0 Crossref
- 0 Scopus
Abstract
The prevalence of osteoporosis and incidence of osteoporotic fractures is increasing gradually as life expectancy is prolonged and the aged population increases. Osteoporotic hip fractures (femoral neck fractures and femoral intertrochanteric fractures) have high mortality because the patients with these fractures are elderly and have several comorbidities. Thorough preparation and a multidisciplinary approach in the preoperative period are critical, and early surgery is recommended. There are also several principles to treat osteoporotic hip fractures and prevent fixation failures. Many studies have suggested various treatment methods for femoral neck fractures and femoral intertrochanteric fractures. Functional recovery treatment is essential based on the patient’s health and activity levels. Finally, aggressive management of osteoporosis and the prevention of falling is needed to treat osteoporotic hip fractures successfully.
J Korean Fract Soc. 2024 Jan;37(1):52-59. Korean.
Published online Jan 24, 2024.
https://doi.org/10.12671/jkfs.2024.37.1.52
Published online Jan 24, 2024.
https://doi.org/10.12671/jkfs.2024.37.1.52
Copyright © 2024 The Korean Fracture Society.
Review
골다공증성 고관절 골절: 어떻게 결과를 좋게 할 것인가?
Osteoporotic Hip Fracture: How We Make Better Results?
Byung-Chan Choi , M.D.
and Kyung-Jae Lee, M.D., Ph.D.
, M.D.
and Kyung-Jae Lee, M.D., Ph.D.
, M.D.
and Kyung-Jae Lee, M.D., Ph.D.
초록
기대 수명의 연장 및 노령 인구의 증가로 인해 골다공증 환자와 이로 인한 골다공증성 골절(osteoporotic fracture) 환자 역시 꾸준히 증가 추세에 있다. 골다공증성 골절 중 고관절(대퇴 경부 및 전자간부) 골절은 특히 환자의 연령이 높아 동반질환이 많아 사망률이 높은 골절이다. 골다공증성 고관절 골절 환자를 치료하기 위해서는 수술 전 면밀한 준비와 다학제적 접근이 중요하며 가능한 한 조기 수술이 추천된다. 또한, 고정 실패를 줄이기 위한 수술 중 원칙이 있으며 대퇴 경부 골절과 대퇴 전자간부 골절을 적절하게 치료하기 위한 방법이 제시되어 왔다. 골다공증성 고관절 골절의 성공적인 치료를 위해서는 수술 후 환자의 건강 상태와 보행 능력에 맞춰 기능회복 치료를 시행해야 하고 적극적인 골다공증 관리와 낙상 예방이 필요하다.
Abstract
The prevalence of osteoporosis and incidence of osteoporotic fractures is increasing gradually as life expectancy is prolonged and the aged population increases. Osteoporotic hip fractures (femoral neck fractures and femoral intertrochanteric fractures) have high mortality because the patients with these fractures are elderly and have several comorbidities. Thorough preparation and a multidisciplinary approach in the preoperative period are critical, and early surgery is recommended. There are also several principles to treat osteoporotic hip fractures and prevent fixation failures. Many studies have suggested various treatment methods for femoral neck fractures and femoral intertrochanteric fractures. Functional recovery treatment is essential based on the patient’s health and activity levels. Finally, aggressive management of osteoporosis and the prevention of falling is needed to treat osteoporotic hip fractures successfully.
Keywords
Osteoporosis, Hip fractures, Femoral neck fracture, Osteoporotic fracture
골다공증, 고관절 골절, 대퇴 경부 골절, 골다공증성 골절
서론
최근 기대 수명의 연장 및 노령 인구의 증가로 인해 골다공증 환자와 이로 인한 골다공증성 골절(osteoporotic fracture) 환자 역시 꾸준히 증가 추세에 있다.1,2) 전 세계적으로 약 2억명이 골다공증 진단을 받고 있으며,3) 매년 약 9백만 건의 골다공증성 골절이 발생하고 이는 2040년까지 2배가량 증가할 것으로 기대된다.1) 골다공증성 골절은 약 90%가 서있는 높이에서 넘어지는 등의 저에너지 손상(low-energy injury)으로 발생하며, 척추 골절(27%)이 가장 흔하고 이어서 골간단부인 손목(19%), 근위 대퇴골(14%), 그리고 근위 상완골(5%) 순으로 발생률이 높은 것으로 알려져 있다.4,5,6)
이러한 골다공증성 골절 중 고관절(대퇴 경부 및 전자간부) 골절은 특히 환자의 연령이 높아 동반질환이 많고 사망률이 높으며 수술 후 보행 능력 감소 등으로 인해 환자 개인뿐만 아니라 사회경제적으로 큰 부담이 아닐 수 없다.7) LeBlanc 등8)은 5,580명의 골다공증성 고관절 골절 환자들을 대상으로 한 연구에서 대조군에 비해 고관절 골절 환자군의 1년 사망률이 2배 정도 증가한다고 보고하였고, 다른 연구에서도 고령의 고관절 골절 환자의 1년 사망률을 22%로 높게 보고하였다.9) 또한 약 50%의 환자가 결국 일상생활을 위해 도움이 필요하게 되고, 11.3%의 환자에서 2차성 고관절 골절이 발생하는 등 그 예후 역시 좋지 못한 것으로 알려져 있다.10) 따라서 고령의 고관절 골절 환자의 치료 목표는 골절 후 가능한 한 조기에 안정적이고 통증이 없으며, 보행이 가능한(stable, painless, and walkable) 하지를 만들어 주는 데 있으며, 이러한 조기 보행 능력의 회복이 2차성 고관절 골절의 위험을 줄일 수 있는 인자 중 하나로 보고되고 있다.11)
본 논문에서는 골다공증성 고관절 골절 환자에서 이러한 목표를 달성하기 위해 수술 전, 수술 중 및 수술 후 주의점 등에 대해서 소개하고자 한다.
수술 전 준비
고령 환자에서 고관절 골절 수술을 얼마나 빨리 할 것인가에 대해서는 아직 논란이 있으나 많은 연구에서 사망률과 이환율(morbidity)을 낮추고 욕창이나 심부정맥 혈전증과 같은 합병증 발생을 예방할 수 있기 때문에 가능한 한 조기에 수술하는 것을 권장하고 있다.12,13,14,15) Pincus 등13)은 42,230명의 고관절 골절 환자에서 30일 사망률이 7%이고, 24시간 이내에 수술을 시행 받은 환자와 그렇지 못한 환자들을 비교했을 때 의미 있는 차이를 보였다고 보고하였다. Chang 등14)도 고관절 골절 수술 후 사망률을 높이는 위험인자로 암, 주거 형태(요양원/집), 호흡기질환, 당뇨병, 심혈관질환 등과 함께 48시간 이내의 수술 시간이 관련됨을 보고하였다. 따라서 고령의 고관절 골절 환자에서 동반질환에 대한 검사를 위해 수술을 지연하는 것은 합병증과 사망률을 증가시킬 수 있기 때문에 응급실 내원 시부터 다학제적 접근(multidisciplinaryapproach)을 통해 가능한 한 조기 수술을 위해 노력해야 한다. 빠른 시간 안에 마취와 수술을 위한 기본 검사들을 시행하고 문제가 발견된다면 24시간 안에 교정 가능한 것과 그렇지 못한 것을 구분하여 교정 가능한 문제들부터 해결해 주어야 한다. 또한 수술 전후로 pericapsular neve group (PENG) block이나 fascia iliaca compartment block (FICB) 등과 같은 적극적인 통증 조절을 통해서 오피오이드 사용량을 줄이고, 욕창이나 섬망(delirium) 같은 합병증을 줄여 빠른 기능회복 치료가 가능하도록 하기 위해 노력해야 한다.16,17,18,19)
또한 고령의 고관절 골절 환자들은 기저질환이 많고, 환자 개개인마다 수상 전 건강 상태나 보행 능력이 모두 다르기 때문에 같은 골절이라고 하더라도 모두 같은 수술 방법이나 기능회복 프로그램이 적용될 수 없다. 따라서 수상 전 환자의 보행 능력을 포함한 기저질환 등에 대한 철저한 병력 청취를 통해 환자 개개인에 가장 적합한 수술 방법에 대한 계획을 수립하여야 한다. 또한 고정 실패로 인해 재수술을 시행할 경우 사망률 역시 증가하므로 골절 형태, 분쇄 정도 등을 고려하여 적절한 수술 방법을 선택함으로써 한 번의 수술로 보행 가능한 하지를 만들 수 있도록 계획하여야 한다(Fig. 1,2).20)
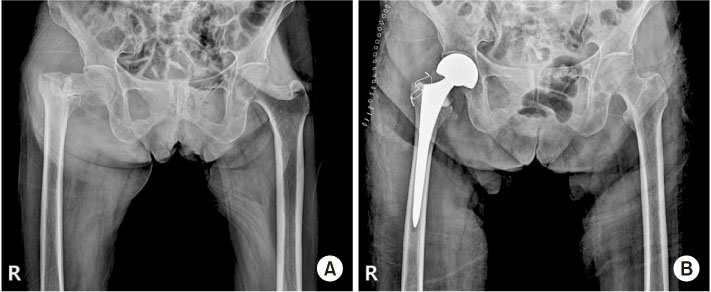
Fig. 1
(A) Plain radiograph shows femoral intertrochanteric fracture accompanied by femoral neck fracture. (B) Bipolar hemiarthroplasty was performed because of concern about fixation failure or post-traumatic avascular necrosis after internal fixation.
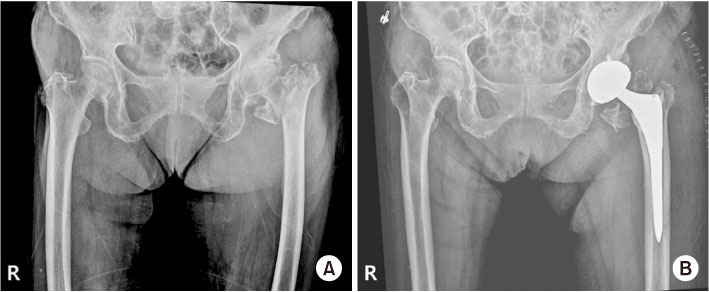
Fig. 2
(A) Plain radiograph shows femoral intertrochanteric fracture and arthritis on the ipsilateral hip joint. (B) Total hip arthroplasty was performed.
고정 실패를 줄이기 위한 수술 중 노력
고령의 고관절 골절에 대한 치료 목표는 조기 보행에 있으며 이는 술 후 합병증 및 장기 사망률을 낮추는 데 있어서 중요한 요소이다.7) 따라서 수술 방법 역시 안정적인 내고정(stable internal fixation)을 통해 조기 보행이 가능하도록 동일한 골절이라 하더라도 환자 개개인의 상태에 따라서 달라져야 하며, 다음과 같은 골다공증성 골절에서의 고정 원칙을 잘 지켜야 한다.
먼저, 절대적 안정성이 반드시 필요한 적응증이 아니라면 상대적 안정성을 통한 골절의 치유를 도모하는 것이 선호된다. 상대적 안정성을 통한 골절의 치유에서는 골절 부위 혈종과 연부조직의 손상을 최소화하면서 연골내 골화를 통한 이차 골 치유(secondary bone healing)를 도모하게 된다. 골다공증성 골절에서는 분쇄 골절이 흔하고 조골세포와 파골세포의 작용의 불균형이 있기 때문에 상대적 안정성을 통한 골절 치유가 선호된다.21) 또한, 내고정술 중에는 체중부하를 균등하게 분배할 수 있는 금속정과 같은 기구가 선호된다. 이는 골다공증성 골절을 가진 환자들이 체중 부하의 제한에 대한 순응도가 낮고 이를 조절할 수 없는 경우가 많음에서 기인한다. 골다공증성 골절의 경우, 피질골의 두께가 얇고 골수강의 직경이 큰 경우가 많아 골수강 내 금속정(intramedullary nail)을 사용할 때도 직경이 큰 금속정이 필요한 경우가 흔하다. 금속판을 사용해야 하는 경우, 응력 집중(stress riser or concentration)을 방지하기 위해서 가능한 한 길이가 긴 금속판을 사용하는 것이 좋다.22) 골다공증성 골절 치유에 있어서 뼈와 내고정기구 사이(bone-implant interface)가 초기 고정 실패의 원인이기 때문에 뼈와 내고정기구의 접촉면을 최대화하여 응력을 분산함으로써 고정 실패를 줄일 수 있다.23) 피질골이 얇고 해면골 또한 다공성으로 변화되어 있기 때문에 나사못을 사용할 때는 가능하면 나사못을 양측 피질골에 모두 고정하여 나사못 뽑힘 강도(pull out strength)를 증가시킬 수 있다. 또한, 잠김 나사(locking screw)와 잠김 금속판(locking plate)을 사용하면 나사못 뽑힘 강도를 증가시키고 금속판의 압박력이 작용하지 않아 피질골의 혈액공급을 보존할 수 있다.24) 잠김 금속판을 사용하는 경우 기구 주위 골절 발생을 줄이기 위해서 가장 바깥쪽 나사못은 잠김 나사가 아닌 피질골나사를 사용하는 것이 좋다.25) 또한, 내고정기구의 고정 실패와 대퇴 골두의 천공(cut out) 등 기계적 합병증을 줄이기 위해서 경우에 따라서 수산화인회석(hydroxyapatite) 혹은 polymethylmetacrylate (PMMA) 등을 골절 부위 혹은 주변부에 보강(augmentation)할 수 있다.2)
1. 대퇴 경부 골절
대퇴 경부 골절의 치료는 골절 부위의 전위 정도에 따라 달라진다. 전위 골절의 경우 무혈성 괴사의 발생 위험이 높기 때문에 고령 환자에서는 내고정술보다는 관절치환술(arthroplasty)이 더 선호된다.26,27) 관절치환술 시 반치환술(hemiarthroplasty)을 시행할 것인지 전치환술(total hip arthroplasty)을 시행할 것인지에 대해서는 논란이 있으나 일반적으로 동반질환의 정도, 기존 관절염의 유무, 수상 전 활동 정도 및 나이 등을 고려하여 결정할 것이 추천된다.7)
전위가 없거나 경미한 경우(Garden type I 또는 II) 다발성 유관 나사(cannulated screw) 또는 역동적 고 나사(dynamic hip screw) 등을 이용하여 고정술을 시행할 수 있다. 다발성 유관 나사 고정술은 전단 변형력(shear stress)이 상대적으로 적은 Pauwels 1, 2형의 대퇴 경부 골절에서 선호되며 일반적으로 역삼각형 형태(inverted triangular configuration)로 각각 전방, 후방 및 하방(calcar) 피질골에 인접하여 고정할 것이 권장된다(Fig. 3).28,29) 또한 필요할 경우 와셔(washer)를 사용할 경우 외측 피질골에 가해지는 힘을 분산할 수 있기 때문에 나사 삽입 토크를 높여주고, 골절 부위의 압박력을 높여 줄 수 있으며, 유관 나사의 탈출(screw backout)을 줄여줄 수 있다.30) 4번째 나사에 대해서는 논란이 있으나 후방 피질골에 분쇄가 있는 경우 고려할 수 있다.7)
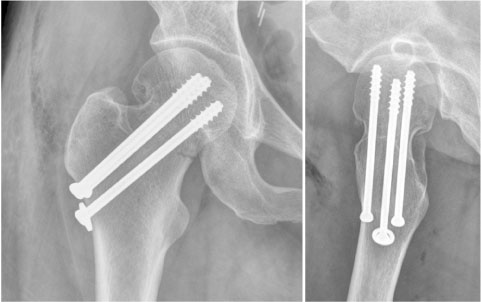
Fig. 3
Multiple cannulated screws were used in an inverted triangular configuration to fix a Garden type I femoral neck fracture.
Pauwels 3형의 대퇴 경부 골절에서는 골절선에 수직인 방향으로 삽입하는 Pauwels 나사를 사용하거나31) 대퇴 경부 내측에 지지 금속판을 이용할 수 있으며,32) 역동적 고 나사를 사용함으로써7) 기존의 다발성 유관 나사보다 전단 변형력에 강한 저항력을 가질 수 있다.
역동적 고 나사는 유관 나사의 대안으로 사용될 수 있으며 배럴(barrel) 안에서 래그 나사(lag screw)의 미끄러짐(sliding)이 일어날 수 있도록 함으로써 골절 부위의 압박력을 얻는다. 특히 역동적 고 나사는 고정각 장치(fixed angle device)로 유관 나사에 비하여 전단 변형력(shear stress)에 강한 저항을 나타내므로 대퇴 경부 기저부 골절(basicervical femoral neck fracture)에서 우수한 결과를 보여준다(Fig. 4).7) 다만 최근 연구에서 역동적 고 나사가 유관 나사에 비해서 무혈성 괴사의 발생 위험이 높다는 연구가 있어 이에 대한 주의가 필요하다.33)
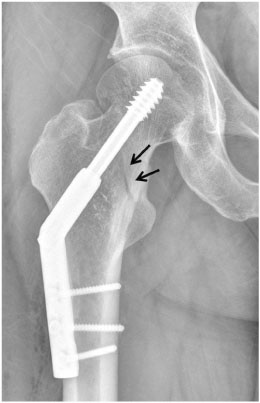
Fig. 4
Dynamic hip screw was used to fix a basicervical femoral neck fracture (arrows).
Lim 등34)이 발표한 Pauwels 2형 혹은 3형의 대퇴 경부 골절에 관한 체계적 문헌고찰 및 메타분석을 살펴보면 역동적 고 나사를 이용했을 때 다발성 유관 나사를 삽입했을 때보다 불유합의 발생 빈도가 유의하게 낮았으며, 두 수술 방법 간 무혈성 괴사의 발생 빈도는 차이가 없다고 보고한 바 있다. 수술 방법에 따른 임상적, 방사선학적 결과와 합병증의 발생 빈도가 다양한 만큼 이에 대한 큰 규모의 연구가 필요할 것으로 생각된다.
최근에는 대퇴 경부 기저부 골절에서의 수술 방법에 대해서 다양한 연구 결과가 나오고 있다. 대퇴 경부 기저부 골절은 대퇴 경부의 골두하 골절(subcapital femoral neck fracture) 혹은 중간경부 골절(transcervical femoral neck fracture)과 비교했을 때 골절의 근위 골편의 회전 불안정성이 더 심한 특징을 가지고 있다.35) 이러한 특성 때문에 대퇴 경부 기저부 골절에서는 고정 실패의 위험도가 높으며, 대퇴 전자간부 골절에 준하여 치료를 해야 한다고 알려져 있으나 이 또한 좋지 못한 결과를 보이며 궁극적으로 많은 환자에서 관절치환술을 필요로 하게 된다.35)
2. 대퇴 전자간부 골절
대퇴 전자간부 골절 치료를 위한 기구의 선택은 골절의 안정성(stability of fracture pattern)과 외측 피질골의 상태(integrity of lateral cortex)에 따라 달라질 수 있다. 안정형 대퇴 전자간 골절은 후내측 대퇴거(posteromedial cortical calcar)가 온전하거나 잘 정복이 될 수 있는 골절 형태로 이러한 경우 근위 대퇴부의 스트레스를 분산시키고 내측 압박력에 저항할 수 있게 된다. 따라서 안정형 대퇴 전자간 골절은 역동적 고 나사와 골수강내 금속정 모두 만족할 만한 임상 결과를 보여준다.36)
불안정형 골절은 4분형 골절인 경우, 역경사 골절(reverse oblique fracture)이나 횡골절(transtrochanteric fracture)처럼 외측벽이 손상된 경우, 대퇴거의 분쇄나 큰 후내측 골편이 있는 경우, 골절이 전자하부로 진행된 경우 등이 있다(Fig. 5,6,7,8). 이러한 불안정형 대퇴 전자간 골절에서는 생체 역학적으로 골수강내 금속정이 응력 중심 간 거리(lever arm)가 짧고, 외측벽으로서의 기능을 할 수 있기 때문에 역동적 고 나사에 비해 장점이 있다.7) 다만 대퇴 경부 단축을 줄여주는 등의 방사선학적 장점은 있으나 임상적 결과에는 큰 차이가 없다는 결과도 있어 추가적인 연구가 필요할 것으로 생각된다.37)

Fig. 5
Plain radiograph (A) and computed tomography (B) show unstable femoral intertrochanteric fracture (four-part femoral intertrochanteric fracture).

Fig. 6
Plain radiograph shows unstable femoral intertrochanteric fracture concomitant with a lateral wall fracture. (A) Reverse oblique type. (B) Transverse type.
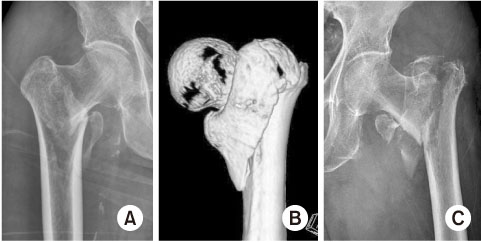
Fig. 7
Plain radiograph and computed tomography (CT) show unstable femoral intertrochanteric fracture concomitant with a posteromedial fragment. (A) Large posterior fragment. (B) CT image of a large posterior fragment. (C) Comminuted fracture in femoral calcar area.

Fig. 8
Plain radiograph shows unstable femoral intertrochanteric fracture. The fracture line is extended to the subtrochanteric area.
역동적 고 나사의 흔한 합병증 중 하나인 대퇴골두 천공을 줄이기 위해 최근 전통적인 래그 나사 대신 나선형 날(helical blade)을 사용하기도 한다. 생체 역학 연구에서 전통적인 래그 나사에 비해 나사못 뽑힘 강도 및 회전 안정성이 더 높은 것으로 보고되었으며,38) 임상적으로도 고정 실패가 더 낮다고 보고되었다.39) 다만 재수술률이나 대퇴골두 천공의 빈도는 두 기구에서 차이가 없다는 보고도 있고, 골수강내 금속정에서는 helical blade 역시 대퇴 골두 천공 발생의 빈도가 높다는 보고도 있기 때문에 helical blade에 대해서는 추가적인 연구가 필요할 것으로 생각된다.39,40)
수술 후 관리
일반적으로 고령의 고관절 골절 환자는 수술 후 평균적으로 1단계 정도의 보행 능력 감소가 있을 수 있고, 약 50%의 환자는 결국 일상생활을 위해 도움을 필요로 하게 되며,10) 수술 후 조기 보행 능력 회복은 2차 골절을 줄이고 이로 인한 사망률 감소에도 영향을 미치는 것으로 알려져 있다.11,41) 따라서 수상 전 환자의 건강 상태나 보행 능력에 맞춰 수술 직후부터 기능회복 치료를 시행할 수 있도록 다학제적 접근이 이루어져야 하며 이를 위해서 내외과적 기저질환의 관리, 체계적 기능회복 프로그램의 관리 및 환자와 보호자에 대한 교육이 필수적이다.
골다공증성 고관절 골절 이후 2차성 고관절 골절의 발생은 사망률을 높이고 환자의 활동성(mobility)을 저하시키는 주된 원인이 되고 있으며, 여러 연구에서 2차성 고관절 골절의 발생이 4.8%에서 11.3%까지 보고되고 있어 그 빈도 역시 적지 않다.10,11) 따라서 2차성 고관절 골절을 줄이기 위해 낙상 예방 및 골다공증 관리 역시 중요하다. 특히 골다공증성 고관절 골절 환자는 대부분 초고위험 환자군에 속하기 때문에 골다공증 관리는 먼저 부갑상선 호르몬제제와 같은 골형성 촉진제를 사용하고 이어서 골흡수 억제제를 사용하는 순차요법이 추천되며,42) 정형외과 의사는 다학제 시스템 내에서 골다공증 치료를 시작하고 지속 여부를 점검하는 역할을 해야 한다.
결론
골다공증성 고관절 골절 환자의 치료는 단순히 정형외과적 수술 기법이 좋아진다고 좋은 결과를 얻을 수 있는 것이 아니다. 수술 전부터 다학제적 접근을 통해 조기 수술이 가능하도록 병원 시스템을 갖추어야 하며, 골다공증성 고관절 골절의 고정 원칙에 대한 이해를 통해 조기에 통증 없이 보행 가능한 하지를 만들어줄 수 있는 최선의 수술 방법을 환자 개개인에 맞게 찾아야 한다. 수술 후에도 낙상 예방 및 골다공증 관리를 통해 2차 골절을 예방하고 고정 실패를 줄여 줌으로써 성공적인 결과를 기대할 수 있을 것이다.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Yaacobi E, Sanchez D, Maniar H, Horwitz DS. Surgical treatment of osteoporotic fractures: an update on the principles of management. Injury 2017;48 Suppl 7:S34–S40.
-
-
Schuetze K, Eickhoff A, Röderer G, Gebhard F, Richter PH. Osteoporotic bone: when and how to use augmentation? J Orthop Trauma 2019;33 Suppl 8:S21–S26.
-
-
Bogunovic L, Cherney SM, Rothermich MA, Gardner MJ. Biomechanical considerations for surgical stabilization of osteoporotic fractures. Orthop Clin North Am 2013;44:183–200.
-
-
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res 2007;22:465–475.
-
-
Konstantinidis L, Helwig P, Hirschmüller A, Langenmair E, Südkamp NP, Augat P. When is the stability of a fracture fixation limited by osteoporotic bone? Injury 2016;47 Suppl 2:S27–S32.
-
-
Bell JE, Leung BC, Spratt KF, et al. Trends and variation in incidence, surgical treatment, and repeat surgery of proximal humeral fractures in the elderly. J Bone Joint Surg Am 2011;93:121–131.
-
-
Lu Y, Uppal HS. Hip fractures: relevant anatomy, classification, and biomechanics of fracture and fixation. Geriatr Orthop Surg Rehabil 2019;10:2151459319859139
-
-
LeBlanc ES, Hillier TA, Pedula KL, et al. Hip fracture and increased short-term but not long-term mortality in healthy older women. Arch Intern Med 2011;171:1831–1837.
-
-
Tiihonen R, Helkamaa T, Nurmi-Lüthje I, Kaukonen JP, Kataja M, Lüthje P. Patient-specific factors affecting survival following hip fractures-a 14-year follow-up study in Finland. Arch Osteoporos 2022;17:107
-
-
Fukushima T, Sudo A, Uchida A. Bilateral hip fractures. J Orthop Sci 2006;11:435–438.
-
-
Lee KJ, Choi JH, Ye HU, Kim YH, Lim KH. Risk factors for subsequent contralateral hip fracture following osteoporotic hip fracture surgery. J Korean Fract Soc 2021;34:51–56.
-
-
Leung F, Lau TW, Kwan K, Chow SP, Kung AW. Does timing of surgery matter in fragility hip fractures? Osteoporos Int 2010;21 Suppl 4:S529–S534.
-
-
Pincus D, Ravi B, Wasserstein D, et al. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. JAMA 2017;318:1994–2003.
-
-
Chang W, Lv H, Feng C, et al. Preventable risk factors of mortality after hip fracture surgery: systematic review and meta-analysis. Int J Surg 2018;52:320–328.
-
-
Rai SK, Varma R, Wani SS. Does time of surgery and complication have any correlation in the management of hip fracture in elderly and can early surgery affect the outcome? Eur J Orthop Surg Traumatol 2018;28:277–282.
-
-
Kim CH, Yang JY, Min CH, Shon HC, Kim JW, Lim EJ. The effect of regional nerve block on perioperative delirium in hip fracture surgery for the elderly: a systematic review and meta-analysis of randomized controlled trials. Orthop Traumatol Surg Res 2022;108:103151
-
-
Girón-Arango L, Peng PWH, Chin KJ, Brull R, Perlas A. Pericapsular Nerve Group (PENG) block for hip fracture. Reg Anesth Pain Med 2018;43:859–863.
-
-
Mosaffa F, Taheri M, Manafi Rasi A, Samadpour H, Memary E, Mirkheshti A. Comparison of pericapsular nerve group (PENG) block with fascia iliaca compartment block (FICB) for pain control in hip fractures: a double-blind prospective randomized controlled clinical trial. Orthop Traumatol Surg Res 2022;108:103135
-
-
Salottolo K, Meinig R, Fine L, et al. A multi-institutional prospective observational study to evaluate fascia iliaca compartment block (FICB) for preventing delirium in adults with hip fracture. Trauma Surg Acute Care Open 2022;7:e000904
-
-
Palmer SJ, Parker MJ, Hollingworth W. The cost and implications of reoperation after surgery for fracture of the hip. J Bone Joint Surg Br 2000;82:864–866.
-
-
Hollensteiner M, Sandriesser S, Bliven E, von Rüden C, Augat P. Biomechanics of osteoporotic fracture fixation. Curr Osteoporos Rep 2019;17:363–374.
-
-
Bottlang M, Doornink J, Byrd GD, Fitzpatrick DC, Madey SM. A nonlocking end screw can decrease fracture risk caused by locked plating in the osteoporotic diaphysis. J Bone Joint Surg Am 2009;91:620–627.
-
-
von Rüden C, Augat P. Failure of fracture fixation in osteoporotic bone. Injury 2016;47 Suppl 2:S3–S10.
-
-
Bottlang M, Doornink J, Fitzpatrick DC, Madey SM. Far cortical locking can reduce stiffness of locked plating constructs while retaining construct strength. J Bone Joint Surg Am 2009;91:1985–1994.
-
-
Kammerlander C, Erhart S, Doshi H, Gosch M, Blauth M. Principles of osteoporotic fracture treatment. Best Pract Res Clin Rheumatol 2013;27:757–769.
-
-
Parker MJ. Hemiarthroplasty versus internal fixation for displaced intracapsular fractures of the hip in elderly men: a pilot randomised trial. Bone Joint J 2015;97-B:992–996.
-
-
Parker MJ, Pryor G, Gurusamy K. Hemiarthroplasty versus internal fixation for displaced intracapsular hip fractures: a long-term follow-up of a randomised trial. Injury 2010;41:370–373.
-
-
Zdero R, Keast-Butler O, Schemitsch EH. A biomechanical comparison of two triple-screw methods for femoral neck fracture fixation in a synthetic bone model. J Trauma 2010;69:1537–1544.
-
-
Selvan VT, Oakley MJ, Rangan A, Al-Lami MK. Optimum configuration of cannulated hip screws for the fixation of intracapsular hip fractures: a biomechanical study. Injury 2004;35:136–141.
-
-
Zlowodzki MP, Wijdicks CA, Armitage BM, Cole PA. Value of washers in internal fixation of femoral neck fractures with cancellous screws: a biomechanical evaluation. J Orthop Trauma 2015;29:e69–e72.
-
-
Hawks MA, Kim H, Strauss JE, et al. Does a trochanteric lag screw improve fixation of vertically oriented femoral neck fractures? A biomechanical analysis in cadaveric bone. Clin Biomech (Bristol, Avon) 2013;28:886–891.
-
-
Ye Y, Chen K, Tian K, Li W, Mauffrey C, Hak DJ. Medial buttress plate augmentation of cannulated screw fixation in vertically unstable femoral neck fractures: surgical technique and preliminary results. Injury 2017;48:2189–2193.
-
-
Fixation using Alternative Implants for the Treatment of Hip fractures (FAITH) Investigators. Fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet 2017;389:1519–1527.
-
-
Lim EJ, Shon HC, Cho JW, Oh JK, Kim J, Kim CH. Dynamic hip screw versus cannulated cancellous screw in pauwels type II or type III femoral neck fracture: a systematic review and meta-analysis. J Pers Med 2021;11:1017
-
-
Yoo JI, Cha Y, Kwak J, Kim HY, Choy WS. Review on basicervical femoral neck fracture: definition, treatments, and failures. Hip Pelvis 2020;32:170–181.
-
-
Kaplan K, Miyamoto R, Levine BR, Egol KA, Zuckerman JD. Surgical management of hip fractures: an evidence-based review of the literature. II: intertrochanteric fractures. J Am Acad Orthop Surg 2008;16:665–673.
-
-
Reindl R, Harvey EJ, Berry GK, Rahme E. Intramedullary versus extramedullary fixation for unstable intertrochanteric fractures: a prospective randomized controlled trial. J Bone Joint Surg Am 2015;97:1905–1912.
-
-
O’Neill F, Condon F, McGloughlin T, Lenehan B, Coffey JC, Walsh M. Dynamic hip screw versus DHS blade: a biomechanical comparison of the fixation achieved by each implant in bone. J Bone Joint Surg Br 2011;93:616–621.
-
-
Fang C, Lau TW, Wong TM, Lee HL, Leung F. Sliding hip screw versus sliding helical blade for intertrochanteric fractures: a propensity score-matched case control study. Bone Joint J 2015;97-B:398–404.
-
-
Stern LC, Gorczyca JT, Kates S, Ketz J, Soles G, Humphrey CA. Radiographic review of helical blade versus lag screw fixation for cephalomedullary nailing of low-energy peritrochanteric femur fractures: there is a difference in cutout. J Orthop Trauma 2017;31:305–310.
-
-
Iosifidis M, Iliopoulos E, Panagiotou A, Apostolidis K, Traios S, Giantsis G. Walking ability before and after a hip fracture in elderly predict greater long-term survivorship. J Orthop Sci 2016;21:48–52.
-
-
Shoback D, Rosen CJ, Black DM, Cheung AM, Murad MH, Eastell R. Pharmacological management of osteoporosis in postmenopausal women: an Endocrine Society guideline update. J Clin Endocrinol Metab 2020;105:dgaa048
-
 Cite
Cite
