 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 20(2); 2007 > Article
-
Original Article
- Posterior Plating in Distal Fibular Fracture
- Choong-Hyeok Choi, M.D., Young-A Cho, M.D., Jae-Hoon Kim, M.D., Il-Hoon Sung, M.D.
-
Journal of the Korean Fracture Society 2007;20(2):161-165.
DOI: https://doi.org/10.12671/jkfs.2007.20.2.161
Published online: June 14, 2016
Department of Orthopedic Surgery, Hanyang University College of Medicine, Seoul, Korea.
- Address reprint requests to: Il-Hoon Sung, M.D. Department of Orthopedic Surgery, Hanyang University Hospital, 17, Haengdang-dong, Seongdong-gu, Seoul 133-792, Korea. Tel: 82-2-2290-8485, Fax: 82-2-2299-3774, sungih@hanyang.ac.kr
Copyright © The Korean Fracture Society. All rights reserved
- 1,215 Views
- 20 Download
- 1 Crossref
Abstract
-
Purpose
- To report the technical experience of posterior plating for the distal fibular fracture.
-
Materials and Methods
- 20 Weber type-B fibular fractures were included in this study, which were treated with the posterior plating. 1/3 semitubular plate was used and orientation of all screws were intended to be perpendicular to the plate as possible. Fixation stability and maintenance of reduction after plating was assessed manually in the operating field. Clinical results were evaluated at least 1 year after operation, using American Orthopaedic Foot and Ankle Society (AFOAS) Ankle-Hindfoot score.
-
Results
- 5 cases were firmly stabilized without using any lag screw or fixation of distal fragment. For improving stability or achieving proper reduction, a lag screw was placed posteroanteriorly through the plate in 14 cases. Anteroposterior interfragmentary fixation in 1 case before plating, and contouring of the plate in 3 cases were needed in cases of which the posterior plating impeded reduction of distal fibular fracture. In all cases, fracture was stabilized without fixation through the most distal hole. There were no major postoperative complications. AFOAS score was 95.5±5.2.
-
Conclusion
- The posterior plating technique for distal fibular fracture is regarded as a recommendable option. Additional fixation with interfragmentary screw or contouring of the plate, however, would be needed in some cases to achieve anatomical reduction or sufficient stability.
- 1. Broos PL, Bisschop AP. Operative treatment of ankle fractures in adults: correlation between types of fracture and final results. Injury, 1991;22:403-406.Article
- 2. Brunner CF, Weber BG. The antiglide plate: special techniques in internal fixation. New York: Springer-Verlag; 1982. p. 115-133.
- 3. de Souza LJ, Gustilo RB, Meyer TJ. Results of operative treatment of displaced external rotation-abduction fractures of the ankle. J Bone Joint Surg Am, 1985;67:1066-1074.Article
- 4. Hughes JL, Weber H, Willenegger H, Kuner EH. Evaluation of ankle fractures: non-operative and operative treatment. Clin Orthop Relat Res, 1979;138:111-119.
- 5. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int, 1994;15:349-353.ArticlePDF
- 6. Kwak HY, Song BY, Bae SW, Choi NH, Kim JY. The treatment of Danis-Weber type B fractures of the distal fibula by multiple Kirschner wires fixation. J Korean Soc Fract, 2000;13:529-536.Article
- 7. Lee WC, Ahn JH. Nonoperative treatment of isolated lateral malleolar fracture. J Korean Fract Soc, 2005;18:291-293.Article
- 8. Lindsjo U. Classification of ankle fractures: the Lauge-Hansen or AO system? Clin Orthop Relat Res, 1985;199:12-16.
- 9. Pettrone FA, Gail M, Pee D, Fitzpatrick T, Van Herpe LB. Quantitative criteria for prediction of the results after displaced fracture of the ankle. J Bone Joint Surg Am, 1983;65:667-677.Article
- 10. Roberts RS. Surgical treatment of displaced ankle fractures. Clin Orthop Relat Res, 1983;172:164-170.Article
- 11. Schaffer JJ, Manoli A 2nd. The antiglide plate for distal fibular fixation. A biomechanical comparison with fixation with a lateral plate. J Bone Joint Surg Am, 1987;69:596-603.Article
- 12. Yablon IG, Heller FG, Shouse L. The key role of the lateral malleolus in displaced fractures of the ankle. J Bone Joint Surg Am, 1977;59:169-173.Article
REFERENCES
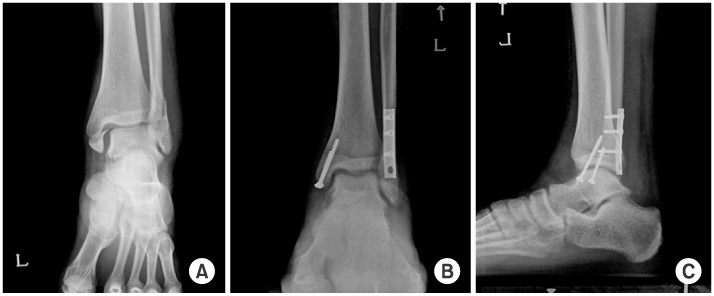
Fig. 1
(A) Preoperative anteroposterior radiography of ankle fracture.
(B, C) Standing anteroposterior and lateral radiography of ankle, 6 months after operation.

A case, showing bimalleolar fracture of which distal fibula was fixed, using posterior plate without lag screw or fixation of distal fragment.
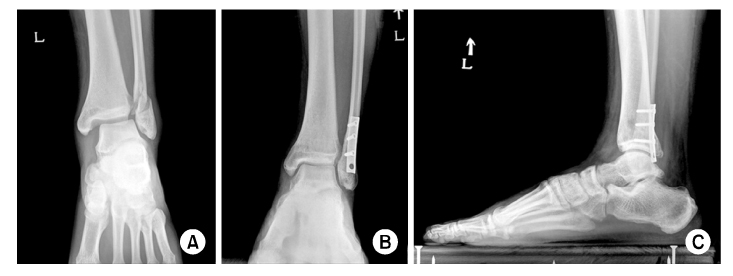
Fig. 2
(A) Preoperative anteroposterior radiography of ankle fracture.
(B, C) Standing anteroposterior and lateral radiography of ankle, 6 months after operation.
A case, showing bimalleolar fracture of which distal fibula was fixed, using posterior plate with a posteroanterior lag screw.
Fig. 3
(A) Preoperative anteroposterior radiography of ankle fracture.
(B, C) Standing anteroposterior and lateral radiography of ankle, 6 months after operation.
A case, showing bimalleolar equivalent fracture of which distal fibula was fixed, using manually contoured posterior plate with a posteroanterior lag screw.
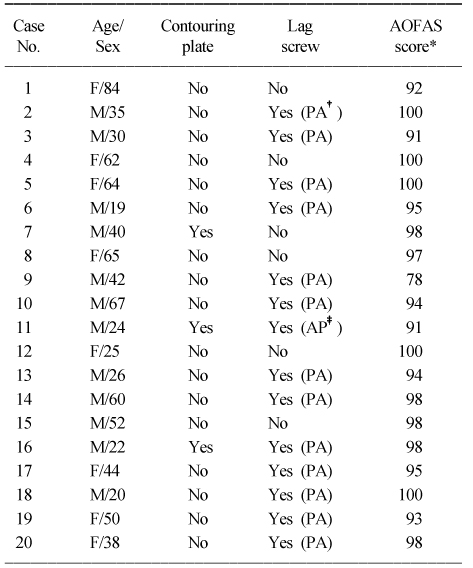
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- A Specialized Fibular Locking Plate for Lateral Malleolar Fractures
Eui Dong Yeo, Hak Jun Kim, Woo In Cho, Young Koo Lee
The Journal of Foot and Ankle Surgery.2015; 54(6): 1067. CrossRef
 Cite
CitePosterior Plating in Distal Fibular Fracture
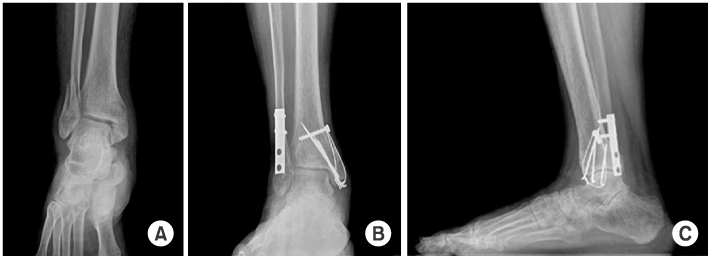
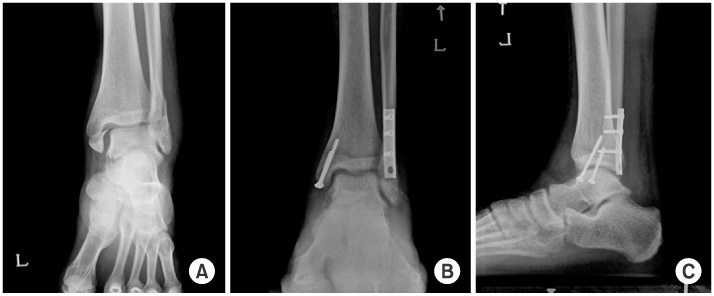
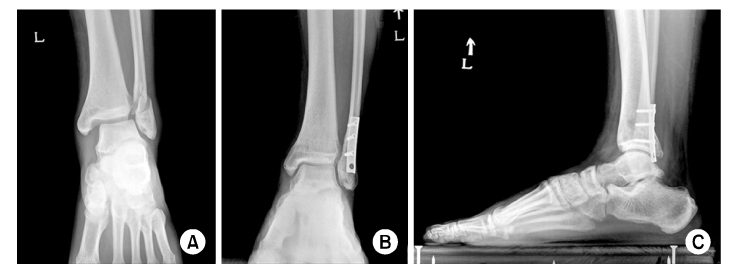
Fig. 1
A case, showing bimalleolar fracture of which distal fibula was fixed, using posterior plate without lag screw or fixation of distal fragment.
(A) Preoperative anteroposterior radiography of ankle fracture.
(B, C) Standing anteroposterior and lateral radiography of ankle, 6 months after operation.
Fig. 2
A case, showing bimalleolar fracture of which distal fibula was fixed, using posterior plate with a posteroanterior lag screw.
(A) Preoperative anteroposterior radiography of ankle fracture.
(B, C) Standing anteroposterior and lateral radiography of ankle, 6 months after operation.
Fig. 3
A case, showing bimalleolar equivalent fracture of which distal fibula was fixed, using manually contoured posterior plate with a posteroanterior lag screw.
(A) Preoperative anteroposterior radiography of ankle fracture.
(B, C) Standing anteroposterior and lateral radiography of ankle, 6 months after operation.
Fig. 1
Fig. 2
Fig. 3
Posterior Plating in Distal Fibular Fracture
Clinical data of patients
*AOFAS score: American Orthopaedic Foot and Ankle Society Ankle-Hindfoot score, †PA: Posteroanterior, ‡AP: Anteroposterior.
Table 1
Clinical data of patients
*AOFAS score: American Orthopaedic Foot and Ankle Society Ankle-Hindfoot score, †PA: Posteroanterior, ‡AP: Anteroposterior.

