 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 28(3); 2015 > Article
-
Original Article
- A Comparison of Quality of Life Using Short Form 36 between Femoral Shaft Fracture and Tibia Shaft Fracture Treated with Antegrade Nailing
- Sangbong Ko, M.D., Hojin Chang, M.D.
-
Journal of the Korean Fracture Society 2015;28(3):163-168.
DOI: https://doi.org/10.12671/jkfs.2015.28.3.163
Published online: July 22, 2015
Department of Orthopaedic Surgery, Daegu Catholic University Medical Center, Daegu Catholic University School of Medicine, Daegu, Korea.
- Address reprint requests to: Hojin Chang, M.D. Department of Orthopaedic Surgery, Daegu Catholic University Medical Center, 33 Duryugongwon-ro 17-gil, Nam-gu, Daegu 705-718, Korea. Tel: 82-53-650-4283, Fax: 82-53-626-4272, hoji98@gmail.com
• Received: February 13, 2015 • Revised: April 26, 2015 • Accepted: April 29, 2015
Copyright © 2015 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,092 Views
- 1 Download
- 1 Crossref
Abstract
-
Purpose
- We sought to compare the quality of life between two similar groups of patients; one group who sustained an isolated femoral shaft fracture, and the other group who sustained an isolated tibial shaft fracture.
-
Materials and Methods
- From February 1995 to July 2010, two groups of 168 patients who underwent implant removal operations after intramedullary nailing for an isolated femoral shaft fracture or an isolated tibial shaft fracture were enrolled. Short Form 36 (SF-36) questionnaires were completed at the final follow-up visit. Data analysis was performed by another physician not otherwise involved with clinical evaluation or the surgeries.
-
Results
- Patients ranged in age from 18 to 37 years old. The two groups had similar characteristics, including age, gender ratio, body weight, smoking, and mean follow-up period (all p>0.05). No significant difference in functional outcome using SF-36 was observed between the groups except in the domain of physical functioning (PF) where femoral shaft fracture patients had a slightly higher score (p=0.002).
-
Conclusion
- Femoral shaft fracture patients and tibial shaft fracture patients who underwent intramedullary nailing and subsequent implant removal after fracture union with similar epidemiological characteristics had similar functional outcomes using the SF-36 survey, except in the domain of PF, where femoral shaft fracture patients had a slightly better outcome.
- 1. Dimitriou R, Giannoudis PV. Tibia shaft fractures. In: Bentley G, editor. European surgical orthopaedics and traumatology: the EFORT textbook. New Delhi, India: Springer Referene; 2014. p. 2854-2876.
- 2. Ware JE Jr, Kosinski M, Bayliss MS, McHorney CA, Rogers WH, Raczek A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the Medical Outcomes Study. Med Care, 1995;33:AS264-AS279.
- 3. Safran M, Botser IB. Hip anaotmy and biomechanics. In: Miller MD, Thompson SR, editors. DeLee & Drez's orthopaedic sports medicine. 4th ed. Philadelphia, PA: Elsevier Saunders; 2010. p. 920.
- 4. Bucholz RW, Brumback RJ. Fractures of the shaft of the femur. In: Rockwood CA, Green DP, Bucholz RW, Heckman JD, editors. Rockwood and Green's fractures in adults. 4th ed. Philadelphia, PA: Lippincott-Raven; 1996. p. 1827-1828.
- 5. Whittle AP, Wood GW II. Fractures of the lower extremity. In: Canale ST, editor. Campbell's operative orthopedics. 10th ed. St. Louis, MO: Mosby; 2003. p. 2754-2825.
- 6. Moghaddam A, Zimmermann G, Hammer K, Bruckner T, Grützner PA, von Recum J. Cigarette smoking influences the clinical and occupational outcome of patients with tibial shaft fractures. Injury, 2011;42:1435-1442.Article
- 7. Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators. Bhandari M, Guyatt G, et al. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. J Bone Joint Surg Am, 2008;90:2567-2578.Article
- 8. Cannada LK, Anglen JO, Archdeacon MT, Herscovici D Jr, Ostrum RF. Avoiding complications in the care of fractures of the tibia. J Bone Joint Surg Am, 2008;90:1760-1768.
- 9. Castillo RC, Bosse MJ, MacKenzie EJ, Patterson BM. LEAP Study Group. Impact of smoking on fracture healing and risk of complications in limb-threatening open tibia fractures. J Orthop Trauma, 2005;19:151-157.Article
- 10. Moghaddam A, Elleser C, Biglari B, Wentzensen A, Zimmermann G. Clinical application of BMP 7 in long bone non-unions. Arch Orthop Trauma Surg, 2010;130:71-76.ArticlePDF
- 11. Ware JE Jr, Sherbourne CD. The MOS 36-item shortform health survey (SF-36). I. Conceptual framework and item selection. Med Care, 1992;30:473-483.
- 12. McHorney CA, Ware JE Jr, Lu JF, Sherbourne CD. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care, 1994;32:40-66.
- 13. Greenwood DC, Muir KR, Doherty M, Milner SA, Stevens M, Davis TR. Conservatively managed tibial shaft fractures in Nottingham, UK: are pain, osteoarthritis, and disability long-term complications? J Epidemiol Community Health, 1997;51:701-704.Article
- 14. Busse JW, Bhandari M, Guyatt GH, et al. SPRINT Investigators. Use of both Short musculoskeletal function assessment questionnaire and short form-36 among tibialfracture patients was redundant. J Clin Epidemiol, 2009;62:1210-1217.
- 15. Koh SB, Chang SJ, Kang MG, Cha BS, Park JK. Reliability and validity on measurement instrument for health status assessment in occupational workers. Korean J Prev Med, 1997;30:251-266.
- 16. Bone LB, Sucato D, Stegemann PM, Rohrbacher BJ. Displaced isolated fractures of the tibial shaft treated with either a cast or intramedullary nailing An outcome analysis of matched pairs of patients. J Bone Joint Surg Am, 1997;79:1336-1341.Article
- 17. Court-Brown CM, Christie J, McQueen MM. Closed intramedullary tibial nailing Its use in closed and type I open fractures. J Bone Joint Surg Br, 1990;72:605-611.ArticlePDF
- 18. Lefaivre KA, Guy P, Chan H, Blachut PA. Long-term follow-up of tibial shaft fractures treated with intramedullary nailing. J Orthop Trauma, 2008;22:525-529.Article
- 19. Wyrwich KW, Tierney WM, Babu AN, Kroenke K, Wolinsky FD. A comparison of clinically important differences in health-related quality of life for patients with chronic lung disease, asthma, or heart disease. Health Serv Res, 2005;40:577-591.Article
REFERENCES

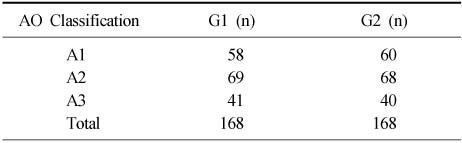
Table 3
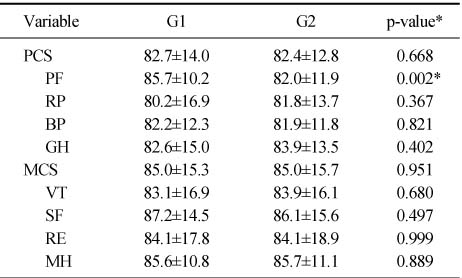
Results of Functional Outcomes
Values are presented as mean±standard deviation. *p<0.05. G1: Patients of femoral shaft fractures treated with intramedullary nail, G2: Patients of tibial shaft fractures treated with intramedullary nail, PCS: Physical component score in Short Form 36 (SF-36), PF: Physical functioning, RP: Role limitation due to physical health problems, BP: Bodily pain, GH: General health perception, MCS: Mental component score in SF-36, VT: Vitality, SF: Social functioning, RE: Role limitation due to emotional problems, MH: Mental health.
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Health‐related quality of life outcomes after surgical treatment of atypical femur fractures: a multicenter retrospective cohort study
Jonathon Spanyer, Lauren A. Barber, Harrison Lands, Alexander Brown, Mary Bouxsein, Marilyn Heng, Madhusudhan Yakkanti
JBMR Plus.2021;[Epub] CrossRef
 Cite
CiteA Comparison of Quality of Life Using Short Form 36 between Femoral Shaft Fracture and Tibia Shaft Fracture Treated with Antegrade Nailing
A Comparison of Quality of Life Using Short Form 36 between Femoral Shaft Fracture and Tibia Shaft Fracture Treated with Antegrade Nailing
Epidemiologic Characteristics of Populations
Values are presented as mean±standard deviation (range), number, or mean±standard deviation only. *p<0.05. G1: Patients of femoral shaft fractures treated with intramedullary nail, G2: Patients of tibial shaft fractures treated with intramedullary nail.
AO/OTA Classification of Populations
G1: Patients of femoral shaft fractures treated with intramedullary nail, G2: Patients of tibial shaft fractures treated with intramedullary nail, A1: Spiral fracture, A2: Oblique fracture, A3: Transverse fracture.
Results of Functional Outcomes
Values are presented as mean±standard deviation. *p<0.05. G1: Patients of femoral shaft fractures treated with intramedullary nail, G2: Patients of tibial shaft fractures treated with intramedullary nail, PCS: Physical component score in Short Form 36 (SF-36), PF: Physical functioning, RP: Role limitation due to physical health problems, BP: Bodily pain, GH: General health perception, MCS: Mental component score in SF-36, VT: Vitality, SF: Social functioning, RE: Role limitation due to emotional problems, MH: Mental health.
Table 1
Epidemiologic Characteristics of Populations
Values are presented as mean±standard deviation (range), number, or mean±standard deviation only. *p<0.05. G1: Patients of femoral shaft fractures treated with intramedullary nail, G2: Patients of tibial shaft fractures treated with intramedullary nail.
Table 2
AO/OTA Classification of Populations
G1: Patients of femoral shaft fractures treated with intramedullary nail, G2: Patients of tibial shaft fractures treated with intramedullary nail, A1: Spiral fracture, A2: Oblique fracture, A3: Transverse fracture.
Table 3
Results of Functional Outcomes
Values are presented as mean±standard deviation. *p<0.05. G1: Patients of femoral shaft fractures treated with intramedullary nail, G2: Patients of tibial shaft fractures treated with intramedullary nail, PCS: Physical component score in Short Form 36 (SF-36), PF: Physical functioning, RP: Role limitation due to physical health problems, BP: Bodily pain, GH: General health perception, MCS: Mental component score in SF-36, VT: Vitality, SF: Social functioning, RE: Role limitation due to emotional problems, MH: Mental health.

