 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 28(3); 2015 > Article
-
Original Article
- Additional Hinged External Fixation in Complex Elbow Injury
- Tong-Joo Lee, M.D., Ph.D., Taek Ho Hong, M.D., Nak Chul Kim, M.D.
-
Journal of the Korean Fracture Society 2015;28(3):169-177.
DOI: https://doi.org/10.12671/jkfs.2015.28.3.169
Published online: July 22, 2015
Department of Orthopedic Surgery, Inha University School of Medicine, Incheon, Korea.
- Address reprint requests to: Tong-Joo Lee, M.D., Ph.D. Department of Orthopedic Surgery, Inha University Hospital, 27 Inhang-ro, Jung-gu, Incheon 400-711, Korea. Tel: 82-32-890-3043, Fax: 82-32-890-3047, TJLEE@inha.ac.kr
• Received: January 11, 2015 • Revised: April 8, 2015 • Accepted: May 19, 2015
Copyright © 2015 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 751 Views
- 2 Download
Abstract
-
Purpose
- The purpose of this study was to evaluate the use of hinged external fixation in management of complex elbow injury.
-
Materials and Methods
- We retrospectively reviewed clinical outcomes in 10 patients with elbow dislocation and associated fractures of both the radial head and the coronoid process from January 2007 to December 2013. All ten patients were treated by hinged external fixation after open reduction and internal fixation. The indication for use of a hinged external fixator was persistent instability after fixation of the fractures. Early mobilization was started at 1 week (6.5 days) after surgery. The external fixator was removed at 6 weeks after surgery. Cassebaum classification and Mayo elbow performance score were used for clinical and functional evaluation. The follow-up period was at least 1 year.
-
Results
- At the last follow-up, the average further flexion was 127°, and the average flexion contracture was 16°. The average pronation was 83° and the average supination was 78°. By the Cassebaum classification after 1 year follow-up, patients were classified as 4 excellent, 4 good, and 2 poor. According to the Mayo elbow performance score, the average score was 87 points (65-100 points) with 3 excellent, 6 good, and 1 fair. Stability was restored in all patients at the last follow-up. There was no case of nonunion and the average union period was 11.5 weeks.
-
Conclusion
- This study advocated the additional use of a hinged external fixator in the treatment of complex elbow instability, especially when fixation of fractures and repair of soft tissues were not sufficient. Providing adequate stability and allowing early motion, additional external fixation could improve the functional outcome.
- 1. Josefsson PO, Gentz CF, Johnell O, Wendeberg B. Dislocations of the elbow and intraarticular fractures. Clin Orthop Relat Res, 1989;(246):126-130.Article
- 2. Ball CM, Galatz LM, Yamaguchi K. Elbow instability: treatment strategies and emerging concepts. Instr Course Lect, 2002;51:53-61.
- 3. Broberg MA, Morrey BF. Results of treatment of fracture-dislocations of the elbow. Clin Orthop Relat Res, 1987;(216):109-119.Article
- 4. Zilkens C, Graf M, Anastasiadis A, Smajic S, Muhr G, Kälicke T. Treatment of acute and chronic elbow instability with a hinged external fixator after fracture dislocation. Acta Orthop Belg, 2009;75:167-174.
- 5. McKee MD, Bowden SH, King GJ, et al. Management of recurrent, complex instability of the elbow with a hinged external fixator. J Bone Joint Surg Br, 1998;80:1031-1036.ArticlePDF
- 6. Pugh DM, Wild LM, Schemitsch EH, King GJ, McKee MD. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am, 2004;86-A:1122-1130.Article
- 7. Papandrea RF, Morrey BF, O'Driscoll SW. Reconstruction for persistent instability of the elbow after coronoid fracture-dislocation. J Shoulder Elbow Surg, 2007;16:68-77.Article
- 8. Ring D, Hannouche D, Jupiter JB. Surgical treatment of persistent dislocation or subluxation of the ulnohumeral joint after fracture-dislocation of the elbow. J Hand Surg Am, 2004;29:470-480.Article
- 9. Kälicke T, Westhoff J, Wingenfeld C, Muhr G, Arens S. Fracture dislocation of the elbow involving the coronoid process. Unfallchirurg, 2003;106:300-305.
- 10. Berendes S, Zilkens C, Anastasiadis A, Graf M, Muhr G, Kalicke T. Additional external hinged fixator after open repositioning and internal fixation of acute elbow instability in non-compliant patients. Orthop Rev (Pavia), 2010;2:e21.
- 11. Stavlas P, Gliatis J, Polyzois V, Polyzois D. Unilateral hinged external fixator of the elbow in complex elbow injuries. Injury, 2004;35:1158-1166.Article
- 12. Rettig AC. Traumatic elbow injuries in the athlete. Orthop Clin North Am, 2002;33:509-522.Article
- 13. Kim BS, Kim YB. Hinged elbow fixation for persistent instability following complex elbow fracture dislocation. J Korean Soc Surg Hand, 2007;12:120-124.
- 14. Madey SM, Bottlang M, Steyers CM, Marsh JL, Brown TD. Hinged external fixation of the elbow: optimal axis alignment to minimize motion resistance. J Orthop Trauma, 2000;14:41-47.Article
- 15. King GJ, Zarzour ZD, Rath DA, Dunning CE, Patterson SD, Johnson JA. Metallic radial head arthroplasty improves valgus stability of the elbow. Clin Orthop Relat Res, 1999;(368):114-125.Article
- 16. Closkey RF, Goode JR, Kirschenbaum D, Cody RP. The role of the coronoid process in elbow stability. A biomechanical analysis of axial loading. J Bone Joint Surg Am, 2000;82-A:1749-1753.
- 17. Chemama B, Bonnevialle N, Peter O, Mansat P, Bonnevialle P. Terrible triad injury of the elbow: how to improve outcomes? Orthop Traumatol Surg Res, 2010;96:147-154.Article
REFERENCES
Fig. 1

A 33-year-old male, initial radiographs and computed tomography showed fracture of the radial head, coronoid process and olecranon process of ulna, and elbow dislocation. Postoperative radiographs show resection arthroplasty for radial head fracture, circlage wiringfor coronoid process fracture, and tension band wiring for olecranon process fractures and hinged external fixation for elbow instability. (A) Preoperative elbow anteroposterior (AP) image. (B) Preoperative elbow lateral image. (C) Preoperative 3-dimensional computed tomography image. (D) Postoperative elbow AP image. (E) Postoperative elbow lateral image.
Fig. 2

A 65-year-old male, initial radiographs and computed tomography showed fracture of the radial head, coronoid process and elbow dislocation. Postoperative radiographs show fragment resection for the radial head fracture, screw fixation for coronoid process fracture, and hinged external fixation for elbow instability. (A) Preoperative elbow anteroposterior (AP) image. (B) Preoperative elbow lateral image. (C) Preoperative 3-dimensional elbow computed tomography image. (D) Postoperative elbow AP image. (E) Postoperative elbow lateral image.




Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteAdditional Hinged External Fixation in Complex Elbow Injury


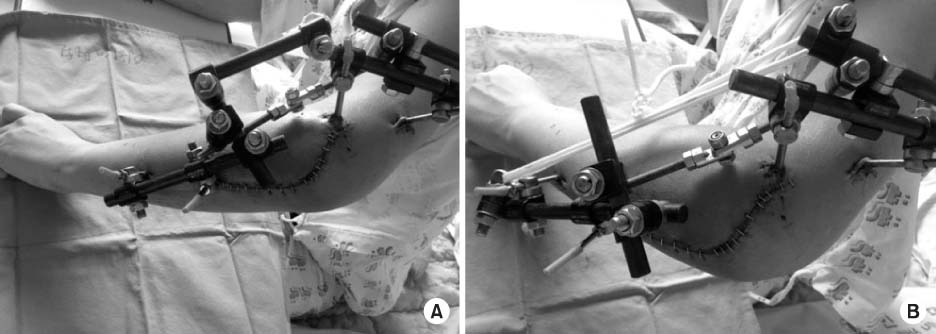
Fig. 1
A 33-year-old male, initial radiographs and computed tomography showed fracture of the radial head, coronoid process and olecranon process of ulna, and elbow dislocation. Postoperative radiographs show resection arthroplasty for radial head fracture, circlage wiringfor coronoid process fracture, and tension band wiring for olecranon process fractures and hinged external fixation for elbow instability. (A) Preoperative elbow anteroposterior (AP) image. (B) Preoperative elbow lateral image. (C) Preoperative 3-dimensional computed tomography image. (D) Postoperative elbow AP image. (E) Postoperative elbow lateral image.
Fig. 2
A 65-year-old male, initial radiographs and computed tomography showed fracture of the radial head, coronoid process and elbow dislocation. Postoperative radiographs show fragment resection for the radial head fracture, screw fixation for coronoid process fracture, and hinged external fixation for elbow instability. (A) Preoperative elbow anteroposterior (AP) image. (B) Preoperative elbow lateral image. (C) Preoperative 3-dimensional elbow computed tomography image. (D) Postoperative elbow AP image. (E) Postoperative elbow lateral image.
Fig. 3
(A) Postoperative photo with hinged external fixator. (B) After removal of a rod of the external fixator and loosening the hinge, patients started elbow joint movement. One week after surgery.
Fig. 1
Fig. 2
Fig. 3
Additional Hinged External Fixation in Complex Elbow Injury
Summary of Cases
R: Right, L: Left, M: Male, F: Female.
Cassebaum Classification for Elbow Range of Motion
Mayo Elbow Performance Score
Classification: Excellent >90; Good 75-89; Fair 60-74; Poor <60.
Table 1
Summary of Cases
R: Right, L: Left, M: Male, F: Female.
Table 2
Cassebaum Classification for Elbow Range of Motion
Table 3
Mayo Elbow Performance Score
Classification: Excellent >90; Good 75-89; Fair 60-74; Poor <60.

