 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 26(3); 2013 > Article
-
Review Article
- Anatomy, Classification and Radiology of the Pelvic Fracture
- Jae Min Ahn, M.D., Jeung Tak Suh, M.D., Ph.D.
-
Journal of the Korean Fracture Society 2013;26(3):221-229.
DOI: https://doi.org/10.12671/jkfs.2013.26.3.221
Published online: July 15, 2013
*Department of Orthopaedic Surgery, Pusan National University Hospital, Busan, Korea.
†Pusan National University Hospital Trauma Center, Busan, Korea.
- Address reprint requests to: Jae Min Ahn, M.D. Department of Orthopaedic Surgery, Pusan National University Hospital, 179 Gudeok-ro, Seo-gu, Busan 602-739, Korea. Tel: 82-51-240-7248, Fax: 82-51-247-8395, osahnjaemin@pusan.ac.kr
Copyright © 2013 The Korean Fracture Society. All rights reserved.
This is anOpen Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,176 Views
- 91 Download
- 2 Crossref
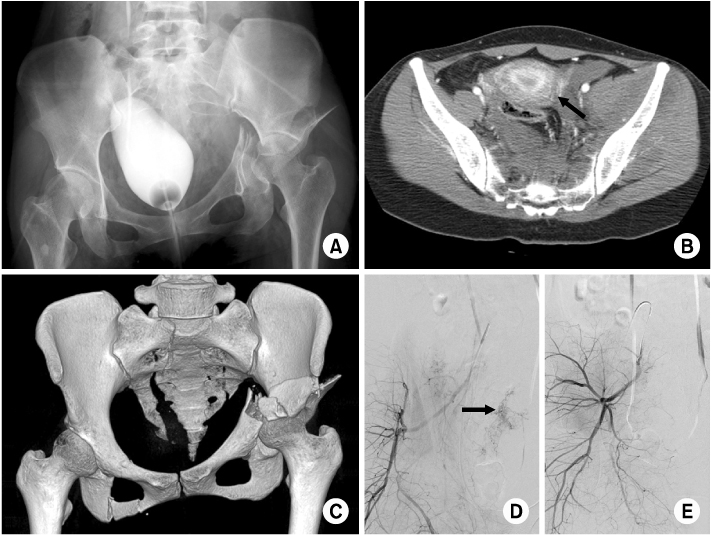
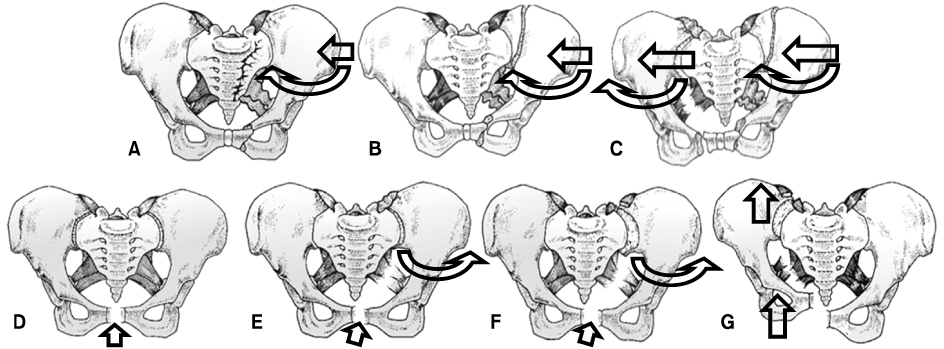
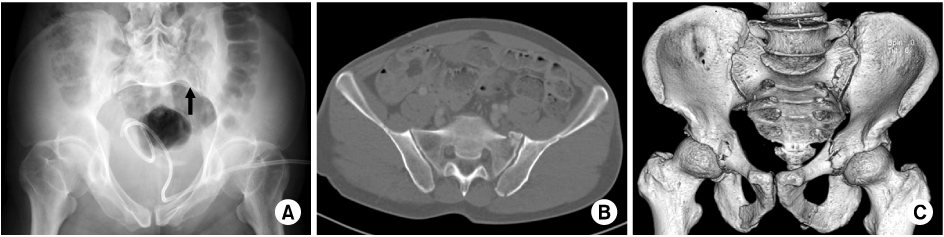
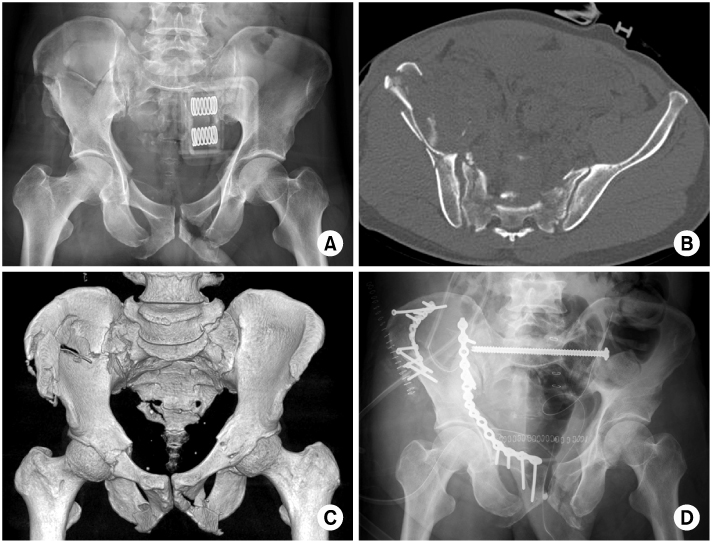
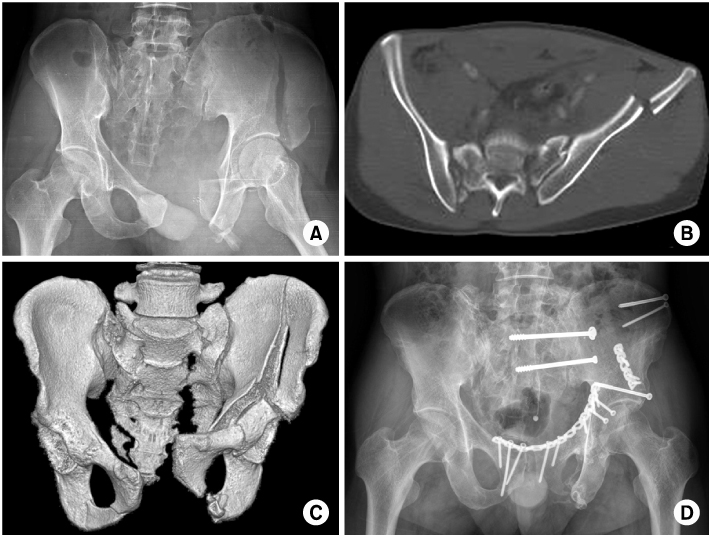
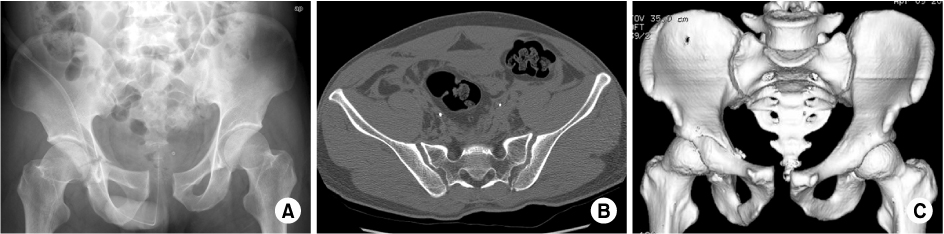
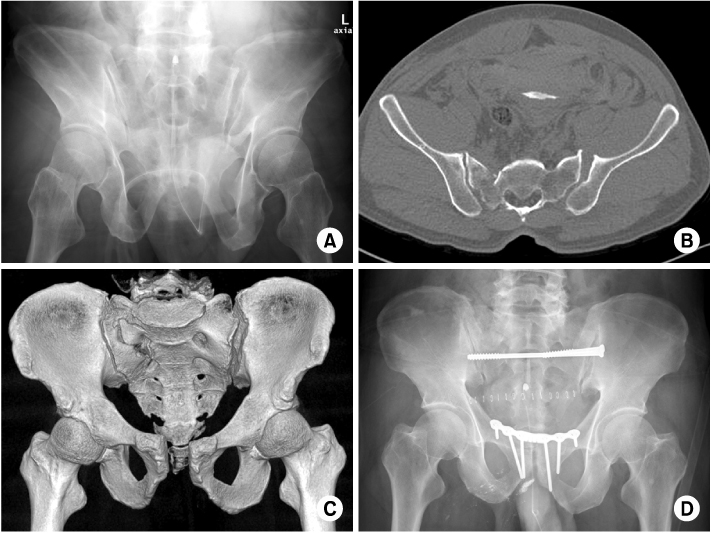

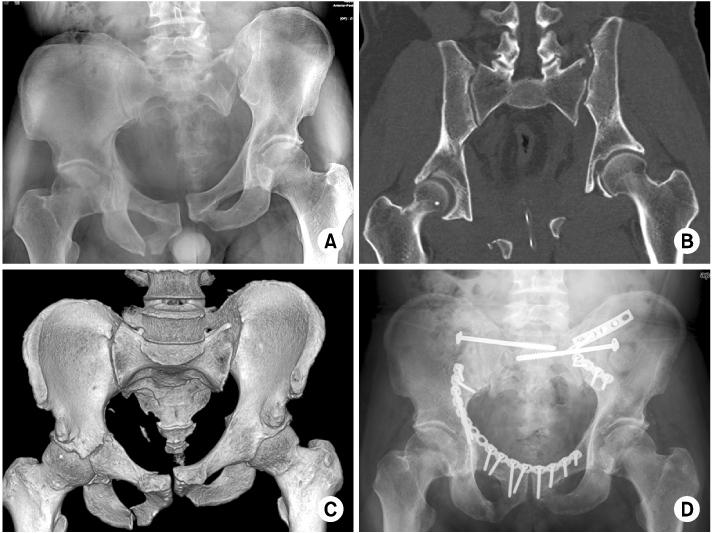
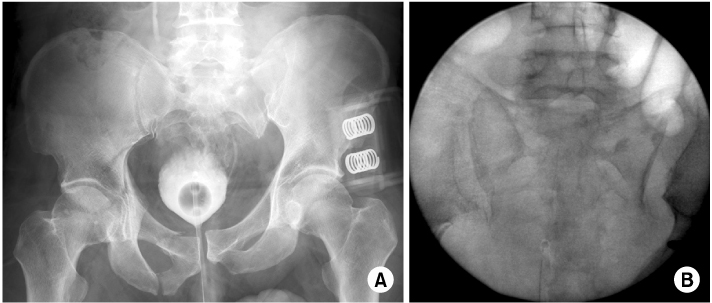
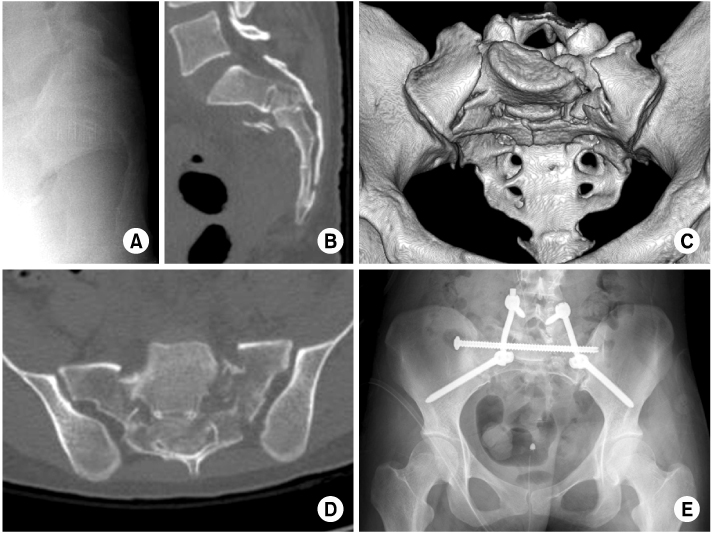
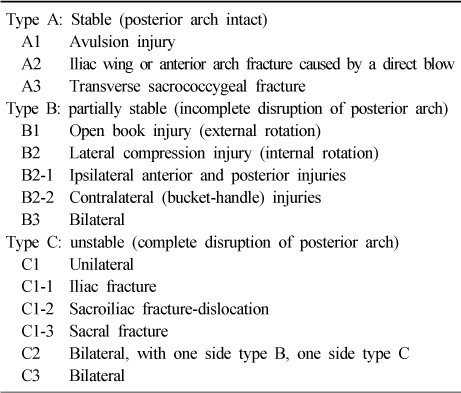
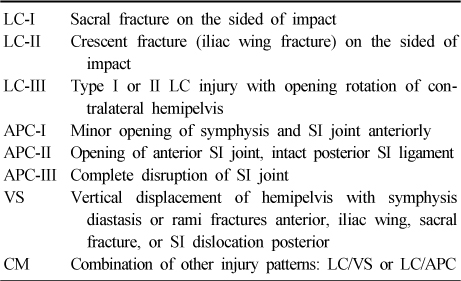
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Radiostereometric Analysis Allows Assessment of the Stability and Inducible Displacement of Pelvic Ring Disruptions during Healing: A Case Series
Andreas Ladurner, Stuart A. Callary, Aniruddha Mitra, Mark Rickman, Dominic Thewlis, Lucian B. Solomon
Journal of Clinical Medicine.2020; 9(11): 3411. CrossRef - Case Report of a Pelvic Pain Patient with Pubic Fracture Caused by Traffic Accident
Ji-Hyun Lee, Mi-Hwa Song, Chang-Min Choi
The Journal of Oriental Obstetrics and Gynecology.2015; 28(4): 88. CrossRef
 Cite
CiteAnatomy, Classification and Radiology of the Pelvic Fracture
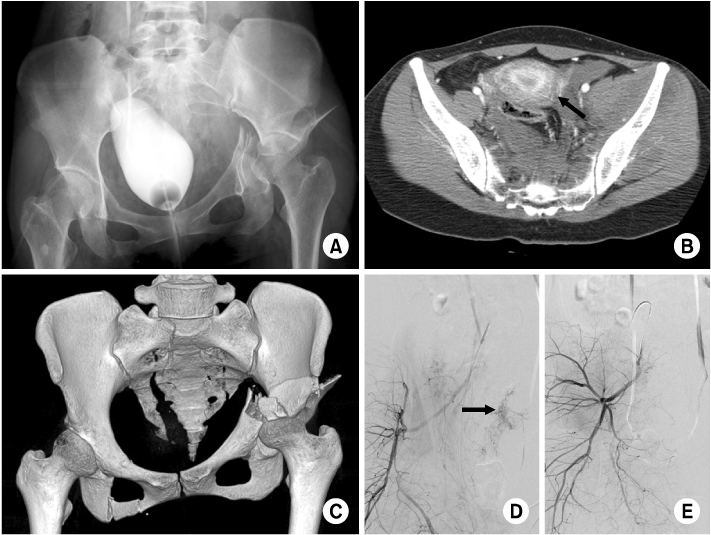
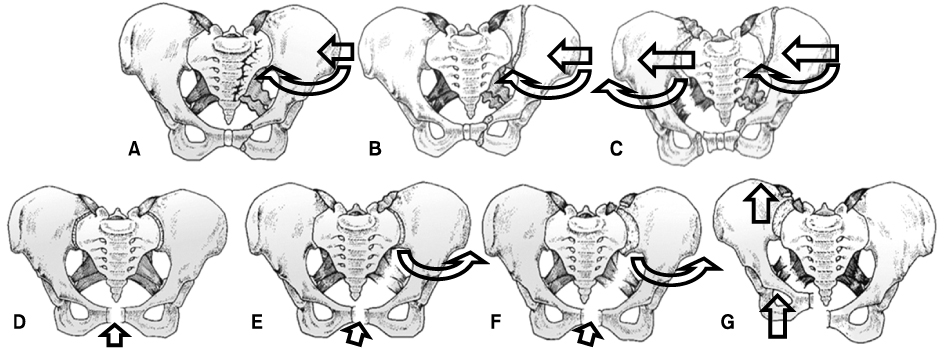

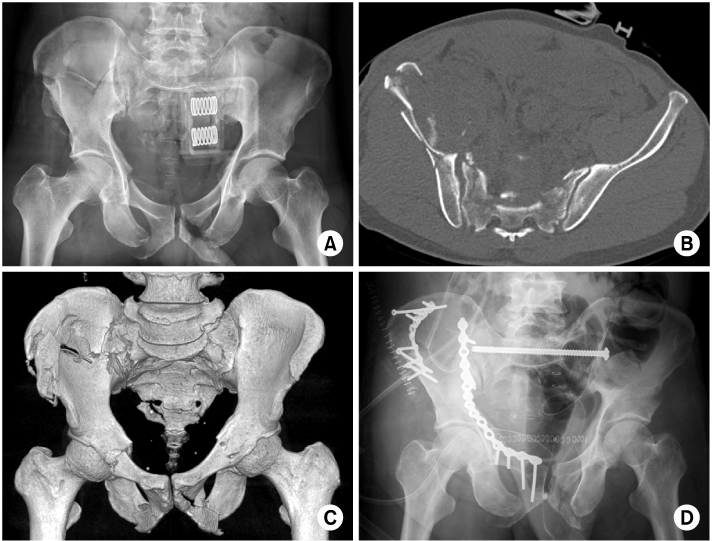
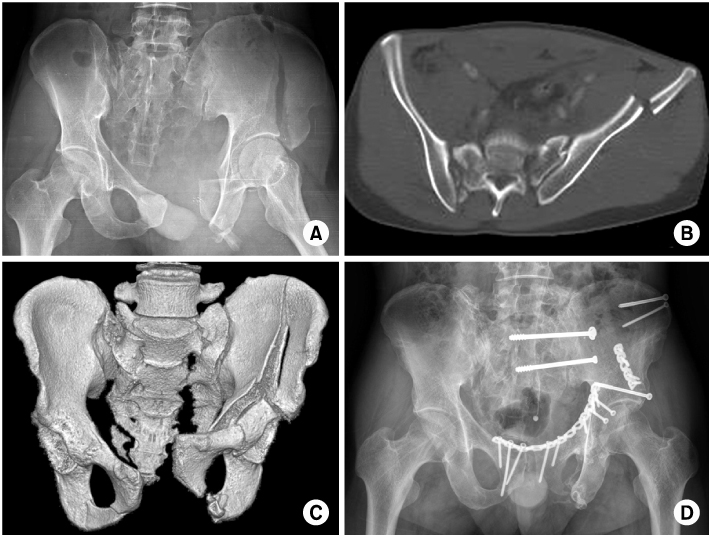
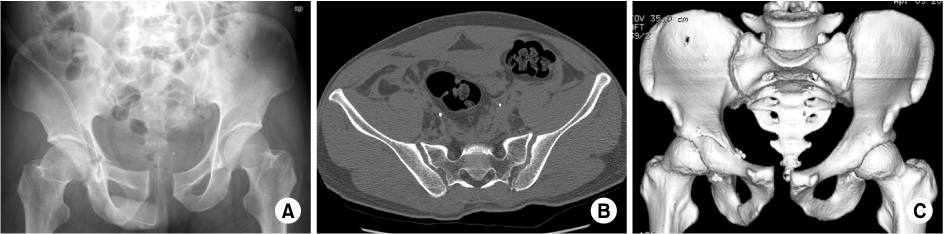
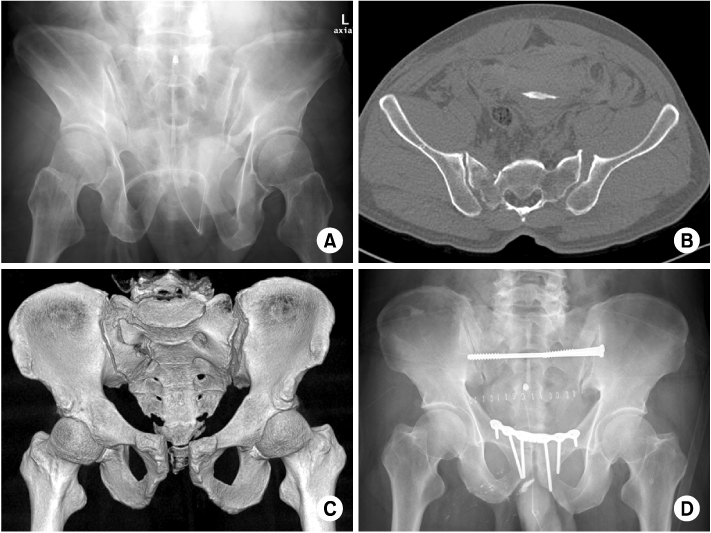

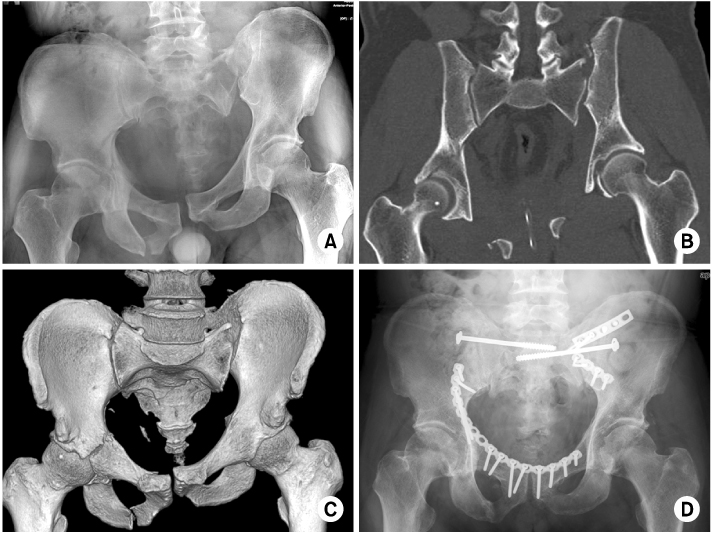
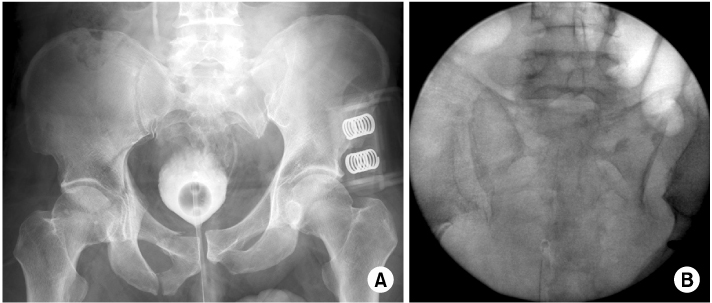
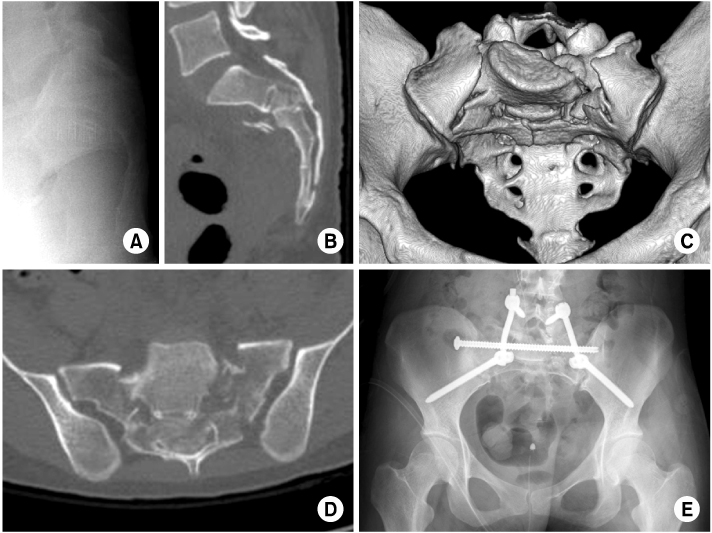
Fig. 1
Initial pelvis anteroposterior radiographs (A) of the hemodynamic unstable patient shows left acetabular fracture with a space occupying lesion on the left pelvic cavity. Axial image of the enhanced computed tomography (CT) scan (B) shows hematoma with active bleeding (arrow). Three-dimensional image of the CT scan (C) shows both transforaminal sacral fractures with left acetabular fracture. Fluoroscopic view of conventional angiography (D) shows active dye staining (arrow) on the branches of the internal iliac artery. Fluoroscopic image after angiographic embolization (E) shows significant decrease of active dye staining.
Fig. 2
Illustrations of the Young-Burgess classification of pelvic fractures2). (A) LC-I, (B) LC-II, (C) LC-III, (D) APC-I, (E) APC-II, (F) APC-III, (G) VS. The arrows in each illustration indicates the direction of impact force and direction of hemipelvis rotation or displacement. LC: Lateral compression, APC: Anteroposterior compression, VS: Vertical shear.
Fig. 3
Pelvis inlet radiograph (A), computed tomography (CT) scan axial image (B), three-dimensional image (C) of a LC-I pelvic injury show anterior compression fracture of left sacral ala with both pubic rami fractures. The arrow indicates sacral alar fracture. LC: Lateral compression.
Fig. 4
Preoperative pelvis anteroposterior radiograph (A), computed tomography scan axial image (B) and three-dimensional image (C) of a LC-II pelvic injury show SI joint fracture-dislocation and pubic rami fractures. Postoperative radiograph (D) shows anterior and posterior pelvic ring fixation. LC: Lateral compression, SI: Sacroiliac.
Fig. 5
Preoperative pelvis anteroposterior radiograph (A), computed tomography scan axial image (B) and three-dimensional image (C) of a LC-III pelvic injury show internal rotation of the right hemipelvis, right sacral compression fracture, external rotation of the left hemipelvis, left sacral transforaminal fracture with gap, symphysis diastasis and left acetabular anterior wall and column fractures. Radiograph two years after operation (D) show healed stable pelvis with anterior and posterior pelvic ring fixation. LC: Lateral compression.
Fig. 6
Pelvis anteroposterior radiograph (A), computed tomography scan axial image (B) and three-dimensional image (C) of an APC-I pelvic injury show mild diastasis of symphysis, but intact both SI joint with right undisplaced transvers acetabular fracture. APC: Anteroposterior compression, SI: Sacroiliac.
Fig. 7
Preoperative pelvis outlet radiograph (A), computed tomography scan axial image (B) and three-dimensional image (C) of an APC-II pelvic injury show diastasis of symphysis with opening of the left anterior SI joint, but intact gap of posterior SI joint. Postoperative radiograph (D) shows anterior plating of symphysis with posterior fixation with S2 iliosacral screw fixation due to sacral dysmorphism. APC: Anteroposterior compression, SI: Sacroiliac.
Fig. 8
Preoperative pelvis anteroposterior radiograph (A), computed tomography scan axial image (B) and three-dimensional image (C) of an APC-III injury of the right hemipelvis show severe external rotation of the right hemipelvis with SI joint fracture-dislocation, wide diastasis of symphysis with perineal injury and a VS type injury of the left hemipelvis. Postoperative radiograph (D) shows anterior plating of the right SI joint and iliosacral screw fixation of the left SI joint with supraacetabular external fixator pins. APC: Anteroposterior compression, SI: Sacroiliac, VS: Vertical shear.
Fig. 9
Preoperative pelvis anteroposterior radiograph (A), computed tomography scan coronal image (B) and three-dimensional image (C) of a VS type pelvic injury show cephalic displacement of the left hemipelvis with avulsion fracture of the fifth lumbar transverse process as well as right pubic rami fractures with acetabular transverse fracture. Radiograph of six months after operation (D) shows healed stable pelvis with anterior and posterior pelvic ring fixation. VS: Vertical shear.
Fig. 10
Initial pelvic anteroposterior radiograph (A) of the hemodynamic unstable patient with pelvic belt shows a VS type injury of the left SI joint, but normal gap of the right SI joint. Intra-operative image of C-arm fluoroscopy (B) shows opening of the right SI joint with complete disruption of the left SI joint. VS: Vertical shear, SI: Sacroiliac.
Fig. 11
Preoperative sacrum lateral radiograph (A) shows nonspecific findings, but the computed tomography (CT) scan coronal image (B) shows S2 transverse and compression fracture with mild flexion deformity. CT scan three-dimensional image (C) shows a U-shape sacral jumper's fracture with coronal fracture of S1 body. CT scan axial image (D) shows complete obliteration of sacral canal by displaced fracture fragment. Postoperative radiograph (E) shows rigid lumbopelvic fixation with trans-sacral iliosacral screw fixation.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Fig. 9
Fig. 10
Fig. 11
Anatomy, Classification and Radiology of the Pelvic Fracture
Table 1
Tile Classification of Pelvic Ring Lesions23)
Table 2
Young and Burgess Pelvic Fracture Classification3,25)
LC: Lateral compression, APC: Anteroposterior compression, VS: Vertical shear, CM: Combined mechanism, SI: Sacroiliac.

