 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 23(4); 2010 > Article
-
Review Article
- Surgical Treatment of Common Osteoporotic Fracture: Distal Radius
- Jong Woong Park, M.D., Ph.D.
-
Journal of the Korean Fracture Society 2010;23(4):391-398.
DOI: https://doi.org/10.12671/jkfs.2010.23.4.391
Published online: October 31, 2010
- Address reprint requests to: Jong Woong Park, M.D., Ph.D. Department of Orthopaedic Surgery, Ansan Hospital, Korea University College of Medicine, 516, Gojan-1-dong, Danwon-gu, Ansan 425-707, Korea. Tel: 82-31-412-6583, Fax: 82-31-412-5549, ospark@korea.ac.kr
Copyright © 2010 The Korean Fracture Society
- 1,551 Views
- 5 Download
- 3 Crossref


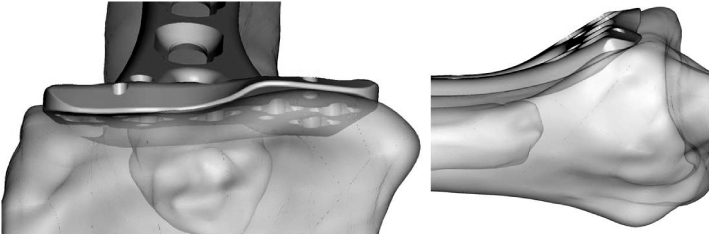

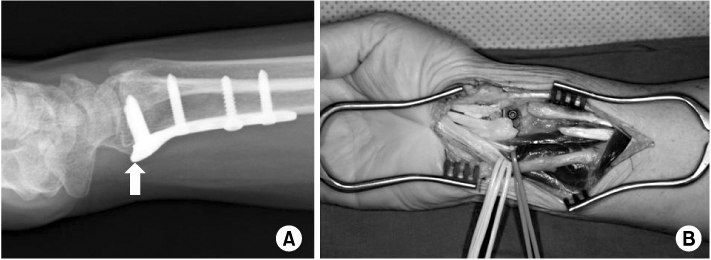
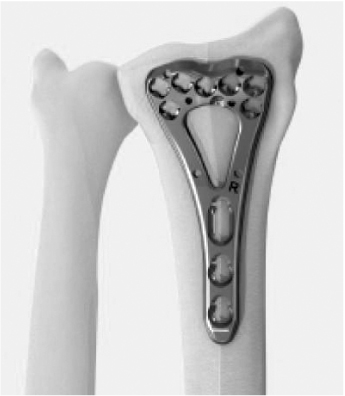
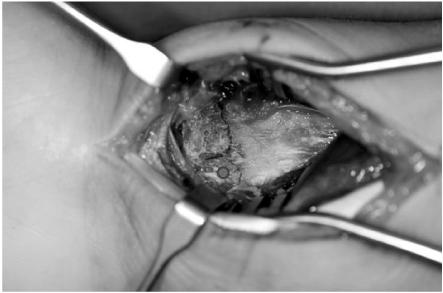
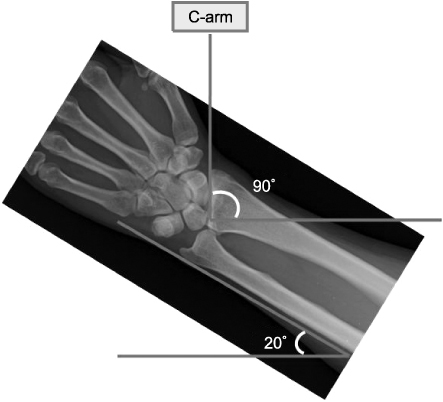



Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Is dorsal cortex drilling necessary for distal radius fractures treated with a volar locking plate? A comparative study of near-cortex-only and far-cortex drilling
Chul Hong Kim, Sung Yoon Jung, Hyeon Jun Kim, Si-Hyun Park
Journal of Trauma and Injury.2025; 38(3): 248. CrossRef - Functional Outcomes of Percutaneous K-Wire Fixation for Distal Radius Fractures with or without Osteoporosis
Ki-Chan An, Gyu-Min Kong, Jang-Seok Choi, Hi-Chul Gwak, Joo-Yong Kim, Sung-Yub Jin
Journal of the Korean Fracture Society.2013; 26(4): 248. CrossRef - Results of the Kapandji Procedure in the AO Type C Distal Radius Fracture in Patients over Age 60
Chul Hong Kim, Sung Soo Kim, Myung Jin Lee, Hyeon Jun Kim, Bo Kun Kim, Young Hoon Lim
Journal of the Korean Fracture Society.2012; 25(3): 191. CrossRef
 Cite
CiteSurgical Treatment of Common Osteoporotic Fracture: Distal Radius


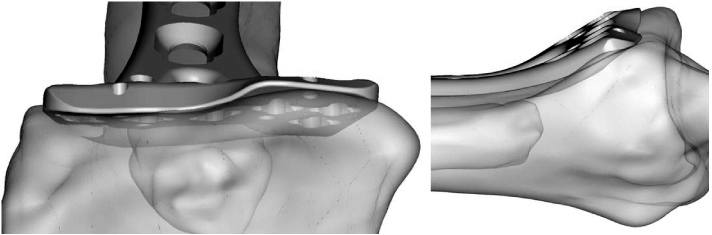

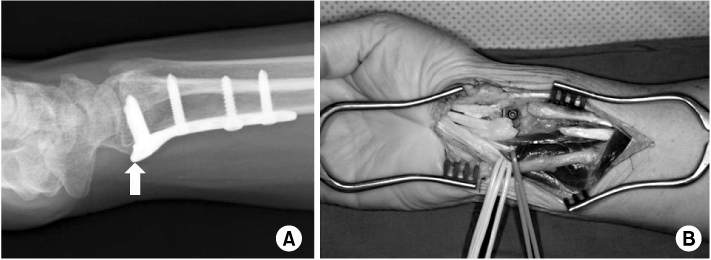
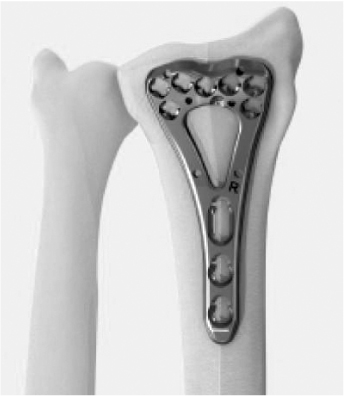
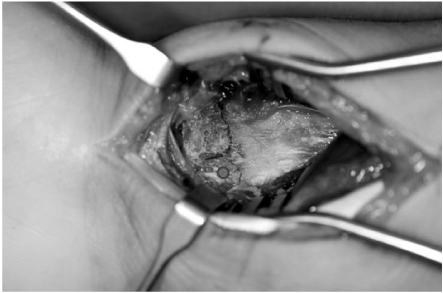
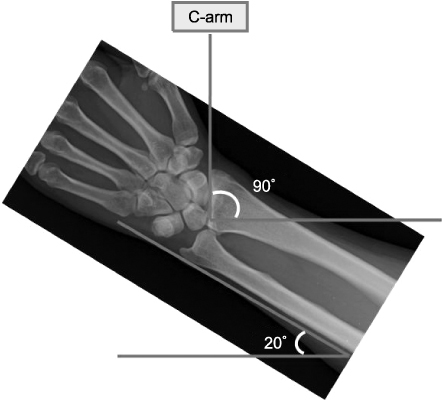



Fig. 1
K-wire fixation for the treatment of osteoporotic distal radius fracture. Increased risk of reduction loss and wire migration. Arrows show migrated K-wire with reduction loss of the fracture site.
Fig. 2
Locking plates provide improved fixability in fixation of the osteoporotic distal radius fracture.
(A) Variable angle locking plate (VA-LCP, Synthes®).
(B) Fixed angle locking plate (Aculoc, Acumed®).
Fig. 3
Advanced design of a locking plate shows low profile and meets well with the anatomy of the distal radius.
Fig. 4
Protruded radial limb of the previously used locking plate irritates skin. An arrow shows protruded edge of the plate.
Fig. 5
(A) Too much distal positioning of the plate irritates flexor tendons. An arrow indicates too distally positioned plate over the 'watershed line'. (B) Flexor tendon ruptures due to attrition by the plate end.
Fig. 6
Anatomically precontoured design of the newly developed plate allows better fitting on the volar surface of the distal radius.
Fig. 7
Sufficient exposure is important to see the intermediate column. A dot indicates an intermediate column of the distal radius.
Fig. 8
A true lateral view (articular view) is mandatory during insertion of the distal locking screws. 20 degrees of inclination of the wrist joint usually makes a true lateral view under the C-arm.
Fig. 9
Volar locking plate fixation for the distal radius fracture.
Fig. 10
Multidimentional columnar locking plate fixation for the distal radius fracture.
Fig. 11
2.0 mm small locking plate provides sufficient stability for the comminuted distal ulna fracture.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Fig. 9
Fig. 10
Fig. 11
Surgical Treatment of Common Osteoporotic Fracture: Distal Radius

