 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > > Ahead-of print articles > Article
-
Original Article
- Open reduction and internal fixation for distal humerus fractures in older adults: a retrospective comparative study by osteoporosis status
-
Tong Joo Lee
 , Hee Beom Shin, Yongseok Lee
, Hee Beom Shin, Yongseok Lee -
DOI: https://doi.org/10.12671/jmt.2026.00101
Published online: July 15, 2026
Department of Orthopedic Surgery, Inha University Hospital, Incheon, Korea
- Correspondence to: Tong Joo Lee Department of Orthopedic Surgery, Inha University Hospital, Incheon 22332, Korea Tel: +82-32-890-3662 Email: TJLee@inha.ac.kr
• Received: February 15, 2026 • Revised: May 6, 2026 • Accepted: May 11, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 13 Views
- 1 Download
Abstract
-
Background Distal humerus fractures in older patients, particularly those with osteoporosis, pose substantial treatment challenges because of increased fracture complexity and compromised bone stock. Open reduction and internal fixation (ORIF) is the preferred treatment but may be complicated by fixation failure. This study investigated the outcomes of ORIF in older osteoporotic and nonosteoporotic patients with complete articular distal humerus fractures.
-
Methods This retrospective study included 19 patients with Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA) 13C distal humerus fractures who underwent surgical treatment between 2012 and 2024. The mean patient age was 79.1 years. Patients were divided into osteoporotic (n=11) and nonosteoporotic (n=8) groups based on the lowest recorded dual-energy X-ray absorptiometry T-score at the femoral neck or lumbar spine. Osteoporosis was defined as a T-score of −2.5 or lower, and the nonosteoporotic group included patients with osteopenia. All fractures were treated with ORIF using bicolumnar plating. All included patients completed 12 months of clinical follow-up for visual analog scale (VAS) and Mayo Elbow Performance Score (MEPS) assessments. Radiographic follow-up was recorded separately and continued until union was confirmed; imaging follow-up extended to 12 months or longer in 14 patients and was limited to 6 months in five asymptomatic patients after confirmed union.
-
Results Both groups showed significant within-group improvement in pain, as assessed using the VAS, and function, as assessed using the MEPS, over time. Between-group comparisons at each follow-up time point showed no statistically significant differences in VAS or MEPS. No radiographic nonunion was observed during the available imaging follow-up, and complications were limited to one case of screw pullout/loosening and one case of postoperative stiffness.
-
Conclusion ORIF provides reliable outcomes for older patients with complex distal humerus fractures, regardless of osteoporosis status, when stable reconstruction is achievable. These findings suggest that ORIF remains a viable treatment option, with satisfactory functional recovery and low complication rates in this population.
-
Level of evidence III.
Introduction
Distal humerus fractures are relatively uncommon, accounting for approximately 1%–2% of adult fractures, yet they can result in substantial functional impairment because elbow stiffness and pain may markedly limit activities of daily living (ADL)—especially in older patients [1,2]. These injuries show a bimodal distribution, with high-energy trauma predominating in younger patients and low-energy falls predominating in older, often osteoporotic patients; consequently, the incidence of distal humerus fractures in the geriatric population is expected to rise as the population ages [1,2]. Complete articular fractures (Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association [AO/OTA] type 13C) are frequently encountered in elderly patients and are commonly associated with severe intra-articular comminution and compromised bone stock, making stable reconstruction particularly challenging [1,3]. As osteoporosis is highly prevalent among older adults, particularly in women, the burden of fragility fractures in the elderly population has been steadily increasing [4].
Importantly, osteoporosis appears not only to increase fracture complexity but also to adversely influence fixation outcomes. In a multicenter study of patients >65 years treated with plate fixation for distal humerus fractures, osteoporosis was identified as the main predictor of failure, increasing the risk of combined clinical and radiological failure regardless of the construct or hardware used [5]. Open reduction and internal fixation (ORIF) with bicolumnar plating remains a principal reconstructive strategy for intra-articular distal humerus fractures, aiming to restore the articular surface and provide sufficient stability to permit early motion [1,2]. With contemporary anatomic locking plate constructs, ORIF for AO/OTA 13C fractures in older adults has been reported to yield satisfactory patient-reported outcomes (Oxford Elbow Score, Mayo Elbow Performance Score [MEPS], and Quick Disabilities of the Arm, Shoulder and Hand [Quick DASH]), although revision surgery remains a relevant concern [3]. Nevertheless, even with modern implants, complex complete articular fractures continue to be associated with complications such as fixation failure or nonunion, reflecting the inherent severity of intra-articular comminution in osteoporotic bone [1,5].
Total elbow arthroplasty (TEA) has also been advocated as an alternative primary option for selected elderly patients with highly comminuted or “unreconstructible” distal humerus fractures [1,2]. Good to excellent short-term clinical results after primary TEA have been reported in elderly Asian patients with distal humerus fractures, and some authors have suggested that arthroplasty may provide more predictable early outcomes than ORIF in carefully selected patients; however, the optimal strategy remains debated [6,7].
A comparative systematic review and meta-analysis of elderly distal humerus fractures reported that while TEA may yield a greater flexion-extension arc and lower rates of reoperation and postoperative stiffness, functional outcome scores (e.g., MEPS and DASH) were overall similar between ORIF and TEA [2,8]. Evidence stratified by osteoporosis status in elderly patients undergoing ORIF for complete articular distal humerus fractures remains scarce. Therefore, the purpose of the present study was to compare the radiographic and clinical outcomes of ORIF between osteoporotic and nonosteoporotic elderly patients [2,3].
Methods
The study was approved by the Institutional Review Board (IRB) of Inha University Hospital (IRB No. 2025-08-001-000) and performed in accordance with the principles of the Declaration of Helsinki. The need for written informed consent was waived because of its retrospective design by the IRB.
This retrospective study was conducted at Inha University Hospital and included 19 patients who underwent ORIF for complete articular distal humerus fractures (AO/OTA 13C) after low-energy falls between 2012 and 2024. All surgeries were performed by a single experienced surgeon, who maintained consistent surgical principles, exposure strategy, and bicolumnar fixation concept throughout the study period, although minor temporal changes in implants or perioperative care may still have occurred.
The cohort consisted of five males and 14 females, with a mean age of 79.1 years at the time of injury.
All fractures were classified as AO/OTA 13C type, representing complex distal humeral fractures. Inclusion criteria were age ≥75 years, AO/OTA 13C distal humerus fracture, treatment with ORIF, and availability of at least 12 months of clinical follow-up for VAS and MEPS assessment. Exclusion criteria were patients managed nonoperatively, patients treated with strategies other than ORIF, fracture patterns other than AO/OTA 13C (including extra-articular fractures), and cases without at least 12 months of clinical follow-up.
Treatment-selection bias cannot be excluded because the analysis was restricted to ORIF-treated cases deemed suitable for reconstruction.
Group classification was based on the lowest recorded dual-energy X-ray absorptiometry T-score at the femoral neck or lumbar spine. Osteoporosis was defined as a T-score of –2.5 or lower at either site, whereas nonosteoporotic status was defined as a T-score greater than –2.5; therefore, the nonosteoporotic group included patients with osteopenia.
Union was defined as progressive reduction of the fracture gap and evidence of osteogenesis with cortical continuity or bridging trabecular bone across the fracture site on serial radiographs compared with prior images, together with maintained alignment. Nonunion was defined as absence of progressive healing on serial radiographs, persistent fracture gap or implant-related instability, or the need for additional surgery because of failure of union. Radiographs and postoperative complications were assessed by the treating surgeon during outpatient follow-up and were reviewed retrospectively from the stored images and clinical records.
Clinical evaluations were conducted at approximately 3 months, 6 months, and 12 months, and functional outcomes, including the MEPS, VAS, and range of motion (ROM), were reviewed. In this study, the minimum follow-up criterion referred to clinical follow-up: all included patients completed clinical follow-up through 12 months for VAS and MEPS assessment.
Radiographic evaluation was performed with serial anteroposterior and lateral elbow radiographs to assess fracture healing, alignment, and complications. In clinically asymptomatic patients in whom union had already been confirmed, further radiographic follow-up was not routinely continued; accordingly, radiographic follow-up was limited to 6 months in five patients, whereas the remaining patients had radiographic follow-up to 12 months or longer (up to 3 years).
Statistical analysis was performed using Python ver. 3.6.2 (Python Software Foundation). Continuous variables were expressed as mean±standard deviation, and categorical variables were presented as frequencies and percentages. Within-group changes over time were assessed using Friedman tests followed by Wilcoxon signed-rank tests with Bonferroni correction. Between-group comparisons at each time point were performed using Mann-Whitney U tests, and a P<0.05 was considered statistically significant.
Postoperatively, patients were initially placed in a posterior long-arm splint to immobilize the elbow joint and protect the surgical site for the first 2 weeks. After 2 weeks, the splint was removed, stitch removal was performed, and a hinged elbow brace was applied to control the ROM within a safe arc. This brace was maintained for an additional 2 weeks to allow for controlled early motion. From 1 month postoperatively, passive ROM exercises were initiated to prevent stiffness and promote joint mobility. Initially, these exercises were passive, and patients were encouraged to perform them under the guidance of a trained physical therapist. After 3 months, patients were gradually allowed to return to ADL, with increasing levels of strength and functional activity. At this point, the rehabilitation protocol transitioned from passive ROM exercises to active exercises aimed at strengthening the elbow and regaining full function. Throughout the rehabilitation process, patients were monitored closely to ensure appropriate healing, and the therapy was adjusted based on individual progress and complications.
Results
Nineteen patients met the inclusion criteria, including 14 females (73.7%) and five males (26.3%). The mean age at injury was 79.1±3.9 years (range, 75–88 years). All injuries resulted from low-energy falls. All fractures were classified as complete articular distal humerus fractures (AO/OTA 13C). Fracture subtypes included 13C1 in eight patients (42.1%), 13C2 in five (26.3%), and 13C3 in six (31.6%). Patients were stratified into a nonosteoporotic group (n=8) and an osteoporotic group (n=11) based on bone mineral density (BMD). The osteoporotic group had a lower mean BMD T-score than the nonosteoporotic group (−3.29±0.71 vs. −1.24±0.48). All 19 patients completed clinical follow-up through 12 months for VAS and MEPS assessment. Radiographic follow-up was continued until union was confirmed; therefore, imaging follow-up was limited to 6 months in five asymptomatic patients after confirmed union and extended to 12 months or longer (up to 3 years) in 14 patients. Accordingly, any shorter follow-up duration shown in the demographic data refers to radiographic rather than clinical follow-up. Baseline characteristics are summarized in Table 1.
An olecranon osteotomy was performed to facilitate intra-articular exposure in 15/19 cases (78.9%), including 7/8 (87.5%) in the nonosteoporotic group and 8/11 (72.7%) in the osteoporotic group. A posterior approach without osteotomy was used in 4/19 cases (21.1%). All fractures were treated with ORIF using bicolumnar (dual-plate) constructs; parallel dual-plate fixation supplemented with cannulated screw fixation was documented in 13/19 patients (68.4%) [9-12].
Mean group trajectories for pain (VAS) and function (MEPS) are shown in Figs. 1 and 2, respectively. VAS scores decreased over time in both groups. In the nonosteoporotic group, mean VAS decreased from 3.38±0.74 at 3 months to 1.25±1.39 at 6 months and 0.62±1.41 at 12 months. In the osteoporotic group, mean VAS decreased from 4.64±1.96 at 3 months to 1.18±0.98 at 6 months and 0.18±0.40 at 12 months. Within-group improvement over time was statistically significant for both the nonosteoporotic group (Friedman P=0.0015) and the osteoporotic group (Friedman P<0.001). Post-hoc Wilcoxon signed-rank tests showed significant reductions from 3 to 6 months and from 3 to 12 months in both groups (Bonferroni-adjusted P<0.05); the 6- to 12-month interval did not reach significance in the nonosteoporotic group for VAS (Bonferroni-adjusted P=0.307).
MEPS increased over time in both groups. In the nonosteoporotic group, mean MEPS improved from 74.38±8.63 at 3 months to 83.12±5.94 at 6 months and 90.62±4.17 at 12 months. In the osteoporotic group, mean MEPS improved from 65.00±13.78 at 3 months to 83.18±8.15 at 6 months and 92.27±4.67 at 12 months. Within-group improvement over time was significant for both the nonosteoporotic group (Friedman P=0.00042) and the osteoporotic group (Friedman P<0.001). Post-hoc Wilcoxon signed-rank tests demonstrated significant improvements across all intervals for MEPS in both groups after Bonferroni correction (all adjusted P<0.05).
Between-group comparisons at each time point did not show statistically significant differences in VAS (3 months, P=0.124; 6 months, P=0.931; 12 months, P=0.684) or MEPS (3 months, P=0.102; 6 months, P=0.898; 12 months, P=0.295). Although the osteoporotic group had numerically less favorable 3-month scores, no between-group difference reached statistical significance at any fixed time point. Therefore, these subgroup observations should not be interpreted as evidence of a different treatment effect according to osteoporosis status.
No radiographic nonunion was recorded during the available imaging follow-up. In five patients, radiographic follow-up was limited to 6 months because union had already been confirmed and the patients remained clinically asymptomatic. In the two representative cases shown in Figs. 3-5 (one from each group), postoperative radiographs obtained at approximately 4 months (Fig. 5) demonstrated maintained alignment and progression to union without evidence of nonunion.
Complications were recorded in 2/19 patients (10.5%). One patient in the nonosteoporotic group developed postoperative stiffness with hematoma, and one patient in the osteoporotic group demonstrated screw pullout/loosening. Both were managed without documented nonunion. No other major complications were recorded.
A representative nonosteoporotic case and an osteoporotic case are presented in Figs. 3-5. In both cases, an olecranon osteotomy provided adequate joint exposure for intra-articular reduction, ulnar nerve transposition was performed to protect the ulnar nerve, and stable fixation was achieved using parallel dual-plate constructs supplemented with cannulated screw fixation. At 12 months, both representative cases demonstrated low pain (VAS, 0 and 1, respectively) and excellent elbow function (MEPS, 95 and 95, respectively).
Discussion
The management of complete articular distal humerus fractures in elderly patients remains particularly challenging, especially in the context of osteoporosis. Previous studies have emphasized that intra-articular distal humerus fractures in older adults are technically demanding because of fracture complexity, comminution, and compromised bone quality [13]. With ongoing population aging and the increasing prevalence of fragility fractures, the incidence of complex intra-articular distal humerus fractures in elderly patients is expected to continue to rise [14].
In the present study, ORIF yielded satisfactory radiographic and functional outcomes in selected patients aged ≥75 years with complete articular distal humerus fractures (AO/OTA type 13C). No radiographic nonunion was identified during the available imaging follow-up, and both groups showed progressive improvement in pain and elbow function over time. Because between-group differences at fixed postoperative time points were not statistically significant, these subgroup findings should be regarded as descriptive rather than confirmatory.
The optimal surgical approach for AO/OTA type 13C distal humerus fractures remains debated. Olecranon osteotomy and posterior triceps-sparing (paratricipital) approaches are both commonly used, and comparative evidence suggests that overall functional outcomes are similar; therefore, the approach can be individualized based on fracture morphology and the need for articular visualization [15,16]. Olecranon osteotomy can provide excellent exposure for accurate reduction in extensively comminuted patterns, but it introduces osteotomy-specific risks such as delayed union/nonunion, symptomatic hardware, and infection [17]. Triceps-sparing approaches preserve the extensor mechanism and avoid osteotomy-related complications, but limited exposure may compromise reduction quality in severely comminuted fractures [15,16].
Given the predominance of highly comminuted AO/OTA type 13C fractures in the present cohort, olecranon osteotomy was preferentially employed to obtain adequate articular exposure and achieve stable reconstruction. Despite its potential disadvantages, this approach resulted in reliable fracture union and favorable functional outcomes, supporting its continued role in the management of complex intra-articular distal humerus fractures when complete visualization of the articular surface is required [15,16].
The role of bone grafting in the surgical management of comminuted distal humerus fractures remains controversial. Bone grafting may be considered to address metaphyseal voids or segmental defects and to augment fixation when structural support and/or biology are a concern, but the decision depends on graft source, timing, and alternative options. Autograft offers osteogenic, osteoinductive, and osteoconductive potential but entails donor-site morbidity, whereas allograft avoids donor-site morbidity but may incorporate more slowly and carries risks related to immune response and infection transmission [18]. Regardless of graft use, heterotopic ossification and postoperative elbow stiffness are recognized complications after distal humerus fracture fixation and should be minimized through careful soft-tissue handling and early rehabilitation [19].
In this series, bone grafting was not performed in any patient. Instead, surgical management focused on meticulous reduction, preservation of native bone fragments, rigid bicolumnar fixation, and restoration of overall articular congruity [10-12,20]. Despite severe comminution and osteoporotic bone quality, all fractures achieved radiographic union within 1 year, without excessive postoperative stiffness or heterotopic ossification. These findings suggest that routine bone grafting may not be mandatory in elderly patients with complex intra-articular distal humerus fractures when stable fixation and accurate reconstruction are achieved [19].
Routine anterior ulnar nerve transposition was performed in all cases to minimize the risk of postoperative ulnar neuropathy. In distal humerus fractures treated through posterior approaches, the ulnar nerve is susceptible to traction, compression, and implant-related irritation. However, comparative studies have reported that routine transposition in patients without preoperative ulnar neuropathy may not reduce—and may increase—the incidence of postoperative ulnar neuritis compared with in-situ management [21,22]. In the present cohort, no clinically significant ulnar nerve complications were observed, underscoring the importance of careful ulnar nerve identification, decompression, and gentle handling regardless of the chosen strategy [19].
This study has several limitations. First, its retrospective single-center design and the fact that all procedures were performed by a single surgeon introduce potential selection bias and limit external generalizability. In addition, the relative rarity of distal humerus fractures resulted in a small sample size (n=19), leading to limited statistical power to detect small-to-moderate effects and reducing the power of subgroup analyses; therefore, the findings should be interpreted as exploratory.
Second, patients were included over a 12-year period. Although the same surgeon maintained consistent surgical principles, exposure strategy, and bicolumnar fixation concept, temporal changes in implant availability, perioperative care, and accumulated surgeon experience may still have introduced time-related confounding.
Third, only patients treated with ORIF were included, whereas those managed nonoperatively or with other treatment strategies were excluded. Because only cases considered suitable for reconstruction were analyzed, treatment-selection bias cannot be excluded.
Fourth, although clinical outcomes (VAS and MEPS) were available through 12 months in all included patients, radiographic follow-up duration was shorter in five asymptomatic patients because imaging was discontinued after confirmed union at 6 months. Accordingly, the radiographic follow-up range should not be interpreted as incomplete 12-month clinical follow-up, although this approach may still have limited the assessment of later radiographic changes.
Fifth, although ROM was assessed clinically, measurements were not obtained under a fully standardized protocol at every visit, and other validated patient-reported outcome measures were not uniformly available.
ORIF can provide satisfactory clinical recovery and reliable radiographic union in selected elderly patients with severely comminuted intra-articular distal humerus fractures. In this small retrospective case series, postoperative outcomes at predefined time points were not significantly influenced by osteoporosis status.
However, given the limited sample size and noncomparative design, these findings should be interpreted with caution. Further large-scale studies with standardized follow-up protocols and comparative analyses are warranted to better define the role of ORIF relative to alternative treatment strategies in this patient population.
-
Author contributions
Conceptualization: TJL. Data curation: HBS, YL. Formal analysis: TJL, HBS, YL. Funding acquisition: TJL. Writing–original draft: TJL, HBS, YL. Writing–review & editing: TJL, HBS, YL. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This research was supported by an Inha University Research Grant (2025).
-
Data availability
Contact the corresponding author for data availability.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.
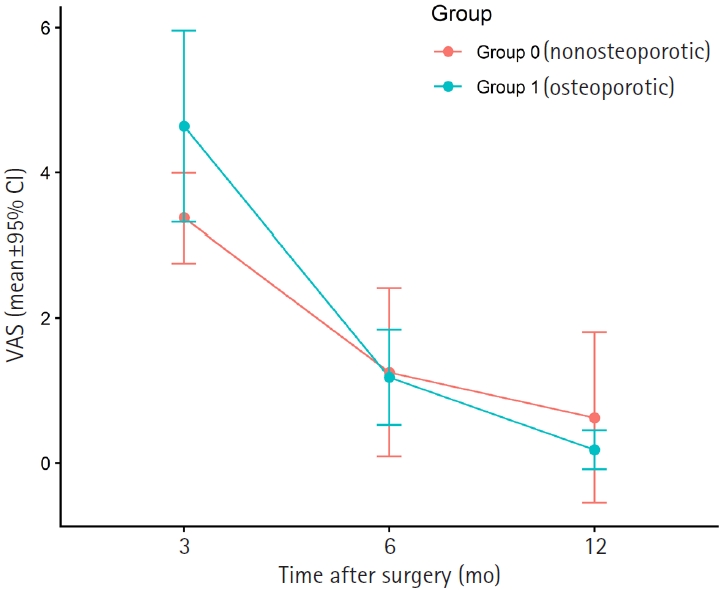
Visual analog scale (VAS) scores over time (mean±95% confidence interval [CI]). Mean VAS pain scores at 3, 6, and 12 months postoperatively are shown for osteoporotic (n=11) and nonosteoporotic (n=8) groups. The points represent group means and error bars indicate 95% CI. Lower VAS scores indicate less pain.
Fig. 2.
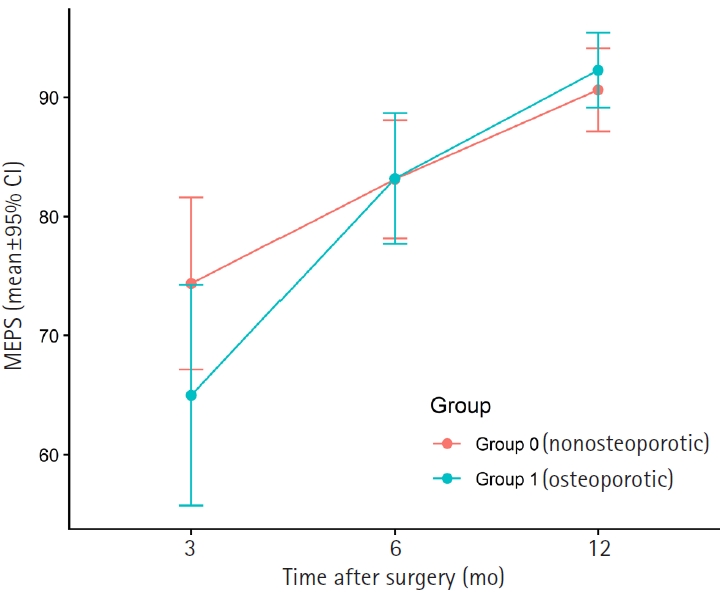
Mayo Elbow Performance Score (MEPS) over time (mean±95% confidence interval [CI]). MEPS at 3, 6, and 12 months postoperatively are shown for osteoporotic (n=11) and nonosteoporotic (n=8) groups. Points represent group means and error bars indicate 95% CI. Higher MEPS values indicate better elbow function.
Fig. 3.

Preoperative radiographs of nonosteoporotic and osteoporotic patients with complete articular distal humerus fractures. Nonosteoporotic patient: (A) oblique view and (B) anteroposterior (AP) view. Osteoporotic patient: (C) lateral view and (D) AP view.
Fig. 4.
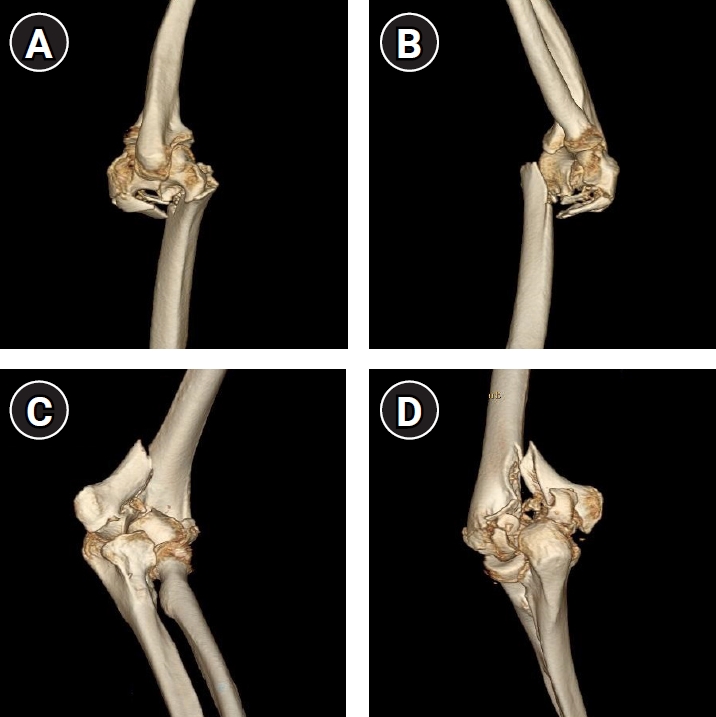
Preoperative three-dimensional computed tomography reconstructions of complete articular distal humerus fractures. (A, B) Lateral view of a nonosteoporotic patient. (C) External oblique view and (D) posterior view of an osteoporotic patient, demonstrating more severe comminution and bone fragmentation.
Fig. 5.

Postoperative (4-mo) radiographs demonstrating successful union in both groups. Nonosteoporotic patient: (A) anteroposterior view and (B) lateral view. Osteoporotic patient: (C) lateral view and (D) anteroposterior view.
Table 1.
Baseline demographics by osteoporosis status
Values are presented as median (interquartile range, IQR) for continuous variables and number (%) for categorical variables. P-values were calculated using the Mann-Whitney U test for continuous variables and the Fisher exact test for categorical variables (two-sided). BMD T-score was used to define group allocation; therefore, no statistical comparison was performed for this variable.
BMI, body mass index; BMD, bone mineral density; ER, emergency room; AO/OTA, Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association; IQR, interquartile range.
- 1. Beazley JC, Baraza N, Jordan R, Modi CS. Distal humeral fractures: current concepts. Open Orthop J 2017;11:1353-63.ArticlePubMedPMCPDF
- 2. Seok HG, Park JJ, Park SG. Comparison of the complications, reoperations, and clinical outcomes between open reduction and internal fixation and total elbow arthroplasty for distal humeral fractures in the elderly: a systematic review and meta-analysis. J Clin Med 2022;11:5775.ArticlePubMedPMC
- 3. Kervinen KV, Salmela MT, Lähdeoja TA. Outcomes of AO/OTA C-type fractures of the distal humerus after open reduction and internal fixation with locking plate constructs in patients at least 65 years old. BMC Musculoskelet Disord 2022;23:523.ArticlePubMedPMCPDF
- 4. Sarafrazi N, Wambogo EA, Shepherd JA. Osteoporosis or low bone mass in older adults: United States, 2017-2018. NCHS Data Brief 2021;(405):1-8.Article
- 5. Clavert P, Ducrot G, Sirveaux F, Fabre T, Mansat P. Outcomes of distal humerus fractures in patients above 65 years of age treated by plate fixation. Orthop Traumatol Surg Res 2013;99:771-7.ArticlePubMed
- 6. Lee KT, Lai CH, Singh S. Results of total elbow arthroplasty in the treatment of distal humerus fractures in elderly Asian patients. J Trauma 2006;61:889-92.ArticlePubMed
- 7. Parker P, Furness ND, Evans JP, Batten T, White WJ, Smith CD. A systematic review of the complications of contemporary total elbow arthroplasty. Shoulder Elbow 2021;13:544-51.ArticlePDF
- 8. Githens M, Yao J, Sox AH, Bishop J. Open reduction and internal fixation versus total elbow arthroplasty for the treatment of geriatric distal humerus fractures: a systematic review and meta-analysis. J Orthop Trauma 2014;28:481-8.ArticlePubMed
- 9. Shin SJ, Sohn HS, Do NH. A clinical comparison of two different double plating methods for intraarticular distal humerus fractures. J Shoulder Elbow Surg 2010;19:2-9.Article
- 10. O'Driscoll SW. Optimizing stability in distal humeral fracture fixation. J Shoulder Elbow Surg 2005;14(1 Suppl S):186S-194S.Article
- 11. Sanchez-Sotelo J, Torchia ME, O'Driscoll SW. Complex distal humeral fractures: internal fixation with a principle-based parallel-plate technique. J Bone Joint Surg Am 2007;89:961-9.ArticlePubMed
- 12. Lee SK, Kim KJ, Park KH, Choy WS. A comparison between orthogonal and parallel plating methods for distal humerus fractures: a prospective randomized trial. Eur J Orthop Surg Traumatol 2014;24:1123-31.ArticlePubMedPDF
- 13. Stoddart MT, Panagopoulos GN, Craig RS, et al. A systematic review of the treatment of distal humerus fractures in older adults: a comparison of surgical and non-surgical options. Shoulder Elbow 2024;16:175-85.ArticlePubMedPDF
- 14. Charissoux JL, Vergnenegre G, Pelissier M, Fabre T, Mansat P. Epidemiology of distal humerus fractures in the elderly. Orthop Traumatol Surg Res 2013;99:765-9.ArticlePubMed
- 15. Jeong HS, Yang JY, Jeon SJ, Shon HC, Oh JK, Lim EJ. Comparison of olecranon osteotomy and paratricipital approach in distal humerus intra-articular fracture: a systematic review and meta-analysis. Medicine (Baltimore) 2022;101:e30216.Article
- 16. Chen G, Liao Q, Luo W, Li K, Zhao Y, Zhong D. Triceps-sparing versus olecranon osteotomy for ORIF: analysis of 67 cases of intercondylar fractures of the distal humerus. Injury 2011;42:366-70.ArticlePubMed
- 17. Spierings KE, Schoolmeesters BJ, Doornberg JN, Eygendaal D, van den Bekerom MP. Complications of olecranon osteotomy in the treatment of distal humerus fracture. Clin Shoulder Elb 2022;25:163-9.ArticlePubMedPMCPDF
- 18. Egol KA, Nauth A, Lee M, Pape HC, Watson JT, Borrelli J. Bone grafting: sourcing, timing, strategies, and alternatives. J Orthop Trauma 2015;29 Suppl 12:S10-4.ArticlePubMed
- 19. Savvidou OD, Zampeli F, Koutsouradis P, et al. Complications of open reduction and internal fixation of distal humerus fractures. EFORT Open Rev 2018;3:558-67.ArticlePubMedPMCPDF
- 20. Self J, Viegas SF, Buford WL, Patterson RM. A comparison of double-plate fixation methods for complex distal humerus fractures. J Shoulder Elbow Surg 1995;4(1 Pt 1):10-6.Article
- 21. Chen RC, Harris DJ, Leduc S, Borrelli JJ, Tornetta P, Ricci WM. Is ulnar nerve transposition beneficial during open reduction internal fixation of distal humerus fractures? J Orthop Trauma 2010;24:391-4.ArticlePubMed
- 22. Ahmed AF, Parambathkandi AM, Kong WJ, et al. The role of ulnar nerve subcutaneous anterior transposition during open reduction and internal fixation of distal humerus fractures: a retrospective cohort study. Int Orthop 2020;44:2701-8.ArticlePubMedPMCPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
Cite- Figure
-
- We recommend
- Related articles
-
- Hook plate versus periarticular-type volar locking plate for distal radius fractures involving the volar lunate facet in Korea: a retrospective cohort study
- Comparative results of the femoral neck system versus the dynamic hip screw for stable femoral neck fractures in older adults in Korea: a retrospective cohort study
- Correlation of bone mineral density with ankle fractures in older adults in Korea: a retrospective cohort study
Open reduction and internal fixation for distal humerus fractures in older adults: a retrospective comparative study by osteoporosis status
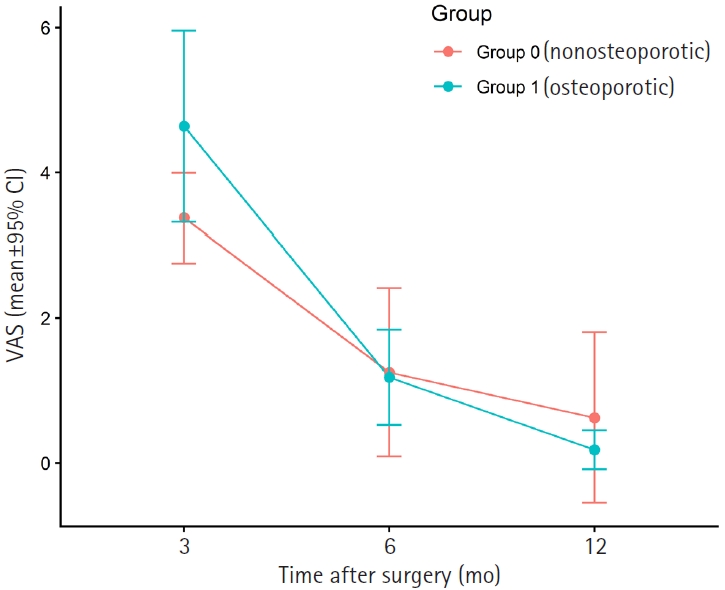
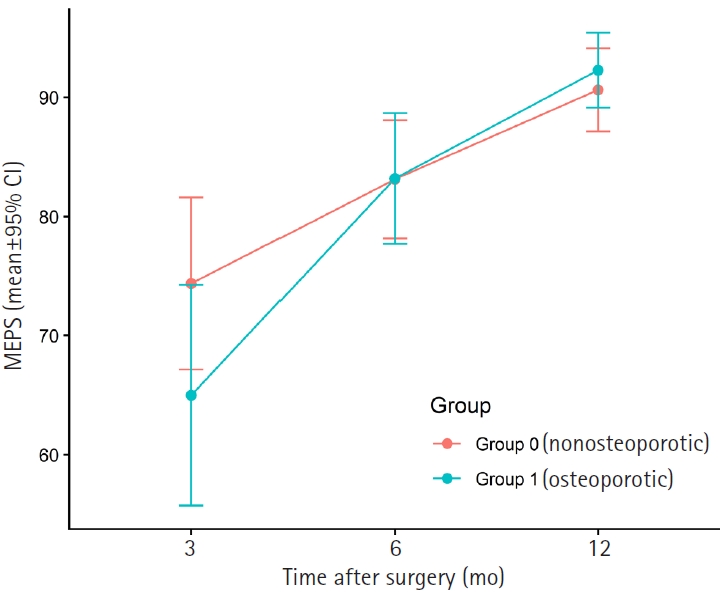

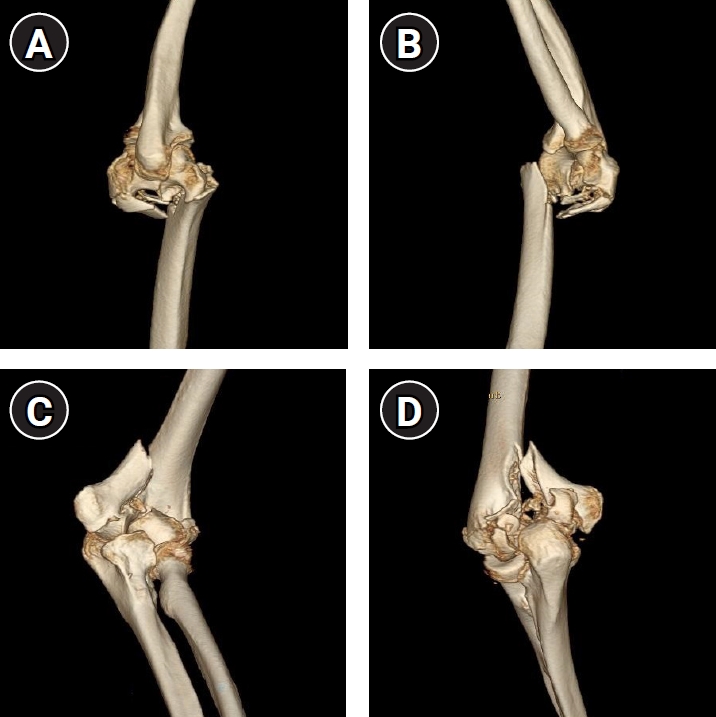

Fig. 1. Visual analog scale (VAS) scores over time (mean±95% confidence interval [CI]). Mean VAS pain scores at 3, 6, and 12 months postoperatively are shown for osteoporotic (n=11) and nonosteoporotic (n=8) groups. The points represent group means and error bars indicate 95% CI. Lower VAS scores indicate less pain.
Fig. 2. Mayo Elbow Performance Score (MEPS) over time (mean±95% confidence interval [CI]). MEPS at 3, 6, and 12 months postoperatively are shown for osteoporotic (n=11) and nonosteoporotic (n=8) groups. Points represent group means and error bars indicate 95% CI. Higher MEPS values indicate better elbow function.
Fig. 3. Preoperative radiographs of nonosteoporotic and osteoporotic patients with complete articular distal humerus fractures. Nonosteoporotic patient: (A) oblique view and (B) anteroposterior (AP) view. Osteoporotic patient: (C) lateral view and (D) AP view.
Fig. 4. Preoperative three-dimensional computed tomography reconstructions of complete articular distal humerus fractures. (A, B) Lateral view of a nonosteoporotic patient. (C) External oblique view and (D) posterior view of an osteoporotic patient, demonstrating more severe comminution and bone fragmentation.
Fig. 5. Postoperative (4-mo) radiographs demonstrating successful union in both groups. Nonosteoporotic patient: (A) anteroposterior view and (B) lateral view. Osteoporotic patient: (C) lateral view and (D) anteroposterior view.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Open reduction and internal fixation for distal humerus fractures in older adults: a retrospective comparative study by osteoporosis status
| Variable | Nonosteoporotic group | Osteoporotic group | P-value |
|---|---|---|---|
| No. of patients | 8 | 11 | |
| Age at injury (yr) | 77.0 (75.0 to 78.0) | 80.0 (77.5 to 82.0) | 0.113 |
| Female sex | 4 (50.0) | 10 (90.9) | 0.111 |
| BMI (kg/m²) | 24.5 (22.1 to 27.1) | 24.5 (22.8 to 26.9) | 0.821 |
| BMD T-score | –1.2 (–1.6 to –0.8) | –3.2 (–3.6 to –2.8) | |
| Radiographic follow-up (mo) | 21.0 (6.0 to 25.5) | 12.0 (12.0 to 16.5) | 0.387 |
| Olecranon osteotomy approach | 7 (87.5) | 8 (72.7) | 0.603 |
| ER visit | 8 (100.0) | 7 (63.6) | 0.103 |
| AO/OTA subtype | |||
| 13C1 | 3 (37.5) | 5 (45.5) | |
| 13C2 | 2 (25.0) | 3 (27.3) | |
| 13C3 | 3 (37.5) | 3 (27.3) |
Table 1. Baseline demographics by osteoporosis status
Values are presented as median (interquartile range, IQR) for continuous variables and number (%) for categorical variables. P-values were calculated using the Mann-Whitney U test for continuous variables and the Fisher exact test for categorical variables (two-sided). BMD T-score was used to define group allocation; therefore, no statistical comparison was performed for this variable. BMI, body mass index; BMD, bone mineral density; ER, emergency room; AO/OTA, Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association; IQR, interquartile range.

