 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(2); 2026 > Article
-
Review Article
- Combined acetabular and pelvic ring injuries: a reference-frame algorithm for definitive fixation sequencing
-
Jeong-Hyun Koh
 , Seungyeob Sakong
, Seungyeob Sakong -
Journal of Musculoskeletal Trauma 2026;39(2):83-92.
DOI: https://doi.org/10.12671/jmt.2026.00031
Published online: March 31, 2026
Department of Orthopedic Surgery, Ajou University School of Medicine, Suwon, Korea
- Correspondence to: Seungyeob Sakong Department of Orthopedic Surgery, Ajou University School of Medicine, 164 Worldcup-ro, Yeongtong-gu, Suwon 16499, Korea Tel: +82-31-219-5220, Email: sgsy4040@gmail.com
• Received: January 8, 2026 • Revised: January 18, 2026 • Accepted: January 25, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 950 Views
- 23 Download
- Abstract
- Introduction
- Scope, terminology, and classification
- Working framework: MCAPI vs. non-MCAPI
- Epidemiology, injury patterns, and assessment pearls for definitive planning
- Decision points and operative planning
- Definitive fixation strategy and sequence
- Outcomes, complications, and postoperative considerations
- Discussion: pitfalls, controversies, and future directions
- Summary and key messages
- Article Information
- References
Abstract
- Combined acetabular and pelvic ring injuries are not simply “two fractures in one patient.” Reduction and fixation of one component can alter the alignment and reducibility of the other, rendering operative sequencing a primary decision variable rather than a secondary consideration. These injuries typically result from high-energy trauma, frequently occur in patients with polytrauma, and are further influenced by physiological tolerance and the feasibility of available operative corridors. The existing evidence base remains constrained by retrospective study designs, inconsistent definitions, variable classification systems, and heterogeneous outcome reporting, all of which limit the strength of comparative recommendations. This state-of-the-art review presents a surgeon-facing, algorithmic approach grounded in a reference-frame mindset. We emphasize computed tomography (CT)-based mapping and the use of consistent terminology to characterize acetabular morphology, pelvic ring instability, deformity vectors, suspicion of mechanical coupling, and feasible operative corridors. Mechanically connected acetabular and pelvic ring injuries (MCAPI) are introduced as a working framework for identifying patterns in which reduction or fixation of one injury predictably influences the other. In cases of suspected MCAPI, a posterior ring-based sequence is generally preferred, typically consisting of posterior ring reduction and fixation, definitive acetabular reconstruction, and subsequent anterior ring fixation. We propose an explicit intraoperative “GO/NO-GO” checkpoint (reference acceptable, stable, corridors feasible) to prevent acetabular reconstruction on a moving target. Acetabulum-first strategies may be appropriate only in selected anteroposterior compression-type configurations in which acetabular fixation plausibly restores sacroiliac congruency and posterior stabilization remains technically feasible. We summarize key outcome domains and complication patterns, highlighting hip dislocation as an important risk factor associated with both neurologic deficits and overall complications. Standardized CT-based definitions and outcome instruments, together with multicenter cohorts employing predefined decision pathways, are required to test sequencing strategies and to determine whether improved radiographic reduction translates into durable functional benefit.
Introduction
Combined acetabular and pelvic ring injuries represent a distinct and challenging subset of pelvic trauma. Unlike isolated acetabular or pelvic ring fractures, these combined patterns often occur after high-energy mechanisms and are frequently accompanied by substantial associated injuries, creating a narrow therapeutic window in which surgeons must balance physiological priorities with the technical demands of achieving stable pelvic alignment and accurate articular reconstruction [1,2]. Early reports and subsequent series have consistently emphasized that these injuries behave differently from “two independent fractures,” because the reduction and fixation of one component may influence the alignment and reducibility of the other [3,4].
Despite their clinical importance, the evidence remains fragmented. Definitions of what constitutes a “true” combined injury vary across studies, classification usage is inconsistent, and outcome reporting is heterogeneous—factors repeatedly highlighted in systematic reviews [5,6]. In addition, the spectrum of pelvic ring instability and acetabular fracture morphology is broad, and shared terminology is essential for translating published experiences into reproducible surgical decision-making [7-9]. Consequently, surgical strategies, particularly the optimal sequence of fixation and approach planning, continue to show substantial variations across centers [10,11].
To address this gap, we adopted the concept of mechanically connected acetabular and pelvic ring injuries (MCAPI) as a practical working framework rather than a rigid taxonomy. MCAPI highlights combined patterns in which the acetabulum and pelvic ring function as a mechanically coupled system, such that the fixation order and reduction strategy are decisive for achieving a stable reference frame and a congruent hip joint [2,12]. Building on contemporary state-of-the-art perspectives and representative clinical series, we synthesized the decision points most relevant to pelvic and acetabular surgeons, including pattern recognition, fixation sequencing, approach and positioning considerations, and staging and timing modifiers, and translated them into an actionable algorithm (Fig. 1) [13-15]. The key studies underpinning this framework are summarized in Table 1 [1,2,4-6,10,12,13,16,17].
To populate Table 1, we used a pragmatic evidence-selection approach aligned with the goals of a surgeon-facing narrative review. We identified relevant publications through targeted database searching and reference-list screening of major reviews and clinical series, then prioritized studies that (1) explicitly addressed combined acetabular-pelvic ring injuries, (2) provided decision-relevant information on sequencing, reference-frame stability, or corridor feasibility, and (3) reported reproducible clinical or radiographic outcomes and complication signals. The final set of ‘key studies’ was selected by author consensus to represent the spectrum of definitions and sequencing strategies and to foreground decision-relevant signals, rather than to provide an exhaustive systematic synthesis.
This surgeon-facing narrative review aimed to provide a standardized decision-making framework to address the current ambiguity surrounding surgical sequencing. To achieve this, our objective was threefold: (1) to standardize key terminology and classification language for combined injuries, (2) to provide a practical MCAPI-based approach to operative sequencing with clearly stated “generally favored” principles and selected exceptions, and (3) to summarize outcome expectations and complication risk signals that can inform preoperative counseling and intraoperative strategy [16,17].
Scope, terminology, and classification
Combined acetabular and pelvic ring injuries involve multiple threats, including high injury severity, frequently associated visceral and vascular injuries, and competing priorities between restoring pelvic stability and articular congruity [1,4]. Definitive management is often a sequential problem, in which the order of reduction and fixation determines whether the acetabulum is reconstructed on a stable reference frame [12]. Definitions vary because fracture lines near the pubic root and anterior column can be interpreted differently across centers. High pubic root or ramus injuries may be mislabeled as low anterior column fractures, whereas some acetabular fractures extend toward the sacroiliac (SI) region without meaningfully destabilizing the ring [5]. In this review, we included injuries with a true acetabular articular component and pelvic ring disruption, where at least one component was potentially operative, and the interaction could influence the reduction strategy or fixation sequence.
Computed tomography (CT)-based mapping is essential, and a practical “common language” is to describe acetabular morphology using Judet-Letournel patterns and pelvic ring instability using AO/OTA (Arbeitsgemeinschaft für Osteosynthesefragen/Orthopedic Trauma Association) descriptors, with Young-Burgess anteroposterior compression (APC) and lateral compression (LC) concepts as deformity-oriented adjuncts when needed [7-9]. Imaging deliverables should address three operative questions: mechanical linkage (suspected MCAPI), dominant deformity and reduction targets, and corridor feasibility in the context of soft tissues and physiology [2]. Although combined patterns represent a small proportion of acetabular and pelvic ring fractures, they carry disproportionate resource utilization and complication risks; the mechanisms are typically high-energy, and polytrauma physiology frequently necessitates staged definitive fixation [1,2,5,18].
Most evidence consists of retrospective series with heterogeneous inclusion criteria and variable outcome instruments, and systematic reviews have concluded that these limitations preclude strong comparative recommendations on timing, sequencing, or surgical approach [5,6,19]. Nevertheless, an algorithmic approach can add value by standardizing key decision points (mechanical linkage, reference frame selection, and sequence checkpoints) and aligning terminology across studies (Table 1) [2,11].
Working framework: MCAPI vs. non-MCAPI
MCAPI refers to combined injuries in which the reduction or fixation of one component predictably affects the other, whereas non-MCAPI refers to injuries that behave more independently [2]. This distinction is important because it promotes a reference-frame mindset: the first fixation step should be selected to make subsequent acetabular reduction reliable and reproducible [4,12].
For practical application, MCAPI can be suspected using a concise checklist: (1) an ipsilateral unstable pelvic ring likely requiring fixation (commonly AO/OTA B2–B3 or C-type), (2) acetabular morphology with a transverse or anterior-column–linked component (including T-type or both-column variants), (3) CT features suggesting coupled displacement such that hemipelvic reduction is expected to change acetabular alignment, and (4) anticipated interdependence in corridor feasibility or positioning where the first fixation step predictably alters reducibility or deliverability of the other component. As a high-risk coupling signal, hip dislocation or central instability—particularly with transverse-oriented morphology—should heighten suspicion and may justify earlier stability decisions to protect neurologic risk and optimize final congruity [2,12,16]. In contrast, non-MCAPI is more likely when the acetabular injury involves an isolated wall or column pattern, or when the injuries are contralateral without a plausible mechanical linkage [2,11]. In these settings, the fixation sequence is determined by displacement, urgency, and corridor feasibility; regardless of the order, pelvic stability should be reverified before committing to final articular reconstruction.
Clinically, combined-injury cohorts often show higher injury severity, more frequent associated injuries, and more frequent staging than isolated injuries [1,17]. In particular, hip dislocation has been associated with residual neurologic deficits and overall complications and should be treated as a key risk signal during counseling and operative planning [16]. Finally, MCAPI is most useful because it clarifies which structure must be reduced and stabilized first to establish a reliable reference for acetabular reconstruction; when coupling is likely, posterior ring reduction and stabilization commonly precede definitive acetabular fixation, with explicit checkpoints before articular reconstruction (Fig. 1) [2,3,12].
Epidemiology, injury patterns, and assessment pearls for definitive planning
Combined cohorts tend to present with greater injury severity, multisystem trauma, and a higher likelihood of staged definitive fixation than isolated injuries [1,17]. These contextual factors often drive timing, positioning tolerance, and corridor selection as much as fracture morphology itself [18].
A mechanism-informed language is useful because it predicts deformity vectors. APC patterns suggest external rotation and anterior instability that can alter acetabular relationships, whereas LC patterns suggest internal rotation and impaction tendencies that may influence reduction strategy and corridor selection [4,7]. In practice, several “red flags” commonly modify definitive strategy, including hip dislocation, major posterior ring displacement, and soft-tissue or visceral constraints that limit early corridors; early identification of these factors helps anticipate sequence, staging, and operative time requirements [1,10,12].
CT should provide a reproducible and shared map for the team, including ring deformity and instability, acetabular articular displacement, evidence of coupling, and feasible corridors in the context of soft-tissue and physiology [2,4]. Two practical pearls repeatedly influence definitive planning. First, definitive acetabular fixation should be avoided until the pelvic reference frame is acceptable and stable; otherwise, the acetabulum is reconstructed on a moving target [3,12]. Second, deciding early whether a case is likely to represent MCAPI helps avoid unplanned repositioning and prolonged operative time [2].
Decision points and operative planning
The primary goal in combined acetabular and pelvic ring injuries is to create a reliable hemipelvic reference frame for acetabular reduction by addressing instability that can shift acetabular alignment. Therefore, the fixation sequence is often more important than approach selection, particularly when the two injuries interact mechanically [2,4]. Before committing to definitive acetabular fixation, preoperative planning should explicitly state what provides the reference frame and what constitutes an acceptable checkpoint for proceeding with definitive acetabular reconstruction [12].
MCAPI triage can be performed preoperatively using CT and pattern recognition. An ipsilateral unstable ring combined with transverse- or anterior-column-linked acetabular morphology, along with CT features suggesting coupled displacement, increases the likelihood that reduction or fixation of one component will predictably affect the other [2,17]. The goal is not to force cases into a rigid category, but to use coupling suspicion as a trigger to plan an explicit reference-frame sequence and to anticipate situations in which indirect reduction may fail.
A simple intraoperative checkpoint can improve reproducibility and help avoid reconstruction of the acetabulum on a “moving target.” In practice, definitive acetabular fixation should proceed only if the GO/NO-GO checkpoint is met: (1) reference acceptable (posterior ring reduction acceptable), (2) reference stable (temporary or definitive fixation has converted the hemipelvis into a reliable platform), and (3) corridors feasible (positioning/approach constraints reconciled without compromising reduction priorities) [2,3,12,14].
Staging is common and should be planned deliberately, driven by physiology, soft tissues, and operative time rather than treated as an afterthought [4,18]. Early coordination between pelvic and acetabular teams helps preserve the intended sequence when physiological constraints require staged corridors [2,10]. Approach and positioning should follow the planned sequence: when MCAPI is likely, posterior ring reduction and stabilization often precede acetabular reconstruction, and corridor choice should minimize repositioning without compromising establishment of the reference frame first [2,3]. Finally, fixation philosophy (percutaneous vs. open) should be framed as a constraint-driven decision point. Percutaneous strategies may reduce soft-tissue insult and operative time in polytrauma but require a stable reference frame, accurate imaging, and clear reduction targets, whereas an open strategy may be necessary to achieve accurate articular reduction in complex coupled patterns [2,10,15,17].
Definitive fixation strategy and sequence
Combined acetabular and pelvic ring injuries are not simply “two fractures in one patient.” Operative planning must integrate approach, positioning, and fixation order, because reduction of one component can influence the reduction (or reducibility) of the other. Fig. 1 provides an algorithmic overview of the key decision points and generally favors specific sequencing strategies in this setting [2,4,5].
The term MCAPI has been proposed to distinguish patterns in which reduction or fixation of one injury is expected to affect the other from “coexisting but noninteracting” combinations (non-MCAPI) [2]. CT-based characterization is typically required to define fracture morphology and associated injuries, and the use of a unified classification language (such as Judet-Letournel for the acetabulum and AO/OTA for the pelvic ring) supports consistent decision-making across patterns [5,8,9].
From a practical standpoint, MCAPI should be suspected in ipsilateral acetabular patterns with an anterior column or transverse component (including T-type and both-column variants) combined with an unstable pelvic ring injury (commonly AO/OTA B2–B3 or C patterns), in which indirect posterior reduction through anterior-only maneuvers may be unreliable because of an “interrupting fracture” [2,12]. In these mechanically coupled patterns, definitive treatment is best framed as a reference frame problem, and the fixation sequence should be chosen to establish a stable hemipelvic platform before committing to definitive acetabular reconstruction.
For definitive treatment of MCAPI, a posterior ring-based sequence is generally favored in contemporary series and strategy articles [2,12]. The rationale is that incomplete posterior ring reduction may compromise acetabular reduction, particularly in transverse-oriented acetabular patterns [4,12].
Accordingly, a commonly adopted sequence is (1) reduction and fixation of the displaced posterior ring, (2) definitive acetabular fixation, and (3) fixation of the anterior ring (such as symphysis or rami), as indicated [2,4]. Clinical observations support this linkage, which reports of worse acetabular reduction quality in the presence of residual posterior displacement or SI separation [12,17]. Therefore, an intraoperative checkpoint is reasonable: if meaningful residual posterior malreduction persists (especially in transverse-oriented acetabular fractures), re-optimization of the posterior reduction should precede definitive acetabular fixation [2,12].
An MCAPI-centered approach should also acknowledge pattern-driven exceptions. An acetabulum-first sequence may be considered in selected configurations, most notably transverse acetabular fractures combined with an AO/OTA B2.3 (APC2) pelvic ring injury, in which acetabular fixation may nearly restore SI congruency and allow percutaneous fixation or case-dependent nonoperative management of the posterior ring [2]. An acetabulum-first strategy may also be discussed when percutaneous acetabular fixation is appropriate and can be performed efficiently before pelvic ring fixation; however, these scenarios should be regarded as selected exceptions rather than routine alternatives [2,5,6].
Sequence decisions are inseparable from approach, positioning, and staging. Planning should minimize unnecessary repositioning while accepting staged corridors when required by fracture morphology and patient physiology [2,10]. When posterior acetabular components, such as a posterior wall fracture, are present, posterior approaches (such as Kocher-Langenbeck) are commonly required for reliable fixation [8,9]. Given that pelvic ring disruptions may be immediately life-threatening and physiological tolerance can limit operative duration, staged fixation is frequently necessary. Stabilizing the pelvic ring first and staging acetabular reconstruction is reasonable when blood loss, operative time, or cardiopulmonary status preclude a single-stage procedure [5,12]. Definitive fixation should proceed once physiological optimization is achieved and soft-tissue conditions permit. In published series, surgery commonly occurs within an early window (approximately 3–7 days), although substantial variation exists, and timing should be individualized based on concomitant injuries, competing priorities, and operative logistics [2,5].
Outcomes, complications, and postoperative considerations
Outcomes of combined acetabular and pelvic ring injuries are best interpreted across three domains: acetabular articular congruity, pelvic alignment and stability, and patient-centered function. However, heterogeneous definitions and outcome instruments continue to limit cross-study comparisons and preclude firm conclusions regarding an optimal strategy [5,6,19].
Complication burdens are substantial across reported series, although exact rates vary with inclusion criteria and injury severity. Hip dislocation is a particularly important risk factor associated with residual neurologic deficits and overall complications, and should be highlighted during preoperative counseling and planning [16]. Recent studies further examine predictors of complications and support practical risk stratification, physiological staging, and sequence discipline rather than maximal reconstruction in a single setting when physiological tolerance is limited [13].
Postoperative care should remain principle-based and focus on protection of the reconstruction until pelvic stability and hip congruity are secure; surveillance for thromboembolism, infection, and heterotopic ossification according to institutional protocols; and tailoring weight-bearing progression to construct stability, fixation quality, and associated injuries [2,4]. Follow-up imaging should be consistent, with a low threshold for CT when symptoms or radiographs suggest loss of reduction or when articular congruity is uncertain.
Discussion: pitfalls, controversies, and future directions
Although combined acetabular and pelvic ring injuries are increasingly recognized as a meaningful subset of pelvic trauma, the evidence base remains constrained by retrospective study designs, inconsistent definitions, variable classifications, and heterogeneous outcome reporting. Systematic reviews consistently highlight these limitations and caution against overgeneralizing “best” strategies from small case series [5,6,19]. Accordingly, the most defensible contribution of a modern review is not to prescribe a single universal protocol, but to clarify decision points and identify principles that are repeatedly supported across contemporary experiences [2,4].
The MCAPI concept is attractive because it translates a complex fracture spectrum into a clinically actionable question: are the acetabulum and pelvic ring mechanically coupled such that reduction of one will change the other? As a working framework, MCAPI helps surgeons prioritize reference frames and sequencing decisions, particularly in transverse-oriented acetabular patterns with unstable posterior ring injury [2,12,15]. However, MCAPI should not be treated as a definitive classification system. Its boundaries are still evolving, and real-world cases exist along a continuum from “more connected” versus “less connected,” with patient physiology and corridor feasibility frequently overriding purely morphologic considerations [13,14].
The most debated practical question is fixation order. Earlier experience and mechanistic reasoning support a posterior ring-based sequence in mechanically connected patterns, emphasizing that residual posterior malreduction can compromise acetabular reduction quality [2,4,12,13]. More recent cohort studies continue to evaluate whether posterior-first sequencing improves postoperative acetabular reduction metrics and whether such improvements translate into meaningful functional benefits [13]. The selected exceptions remain clinically plausible. In specific configurations, classically described for transverse acetabular fractures with an APC-type ring pattern, acetabular fixation may nearly restore SI congruency, and an acetabulum-first pathway may be reasonable if a stable reference can be reliably achieved and posterior fixation can be performed percutaneously or in a staged fashion [2,6]. A defensible stance is therefore to frame posterior-first sequencing as “generally favored” in MCAPI, while explicitly acknowledging exceptions and emphasizing intraoperative checkpoints rather than rigid rules.
A second practical controversy concerns whether definitive reconstruction should be completed in a single setting or intentionally staged. Combined injuries frequently occur in physiologically stressed patients with multisystem trauma, and unplanned prolonged surgery can amplify risk, even when the technical plan is sound [4,18]. Staging should not be seen as a failure of planning, but rather as a deliberate strategy to secure the reduction reference, limit operative burden, and return for definitive articular reconstruction when conditions permit [2,6]. Similarly, the choice between open and percutaneous strategies is rarely a matter of pure technical preference, as it is often dictated by displacement, comminution, and the need for direct articular reduction. Reported complication burdens reinforce the importance of minimizing soft-tissue morbidity when percutaneous methods can achieve stable alignment without sacrificing articular goals, while recognizing that selection bias remains unavoidable in retrospective evidence [5,15,16].
Progress in this field depends on three practical steps. First, a consistent CT-based definition of “combined injury,” distinguishing true articular acetabular involvement from high pubic root variants, would reduce heterogeneity across reports [2,5]. Second, standardized outcome reporting should include articular metrics (step-off and gapping), pelvic alignment, and patient-reported outcomes with minimum follow-up thresholds to enable meaningful comparison of sequencing and staging strategies [13,19]. Third, multicenter registries or prospective cohorts with predefined decision pathways could clarify whether posterior-first sequencing confers functional advantages beyond improved radiographic reduction in selected MCAPI patterns [14,15].
Summary and key messages
Combined acetabular and pelvic ring injuries represent a distinct subset of pelvic trauma in which reduction or fixation of one component may influence the other, making operative sequencing a primary decision variable rather than an afterthought [2,4]. The MCAPI concept is useful as a working framework to identify mechanically coupled patterns and guide reduction priorities and sequencing; however, it should be applied with “generally favored” principles with explicit exceptions rather than rigid rules [2,15]. Future studies should focus on correlating these sequencing algorithms with long-term patient-reported outcome measures through prospective multicenter registries.
• Suspect MCAPI when an ipsilateral unstable pelvic ring coexists with transverse- or anterior-column-linked acetabular morphology and coupled displacement features; in these cases, establish an acceptable and stable posterior ring reference before definitive acetabular fixation [2,3,12].
• Use a simple intraoperative GO/NO-GO checkpoint (reference acceptable, stable, corridors feasible) to avoid reconstructing the acetabulum on a moving target [2,14].
• Consider an acetabulum-first strategy only in selected APC-type configurations in which acetabular fixation plausibly restores SI congruency and posterior stabilization remains feasible [2].
• Counsel patients regarding substantial complication risks; hip dislocation is a key risk signal and may indicate a higher risk of neurologic deficits and overall complications [13,16].
• The evidence base remains heterogeneous; standardized definitions and outcome measures are required to test sequencing strategies in comparable cohorts [5,6].
-
Author contributions
Conceptualization: JHK, SS. Methodology: JHK, SS. Investigation: JHK. Resources: JHK. Data curation: JHK. Supervision: SS. Project administration: SS. Visualization: JHK. Writing–original draft: JHK. Writing–review & editing: JHK. SS. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.
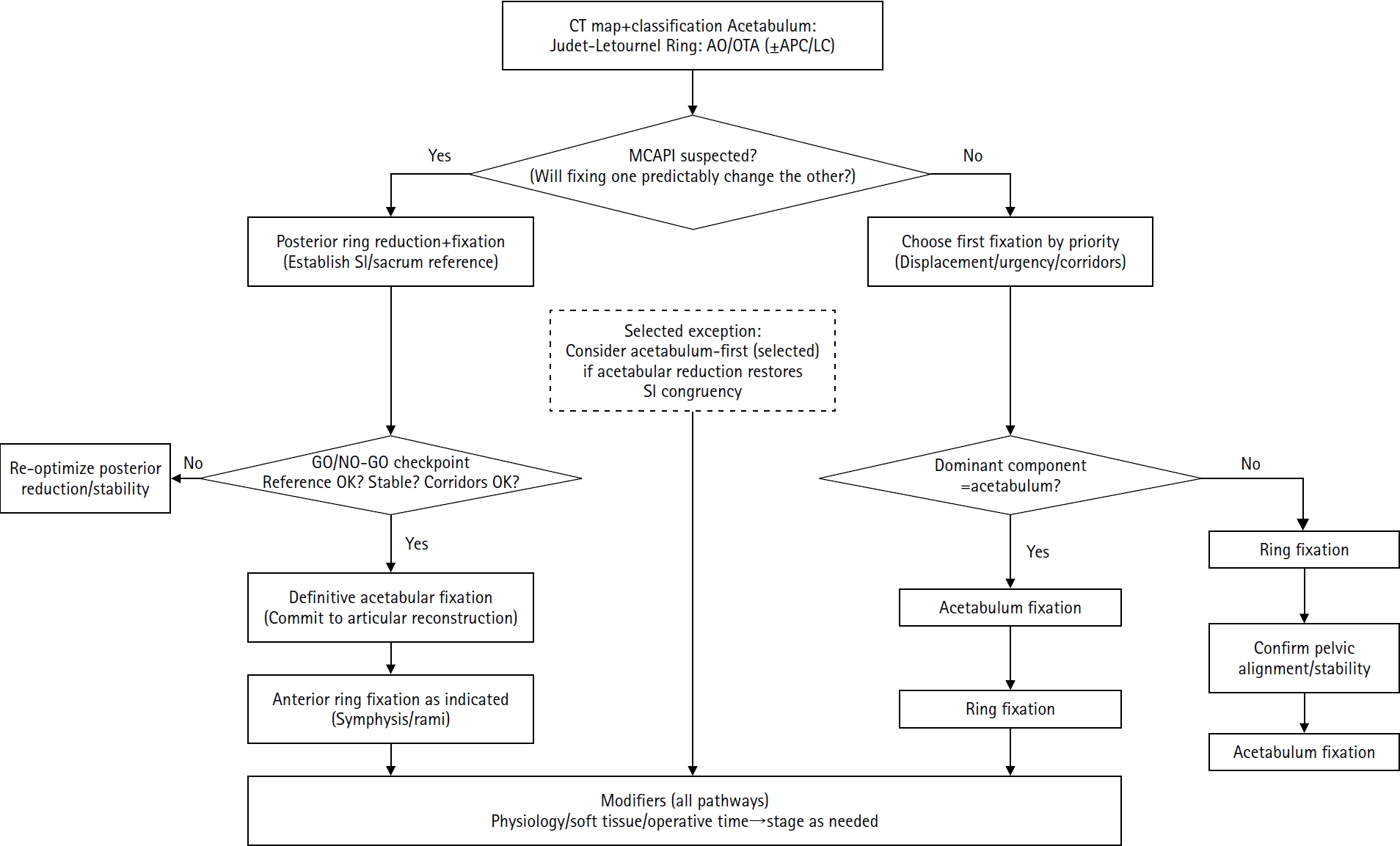
Reference-frame algorithm for definitive fixation sequencing in combined pelvic ring and acetabular injuries.
Following computed tomography (CT)-based morphological mapping (Judet-Letournel for the acetabulum; AO/OTA ± APC/LC for the pelvic ring), the surgical sequence is guided by the presence or absence of mechanical coupling (MCAPI). In suspected MCAPI patterns, posterior ring stabilization is performed to establish a stable sacroiliac and sacral reference, after which a critical GO/NO-GO checkpoint is applied to confirm reference stability and operative corridor feasibility before proceeding with definitive articular reconstruction. In non-MCAPI patterns, the initial fixation target is selected based on the degree of displacement, clinical urgency, and corridor feasibility. Regardless of the chosen sequence, pelvic alignment and overall stability must be reconfirmed before committing to final joint surface reconstruction. Staged surgery may be required in some cases because of physiological status or soft-tissue considerations. CT, computed tomography; AO/OTA, Arbeitsgemeinschaft für Osteosynthesefragen/Orthopedic Trauma Association; APC/LC, anteroposterior compression/lateral compression; MCAPI, mechanically connected acetabular and pelvic ring injuries; SI, sacroiliac.
Table 1.
Core evidence matrix for combined acetabular-pelvic ring injuries (10 key studies)
| Study (yr) | Design | No./scope | Definition/inclusion (as used) | Classification | Sequencing/strategy (key message) | Outcome highlights | Complications/risk signals |
|---|---|---|---|---|---|---|---|
| Halvorson et al. 2014 [4] | Narrative review | Evidence synthesis | Combined acetabular fracture with pelvic ring injury; definitions vary across series | Judet-Letournel ring described with OTA/Young-Burgess concepts | Integrated planning based on mechanical interaction identifies scenarios where acetabular fixation facilitates SI joint reduction | Higher injury burden (ISS) and morbidity than isolated fracture patterns | Emphasizes multidisciplinary care and physiological optimization to manage systemic morbidity |
| Veerappa et al. 2020 [6] | Systematic review (PRISMA) | 8 Retrospective series (≥20 cases) | Combined pelvic and acetabular injuries (heterogeneous definitions) | Lack of standardized terminology | Consensus-based sequencing: reinforces “ring first” standard (posterior → acetabulum → anterior) based on pooled series | Reported incidence: 5%–16% of pelvic/acetabular injuries; transverse and both-column patterns are most frequent | Confirms that heterogeneous definitions and a lack of standardized terminology limit strong comparative conclusions |
| Ross et al. 2023 [5] | Systematic review (PRISMA) | 11 Series (985 patients) | Combined pelvic ring + acetabular fractures (ipsilateral/contralateral included) | Lack of standardized terminology | Sequencing remains debated; unstable rings are often managed with ring first logic; acetabular reduction quality is emphasized | Across studies: mean ISS ~23; pooled mortality ~8%; functional metrics inconsistently reported | Calls for standardized definitions, radiographic metrics, and PROMs |
| Puchwein et al. 2024 [2] | State-of-the-art review | Algorithmic framework | Emphasizes mechanically connected patterns (MCAPI) vs. less connected combinations | Judet-Letournel (acetabulum) + AO/OTA (ring); APC/LC as adjunct | For MCAPI: pelvic ring first (sacrum/SI joint) is generally favored; acetabulum-first is reserved for selected cases with stable posterior rings | Definitive fixation within an early window (~3 to 7 days) is ideal, subject to physiologic and soft-tissue status | Temporary stabilization pitfalls: inadequate initial stability can compromise definitive reduction; emphasize planning for complex coupling |
| Suzuki et al. 2010 [12] | Retrospective cohort (Level I) | 82 Combined (68 operative) | Unstable pelvic injury plus displaced acetabular fracture treated at a Level I center | OTA/Young-Burgess (ring); OTA acetabulum descriptors | Reference-frame principle: prioritizes posterior ring reduction to establish a stable foundation before articular fixation | Mean time to surgery: 5.7 days; | Residual posterior pelvic displacement is a significant predictor of poor acetabular reduction quality |
| Mean postoperative acetabular displacement: 2.2 mm | |||||||
| Osgood et al. 2013 [1] | Retrospective pattern study | 40 Combined (institutional database) | Combined pelvic ring disruption + acetabular fracture identified from institutional registry | Young-Burgess (ring); Letournel (acetabulum) | Morphological mapping: defines common injury combinations, providing a basis for initial planning and corridor assessment | Distribution: APC (53%), LC (45%), VS (3%); | High systemic injury burden: mortality rate of ~13%, characterized by high ISS and frequent associated injuries |
| Posterior wall fractures are significantly less common (~5%) than in isolated cohorts | |||||||
| Cai et al. 2017 [10] | Retrospective case series | 21 Operative | Unstable pelvic fractures with concomitant acetabular fractures are managed operatively | Tile (pelvis) & Letournel (acetabulum) approach- and fixation-based reporting; Matta and functional scores used | Individualized planning: focuses on patient-specific surgical approach and corridor selection when a standardized sequence is not applicable | Functional success: Majeed excellent/good in 85.7% (18/21) at final follow-up | Reports specific complications, including heterotopic ossification, femoral head necrosis, and iatrogenic neurovascular injury |
| Li et al. 2023 [17] | Retrospective case series | 24 Tile B/C | Unstable pelvic fractures combined with acetabular fractures (single center) | Tile (ring); Judet-Letournel (acetabulum) | Posterior-first preference: emphasizes stabilizing posterior ring alignment to provide a reliable template for complex acetabular reconstruction | High functional success: Majeed excellent/good (87.5%) and Merle d’Aubigne excellent/good (83.3%) at final follow-up | Reinforces that anatomic restoration through morphology-based sequencing yields favorable long-term functional results |
| Cunningham et al. 2023 [16] | Retrospective risk-factor study | 70 (≥1-yr follow-up) | Operatively treated combined ring + acetabulum injuries (single Level I center) | Not classification-driven; focuses on predictors of complications | Percutaneous acetabular methods are associated with fewer complications than open approaches | Overall complication rate: 44%; | Hip dislocation is a major predictor of all-cause complications and residual neurologic deficits; angio/embolization is not linked to deep infection |
| Hip dislocation incidence: 40% | |||||||
| Fratus et al. 2025 [13] | Retrospective comparative cohort | 45 (posterior-first vs. others) | Adults requiring operative management; excluded are stable ring/nonoperative acetabulum/nondisplaced percutaneous acetabulum | Postoperative CT step-off and gapping endpoints | Posterior-first preference: validates that addressing the posterior ring first leads to superior anatomic reduction of the acetabulum on CT | CT-based endpoints: anatomic step-off (68.2% vs. 30.4%) and gapping (27.3% vs. 4.4%) significantly favor the posterior-first approach | Reinforces reduction quality but notes that correlation with long-term PROMs remains uncertain |
Definitions and outcomes vary across studies; this table summarizes dominant decision points and sequencing signals rather than prescribing a single universal protocol.
OTA, Orthopedic Trauma Association; ISS, injury severity score; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses; PROM, patient-reported outcome measure; MCAPI, mechanically connected acetabular and pelvic ring injuries (working framework); AO/OTA, Arbeitsgemeinschaft für Osteosynthesefragen/Orthopedic Trauma Association; APC/LC/VS, anteroposterior compression/lateral compression/vertical shear (Young-Burgess); SI joint, sacroiliac joint; CT, computed tomography;
- 1. Osgood GM, Manson TT, O'Toole RV, Turen CH. Combined pelvic ring disruption and acetabular fracture: associated injury patterns in 40 patients. J Orthop Trauma 2013;27:243-7.ArticlePubMed
- 2. Puchwein P, Sandersjoo G, Lindahl J, Eibinger N. Combined pelvic ring and acetabular fractures: strategies and sequence of surgery. State of the art. Arch Orthop Trauma Surg 2024;144:4577-86.ArticlePubMedPMCPDF
- 3. Gänsslen A, Pohlemann T, Paul C, Lobenhoffer P, Tscherne H. Epidemiology of pelvic ring injuries. Injury 1996;27 Suppl 1:S-A13-20.ArticlePubMed
- 4. Halvorson JJ, Lamothe J, Martin CR, et al. Combined acetabulum and pelvic ring injuries. J Am Acad Orthop Surg 2014;22:304-14.ArticlePubMed
- 5. Ross H, Stine S, Blue K, Wolterink TD, Vaidya R. Systematic review of combined pelvic ring and acetabular injuries: what do we know from the literature? Cureus 2023;15:e41843. ArticlePubMedPMC
- 6. Veerappa LA, Tippannavar A, Goyal T, Purudappa PP. A systematic review of combined pelvic and acetabular injuries. J Clin Orthop Trauma 2020;11:983-8.ArticlePubMedPMC
- 7. Burgess AR, Eastridge BJ, Young JW, et al. Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma 1990;30:848-56.PubMed
- 8. Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. Preliminary report. J Bone Joint Surg Am 1964;46:1615-46.PubMed
- 9. Letournel E. Acetabulum fractures: classification and management. Clin Orthop Relat Res 1980;81-106.Article
- 10. Cai L, Lou Y, Guo X, Wang J. Surgical treatment of unstable pelvic fractures with concomitant acetabular fractures. Int Orthop 2017;41:1803-11.ArticlePubMedPDF
- 11. Porter SE, Schroeder AC, Dzugan SS, Graves ML, Zhang L, Russell GV. Acetabular fracture patterns and their associated injuries. J Orthop Trauma 2008;22:165-70.ArticlePubMed
- 12. Suzuki T, Smith WR, Hak DJ, et al. Combined injuries of the pelvis and acetabulum: nature of a devastating dyad. J Orthop Trauma 2010;24:303-8.ArticlePubMed
- 13. Fratus A, Nirunsuk P, Tucker NJ, Parry JA, Mauffrey C. Combined pelvic and acetabular injuries: Decision making and clinical results. Injury 2025;56:112364.ArticlePubMed
- 14. Gansslen A, Lindahl J, Krappinger D, Lindtner RA, Staresinic M. Outcome of pelvic ring injuries. Arch Orthop Trauma Surg 2024;145:47.ArticlePubMedPMC
- 15. Mauffrey C, Bellas N, David G, Le Baron M. Understanding acetabular fractures: a comprehensive review. J Am Acad Orthop Surg 2025 Dec 22 [Epub]. https://doi.org/10.5435/JAAOS-D-25-00741. Article
- 16. Cunningham B, Pearson J, McGwin G, et al. What are the risk factors for complications after combined injury of the pelvic ring and acetabulum? Eur J Orthop Surg Traumatol 2023;33:341-6.ArticlePubMedPDF
- 17. Li R, Zhao P, Guan J, Wang X, Liu L, Wu M. Combined pelvic, acetabular injuries: clinical features and treatment strategies of a unique injury pattern. J Orthop Surg Res 2023;18:415.ArticlePubMedPMC
- 18. Marchand LS, Sepehri A, Hannan ZD, et al. Pelvic ring injury mortality: are we getting better? J Orthop Trauma 2022;36:81-6.ArticlePubMedPMC
- 19. Cuthbert R, Walters S, Ferguson D, et al. Epidemiology of pelvic and acetabular fractures across 12-mo at a level-1 trauma centre. World J Orthop 2022;13:744-52.ArticlePubMedPMC
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteCombined acetabular and pelvic ring injuries: a reference-frame algorithm for definitive fixation sequencing
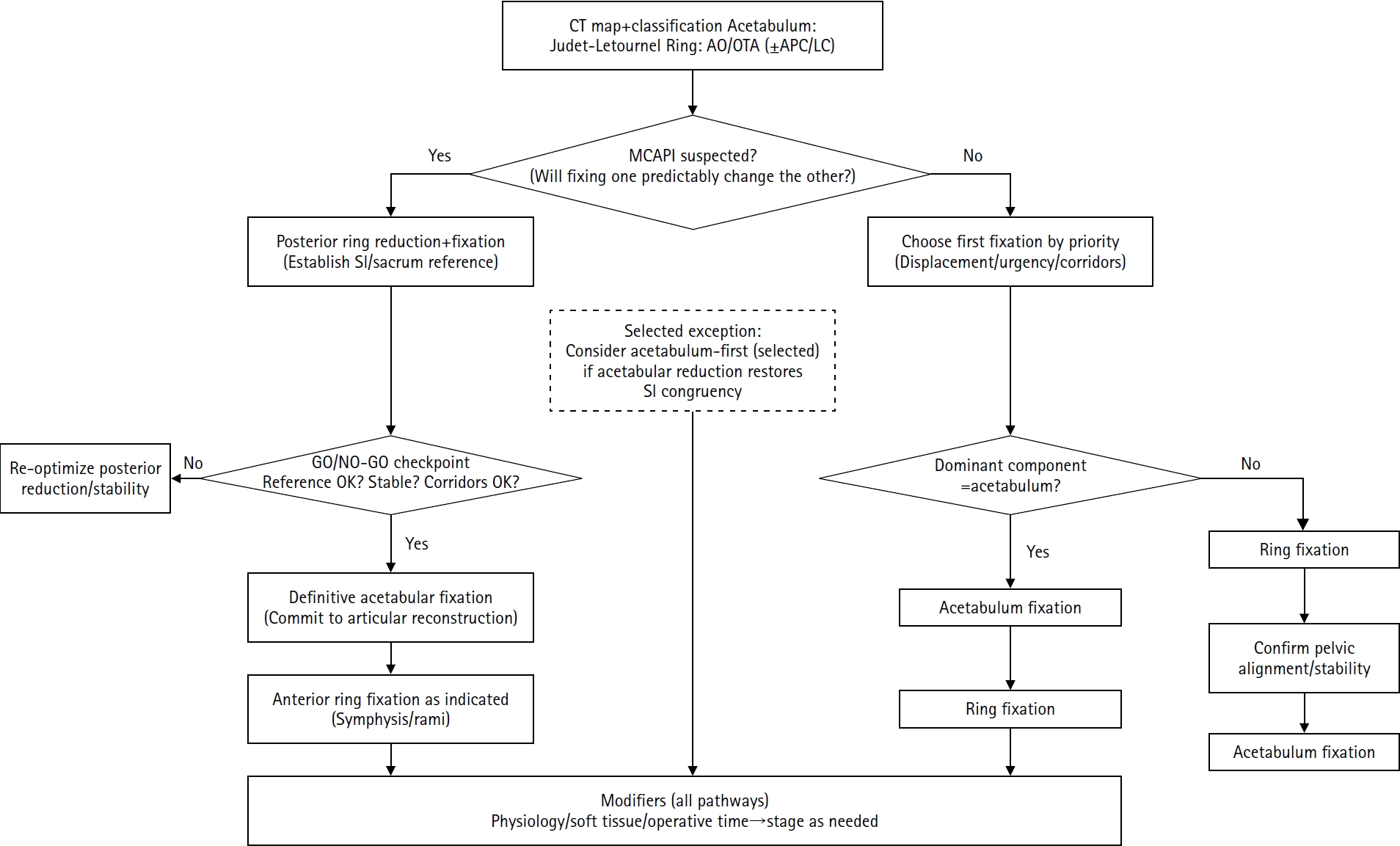
Fig. 1. Reference-frame algorithm for definitive fixation sequencing in combined pelvic ring and acetabular injuries.Following computed tomography (CT)-based morphological mapping (Judet-Letournel for the acetabulum; AO/OTA ± APC/LC for the pelvic ring), the surgical sequence is guided by the presence or absence of mechanical coupling (MCAPI). In suspected MCAPI patterns, posterior ring stabilization is performed to establish a stable sacroiliac and sacral reference, after which a critical GO/NO-GO checkpoint is applied to confirm reference stability and operative corridor feasibility before proceeding with definitive articular reconstruction. In non-MCAPI patterns, the initial fixation target is selected based on the degree of displacement, clinical urgency, and corridor feasibility. Regardless of the chosen sequence, pelvic alignment and overall stability must be reconfirmed before committing to final joint surface reconstruction. Staged surgery may be required in some cases because of physiological status or soft-tissue considerations. CT, computed tomography; AO/OTA, Arbeitsgemeinschaft für Osteosynthesefragen/Orthopedic Trauma Association; APC/LC, anteroposterior compression/lateral compression; MCAPI, mechanically connected acetabular and pelvic ring injuries; SI, sacroiliac.
Fig. 1.
Combined acetabular and pelvic ring injuries: a reference-frame algorithm for definitive fixation sequencing
| Study (yr) | Design | No./scope | Definition/inclusion (as used) | Classification | Sequencing/strategy (key message) | Outcome highlights | Complications/risk signals |
|---|---|---|---|---|---|---|---|
| Halvorson et al. 2014 [4] | Narrative review | Evidence synthesis | Combined acetabular fracture with pelvic ring injury; definitions vary across series | Judet-Letournel ring described with OTA/Young-Burgess concepts | Integrated planning based on mechanical interaction identifies scenarios where acetabular fixation facilitates SI joint reduction | Higher injury burden (ISS) and morbidity than isolated fracture patterns | Emphasizes multidisciplinary care and physiological optimization to manage systemic morbidity |
| Veerappa et al. 2020 [6] | Systematic review (PRISMA) | 8 Retrospective series (≥20 cases) | Combined pelvic and acetabular injuries (heterogeneous definitions) | Lack of standardized terminology | Consensus-based sequencing: reinforces “ring first” standard (posterior → acetabulum → anterior) based on pooled series | Reported incidence: 5%–16% of pelvic/acetabular injuries; transverse and both-column patterns are most frequent | Confirms that heterogeneous definitions and a lack of standardized terminology limit strong comparative conclusions |
| Ross et al. 2023 [5] | Systematic review (PRISMA) | 11 Series (985 patients) | Combined pelvic ring + acetabular fractures (ipsilateral/contralateral included) | Lack of standardized terminology | Sequencing remains debated; unstable rings are often managed with ring first logic; acetabular reduction quality is emphasized | Across studies: mean ISS ~23; pooled mortality ~8%; functional metrics inconsistently reported | Calls for standardized definitions, radiographic metrics, and PROMs |
| Puchwein et al. 2024 [2] | State-of-the-art review | Algorithmic framework | Emphasizes mechanically connected patterns (MCAPI) vs. less connected combinations | Judet-Letournel (acetabulum) + AO/OTA (ring); APC/LC as adjunct | For MCAPI: pelvic ring first (sacrum/SI joint) is generally favored; acetabulum-first is reserved for selected cases with stable posterior rings | Definitive fixation within an early window (~3 to 7 days) is ideal, subject to physiologic and soft-tissue status | Temporary stabilization pitfalls: inadequate initial stability can compromise definitive reduction; emphasize planning for complex coupling |
| Suzuki et al. 2010 [12] | Retrospective cohort (Level I) | 82 Combined (68 operative) | Unstable pelvic injury plus displaced acetabular fracture treated at a Level I center | OTA/Young-Burgess (ring); OTA acetabulum descriptors | Reference-frame principle: prioritizes posterior ring reduction to establish a stable foundation before articular fixation | Mean time to surgery: 5.7 days; | Residual posterior pelvic displacement is a significant predictor of poor acetabular reduction quality |
| Mean postoperative acetabular displacement: 2.2 mm | |||||||
| Osgood et al. 2013 [1] | Retrospective pattern study | 40 Combined (institutional database) | Combined pelvic ring disruption + acetabular fracture identified from institutional registry | Young-Burgess (ring); Letournel (acetabulum) | Morphological mapping: defines common injury combinations, providing a basis for initial planning and corridor assessment | Distribution: APC (53%), LC (45%), VS (3%); | High systemic injury burden: mortality rate of ~13%, characterized by high ISS and frequent associated injuries |
| Posterior wall fractures are significantly less common (~5%) than in isolated cohorts | |||||||
| Cai et al. 2017 [10] | Retrospective case series | 21 Operative | Unstable pelvic fractures with concomitant acetabular fractures are managed operatively | Tile (pelvis) & Letournel (acetabulum) approach- and fixation-based reporting; Matta and functional scores used | Individualized planning: focuses on patient-specific surgical approach and corridor selection when a standardized sequence is not applicable | Functional success: Majeed excellent/good in 85.7% (18/21) at final follow-up | Reports specific complications, including heterotopic ossification, femoral head necrosis, and iatrogenic neurovascular injury |
| Li et al. 2023 [17] | Retrospective case series | 24 Tile B/C | Unstable pelvic fractures combined with acetabular fractures (single center) | Tile (ring); Judet-Letournel (acetabulum) | Posterior-first preference: emphasizes stabilizing posterior ring alignment to provide a reliable template for complex acetabular reconstruction | High functional success: Majeed excellent/good (87.5%) and Merle d’Aubigne excellent/good (83.3%) at final follow-up | Reinforces that anatomic restoration through morphology-based sequencing yields favorable long-term functional results |
| Cunningham et al. 2023 [16] | Retrospective risk-factor study | 70 (≥1-yr follow-up) | Operatively treated combined ring + acetabulum injuries (single Level I center) | Not classification-driven; focuses on predictors of complications | Percutaneous acetabular methods are associated with fewer complications than open approaches | Overall complication rate: 44%; | Hip dislocation is a major predictor of all-cause complications and residual neurologic deficits; angio/embolization is not linked to deep infection |
| Hip dislocation incidence: 40% | |||||||
| Fratus et al. 2025 [13] | Retrospective comparative cohort | 45 (posterior-first vs. others) | Adults requiring operative management; excluded are stable ring/nonoperative acetabulum/nondisplaced percutaneous acetabulum | Postoperative CT step-off and gapping endpoints | Posterior-first preference: validates that addressing the posterior ring first leads to superior anatomic reduction of the acetabulum on CT | CT-based endpoints: anatomic step-off (68.2% vs. 30.4%) and gapping (27.3% vs. 4.4%) significantly favor the posterior-first approach | Reinforces reduction quality but notes that correlation with long-term PROMs remains uncertain |
Table 1. Core evidence matrix for combined acetabular-pelvic ring injuries (10 key studies)
Definitions and outcomes vary across studies; this table summarizes dominant decision points and sequencing signals rather than prescribing a single universal protocol. OTA, Orthopedic Trauma Association; ISS, injury severity score; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses; PROM, patient-reported outcome measure; MCAPI, mechanically connected acetabular and pelvic ring injuries (working framework); AO/OTA, Arbeitsgemeinschaft für Osteosynthesefragen/Orthopedic Trauma Association; APC/LC/VS, anteroposterior compression/lateral compression/vertical shear (Young-Burgess); SI joint, sacroiliac joint; CT, computed tomography;

