 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(2); 2026 > Article
-
Review Article
- Nonoperative management of distal radius fractures: when and how?
- Shin Woo Choi1, Jae Kwang Kim2
-
Journal of Musculoskeletal Trauma 2026;39(2):93-102.
DOI: https://doi.org/10.12671/jmt.2026.00024
Published online: March 10, 2026
1Department of Orthopedic Surgery, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea
2Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- Correspondence to: Jae Kwang Kim Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-3523, Email: orth4535@gmail.com
• Received: January 6, 2026 • Revised: January 28, 2026 • Accepted: January 29, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,910 Views
- 28 Download
Abstract
- Distal radius fractures are among the most common injuries of the upper extremity, particularly in the elderly population. Although the use of volar locking plate fixation has increased in recent years, evidence from randomized and prospective studies demonstrates that, while operative treatment may achieve superior radiographic alignment and enable more rapid early recovery, these advantages tend to diminish over time and do not result in superior long-term patient-reported functional outcomes in elderly patients. In addition, radiographic parameters show only a limited correlation with functional recovery. Consequently, nonoperative treatment remains a valid and important treatment option for distal radius fractures. The decision to pursue nonoperative management should be based on a comprehensive assessment of radiographic parameters—including dorsal tilt, radial shortening, and intraarticular displacement—together with patient-specific factors such as age, activity level, comorbidities, and functional expectations. For stable or minimally displaced fractures, an immobilization period of 3‒4 weeks is generally recommended, whereas displaced fractures typically require immobilization for 5‒6 weeks. In cases requiring manual reduction, traditional treatment protocols recommend weekly radiographic follow-up during the first 2‒3 weeks to monitor for secondary displacement. Successful nonoperative management should also emphasize effective swelling control through limb elevation, as well as the initiation of early finger exercises to prevent hand stiffness. After removal of the cast or splint, active wrist mobilization is essential for restoring optimal range of motion and achieving functional recovery.
Introduction
Distal radius fractures are the most common fractures occurring in the elderly and are known to account for approximately 18% of all fractures in patients over 65 years of age [1]. As an initial treatment strategy, stable and nondisplaced fractures are immobilized immediately with a splint without attempting reduction, whereas in fractures with marked displacement—such as pronounced angular deformity or radial shortening—manual reduction is performed to decrease swelling and pain prior to splint application. Subsequently, decisions regarding operative versus nonoperative management are made by considering radiographic stability and morphology of the fracture, the patient’s age, activity level, underlying comorbidities, and the functional level the patient desires to achieve after recovery. This decision-making process is often challenging.
Operative treatments for distal radius fractures have included closed reduction and percutaneous pinning or external fixation. Over the past several decades, with the development and advancement of locking plates, the frequency of open reduction and internal fixation has increased. In particular, the introduction of anatomically contoured volar locking plates has made it easier to improve and maintain anatomical alignment without displacement even in distal radius fractures where metaphyseal bone quality is poor [2]. However, percutaneous pinning and external fixation have been associated with weak fixation strength, difficulty in obtaining and maintaining articular reduction, and the risk of joint or fracture-site infection due to externally exposed hardware. Volar locking plate fixation also carries a significant complication profile, ranging from mild issues such as flexor tendon irritation and median nerve symptoms to serious complications such as surgical site infection, flexor tendon rupture, and carpal tunnel syndrome; complication rates as high as 16.5% have been reported [3].
Given that such complications remain a concern, that a considerable proportion of distal radius fractures are stable, and that in elderly patients even unstable fractures do not always show a direct correlation between the accuracy of anatomic reduction and functional outcome [4], nonoperative treatment continues to represent an important treatment principle. Accordingly, the authors review established knowledge and current perspectives regarding the nonoperative management of distal radius fractures.
The aim of this narrative review is to synthesize contemporary evidence on the nonoperative management of distal radius fractures and to provide practical, stepwise guidance for fracture reduction, immobilization, follow-up imaging, and rehabilitation. Rather than advocating uniform radiographic thresholds across all patients, we present an evidence-informed decision-making framework stratified by patient age, comorbidity burden, and functional demand. Particular emphasis is placed on older, lower-demand patients, in whom long-term patient-reported outcomes after operative and nonoperative treatment may converge despite differences in radiographic alignment.
Written informed consent was obtained from the patients for publication of their images in this review.
Literature search strategy
This narrative review was informed by a targeted search of PubMed/Medline from inception through December 2025 (last searched December 2025). Search terms were combined using Boolean operators and truncation and included distal radius fracture, nonoperative treatment, casting, splinting, immobilization, and volar locking plate. An example query was (“distal radius fracture” OR “wrist fracture”) AND (cast OR splint OR immobilization) AND (nonoperative OR conservative). We prioritized randomized clinical trials, systematic reviews and meta-analyses, and clinical practice guidelines; reference lists of key articles were also screened. We focused on adults with displaced or potentially unstable distal radius fractures. Because this is a narrative review, study selection was pragmatic rather than exhaustive, and recommendations were anchored to higher-level evidence when available.
Clinical considerations in nonoperative treatment
The general goal of fracture treatment is to achieve bony union in the original anatomical position or in a position close to it, thereby preventing sequelae associated with the fracture. Distal radius fractures mainly involve the metaphyseal region, where abundant soft tissue and vascular supply allow relatively reliable bone healing compared with other anatomical areas. Thus, the role of nonoperative treatment is to maintain the anatomical or near-anatomical alignment during the healing process to prevent long-term complications. Common sequelae associated with distal radius fractures include posttraumatic arthritis, decreased wrist range of motion, ulnar-sided wrist pain, and decreased grip strength. Therefore, clinicians must evaluate the condition of the distal radius fracture at the time of injury to determine whether nonoperative treatment is appropriate, identify radiographic parameters or criteria associated with the development of sequelae, and determine whether nonoperative treatment can be continued if displacement occurs during the course of conservative management.
Radiographic parameters for assessing anatomical displacement
Radial shortening and positive ulnar variance caused by metaphyseal impaction of the distal radius increase tension on the triangular fibrocartilage complex and load on the distal radioulnar joint (DRUJ), potentially leading to articular surface damage, pain, and restricted forearm rotation. Specifically, compared with normal anatomy, a radial shortening of 2.5 mm increases the load on the distal ulna by approximately 18%–42% [5], and a shortening of 10 mm may result in a loss of 47% of pronation and 29% of supination [6].
Improper reduction of intraarticular fractures is a representative cause of posttraumatic arthritis and subsequent limitation of joint motion and pain. Even 1–2 mm of intraarticular incongruity is known to induce arthritis and lead to poor outcomes. Knirk and Jupiter [7] reported that >1 mm of intraarticular incongruity resulted in radiographic arthritis in 91% of cases, and that all patients with ≥2 mm of incongruity developed radiographic arthritis.
Abnormal volar or dorsal tilt of the distal radius in the sagittal plane is associated with wrist range of motion, particularly flexion and extension. As dorsal tilt increases, the load-bearing area shifts from the volar-radial side to the dorsal-ulnar side, leading to compensatory flexion at the midcarpal joint. This can result in painful synovitis and a form of dorsal intercalated segment instability [8,9]. Conversely, excessive volar tilt reduces wrist extension and may cause dorsal subluxation of the ulnar head and restricted supination [10].
Changes in radial inclination affect grip strength, radial and ulnar deviation, and load distribution across the wrist. It has been reported that patients with radial inclination less than 5° experience poor outcomes in 100% of cases [11].
Radiographic and clinical indications
To consider nonoperative treatment immediately after injury, criteria that predict the likelihood of subsequent displacement are necessary, and numerous studies have been conducted on this topic. Weber [12] defined unstable fractures as those in which dorsal cortical comminution exceeds 50% of the anteroposterior diameter of the fracture site on the sagittal view. Cooney [13] classified fractures as unstable if initial radiographs demonstrated >25° of dorsal tilt, >10 mm of radial shortening, or bilateral radius fractures. Lafontaine et al. [14] proposed more specific criteria, widely used for assessing instability, including: >20° dorsal tilt, >5 mm radial shortening, >50% dorsal comminution, intraarticular displacement, associated ulnar metaphyseal fracture, shear fracture of the distal radius, DRUJ fracture-dislocation, and early loss of reduction after initial reduction—meeting three or more of these conditions suggests an unstable fracture.
Radiographic criteria for determining whether to proceed with operative treatment after successful reduction have also been extensively studied. With advances in surgical techniques and implants, operative treatment has shown improved outcomes, narrowing the indications for conservative management, especially in younger patients with high functional demands. Radial shortening of >2 mm, DRUJ subluxation, and significant anteroposterior translation of the distal ulna are generally considered unsuitable for conservative treatment. However, acceptable thresholds for intraarticular incongruity (<1 mm vs. <2 mm) and dorsal tilt (allowing up to 10° vs. allowing only neutral alignment) remain controversial (Fig. 1) [15-19]. Randomized controlled trials comparing conservative and operative treatment for displaced distal radius fractures have consistently demonstrated superior radiographic alignment following surgical fixation, particularly with respect to volar tilt and radial inclination at final follow-up [20]. Several studies have also reported modest advantages in early functional recovery and grip strength in surgically treated patients during the initial postoperative period [21,22]. However, long-term follow-up data in elderly populations indicate that these early advantages do not persist over time. Large prospective studies have shown that although volar locking plate fixation may facilitate faster early recovery, it does not confer superior patient-reported outcomes at 12 months when compared with cast immobilization [23,24]. In line with these findings, a comprehensive systematic review and meta-analysis by Gutierrez-Espinoza et al. [25] concluded that while statistically significant differences in radiologic and functional outcomes favor volar plate fixation, these differences do not exceed minimal clinically important difference thresholds. Furthermore, ulnar variance did not differ significantly between treatment groups, and radiographic parameters showed limited correlation with long-term clinical outcomes (Table 1) [20,22,24,26-28]. Collectively, these data suggest that despite the potential for radiographic malunion in conservatively managed cases, long-term functional recovery is not inferior to surgical intervention, supporting nonoperative management as a viable primary treatment option.
Rather than applying strict radiographic criteria uniformly across all patients, more stringent criteria may be appropriate for younger, active individuals, while more flexible thresholds may be suitable for elderly patients with comorbidities or low functional demands. In particular, several studies have reported that unsatisfactory radiographic results do not always correlate with unsatisfactory functional outcomes in elderly patients [29,30]. Kyung et al. [31] reported that dorsal metaphyseal comminution did not significantly affect radiographic or functional outcomes in patients treated nonoperatively. Kim et al. [32] compared elderly patients (≥65 years) treated nonoperatively versus operatively for unstable distal radius fractures and found that although radial shortening was more pronounced in the nonoperative group, functional evaluation and wrist range of motion did not differ significantly between groups. A recent randomized trial of intraarticular fractures found that intraarticular incongruity did not significantly affect functional outcomes, even though radiographic differences were present (Fig. 2) [16]. These findings support the premise that in elderly patients with lower functional demands, nonoperative treatment can achieve satisfactory outcomes even when anatomical restoration is not perfect.
In addition to radiographic findings, clinical features such as concomitant fractures in the ipsilateral upper extremity, carpal fractures or dislocations, severe soft-tissue damage, or associated neurovascular injury warrant consideration of operative treatment as a priority [15].
Reduction of the fracture and postinjury management
When dorsal metaphyseal comminution is mild, radial length is relatively preserved, or angulation/displacement is minimal, additional fracture reduction is not required. In displaced fractures, longitudinal traction is applied along the forearm with adequate pronation of the hand while directing the distal fragment opposite to the direction of displacement in order to achieve reduction. Typically, the wrist is immobilized in approximately 20°–30° of flexion with ulnar deviation. If needed, local injection of lidocaine at the dorsal aspect of the fracture may be used before attempting reduction to provide pain relief and allow effective traction.
Elevation of the hand is essential to prevent swelling after injury. The use of a sling is not recommended because it positions the hand below the level of the heart; instead, the hand should always be kept above the elbow. Continuous finger motion is necessary. Importantly, finger motion must include full metacarpophalangeal (MCP) joint flexion and full interphalangeal (IP) joint extension rather than motion limited to the IP joints alone (Fig. 3). If active exercise alone is insufficient, assisted active exercise using the contralateral hand should be performed so that the patient can fully clench the fist and achieve full finger extension. Assisted exercises should apply sustained, gentle pressure rather than abrupt force to the joints. Additionally, during prolonged immobilization, contractures may develop in nonimmobilized joints such as the shoulder or elbow; therefore, these joints should be moved regularly from the time of injury [33].
Type and duration of splint or cast immobilization
Because considerable swelling is present immediately after injury, excessive compression during initial bandage or plaster application should be avoided. Joints not requiring immobilization—such as the shoulder and the MCP joints—should remain as mobile as possible. In particular, excessive pressure during plaster wrapping can lead to circulatory compromise, and improper molding before the plaster sets may result in pressure over bony prominences (e.g., radial or ulnar styloid, posterior ulna), causing skin necrosis, nerve palsy, or vascular insufficiency [33].
Various immobilization techniques for conservative treatment of distal radius fractures include sugar-tong splints, long-arm splints or casts, short-arm double splints, short-arm splints or casts, and radial gutter short-arm splints. Among these, sugar-tong splint is most commonly used immediately after injury. It partially restricts elbow motion while preventing forearm rotation in an effort to reduce loss of reduction [34]. However, sugar-tong splints may be uncomfortable during elevation due to their weight, and restriction of elbow motion can lead to elbow stiffness [35,36].
Randomized controlled trials have demonstrated that immobilization methods not involving the elbow provide stability comparable to elbow-including methods, with fewer immobilization-related complications [17,37]. Therefore, the necessity of elbow immobilization in conservative management of distal radius fractures remains controversial. Grafstein et al. [38] also reported no significant differences in redisplacement rates or functional recovery among sugar-tong splints, short-arm double splints, and short-arm casts in displaced distal radius fractures, recommending that physicians use the method they are most familiar with. The American Academy of Orthopaedic Surgeons (AAOS) clinical practice guideline similarly states that there is insufficient evidence to determine the superiority or necessity of elbow immobilization in conservative treatment of distal radius fractures [39].
Emerging technologies such as 3D-printed custom splints have been introduced as alternatives to conventional immobilization. These patient-specific devices, designed based on forearm surface scanning and fabricated using additive manufacturing, offer potential advantages including reduced weight, improved ventilation, and water resistance. A recent randomized controlled trial comparing 3D-printed splints to fiberglass casts in minimally displaced distal radius fractures demonstrated equivalent patient satisfaction and clinical effectiveness, although minor complications such as pressure points and splint breakage occurred more frequently in the 3D-printed group and required design modifications [40].
Regardless of the immobilization technique, it is essential to avoid crossing the metacarpal heads with the distal end of the splint or cast to permit MCP flexion to 90° and to prevent finger stiffness. After splint or cast application, the patient should be instructed to move the MCP joints to confirm absence of discomfort.
The recommended duration of immobilization is generally 3–4 weeks for impacted or minimally displaced fractures and 5–6 weeks for displaced fractures [33,35,41]. Recent evidence suggests that shorter immobilization periods may be appropriate for stable fractures. Multiple studies have demonstrated that 1 week of cast immobilization is safe and feasible for nondisplaced or minimally displaced distal radius fractures, potentially resulting in better functional outcomes and faster return to activities [42]. In displaced fractures, long-arm immobilization using a sugar-tong splint or long-arm cast is applied for the first 2–3 weeks, followed by a short-arm cast for an additional 3–4 weeks; however, actual duration may vary depending on fracture characteristics, patient status, and progression of bone healing [19,43,44]. In cases requiring reduction, weekly radiographs for the first 2–3 weeks are necessary to detect redisplacement or deformity, and if present, treatment should be converted to operative management [33].
Rehabilitation after immobilization
After planned immobilization is completed, active mobilization is required to restore wrist range of motion. With the elbow flexed and the upper arm supported on the table, the patient performs wrist flexion, extension, pronation, and supination through active and assisted active exercises [33]. Pain during early rehabilitation is common after prolonged immobilization; nonsteroidal anti-inflammatory drugs and heat therapy may help alleviate symptoms [33].
Evidence integration
Across randomized and prospective comparative studies summarized in Table 1, operative fixation more consistently improves radiographic alignment at final follow-up than function. Functional benefits are less consistent and often time dependent. Interpretation is limited by heterogeneity in fracture patterns (extraarticular vs. intraarticular), definitions of instability and acceptable alignment, baseline functional demand, outcome measures (e.g., the Disabilities of the Arm, Shoulder and Hand [DASH/QuickDASH], the Patient-Rated Wrist Evaluation [PRWE], range of motion, grip strength), and follow-up duration (commonly 12 months). Early between-group differences in motion, strength, or patient-reported outcomes may diminish over time, and statistically significant effects may not meet thresholds for patient-important change (e.g., minimal clinically important difference). Overall, treatment goals should be individualized: radiographic restoration may be more consequential for younger, high-demand patients, whereas many older, lower-demand patients can achieve acceptable long-term function with nonoperative care when early stability is maintained through structured radiographic surveillance and rehabilitation.
Limitations of the evidence and this review
The existing evidence base is heterogeneous with respect to fracture patterns, definitions of instability and acceptable alignment, treatment and rehabilitation protocols, outcome measures, and duration of follow-up, which limits direct cross-study comparison and consistent interpretation of effect sizes. Many trials are underpowered to detect uncommon but clinically important complications, and follow-up is frequently limited to approximately one year, potentially underestimating late sequelae in younger or higher-demand patients. As a narrative review, this synthesis does not include a formal risk-of-bias assessment or structured evidence grading, and the literature search was not intended to be exhaustive. Accordingly, the conclusions presented should be interpreted as evidence-informed guidance to support individualized clinical decision-making rather than as pooled comparative estimates of treatment efficacy.
Conclusions
Nonoperative treatment remains a fundamental option for distal radius fractures, particularly in elderly patients. Treatment selection should integrate radiographic parameters with patient-specific factors including age, activity level, comorbidities, and functional expectations. During nonoperative management, attention must extend beyond fracture reduction and union to include swelling control and prevention of hand stiffness through finger exercises. Following immobilization, active wrist motion should be encouraged to restore range of motion.
-
Author contributions
Conceptualization: SWC, JKK. Supervision: JKK. Writing-original draft: SWC. Writing-review & editing: SWC, JKK. All authors have read and approved the final version of the manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.
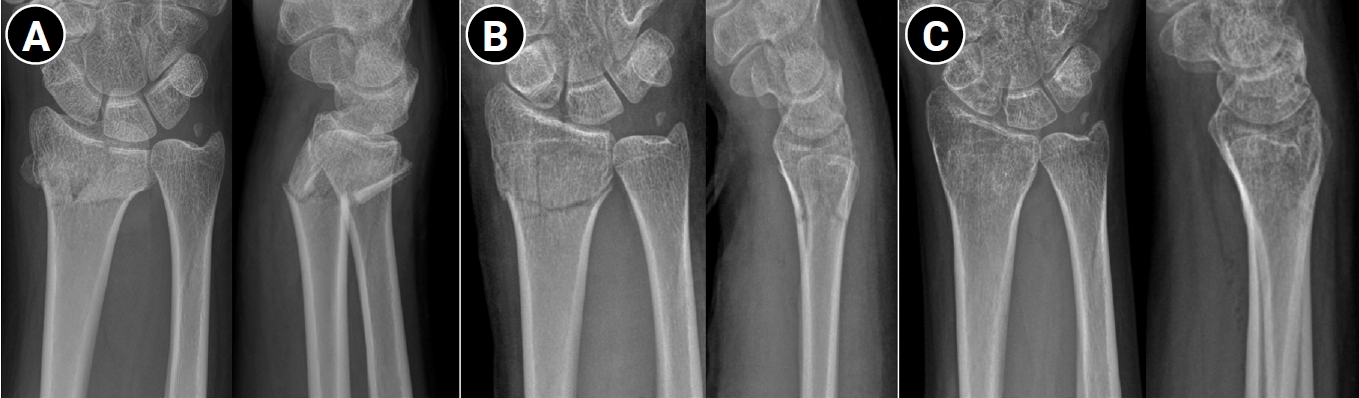
Successful conservative treatment of a displaced distal radius fracture in a 20-year-old female patient. (A) Immediate posttrauma wrist anteroposterior and lateral radiographs demonstrating a dorsally displaced intraarticular distal radius fracture of the right wrist. (B) Wrist radiographs obtained after manual reduction, showing restoration of volar tilt and radial length. (C) Wrist radiographs at 3 months posttrauma, demonstrating maintenance of fracture alignment and satisfactory fracture union.
Fig. 2.
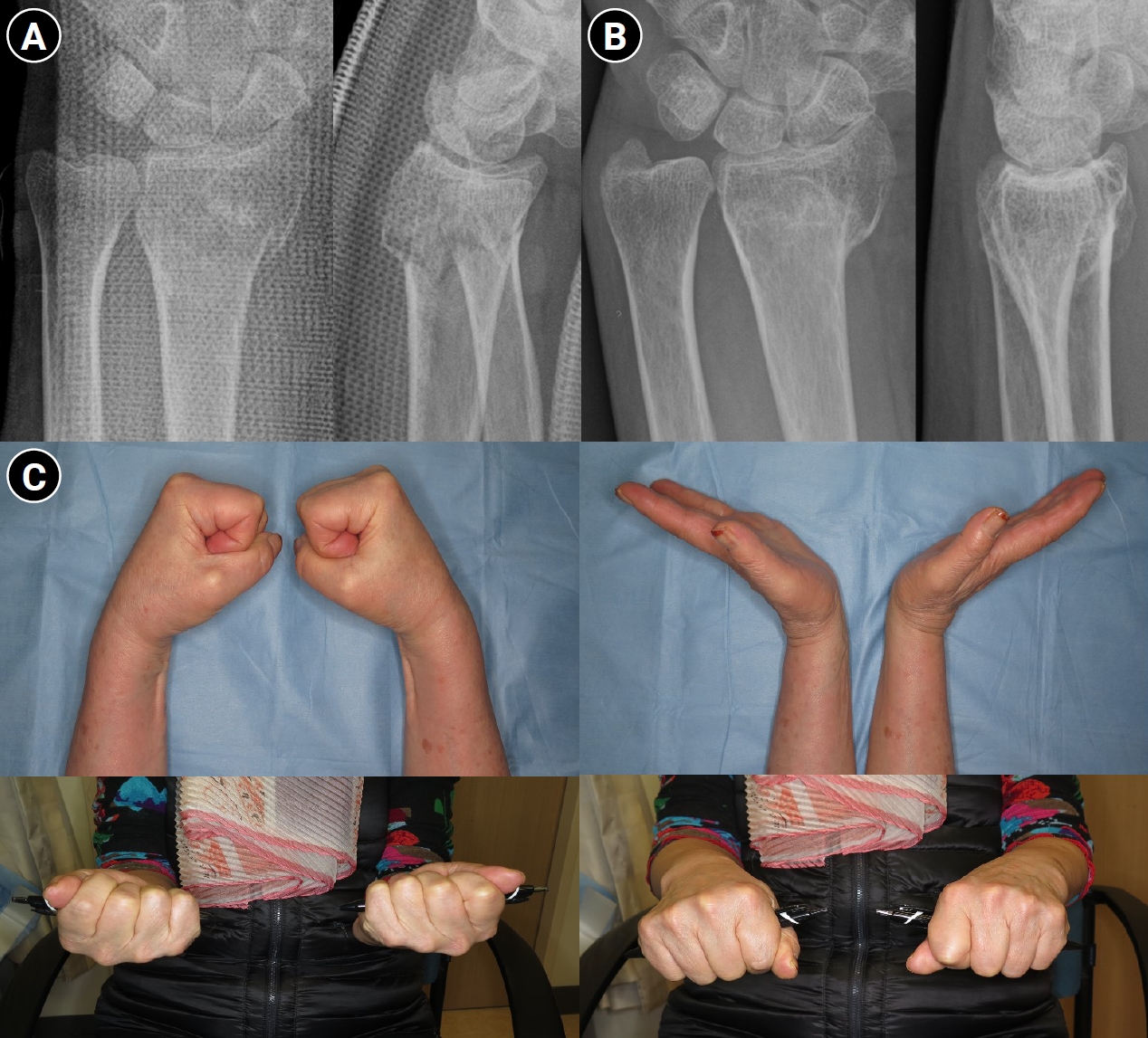
Outcome of conservative treatment in an older patient with a displaced distal radius fracture. Radiographs of a 71-year-old female patient. (A) Wrist anteroposterior and lateral radiographs obtained after initial reduction, demonstrating distal radius and ulnar styloid fractures with intraarticular comminution of the left wrist. Volar tilt and radial length were well restored after reduction. (B) Wrist radiograph obtained 1 year after trauma, showing radial shortening and dorsal tilt of the distal radius. (C) Range of motion of the left wrist was slightly decreased compared with the right side; however, the patient was able to perform daily activities without pain at one year after trauma.
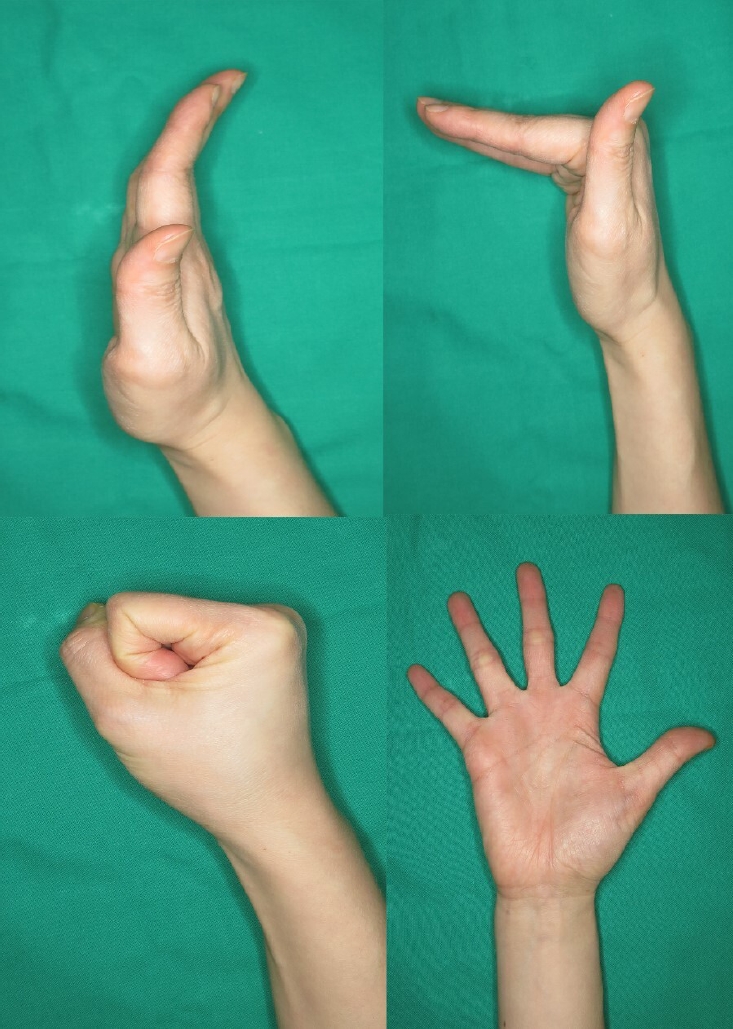
Table 1.
Summary of randomized controlled trials comparing nonoperative and operative treatment for distal radius fracture
| Study | Included patients | Type of treatment | No. | Age (yr) | Sex (male: female) | Severity of fracture (AO type) | Clinical outcomes at final F/U | Radiologic outcomes | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Wrist flexion/extensiona) | Grip strengtha) | Patient-reported outcomes | Dorsal angulation (°)b) | Radial inclination (°)b) | Ulnar variance (mm)b) | |||||||||||||
| Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U | ||||||||||
| 2005, Azzopardi et al. [20] | Unstable, extraarticular fractures | Nonoperative | 27 | 71 | 2:25 | A3 | 88.5% | 72% | SF-36 physical: 38.2 | 29±16 | ‒5±7 | 4±8 | 18±6 | 21±3 | 19±6 | 3±3 | 0±1 | 3±2 |
| Percutaneous pinning | 27 | 72 | 4:23 | A3 | 90.5% | 77% | SF-36 physical: 42.2 | 35±15 | ‒4±7 | ‒3±10c) | 16±6 | 22±3 | 22±5 | 4±3 | 0±1 | 3±2 | ||
| 2010, Wong et al. [28] | Unstable, extraarticular fractures | Nonoperative | 30 | 71 | 5:25 | Frykman classification I:II (18:12) | 143° | 9.0 kg | Mayo wrist scores: 80.5±7.5 | 31±6 | ‒7.5±1 | 3±1 | 13±3 | 23±4 | 16±2 | 4.3±1.2 | 0.5±0.2 | 3.2±1.4 |
| Percutaneous pinning | 30 | 70 | 6:24 | Frykman classification I:II (17:13) | 145° | 8.5 kg | Mayo wrist scores: 82.2±6.2 | 33±6 | ‒8±1 | ‒4±1c) | 13±4 | 23±2 | 20±2c) | 5.2±1.8 | 0.3±0.1 | 2.1±1.1 | ||
| 2011, Arora et al. [26] | Displaced, unstable fractures | Nonoperative | 37 | 77.4 | 10:27 | A2-3, A3-9, C1-11, C2-8, C3-6 | 103.7%c) | 92.6% | DASH scores: 8.0±9.3 | 3.6±11.2 | 10.4±19.1 | 20.3±3.3 | 15.9±9.0 | 0.8±1.7 | 3.2±2.9 | |||
| ORIF with volar locking plate | 36 | 75.9 | 8:28 | A2-3, A3-7, C1-4, C2-12, C3-10 | 92.8% | 102.4%c) | DASH scores: 5.7±11.1 | ‒3.6±6.9c) | ‒0.5±4.7c) | 21.8±2.7c) | 21.2±2.6c) | 0.6±1.6 | 0.7±1.8c) | |||||
| 2014, Sharma et al. [27] | AO type B and C fractures | Nonoperative | 32 | 48.1 | 10:22 | B-13, C-19 | 135.0° | 72.2% | DASH scores: 14.0±10.2 | ‒8.4±0.4 | ‒5.2±0.5 | 18.1±0.9 | 15.2±0.8 | 0.2±0.1 | 0.3±0.1 | |||
| ORIF with volar locking plate | 32 | 52.4 | 9:23 | B-19, C-17 | 168.2°c) | 89.1%c) | DASH scores: 5.0±9.4c) | ‒10.1±1.5c) | ‒8.4±1.0c) | 20.5±1.3c) | 17.9±0.8c) | ‒0.3±0.3 | ‒0.3±0.2 | |||||
| 2019, Saving et al. [22] | Dorsally displaced fractures (≥20° dorsal tilt) | Nonoperative | 64 | 78 | 8:56 | A2-10, A3-28, C1-20, C2-6, C3-0 | 107° | 80.9% | PRWE scores: 22.4±21.4 DASH scores: 23.1±19.8 | 27±8 | 8±8 | 14±13 | 14±8 | 18±6 | 14±7 | 2.3±2.2 | 0.6±1.6 | 2.7±2.2 |
| Volar locking plate | 58 | 80 | 3:55 | A2-6, A3-33, C1-11, C2-7, C3-1 | 118° | 96.0%c) | PRWE scores: 12.7±15.0 DASH scores: 15.6±17.0c) | 31±10 | ‒1±7c) | 1±9c) | 14±13 | 18±8 | 19±8c) | 2.4±2.1 | 0.0±0.3c) | 0.5±1.3c) | ||
| 2021, Hassellund et al. [24] | Displaced, unstable fractures | Nonoperative | 50 | 73.9 | 8:42 | A2-2, A3-12, C1-11, C2-18, C3-7 | 112° | 77% | QuickDASH median: 5 PRWE median: 2 | 23 | 13 | 20 | 18 | 19 | 18 | 3 | 5 | 5 |
| Volar locking plate | 50 | 73.4 | 3:47 | A2-3, A3-9, C1-13, C2-16, C3-9 | 119° | 88%c) | QuickDASH median: 0 PRWE median: 0c) | 21 | ‒1c) | ‒1c) | 19 | 24c) | 25c) | 3 | 2c) | 2c) | ||
Table 1 summarizes key comparative studies. Differences in fracture classification, definitions of instability, and outcome instruments limit direct comparisons across studies. For patient-reported outcomes, statistical significance should be interpreted alongside clinical relevance (e.g., the minimal clinically important difference, when available). Follow-up intervals vary; early functional differences may not persist at later assessments. All of the continuous values are presented as mean or mean±standard deviation.
DASH, Disabilities of the Arm, Shoulder and Hand; SF-36, Short Form-36 Health Survey; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand; PRWE, Patient-Rated Wrist Evaluation.
a)Wrist flexion/extension arc and grip strength of the involved hand are presented as raw data or ratios compared with the contralateral side.
b)Pre denotes the values before the reduction or operation. Post means the values after the reduction or operation. F/U refers to values that were measured at the final follow-up period.
c)The value of this group is statistically significantly better than that of the comparison group.
- 1. Baron JA, Karagas M, Barrett J, et al. Basic epidemiology of fractures of the upper and lower limb among Americans over 65 years of age. Epidemiology 1996;7:612-8.ArticlePubMed
- 2. Orbay JL, Fernandez DL. Volar fixation for dorsally displaced fractures of the distal radius: a preliminary report. J Hand Surg Am 2002;27:205-15.ArticlePubMed
- 3. Bentohami A, de Burlet K, de Korte N, et al. Complications following volar locking plate fixation for distal radial fractures: a systematic review. J Hand Surg Eur Vol 2014;39:745-54.ArticlePubMedPDF
- 4. Kodama N, Takemura Y, Ueba H, Imai S, Matsusue Y. Acceptable parameters for alignment of distal radius fracture with conservative treatment in elderly patients. J Orthop Sci 2014;19:292-7.ArticlePubMed
- 5. Palmer AK, Werner FW. Biomechanics of the distal radioulnar joint. Clin Orthop Relat Res 1984;187:26-35.Article
- 6. Bronstein AJ, Trumble TE, Tencer AF. The effects of distal radius fracture malalignment on forearm rotation: A cadaveric study. J Hand Surg Am 1997;22:258-62.ArticlePubMed
- 7. Knirk JL, Jupiter JB. Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am 1986;68:647-59.ArticlePubMed
- 8. Kazuki K, Kusunoki M, Yamada J, Yasuda M, Shimazu A. Cineradiographic study of wrist motion after fracture of the distal radius. J Hand Surg Am 1993;18:41-6.ArticlePubMed
- 9. Miyake T, Hashizume H, Inoue H, Shi Q, Nagayama N. Malunited Colles’ fracture: analysis of stress distribution. J Hand Surg Br 1994;19:737-42.ArticlePubMed
- 10. Fernandez DL. Malunion of the distal radius: current approach to management. Instr Course Lect 1993;42:99-113.PubMed
- 11. Altissimi M, Antenucci R, Fiacca C, Mancini GB. Long-term results of conservative treatment of fractures of the distal radius. Clin Orthop Relat Res 1986;206:202-10.Article
- 12. Weber ER. A rational approach for the recognition and treatment of Colles’ fracture. Hand Clin 1987;3:13-21.ArticlePubMed
- 13. Cooney WP. Fractures of the distal radius: a modern treatment-based classification. Orthop Clin North Am 1993;24:211-6.ArticlePubMed
- 14. Lafontaine M, Hardy D, Delince P. Stability assessment of distal radius fractures. Injury 1989;20:208-10.ArticlePubMed
- 15. Lee JH. Surgical indications for distal radius fractures. J Korean Soc Surg Hand 2015;20:72-6.Article
- 16. Martinez-Mendez D, Lizaur-Utrilla A, de-Juan-Herrero J. Intra-articular distal radius fractures in elderly patients: a randomized prospective study of casting versus volar plating. J Hand Surg Eur Vol 2018;43:142-7.ArticlePubMedPDF
- 17. Park MJ, Kim JP, Lee HI, et al. Is a short arm cast appropriate for stable distal radius fractures in patients older than 55 years? A randomized prospective multicentre study. J Hand Surg Eur Vol 2017;42:487-92.ArticlePubMedPDF
- 18. Simic PM, Weiland AJ. Fractures of the distal aspect of the radius: changes in treatment over the past two decades. Instr Course Lect 2003;52:185-95.ArticlePubMed
- 19. Song SW. Osteoporotic distal radius fracture-conservative treatment. J Korean Fract Soc 2008;21:81-6.Article
- 20. Azzopardi T, Ehrendorfer S, Coulton T, Abela M. Unstable extra-articular fractures of the distal radius: a prospective, randomised study of immobilisation in a cast versus supplementary percutaneous pinning. J Bone Joint Surg Br 2005;87:837-40.ArticlePubMed
- 21. Haslhofer DJ, Froschauer SM, Gotterbarm T, Schmidt M, Kwasny O, Holzbauer M. Comparison of surgical and conservative therapy in older patients with distal radius fracture: a prospective randomized clinical trial. J Orthop Traumatol 2024;25:46.ArticlePubMedPMCPDF
- 22. Saving J, Wahlgren SS, Olsson K, et al. Nonoperative treatment compared with volar locking plate fixation for dorsally displaced distal radial fractures in the elderly: a randomized controlled trial. J Bone Joint Surg Am 2019;101:961-9.ArticlePubMed
- 23. Chung KC, Kim HM, Malay S, et al. The wrist and radius injury surgical trial: 12-month outcomes from a multicenter international randomized clinical trial. Plast Reconstr Surg 2020;145:1054e-1066e.ArticlePubMedPMC
- 24. Hassellund SS, Williksen JH, Laane MM, et al. Cast immobilization is non-inferior to volar locking plates in relation to QuickDASH after one year in patients aged 65 years and older: a randomized controlled trial of displaced distal radius fractures. Bone Joint J 2021;103-B:247-55.ArticlePubMedPDF
- 25. Gutierrez-Espinoza H, Araya-Quintanilla F, Olguin-Huerta C, et al. Effectiveness of surgical versus conservative treatment of distal radius fractures in elderly patients: a systematic review and meta-analysis. Orthop Traumatol Surg Res 2022;108:103323.ArticlePubMed
- 26. Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am 2011;93:2146-53.ArticlePubMed
- 27. Sharma H, Khare GN, Singh S, Ramaswamy AG, Kumaraswamy V, Singh AK. Outcomes and complications of fractures of distal radius (AO type B and C): volar plating versus nonoperative treatment. J Orthop Sci 2014;19:537-44.ArticlePubMed
- 28. Wong TC, Chiu Y, Tsang WL, Leung WY, Yam SK, Yeung SH. Casting versus percutaneous pinning for extra-articular fractures of the distal radius in an elderly Chinese population: a prospective randomised controlled trial. J Hand Surg Eur Vol 2010;35:202-8.ArticlePubMedPDF
- 29. Jaremko JL, Lambert RG, Rowe BH, Johnson JA, Majumdar SR. Do radiographic indices of distal radius fracture reduction predict outcomes in older adults receiving conservative treatment? Clin Radiol 2007;62:65-72.ArticlePubMed
- 30. Young BT, Rayan GM. Outcome following nonoperative treatment of displaced distal radius fractures in low-demand patients older than 60 years. J Hand Surg Am 2000;25:19-28.ArticlePubMed
- 31. Kyung MG, Chung HW, Kim JS, et al. Closed reduction and cast immobilization for the treatment of distal radius fracture: does dorsal metaphyseal comminution predict radiographic and functional outcomes? J Korean Soc Surg Hand 2013;18:29-36.Article
- 32. Kim JM, Seo HJ, Jeon YD, Lee HM, Son JH. Comparative study of outcomes between operative and non-operative treatment of unstable distal radius fracture in the elderly patients. J Korean Soc Surg Hand 2015;20:43-50.Article
- 33. The Korean Society for Surgery of the Hand. Surgery of the hand. Panmuneducation; 2014.
- 34. Lee JH, Hong SH, Kim YJ, Back JH, Lee JS. Effect of different splints on displacement after closed reduction of the distal radius fractures: a comparison of short arm double splint and sugar-tong splint. J Korean Soc Surg Hand 2015;20:104-9.Article
- 35. Cho JH, Park DY, Kim JY, Han KJ. A comparison of sugar tong splint and radial gutter short arm splint after closed reduction of distal radius fracture. Arch Hand Microsurg 2009;14:194-8.
- 36. Frykman G. Fracture of the distal radius including sequelae—shoulder-hand-finger syndrome, disturbance in the distal radio-ulnar joint and impairment of nerve function: a clinical and experimental study. Acta Orthop Scand 1967;Suppl 108:3.ArticlePubMed
- 37. Bong MR, Egol KA, Leibman M, Koval KJ. A comparison of immediate postreduction splinting constructs for controlling initial displacement of fractures of the distal radius: a prospective randomized study of long-arm versus short-arm splinting. J Hand Surg Am 2006;31:766-70.ArticlePubMed
- 38. Grafstein E, Stenstrom R, Christenson J, et al. A prospective randomized controlled trial comparing circumferential casting and splinting in displaced Colles fractures. CJEM 2010;12:192-200.ArticlePubMed
- 39. Lichtman DM, Bindra RR, Boyer MI, et al. American Academy of Orthopaedic Surgeons clinical practice guideline on: The treatment of distal radius fractures. J Bone Joint Surg Am 2011;93:775-8.ArticlePubMed
- 40. Guebeli A, Thieringer F, Honigmann P, Keller M. In-house 3D-printed custom splints for non-operative treatment of distal radial fractures: a randomized controlled trial. J Hand Surg Eur Vol 2024;49:350-8.ArticlePubMedPDF
- 41. McAuliffe TB, Hilliar KM, Coates CJ, Grange WJ. Early mobilisation of Colles’ fractures. A prospective trial. J Bone Joint Surg Br 1987;69:727-9.ArticlePubMedPDF
- 42. de Bruijn MA, van Ginkel LA, Boersma EZ, et al. The past, present and future of the conservative treatment of distal radius fractures. Injury 2023;54 Suppl 5:110930.ArticlePubMed
- 43. Bucholz R, Rockwood C, Green D. Rockwood and Green’s fractures in adults. 7th ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2010.
- 44. Jung M, Sung S, Choi I. Textbook of fractures. 3rd ed. Gunja; 2008.
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteNonoperative management of distal radius fractures: when and how?
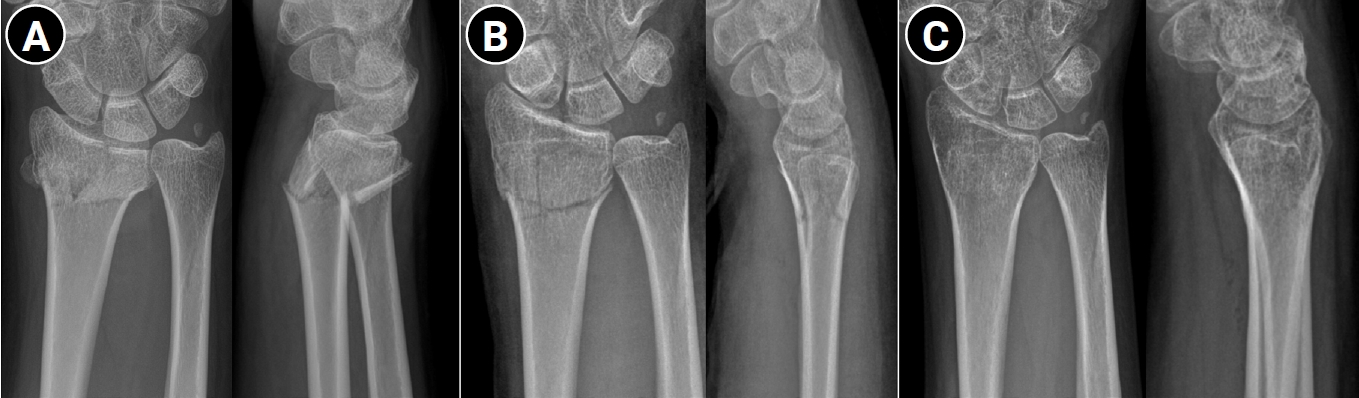
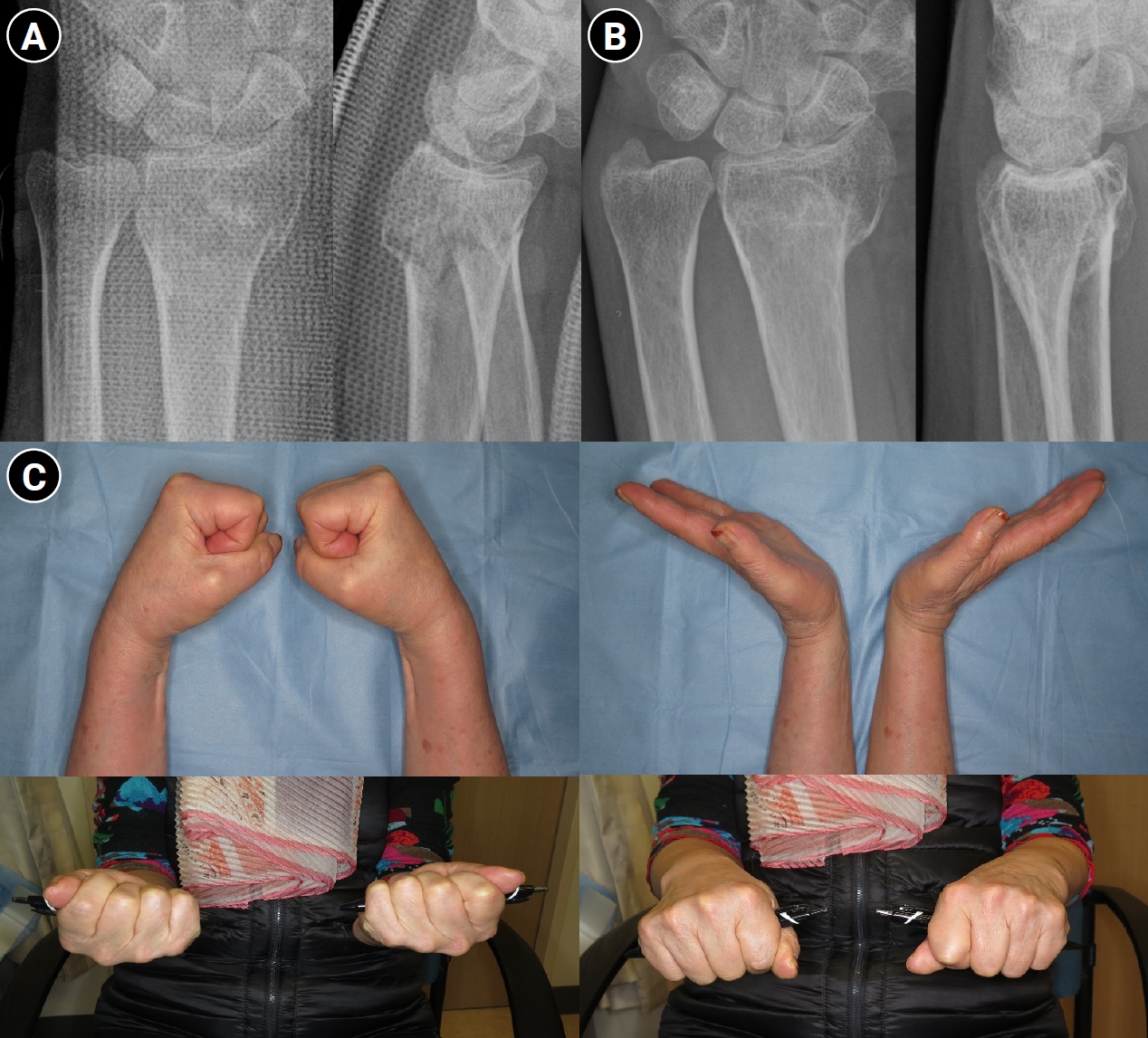
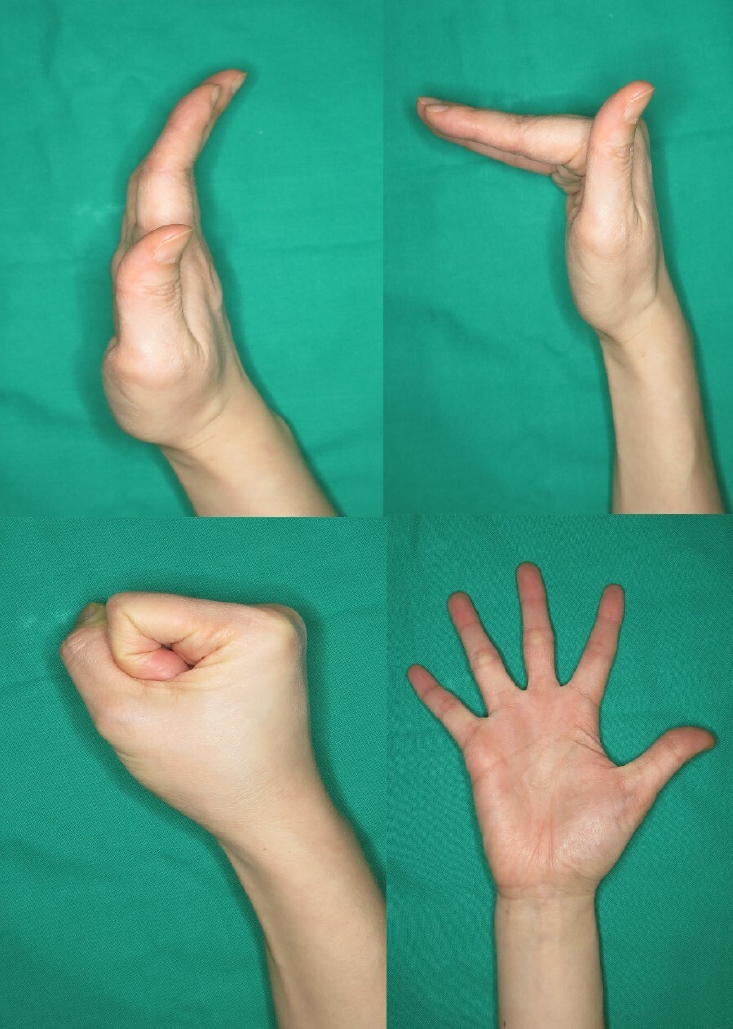
Fig. 1. Successful conservative treatment of a displaced distal radius fracture in a 20-year-old female patient. (A) Immediate posttrauma wrist anteroposterior and lateral radiographs demonstrating a dorsally displaced intraarticular distal radius fracture of the right wrist. (B) Wrist radiographs obtained after manual reduction, showing restoration of volar tilt and radial length. (C) Wrist radiographs at 3 months posttrauma, demonstrating maintenance of fracture alignment and satisfactory fracture union.
Fig. 2. Outcome of conservative treatment in an older patient with a displaced distal radius fracture. Radiographs of a 71-year-old female patient. (A) Wrist anteroposterior and lateral radiographs obtained after initial reduction, demonstrating distal radius and ulnar styloid fractures with intraarticular comminution of the left wrist. Volar tilt and radial length were well restored after reduction. (B) Wrist radiograph obtained 1 year after trauma, showing radial shortening and dorsal tilt of the distal radius. (C) Range of motion of the left wrist was slightly decreased compared with the right side; however, the patient was able to perform daily activities without pain at one year after trauma.
Fig. 3. Active finger range of motion exercise to prevent finger stiffness.
Fig. 1.
Fig. 2.
Fig. 3.
Nonoperative management of distal radius fractures: when and how?
| Study | Included patients | Type of treatment | No. | Age (yr) | Sex (male: female) | Severity of fracture (AO type) | Clinical outcomes at final F/U | Radiologic outcomes | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Wrist flexion/extension |
Grip strength |
Patient-reported outcomes | Dorsal angulation (°) |
Radial inclination (°) |
Ulnar variance (mm) |
|||||||||||||
| Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U | ||||||||||
| 2005, Azzopardi et al. [20] | Unstable, extraarticular fractures | Nonoperative | 27 | 71 | 2:25 | A3 | 88.5% | 72% | SF-36 physical: 38.2 | 29±16 | ‒5±7 | 4±8 | 18±6 | 21±3 | 19±6 | 3±3 | 0±1 | 3±2 |
| Percutaneous pinning | 27 | 72 | 4:23 | A3 | 90.5% | 77% | SF-36 physical: 42.2 | 35±15 | ‒4±7 | ‒3±10 |
16±6 | 22±3 | 22±5 | 4±3 | 0±1 | 3±2 | ||
| 2010, Wong et al. [28] | Unstable, extraarticular fractures | Nonoperative | 30 | 71 | 5:25 | Frykman classification I:II (18:12) | 143° | 9.0 kg | Mayo wrist scores: 80.5±7.5 | 31±6 | ‒7.5±1 | 3±1 | 13±3 | 23±4 | 16±2 | 4.3±1.2 | 0.5±0.2 | 3.2±1.4 |
| Percutaneous pinning | 30 | 70 | 6:24 | Frykman classification I:II (17:13) | 145° | 8.5 kg | Mayo wrist scores: 82.2±6.2 | 33±6 | ‒8±1 | ‒4±1 |
13±4 | 23±2 | 20±2 |
5.2±1.8 | 0.3±0.1 | 2.1±1.1 | ||
| 2011, Arora et al. [26] | Displaced, unstable fractures | Nonoperative | 37 | 77.4 | 10:27 | A2-3, A3-9, C1-11, C2-8, C3-6 | 103.7% |
92.6% | DASH scores: 8.0±9.3 | 3.6±11.2 | 10.4±19.1 | 20.3±3.3 | 15.9±9.0 | 0.8±1.7 | 3.2±2.9 | |||
| ORIF with volar locking plate | 36 | 75.9 | 8:28 | A2-3, A3-7, C1-4, C2-12, C3-10 | 92.8% | 102.4% |
DASH scores: 5.7±11.1 | ‒3.6±6.9 |
‒0.5±4.7 |
21.8±2.7 |
21.2±2.6 |
0.6±1.6 | 0.7±1.8 |
|||||
| 2014, Sharma et al. [27] | AO type B and C fractures | Nonoperative | 32 | 48.1 | 10:22 | B-13, C-19 | 135.0° | 72.2% | DASH scores: 14.0±10.2 | ‒8.4±0.4 | ‒5.2±0.5 | 18.1±0.9 | 15.2±0.8 | 0.2±0.1 | 0.3±0.1 | |||
| ORIF with volar locking plate | 32 | 52.4 | 9:23 | B-19, C-17 | 168.2° |
89.1% |
DASH scores: 5.0±9.4 |
‒10.1±1.5 |
‒8.4±1.0 |
20.5±1.3 |
17.9±0.8 |
‒0.3±0.3 | ‒0.3±0.2 | |||||
| 2019, Saving et al. [22] | Dorsally displaced fractures (≥20° dorsal tilt) | Nonoperative | 64 | 78 | 8:56 | A2-10, A3-28, C1-20, C2-6, C3-0 | 107° | 80.9% | PRWE scores: 22.4±21.4 DASH scores: 23.1±19.8 | 27±8 | 8±8 | 14±13 | 14±8 | 18±6 | 14±7 | 2.3±2.2 | 0.6±1.6 | 2.7±2.2 |
| Volar locking plate | 58 | 80 | 3:55 | A2-6, A3-33, C1-11, C2-7, C3-1 | 118° | 96.0% |
PRWE scores: 12.7±15.0 DASH scores: 15.6±17.0 |
31±10 | ‒1±7 |
1±9 |
14±13 | 18±8 | 19±8 |
2.4±2.1 | 0.0±0.3 |
0.5±1.3 |
||
| 2021, Hassellund et al. [24] | Displaced, unstable fractures | Nonoperative | 50 | 73.9 | 8:42 | A2-2, A3-12, C1-11, C2-18, C3-7 | 112° | 77% | QuickDASH median: 5 PRWE median: 2 | 23 | 13 | 20 | 18 | 19 | 18 | 3 | 5 | 5 |
| Volar locking plate | 50 | 73.4 | 3:47 | A2-3, A3-9, C1-13, C2-16, C3-9 | 119° | 88% |
QuickDASH median: 0 PRWE median: 0 |
21 | ‒1 |
‒1 |
19 | 24 |
25 |
3 | 2 |
2 |
||
Table 1. Summary of randomized controlled trials comparing nonoperative and operative treatment for distal radius fracture
Table 1 summarizes key comparative studies. Differences in fracture classification, definitions of instability, and outcome instruments limit direct comparisons across studies. For patient-reported outcomes, statistical significance should be interpreted alongside clinical relevance (e.g., the minimal clinically important difference, when available). Follow-up intervals vary; early functional differences may not persist at later assessments. All of the continuous values are presented as mean or mean±standard deviation. DASH, Disabilities of the Arm, Shoulder and Hand; SF-36, Short Form-36 Health Survey; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand; PRWE, Patient-Rated Wrist Evaluation. Wrist flexion/extension arc and grip strength of the involved hand are presented as raw data or ratios compared with the contralateral side. Pre denotes the values before the reduction or operation. Post means the values after the reduction or operation. F/U refers to values that were measured at the final follow-up period. The value of this group is statistically significantly better than that of the comparison group.

