 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 36(1); 2023 > Article
- Original Article Comparison of Surgical Outcomes for Lisfranc Joint Injuries: Dorsal Bridge Plating versus Transarticular Screw versus Combination
- Ba Rom Kim, Jun Young Lee, Sung Hun Yang, Seung Hyun Lee
-
Journal of Musculoskeletal Trauma 2023;36(1):17-24.
DOI: https://doi.org/10.12671/jkfs.2023.36.1.17
Published online: January 31, 2023
Department of Orthopaedic Surgery, College of Medicine, Chosun University, Gwangju, Korea �����JFIF���d�d�����Ducky�����d����qhttp://ns.adobe.com/xap/1.0/� ���Adobe�d���������������������������
�����������
����! 1AQa"q�
2#w8���B3��6v�7�X�Rr�$�9��b�C��t%u&��W��s'(xy���4T�5f���H����
�!1AQaq"���2B ��Rbr#��u67�Ѳ3sTt5v8���Sc$4Ă��C�Ô�%U���Ӆ�FV����
��?����������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������_A���נ�j-
�H���>�>�,�m*>
��
���fzp"�����T������r�Kkr����^����r.�����������������������������������������������������������������������������������������������������������|_&��]�|*��v�P��uܶv�o���Q�1������m
��w�VJU�hu-�I�"=L��n���i��Aƕ8���"�۲����
�k�*ҿ[y�u:�.��v�U���Q +�)��%F� D�Hy�V���B� ��k�>�H�y8��j�ݹ
q~�9D��4�KR��m�z���Q����)�^ʔ�.J%k_tVi5NT��jg!'�k��y|5as����O��Ȼ)R��۸ߩFMԿ3L�4�j�6d��ڜ#�NIw UF��]J��q�B���/(�F�a��fJ�Rzq3�\G՛�
?
�~\�
6�)6���W��4�m[O�
�^L0�E�&r�RM�ض*���C
.��]Un�l��-1�
1�r#Rj/����&QɈ˩��s6�Rj=5Tg�.��y�.·Pӡ:�JJ�S���
:��C8��-���2u]�d�&����v���U�z;��7p�
9���
5V��nL֢����"y)��">�iי�(�IDDd|���
Yj0��;
L���R�f����S��:k����tY�K%*�N2^�m�|&dğ
th�":���e��y�)u�P���Q��Z��W)gcC3Pv&�M���M���W���d&�Ŵ�۲��mv �T��Ro�ժM0�3�*�F
3Y��d������ 6����\8�,�\h�ݻ
kߔ���i��<
k� ��NT��wS�Ԫ���mlj���j[>->�p�������������������������������������������������������������������������������������������������������tU���%�'�
L�R>&E�B��H$�
����
�MQAU�x[�$Z6���v��i&�_�a.K�IQ{�h�yƒ�
�j"J�OC���9����e�F��ҝ����f�j���;�˚Ω<[3�_m%����
��l��Q@��4���g���=5$��(J]Y���c-OMq�<����Ǎ��
wS�����z����
ڗ)k�$
��7
�V�I���P�붾ͯnV+卵*t]i�ЎD�31��~S�A��1�
é�C�2u)��ʼn���Qn-U�o�i�3�:��g��rI8���ؓWm*G
z�ܕ)Z�קJ}��
Y� Y�lGeJ6�cB2I �NS3�Q�>k���=KT�� �B�����T]����W�
�����6����+�S�������O��X�QgG�R�?
te�l�ˊ%��-R�e\hѯ2TF�"��C/�O��JΩ��6���r�[N�.0��{����S��pljjX��1�jOs�ӥ;ҭhe}�x�u`�Ք �&�.���)y��O̒
�F�ߑ.$���Qw�;�9�����I�w2o+R��V�JMS�Oj[SoҌ�Z%�;��`d$�b���l�Q{Ro{�Imڌ>3�e�gf��\O�֝U�z��x��"䢸g+mv%G��������ʆ:|V�[N��'&ס-ޝ�'��k��fE�|K���
,G&˳98�J�u�i�n���/����\\Qݿ�̋v�~�����Ǩ!r��t���WU� ��d����|�E��߫R�� 4d�}.��q���Pw*Ӭv5YE���c�n��������~��f5�c�%M�T�M�k��b-F�>�5��JT���,�}�)�
Q��H�g�%�{("Ӕ�ȸ�W�MsY�y�W��NR��rkk��J�r���0�X�ドnͫ�T������ }�r�-j�j,�Ŕʍ\�Q�2Ri>v$5�!�]"�J��B���2����WɅ�)]V�Ԝ�U��c8��i�|��.�j�e�<�X��7��T�=�r[{w�Ol���TUv*�jp��m��8�KŎ}�Xu*A��H�:&�oZ�ljQj�m�����u�C;N���w
ko�ػ@��}_@�*�>�R�O�6�^�V.�����������������������������������������������������������������������������������������������������¸���
��Q�&��#|�ܶ-*�u��O���G%�JA�t��RZR��r]F�FG��\۩���w+?'zչS����ѧ��t
jz�>
�KW&���ot�{7�P�&�2D�;&\�\�����>�Q����2J�zܗ�A�KS����fe�Nn��[��jRr��ԕ�f6,q,F1�t�R�fԗ�>vֶև���j�-�&���R
'�Z��i2=xv���~E�l��bs�vm8������=ӛ"ūB����ȩl�Wa�u[�]ٷ��B��ߨF~�J�!|���I��p���r3�R̴#Y��p)={7�:G{+:\W�}�n�|Q�#%��)7^-�h��
"Ƒ��q���:M*%J�&�$�T軨�I333�g��_�-
��u���c B
�ww������jp�[�6����i�2��5�����$̏�b��U�ٱR�v?G���\~#Iͪ��b��7�<<}��E���zt"��
����q�_��In���w��,�7-���d����������,���G�÷%T�*�
W�g��1��"��䥱�k��q/�A��.�,_���K�h����q�Œ�
x�wvo��� �u�2ۥ�����ۧ.bQ}� Xκ���A��$֣
�+K��״�ZU���NmڸI�I{.��v�{5
�z5�����Ѯ��R�m����e[m��oyƾ��������d~����c��R��ݾ���K'j.\i�&�������/�S�6�f|b�=5��:�� �p!6�i_�
4�j6�=�.s��i˧eƾ�tS�^� ��c�.�Y�^�R�����������������������������������������������������������������������������������������������������J�V��S-Vi3,esi��08�?�H$G�v���Z�gg?���gi䤟2a����dw����릿�:��"۪���l��k�S��N�>q�-4�kI��܋�ێ�e�̊�qۅ�g��DoѨ���9����;�����
#�T��. �Q���
;��7�#�~� �_U�f����s����t���b����_���'w����������~X��w1���X���k,v �cOt��._}��v}�8��"���(�4��Z��� �\��ۘg
k�?��J?��bm�����_��c�����!�g���{��HZV]��F���kk�%~��g�������E�t�)���b秴��
�v�ΰ���B��������|꽸}�m�
�p~E�6ݹ��v���;�7�P٤���v�+��r��i��*3Ԣ��|�'O14�_����~��7����n�P���{7Z�U��\Vű�[�
����+���7o#:�ǥ����Ŭ\�|3�r���%T�
JX]V7���e�z�¨Y�]��lc|O3��V!��
R��
z�b�J'PnGq��V�J"19��WV����eOF�埜E�aEJω qCN5��Z���
��g��-�9[S��<���$����s��U�K�5b|7s�n\7x
����qmv�����������##�FF\
���w�[�=-4���3$^��o�o��VSi�Xօ�v�7iB�۴y�g�>]Vf�"r�$�J3""32!�Z�h���[K������%7�G��vNL��s��+�4��n����B���/B�{vls�obJ�a�Һ���JR�:����0�g�%&�z��R\
S3���T���[�&ִ�or����*ⷳ�����c�3ʊ�O�[ioz��W�٨%�$���gn:�ܶ���WwFB����Թj�H�P���&z���
u&��F�2�\f;ip�W73��
����
[��;���
'_�̽b��;v�i��b�!oe���c�
�d��C����-tS���<���yC7K��Ƶ��۹b�W/ܻu�z���;�q�\4��R3�Mw�����~��Ga
�աn��]�U�Sv}�q�WMj<���o̺�Z�F;�Pj���(y,��� KZ�<��Ө
��ir�%�q���±��V1n�
�
�ܯY�4ݩ��T�iF�d��'��)=�oD,��S�9j:�v���]yy��bٔq��*Ź%~�C�psrn.N1�^7`�����7I���ߘ�c-5���O,}����B�O�L*u
ȧUc�ǔ�K��n$�#�B1�= �/X��Լ
Vռ}F�ܘ|�
�nܨ����j�]��2On�T�l��ye��B��r��]��4'b���
R�E�����{6�pY�nR�%��+Ce!��J������������������i�-�����/���_��H���U�g?*STKF�H�Φ�`B���C�Pj4��'�}�8����-7�������P���y��ͻn�;���0�9� [�
����N)Iʮ�K�ϗN�r?I�e�`r�&4u
�:�ܬ��.�]붡r��ާ
����B���b�U��E���Ʊ�p��pVn�Bٴ�����ܙ5'�W��ǤN�¨�[���VEU5jSl�"��#��iY����[��r���{/L�Dž����e��Jڜ�|�R�j<�m��K:Aȼ��h�M��Llb��'�����'fWa~v�]�Nӄ���5v*�
)�������������������������������������������������������������M4��m-�
{;����L�DG�C">_��_$�X�s��]�l9���&z�$�2/N��>%'�
�����[���}b�{h�/{`�{�J�i����
�YJ��B���/X%���}.|+{(�����S����:q�z���]4���_Kѵo��`���^��t�Y�_�4�����S�#*�
^��z�vݾM�r��+�T���rkQ�
g.8Ͽ�^�<��O�2���'����\\�E���w���^4��蟡z} �-dz~Q�����mkM� ����\�7�w��
���M�w�/3�/�Ǥ��^�|�W�6��lĚ�����
=��WLt��ބ� ���~�}Ve��z��֏��{���'�Q[����'�f+?��c�����b/�������I�==���d�|E�G%�����_��l�����dk�r��r?�na�u����(��O�&g�Y~�яG������,[���!iYvz�� ɭ������0M��~�b����9���3�W������Lw���:���
��������#'��;��f7m]�ɓ?]��NT���*ի-�(Ӫ��/����%�H�D���.����
̋pS����ʎ��W�u��mv������G�8~ky�����p���r�g�����I��^ń"�
�l�Hj��.o_�+��^�p����ܘ�˟Q�F�E\�0�֙�6���*�<�nT�ˮ�v�<ֿ8�G�^˙Zn=�*֓v�ƫEZO�V���y^�+~eu���V*�p���[�J���+.�t�(:UҴ1g��HN;�vE��̳Rȕs��b%��T
�[e� ݼ�R�P��\�\�yt��i>�ӈ��Ǚ��v����i��x�>�
���$o(�
�
�^��qt�*���&���t1oJ��V����u��-��q�l�5��U6��j�CЉmĻ*�"?JT���=K'��O�/�|=Vo���}l�0b}}f�?���X��[�����?
/\�J�S��Be�,�k�P��8E���T�J=��=�?.
p�5ފ��g��b�U9}���Ƕ���dNKk�����_$8�̸͓ۍ8D��i�\B���Կ-1v{FF]�|��.^��ۅ��{v��l1��2�z7-�R������7w�E?�\n�����h\�jN/Kձr_�oBw"�N
Q��M�B�Zq�
e����-m:ӨSn6�j4���%!hQ�����;sv�'�m4�kcM=���
�!8\��m�[�M4�{SMli��ۇ�%�eֽR�&N:��{2A8�)��T�HL�K3Z�j��[�jP�Bx#Bگ�Mf:�G�1\��`edcʮ�?|w�
������(�-�����̮v���X�t�,��b�������W����2�;.ι��NHRR�#��Y�wT��M�"
��<;�mk\���.f�����oI�D�j�m�lJ;v�xy7���o7i\���,�KQ�Ŋ��9d^��M�mg�c�
L�*�.T��
�6t��L�����eIuOH��3S����JQ�3=F��/�ʿ<��9�\�����JM�6��m��N6=�<{x����kP�!�F1�Q�R[�I$�6��ُim��Xu2�A�n2yԒM�U q��
���f�[��I�������B�-'��䤯jY��m�5����2���&�J�G��\���z��д�\~�v��d��g
�Qt�HG��X�w&�1���Lw+�
nD�E�dC�����1�w|YJm��vP)HZ>i��0�BP�βә?��R�:Q�O[�"��]����I_�J�ʏ��
ۍ>�Q��K�yu���^by��cB�q4lXF�~l��
[\*�N>-��J6,�G�q��(Z�r�5h�]CwY��ӤU��~ʶߑ�
����u�*
S��Iv�%���Z�f���J7�)! F����S��*s��_��\�
|I�Ÿ�Z)J
]���ܜ�i4�"��z[�����+��Z��,MOZ�)<�F�32'&����VlUlQǷi(������\�u r�ϕ"l�
�6l���.\�.)��HyKzD�,ֵ��KQ�����W�^ɽ<����E�9JRnR���)JN���m�V��K����c���j�!���J1�RJ1�IF)$�I*c��պ\Xb�h嫞�LK��2о���Ш��xf˴��ǗN7[$�o�݇(҄��D��yC�
N�œ��9�\V2�<�I5N
�r��V�nn�9Q$`�yX�OU4�as/��f��
�V�����Uv��GV�~�&��:��jݙn���.;·���ޑ
��l�$
�-���-��!JRT�i���7�)Q�n4��X��H���uc�V��cR�%o+
��7iU�*.;s^չ�U'��$�/�O��1�u�ͽR���2����²,�IJ3�Z��-�7��K�"�.D���q�6��3��jWk6��G�eK�����-j�-3`�2��Zk�B��,ȖӉQ�k�}
c����]�je���t���v��n�$�IBpjQk����y[Ѵ�`�ʚ.������j����z��pM�ܵr2��T�
���ơߍ�����?��� ��j��T����5��������
����O�������i��c+3��R�Ց��*�v-�wZ�[WX�l�w�Z�G��U�ۥ�rά\�|��JEQ�P���r�������e^{����-i|��fe�cci����W&�r�cf
����
i�Ը�K�W%(�#���_L�7����N���jy��u�?Vm�M��M�cB�7��N2MÇ<�Fۄ�/!�uU���?
�5ժ7�j��R��dXW]^C%f�ͽ.
o]�J�m
?i$��-�9r�v��ۜw��>)}�|��Ʀ���(�RUNII�I���.<��?�fӆ=�?pE�Ry���+i�a�NP�h�%(�����b�vh�9���^���?D�N�����iӦTUy]�UP��V�Ƒ5Q�6ٺ����iN�$����nq��[�
3�u]K��(cdޱKǸ��S�r�J�7D��E���
5玔kZ�:r���j��v�w7.�-�S'�ˍO~<��B��i\����?Է�2���>�˨����r�n}�M)�xx�ӕ�0��
�
eyҵ��7YMAB�]ӣ�U:/ѭ*�6��b��cwP͵
���"���+��q�ēV�j
ŹO��|G����tY�4V�
��j�[mL�V��
M
-m���>�",���B�$�
�G�D1~��j�6O�4|��L�x�nN���mqA�T�N��R�3ε��|DŽ��a����[���f��m��n���-�ڭ+F�i�K��7�P�cm�;�r�5
l�8���r{��#����-<�U��Lgd�y�|����\[F'��
ѩ�@�{�8��nR�ɕ�xi�vo5N9�'8\��$��.�����,r7/Ϭ�*�XZ=�Ў��n��ޚ�o+|(x����b�8����ۄf��d�)�F�7G���3�����G�Q�FR�R)���)��U2�|Wb@�S�D�����Yi m��II�?Q:��l.�k�X\���ó�f�ݸgeB�2n�0�cuF1�RQ�I$�I$zK��B�#�t{��=O��W'R��2�۷t�
�nݹ�bw.\��]'�nrF��h�2ruy��cb;��pW
=�njRqR��J�(��d
�mn�pc���k���N��nʹ+6�]�t�z�~E=ʕ
l ����ZZ�5�jSi3#4��7�.����Lc��fe`���9؏��v囜.��
�F\-�UZ:*�0_���<�Νu��9�Lӵm&<��qX�Ƴ�e\�F
cq[� �N*RJ\)��_�3�\�^ҹ3"���1n1v�����_|�uR�ʞͫr��'��i��ȧN�_��k�H���8���x��Xrj�=������\�М�H)�V���\�ˬ.�X�ʸ
����� oVRC�}��ySU9/��O�BY먌�5
�ٿ�w�ޞ��)��rw8Ӫ���i5*�5Z��Η�c��G�Ʊ
!Z�ۄl�mp�j�J
-�
l� <�R̵�/����J�A�պ�Zuq\������I������dUS
�� �4�8�wXJ����Jtc�g4�cI������~�aqߓ�w��ŷrm��-�v�)G�7��y��S����^���7H�^-�\��m�Ō�Aq|�"�m9�I��B�nF㏉9[N+m�m��y��/!��KK��ۉ%��n �+B�dddfFF6�FQR�N-U5�����;Sv�'�m4�kcM=������M�n���
)�\qιqUd9F���%",���6M�Gd
T%-�
�+�~
f�%+y֛^3�S���r���F>6l���c�(��֪�v�ۊ��N��;���g�.��_0��Sѧ�]
����E���T��W
�رk����Q�Kz�Ge��9��ʨs����KA"yC��
y2\��[�5
��r�ԭ�7Gk��5M���z�w���_4�s��M3��hxЊ����'���oÍ�5jsu�b�
�)�ͪ~�tR�����2�H��]�R�͍>
�̋�m�
6�=�%(˿�(��W�rr-܅�y5(�ܔ��J��Y�unW̹�븹��N��s�qK�
����]���/Q���R#�"�ZM�D�fD|4��3�Qw�|.�_ԡ�S����q���T�Z���B��g��?���?O���
���Ϥ)����/�E�_�U|i}�2
��9Z?¹ �0�:���x��'�3�,�whǣ�?��C
�y�-��A~����=d�a�������J�ј&�M?D1�_P�
��S��+���Oi�&;����a��
�@���������;�Dž�7[������ �z�Z� C"b�v:����j�jMQk�$�M
�RԸ�3u�A\��=wI����.AwC"�^�.�{��?-\����NS�iˏ"�b��}��T�/��}� �q/�
o�.
�1����
M�}R�% :�-���Z�niʒ�L$�S�g�rBW�*��,Mw�'N\�ɇ{s��\��j�]�������V�ryG��'�8f`�}���
'N�<���*/�` U숻�z�
C��wH�q�1�8���J+�vԕK�s�s�4�R�5�3/�&�����XT�t�1b�Z��Ɵ��o\�=�%��nO�)�h��$�r����B�i-�n���K
Ī������^�
���ջڜ�lwkYm��[̑+�/Q�rZo%�TQ�;�T�����Ls(�$2�C:s������.��%��+����eo�
����Ntt�q�۰��k���K�7O0m_�t�_���p������Z��1��SsS�M7"m��e�v��FZ[��w
�-F�J*T*�j�����QRg���
B� S��u|]g�:�ɵz��jq�wm�l���tL.e�3�sRM�چ
�k�Sm���jkmWœިm��++¦�'�t�IL�k*բQ
��D,�P�B��\l�I[�9{<�Y'�L��z�̶p�!�����·j�
��Jݺ�5T�ܔ�oKsG� (<�����C�B4��jyW��?zm�ӍSN����m
[�Ԓ4��=�m� |�۾��%�cZpj|ͩ�Ui�Di��<{l���/���T�=
��Q�^�hO�yH�$�sN� �R�V��:vVnN���+�q���ΰ�77F�v��;[kK*�aUlt�*���[��#���q[�˶��c^���bږ%�Gb� R�6öۍmX��-�Ma���ʉ�A�93��1cs..G<��y
� Iߵ�{'Ÿ�e��g�.|�4���C��u���jQ�տ[9
�}G��-���xwl)I�Q�z
j
��Ó�"�rq�e&��=��]꾧֎���������c)�<��kӳ+��� 0���Jr�R�R3'���T�n��X�i�^x��MF
����Bު�*t��I���L.[h"2"nK�z�Ze�'Z�V/Rr��N�Yz]�8죝���n]���Ķܩ
>��^�Ժ��]�u-7^���\m�Z�j�ܣ9+Rmn
���ߑv��?o����ꋘ?&��ƪ��y^N����4�o=3�
��-�ؔ̿��*��`��}V�݁
���ƒ���P��u���8���%�$���
ݗ]�w�t;\��y���\����>=�'O�jP�Ip/nJ��U8���{϶F����N�M��sf"�ί�Nq�ƹ(�+
ݮ��F2��K��m�
�|jܴ������Z�s%�zf*��eȫ?�]��4)I�۵�nR&F�X
��+
[jD�h��(�#�
�哑9�q9�E�ծj8n�o�Ǖ��Z�f\J�-�l���&��Z������˫}`���ӎh�yrΉ���n\ű�n�]��9p������ʌ����ӣ" ������W���t?N4��_�I��_~�5��4���#/my���1� �Xr�����*척aS#D�T��
�>����q
s��<����F#wM�F�>sΛ�W�;3o���U�aJ��S�����R�M��D��gQnt��:�Ql�,��/ ܷfR���q�iM��
�Ȼ�>����Co�b;A���>ڦ��Wق�M9X���~���/!'�M�W.�}Vrߔꔵ!�5
|���iB����(�0-����z�
F=���}�����okڢ�E$�^w���W�~n�okY�߮�\�6՜
̌
{i�-AF*�9)\t��9�I��V���
������6����۸�5�Z�UF��6�R$ŨQ�Iq砳Y�UZ]e�yv��� �>hI櫥<����w0���N
�)���&��l Ju�
l��wE1��G����D�Ou� F�N2�|
�}馥��uC�1��rޫ�V�+^�g����d�b��&W[4<^e��4�Y�W,d��|h�t�ͮ�sUM)۸�8:{3�d��{A���Ѣ��)��~
��� \#J=N�d�����Ʈ�������ꮓ��90
��|�����1���K $�����v�*?��S�
�]i��$J ���,�C,���SG�?�/�����_՜��pMSƯM��|mG���1V1�$������~�K���>C�S�
v��k����u��j=&�)
-,yLj��uFHK{c駗���.�SO��u��a;��B�r�Sq�j�-ۍZ�#��
�'Jy����s��7��[g��2z
/.u��4�+XV��2V��Q�.ޕ��)$�"�(�%�)#Z������7suZ�%j���
}�B�������Ǭݕe)J��vz�8z�Jf:�hIN�|�svO1�O#I���E�cۍj��ݽ:Sd��Ὦ��v��u^@:o���^�5���c�s>��i/�Vqm�V��m]�ؔ�ܢ���n�6�'v�ޑ��̗J��4�Wn@��O�lKb��X�
��;��n�:h��g��J�9�Ży
Ǒz8�f���܌��q&��Y�
�f��N0��N;[�69�
r�bׅ�
C2��/#�k�E
��l�&2�~�è��MR����.�*%��g�=�Ft�<��N�a��w��R�w��w\���ϊ�k]��5o4^b5�fZ�O9���]�
>.%�؝�e�8<. e�
��=Uv{���~㻏"E�ˑn���vD�ѭ�͜�����Lu��3u0��:�U֝$��[M5<����:o�i��+�V4�V9
���6nXvx��&��_� ��q�
Qq�w�3�W:uϔ����2y���b/�(�ɳ��|5zQ��i��J�#r�|H�w#�.�W�?�4a����D����Ų\ug�W����G�;��Cw��������������������������������������鐢K|x���g)��##�=O���.�d��F��˟�j�MUvW��Ļ�s�r�������.z]�kPc9"]R�)���mkf�Od��*uYf١���R s�B
�A��îh���=k]ʳ���Ur���r�Z�sq����`�d�#�r�$�/<������Yy���F0�nweM�W'��N6�T�q�F��H��y}Qr�y��m
AS�1n �S�`�T�����j�rT >�Ը�3o��^&�l�R�WȍyuW̦��Y�4�Q�DUM�J���6�5��ƒ[�������+��y�g���k
X�K���_±��k#y��:��8(�T��JOSQ�h�Jt2.D��R}�"5 �[�)�
r�)6�V�6�u����5�k:e�XZm�v𭤔!�푊Q[q��Q���}ҹL����E���-
�8�q��IZ�G�|U�M�4�j}Mܕ��[V�wm�{}
N�aqµ"Ԉ�M
��zO�p��KѰ?IA����D�����3I��r�0�'/q1�i�to�B�5{���%�w��kO
��B��n��-ۜd�uqIz�YK6�
��0{+D�ʕ��ܞ�qI����t"��;r����1��m����G����/��\�/�y�m��[�6��J�
ƫ��R�
\L������=S���=OT����@��I�x[T���M�m{>ݾտ֒ݸ�Ӊ�L����Y��Ix�>+"J��V��N�zx����||5r�I?C{�oz�8�۹e\����R-���^\A�2F
��R�+N�9� v�lT]�"ۭ ��d)t֞i ����#�E�2�jB�@=#���/���N�+�!ĕh� x�}I�!�cM��`ą�Z��*ŻɄҒ�߮Y�.�Z}�=�'/oۙ�3��Ip�W�̮�hT�7�c���T�S��uz9�>B}΄�&�h�!��>lӵ�n�~
�j�˅IvU.'�v'�CS�Z�w8��Q���K3G�>�
�,J5��9ٷ���+����HSg��䧎���hJd���zvwv
����-��c�v���x������S�5�[̊n�~ؿ�%��ַ�X?O���0�\�6���n��e�
6��kn��9.ϯ���}����
�*���h��
����8�_���Q��h��L���ݣ
����7q
+=�X����BҲ���5�?�[[�)+�F`�=4���
}B,s��Ng��==����u���*������������Nj��9k_�GJ)�+R�~GS��P�B��ȒZ���:(�����K]h���e��L=vK PӢ��wq�(N��r�G^�ث�ϣ?�#�tC?�.ͼ�[��
���ۅ�o�����؞��y�#%�Ǜ�jVy������LS�w�%T*s92
JTM%�"Y��kQ��О.q� )��gC�Ͳn8cgi�6����j1�M�����Ѿ��[{���9<���Y8�]CK��/�*q�����v�R̃�T��Od��w�����܁9O*e�y��t�0e��
jm]hs�n ��K�BQ��ЏA�y�Y�1s
~�s��76���kz�nJt{ZإJ&ҥ�`rW-��o&�<������7<;��f�UI��V�&����� ����F�T�raJ��h�^�v�Ƙ��ǚ�םidfi.^R�H�m�����g��&�rׇz:}�݃�}x�T����$��ض
k�����'5s-���狶,\��vp��bP�D�،��=�Okf�������.c#c�dz2�F����K�5T���!&�)|��n�t���D�<���+���OŹ�U������
��i��-�G�[�E��E*��FDfe��a��f�
���2�Q�Ƥ���M\�UG_��{
ǹ�m%�\y�r Gy�����:.\�4��wjP�GUJޕ�U�V�7Do\7Vy_13w;��[?�c]�H�\��$IJ,*L��]3b%�L{�y.�J�R�KG2s�q,��B��6��T���}(�#��nW��
|km+��q5]��
�r㪍b���J@y{����by�z ,�b踊3�ϻJ�,'^����xd�،���)JV��w#�.V�ټ<�S}�j�bZ�}�t+�LvAF��"�q\����r㲝
\w!�}jR�����3���ν��d�ҰT��o
�%.�*wo�����7
2m��c
�r���ӓ�
kO��
[�*w��Q⧶���JŘBM�*�o\�TW�'�)b���n�d����}C��zC�����1���)Ŧ<(U��ᰕ(�
4�m:%)$�b��Y����>c��''Ý�պ���Wtb�RؒJ�z��۠8�!�o�9IۄS���95E�9ؔ�-�e9JR{d�m�nッ<�[~�n���$�
<����nZ܈��K~�Y�6{��a$�ҧ
(A$��Qյ�c_�z������8��������s�)I��*�v#�yc��CK���z~���R�q�,ZƱM�NQ�f����&�Y=���>� ���{~�Њ$W���?&���Ր����Y_��? #a.�ߑv��?o����ꋘ?&��ơ|�y^N����4�o=3�t������=��~�7!���/�M���3>n����8�W��홎2�
M`���Qx��+
��z
qy��8�%�]7��_~�5��4���0ۦ�彷��]W��q
C���ѡw�kď���y�������F��5Du���m��_}~�P(��5���.��(�X�,�K9��vᯐ�?�le�B������9;��J����hm����#3�{��CxG��E-��S{��;���@�F�z���� ˙���]=O�'�!ɿ�]'�
r`:��7'��2b����Ж>I��y��,/�e��T�y/�V��<.���H�?�U��Y��Y�{����\�^#�ѣ��r��9������^��7��?x�o�R��Ȇ7��E�o��S�_������������&�?�?��z����������ϾM?��(~Q���-���K&�>"��~a�ߨ
�t7�E����m�s�ϛ��+�?���;f�����Cr���)f�Y�+>��z��$����tIk���j���n_�>�v�nrֳk��i��-˹l=
t;
�'EyC¥�|���/B������LwBJdgjۛ��$s S�1��|ɍV��%JI 6�Kv�əhz���IlBY
ɒ��|�0"�Sy��0F���<����H�b�����ծI}���ы������b|�y5������[��� ��G�
�������c��m��������������
�u¿��q�q�u� ��'�|?�-�:��ꯙ�����w���)`����������������������������������\�g�����K���I{�$�b�ܛ���O-$J�#J�DZ�� z��. �.��T�
[{�ܽ=��W�(ǂ7
�E�lM�k�{-fe̶&
ǗJ��t�m�z�qH�T�*LZ
�:�r���LG#-V�e!
Rz�5�~�ɺ�b��F�"����&�
q��rTj1RM�ټ�
>�>e�o5��W)�O+X˻u�';v�)�2�vV�q۳k�����ۮ������ws?U�ʑBǴYO����漪e
2MIj�PA�ک\�b��1)DD�ؚKm6Z���W�Ψg�ȕ۶yj�ڳ� �2ضN����� ��[C
[|�r�@9J�f�o<_� �e��I7��q.|���c�Ê�V߷:�i��.:$�ȋ�)1�%%�)A�DZ�CEBx�J0MJ���ۥ��y(b���N��s�K���M9��k��43�Iw����N����t.�\���%N簤�I'.��j|ƃ2�$�g���rB�E��ٌ�\}�9:v�*���!n�7��M(��ɽ�]���7c���@�XxƱԨ 37��īf�6�2cT��T��f�FK]9�� wn�����
tQ��
�Hͮ�v�ٱI/f|j��
��=�����7}�\�_V��5U^+:u�l��j�S�ȃ���� Y(X��I��.�ȱ��mo�1�甅j���ڎ�I�Z��2>�#�\����*�:g�Y|4k�\8�Zw�Sq�t�y��A�!�+];бޞ�K���ծ�Ë�¥�����e���)�#�5<�p8I/ڕ�Cc�Z�(�T[B�ʎ
fc$��T�i�
N�r_oap���.�QK�^��8��VdU{*�ѽ�L\�=qm�j�n�
B5>{����� ����Ӟ`��v±5
�����^�k�&O~O�s��hɷ��,�;6n�������O�W>u6�{�R�q�S`�)S%�jp����\ip�dE�BL�fTW���y$G�IYw����~�䲭J���.1�v�SY�5��z.V>^+Ǎvc.�I[���R�{Q�s��NR3ӎ���f�h��d>y?
UJ*}��~�[�e\�i5U^͛�����E�]�G��_F���
S�(�Iɿ]i��8���:4���zj���~շsW,ˆ�s��y�:�%��O}iu�r�]iF�5~3��M:Ӟ#N0�6�)�4 ߧgda�w�I����o�ti��z:�1r����5�YDZL���HBS�i�;NQ�c4��4���la�=��Y� ��kQI�T��*ըl<�S*p[�EZ���R��ϒP�~�W
-T�ԅ�Z�wT4mG�q�
�5�C%ߒNs��i)\s�M��ݷ�� �/,��Ҟ�˜4��r
�~
%K��oۛV�طe]��JTj�6�B�R22R�HQv(��g�n�D���i�5v��+��b�
N������w����ܔT�IxU�b��[h��5��a�pׁ�a���)�dGʒ#�
�gb�c
J�j�����%c��
^+T�J|K�P���U�m��Q��^��)M��2뵓i
<��|�䜃26H�#�\�.��Fw!�����l�+���
�r�3r�d��-�kDtM'��
^h��2�X�l8*q/i��)n��U��˿ӡ�����RQTG��
]�V�ޯ���ҒRt��RE�əcK[M?�������6:g��G�Hxj�����|?�9�_�X�Į&z�N�/�sk��h;�RU�)�uy&�WE
|%\�G�Z����B��UN9�]8~��m�qo�p�~��y~p�\St�j��O�R������^�u��
��^ �Op��zJ�J����Bo[�vu���\x�~U��%���l����~�\\�/ 1'�:ݥNg���Ӧ�j��_/�����b�+���)}���mI�C�j�{]d�*l���� 澩kܓzj5m
O�����b�x�
���.:�H֚�pVm���� ��@��6)�2
�H�A�4�ԕJ�I�>�:tq�2�(�է�9�VO�4뒳��܂�~2��r�q'��nr�V�ZŦ�[��t�7\��oլ���f����b�/�ml��p�
c.I8������콚q^1i��E�~���䰳m�i��[���d�ۧ��w֤�ICfdFe���C��sg:i|���
��6擣�*�
�96��l�u
�s���t�^�{��%��99�UN��RvaM�ܽ�����o��
�a���m���m�i$��e�m4�D�6�DD\�n����A%�$�$�#�}۷/ݕ��r�99JMն�[o����T�����E�"�KT��aP+�HG���kŴj�5��T�M5���x��Ʊ�����OS-k�����`ۛk���ٝWz�;{k�S}�F�;~q�|�~�^��_����|�e�u�wn�E'�pSu��pU�P)V��]v�E��+t�
=Z�R���aVd��G6=� *.ϼ����nj9���:Uɷ�b�ې����mF�_t���ޫ���gH��j���V�
S'
ś���Ǖ�ً��d�k��k��ѻ
�_��]��K��v?�nT>�)��^���e=�A���r�1�
�'�3ԔI�LyD�?�:�-^��i�n):{7.����\���.�:V
}#�����������뺾.3����r̸��*x�b���F�M��
��aȵ��z
�6S�Q��:ײ��j[�
8�n�n
��iFM��w
rR��"5�M���5I旘35��f�^����j�=���'j�:nNW.ʭo�cZ�
����v���Z�K�V��^��ɚJ���.c�M�1�ZI7E'6�rg����탸��5o��Z�=�[�m�
Z`\�h��b�M�UR١����Ȗ�
ĉ)��:Jin!_7��Dй��+����f̷e�KҷvͨB��PR��(V���`��y���6tw����*����MRΝ
���cB����.ڭTn�c;P�
���$8nF��v��m�4�(���D�(�R�#R-�L
-2:��FP�
lx�ZKQc6�I("Km�%�$E��,
7
8�u�X��IF�A$�RQ�I$�J�bInG�]c[ֹ�:Z������M�+�n^�')Jm���JM�JRu{e)7��jQ��Dw��~%��yQ�l}
BZujS�Sf��۩Q�Z+�Dzhd5o����%BI��c'GZ?�}:>Ɵi����vז-%����J5MqG�W��T�Vʦ�����h����������݇�ܟ���~��Օ�_�6�
�n'�{3���~����mϬj�'�������
�J1���1��O�Ȼn߃���r
�Qr����\�3������y�٘�+��� ������W���Ӎ'�W���x�E��s^��O�
3
�o~[�|���7�>]]���H��9�݇����Z�o
�m��T@�]?��������5�B�:��Z ��߂����������'`�����V�_�+/��MS��K���X߆��ޠ��k��3?�o�7�y:4R�/�7��þ]���
�iG�߬�a���������BR
��U��&�?�r�&/��} c����������Q�ߥG�����j��2�?�C�5Y�ś�e�7��h�U����=�?�+����� �x�龳���f��-�܈cz�W�^7���p�%<��Q�/��,�O�9�n�!��@ǯ_���
��
�����r���+|��i���n����.۷�� ���܇CT\��6��<�������^��j��[&V>����-��(\�D4��h��{�U�K&ӡ�n�^m��]F��ݢ��:��`δ��v�j��俜F��+�)�
�y[�{
����{
7
tu��>gv��rěOj��������'��5 ��iRg[��Ͷ�F���j�Ge
�n�~�qT$����c��i�
��ۚ0��oԹc*j�L[s�V���Wq�j�\ݻ�&��6��"W�o��K�:c���nWmr��v
)�o >6��6�(F�>=�W�^�bf�#c�
zz�ʞ��t�پ�y��%��m�ՉPël��
���e���}����J.\��Z�k���4t�tt�>�o�EM���=�q��)h�J���j�I=ͥ(���%]脼���_��8�8ф;���� �͛�g�W����G�;��Cw������������������������������������~��˘�$�4=u���W�����d�Ĝ�Tث�����N�D��kiQ���L9U*��O"4XP`0�2���,Ge�-k5$���h>
ܼ]3�v�r6�!9�RQPIVSnM(��ۓ{�>�;/Qͱ��v�{3&�-[���r�c�)�ܚI$�n�{���Sv�3�[�j00��)��-D�3������z�}�MRzV�Qпj,
T�[u����V�s�0\�����}���Sid;r��(ݝ�����J>æʺ���L�&�c[�j�P�K0�~�d��(FKÝ�W�\�m]����G���Tc���F|�Iׁ��)�I3�~���#�oX�%vҦEݑؼ5Żv���2��qAZT�E�^..�M��{ʐf���ȏ��2#�#.��R�}�*K�ʛZ�z^ӞN*���l����P�����ťL��f\��G6[�W�V�Q��q�uV�]��X�Ai��)5�J�!�,��$��i�����J�6���o$t����P��Z���c;K�
���jx�_�n3�`�qI�e�l�V��~v�L�y{���f���n匋�Ѿ�n�%��;�zV.�n����'���-ұ��dd�2߽1�b�Z�k����s����Pe
�3TI�9�)�$�
ԩ���IN�9V���ơ�\�=2���885N
�\
�p��)�/a柛�w�9g_���l���ױo8ݷ� ��i�ix�JV�&� ғ�R�i�{�N�� ^�_o��AŮE��6�Y�
���7��������I$���N��k���$�|Q)��-�*4�����Z) ���^�¸� �%����4�Qm�
[�I%�.c-OV���+C֧R#%�Ѩ��C�e���3i��;w$G���+_���dy��| Fzj�$�����D�I(��=OA
gj%�v/]�8qԯN��I��S�*֩',Q%�\44��Z��Z%D|Ǧ�ʴ�����6�����&�vֵ�I$�%8�(�Ԭ��ƾS����&�<����S�_�Z�3��>��#�Z��.
��}6z�?b/|J��l�{�ץv&�����m�p����x��4��Z$ڝ4-H%�dGK�fM:sKSRW��eJA�����n]�>�s����6应���-����W�9'H�]'�uȫ�YvgK�^�\cz
p���|M��� y���\鏩w�/ËQ�.�)��]�\Q�iS`8�u�L��뚛̸�=J"�ܻ�i\å�'��-�)�54�Ue��]�:���K�\퓡�v�K���� xw���Bqr���H�\*�֕Tn�z��C.mT�=t-H�]SČ~��Nu╏N���Å�����3�f|��͡�G��~�B��+�X��m[Q�7��U{�9"~��
�jg����K��
Zo�ʰ�7��������"�qJ,ek�S�eN�G��
�g���ϳ]
^�.�6:s}_�,%eR
�g��<���5��z{��ZP�un�
#jRІ����.6�g�
�T�.!]�x��a
�����c�#�j�N$�Zp�l̋H�
������W�Z�����u��8�������W�m� M���R�ýsĮ�?�M�co~�s��x� ��T�U���҆�Q��
�:��K�DG���4���n4��2.<3/'�^?6��/ܠ�ڒ^�����y���r�rÿr2������\D���}}��B���]�^��� E~�^T���
��c�ɛ7϶�Y[���<�֞�[7d��}2%��QP��qOLEQ�R\�C�Isj1?\��}%�t�J�0e~
*�s�k"*)&ۓ��E���i#���{�1����J8��H��rt�|'�ܝR�
�r��8)=Ɣ�N'�RVz:cf�]�F���7�b��ZyZ��UȘ4�x��8�,��#�J��G̒��?.�W���9X��n�O�]�KO��]�%]�ƻ� O�5Γ�/3�q�Ó�j�؍/���r̺�r�Ƶ 5�\��&m�6�h�.����xoeX�����[�=<������3%< l�Z�"2��h\��Z�����[��&��jW�3ejm?�k&[]�ųj+{N{66l����e�u _�+�lj�]��q*�
�
�7g*����knأY��v��=
q� �ە �d��xЬZ|���%�GUr�Q��3jL�ŒqE�T��]�1� %�
q�kX�Yū�Y�����c�� ���[�7Ś]�Q��Y\��
�jk���o�\��<���/Lc�7�+��'hMSU���c6�qX��y��ؙ~
��6��#ѯ�v��.�0��$B�Qi��5�Yy�Ihɍiy��������=�KD�!n3��V�m[V�%��W-B���%sw���
�a������97aj�ۗ�
m�+�9�~����]�f�K�q�|Dda�ˑ0
A���]_v���m�M5*
F�-
B�Y�HJ���5}�q>ʉ.6hy��Dm��p�D�'-_v5;5[��8K�[��v���iJ.3�d���R:o��Y�
�H�H�h9I7����:۽f�i+wm���^�� �[��)���o�dP�ѱ5�2C
���ZU��Ji�c�Sw\�&_s���0uBȍ
�h3�������2�dž��zQ��f��l�c�d^��m|7G���ѹ��E�!�fO�5]]���H��9�݇����Z�o
�m��T@�]?��������5�B�:��Z ��߂����������'`�����V�_�+/��MS��K���X߆��ޠ��k��3?�o�7�y:4R�/�7��þ]���
�iG�߬�a���������BR
��U��&�?�r�&/��} c����������Q�ߥG�����j��2�?�C�5Y�ś�e�7��h�U����=�?�+����� �x�龳���f��-�܈cz�W�^7���p�%<��Q�/��,�O�9�n�!��@ǯ_���
��
�����r���+|��i���n����.۷�� ���܇CT\��6��<�������^��GY
��.�}+tv-ꌻF��{+Ӡ����
C}�跒#��k�o����,�f�52�Y���
����+Wĵԭ۹υ����&ݻ�*��%u�e��&�jMLߣ��
��f_�_5ߍ�}C%�iW&�|�qQ����Idp�x�n���[�n^�k�o��R�H�����
�@�ë�k4�D�S*p D�sa�iIq��m*J���j9�N}�OL�;�=����:J��d��O�;
�j�F���y&��k+H˳;W�݊����E�p�^�E��%J��{w�{r=
e;ܕ�
ݵ�:���C�,&�!��D��<���5,��=[4{M�y��.p�Z�2/�
>5�|Y:S�J�E�\U��-(���a�_�c�ƣ��Uǽ�XX����K�
��
iȞNl����mۊڭڄR�!
*�*���ܤ��M�eȽ$�|���X5��(Ź\�rJ��~�ܮ]�>��'H�B
0�c
p��
X���Fr���_�c�?��f���?��7��<�����������������������������������u<�JM9�RO7a���K��LY5Zlmq*�}=
��p���҃�^��bwa"Dzi;m�*��ȴ�|�p%���?L(����%�[r�˄�kI����H#(�泩�
&�%�W-�C.��M�8�r��d�I%U88J*I��w����
m�՞f�s�&�a�±�t]���#;2�/��U��5(^�ej��$dfkQj�pR�M
�3�Wg���u1�ےO&�����R{k���o��w�-I���mF>�k�Sgov¥i��G��>�>䙗i ��.�+t���+����b�OjI�ܶ ��. ��i^:nm}�s}�(3>�N�Z$��2�Qg��(�[�"��.��>�i�.�ƾ���������)B�̋M8+��"-
���>��eE��6��D�����ݥ�J�nJ��ˣt����
����5��.���˅nJ�GwZD��~�!��i۶�a�,Db�
3�ZQ�3�O#��KO5��/֍o�z��uK����'GbR��i�N��V�_�ҝ��c��v�ם
Z��o�X���}F6�z 7�e��5��_e�:ۓ�j��=���A����B��+��iܔ��ER��a�d��M��B�q*ԯ
DwI/Gy*mĥiRKg�6��s
�kY�/�#�SN��4���e$��-�
�y��X�M�
�Y��L�?^ĸ�N��NӪ{$�r1���JJ��R�SL���O� �]�Aq����m>V/s[��~�i�/j+m>z}eI"Q���vp�]{�Z��Լ:{��vPA�G�2�=T������͡�@����ڐ��#�u"����E*�>�C;o$����~��C#�_d���/�HB�q^��Y��RٽzIKbO�m�\~�ż�����jFFG�diQ(�*/i*#.FF]©�����m=B�m��p�QQ���Q�S�P&Ҫ�!T�&^�>�:
y���)$ˑ�Ð�F�čI
B�ӡ�-t!��b�M�
���W�ҦŶ�'UZ=��}zvn~��oT�/\��ǒ�'nr�8��� A�JIӆ�z�<���^�uߖ4�eFC���1�i+v�!���3q ���N��yߕni�?�4�JZl�m�YF��X�F�ۼ�O��0��B�\���m[�
t�����ʄU��3���s"Sr����(NJ;SK�W72L�4�̏�BV�df^Ҹj\�]��ȱ۪���(ӷm
�?J��-��K�E�mW�ڽ^���4���<8q��u��%9pŹ��W~��877���ܾ��eVг��S(���յe^C�]���yX! �םm4�
���FG��ȋ�\��y'Z����
FX7e�)|��Gj�t�߹�#��������gb��\ŧq_�([R�8[�q��U��$�Z� ��(ʻ
e�zV������2V�!iQ,�i$�
JE�˂��٩�
�a(G�K��'O�{�v��nBvr��yR�d�-RK���4�=��q��xZJM�l���_�C���uuI��z
@�Rt㮽�!|6��8���\-l[џ8���4����-2�P��u"��
�RJ�_^�O��L>G�1�~�X�n�BŬw6�J0�*�Uvlږ�1�N
�G��1�q9���IU�m*�'�o�Wu][��&�Uy�
���YZ�b
BZ���R��ZN�fE�J��f�"+�2��
nF~E�û7n1��xv��.RU��M�$����6
l�Ax��S�Q��J�&�n5ܞ�w
l���Eó�i��"�#>�4Q�.���nEq�7Oko���[1���wg8�ZQ�w�����ZYi�q�tm��&~"�>Bo�?w�͡n�i��2峋<��X�����N��C�E��y
Ҕ���+%��ZJ�
���ʩq*fpˤl,�~��^��Mχ��k1����+�:ݕ
z�&�Y��`K�L�ӪУ�D�r�3�[*Z
:(�S�L����<�����r�8�jQ�Ȼw#r���5(-�j�����K�
e��?`����=o�Q�Dg;#z��!v�Z���q��r
MFI�$kR&Կ�p�����4�:���Ӧ ����|O��5?�<���Q� �]G��U$_n;z�v��i��
J�*�2�Y��J�M�_�:�9ɲ^�J�R(T�
��
5��k��PJ�Q� �Ț7M�f�*�3�s��O���+��ɹ�'n��^�
يN��Î���z��W��������Y�����,[��(E[�۷�.'Yˊ�9ɮ�*��b��^�5��mz��~۔��ԯFTJ�
���%�fJB��
��
8�q��4:˩J�RV�Q~n���z��wHֱ�ei���;w"� /J}�zkjti��?{�9���/]��nT�����I�ڿfn�����g ' Ÿ�.-�C���/O�9f��,I���E�Q!�<(ܒ �T�.�hWo�SF�˝5ĒJ5�ۉ<��ӓ����+�yzb����B9v�:�������;����%ñ�F�O���a��yM�.�ۊ�b���ӕcIݥ��
ӍJ6�Y��ZQ�j}���&�*lTr�Q��1e��hTj<|kB�ڌ�!��-f鸝Cn�Z�Ԡ-|� ���r��^M�2#��:�^��6�8AbZ�h�����:>&ݻ�۬V�q�s��yԭs
x|��i���I߽zZ��r���g��.:mp%���6Ԝ���v�gm�p��IU���t�;�Qb���S.Է)
ǨK�S���V,���*lڌ���|5Jt��3#NP��.�=����+OZ~/��G سI��gbꥹJn
��l_D�UM�\iM!֔�wV�ZuԺ�,yV�.Q�
>f��
v:��݇�W���iaŸN5�Ҕ[��M7S�s����rv���ǣr��MW�=�
\�8��ZW-�js�nڕ.Z���nF2qt� ً[ٻޘ��Y�۷��
Zm�"J�x����r�&�N�AfA-���t����o�9s3�59݆m�Z�+N1��-�q�S�$�D��=��1�7��
x�+%_�
��ve4�ir6�Z��$�F� ����Dڗ��n����F���t������O���r'7��'�{���9C�˨��ꤡa�Yoa
ce�{Ref�n��f�t��
�R�R"4��%ʌ�m:����Sj3)�OdInT�
O��>X�'vxV#jܮ���w9�Fo����g�����;�5.~���Y�5\�~�1�8Y��Q��ܹvj4��+�~���t�7S��
����ﬕs�
%^۵ڴ�DZ�V�6��9��R����^��Y+�rj�$ԇ�o�JK�R5
�wB9C���>��Y:���l+�EǎS���{�ʲ{T��6Wi*�
���^^9k/�y/C���s�\�g*��qڵg��n4T8mE��R�r|Ti+i��P��e;;.��i�\�EBEJ�
丬i�9ɧM�-ԼsG��D��rZ>r#��R>��~X9�y��4��b棇9J�wV۔%m�(b[�T�j���vl}۩�~���nDԺ{�Zo-Y�uK1�vx������.�nWu���O���+��jN�� ��[�ٮ0�%"����C�dT��JK�-RަH�"�$I(�*��v�e�� �&�҉Fz��B,_����Vpqp9��m�8werv�')�E�;�o&��QE��^d9�˦��j\����_�,ڵugZȻ�̧8�k +����j�K{��w���m���r@�3�ӭ��2� �wF���kzFV����qs1�؛�.���v�'�I%$��[��iT��]D�5�D����l���2
n���k7��q�Uxԫ� �L�S��+sا3/Ζ�e�ZYK�<�["%-g��/k�R�s�:�f�����3;*�E�
ت
w�J���%)5�&�+&�������rw*霣�i|�sMҴ�|;R���+���fm�䡩�.���!*��*�d�Ӷ-�6s6����,�]z��A�XM�W�jm�n�z��%SJߴm�2�UXw�7M�Q%<���!t�����K��ys#P�,��W>s;3IYw
x<+i_\\\U��6�
u��7P|���x�b��n_���k&ӓ�V��O�e䦒�
VUr������,-�㘘�"���-
�L�Z�eO�S��Ҡթ��rEv�q�8Kf��%
�5%&K"#%v
���D�/.Z���Y�Y�ŏ+p��$�nZ�
��k��v�އu����W9㓱��Z�
�G
�w�Y�����IF��y�f)?ƎU�m5 �ԉ�/���'�k����8����4���{����K��O:����r���Q���I}��X�R����u�Ԫ|*lu��)��3qZ[�m��S�m�5R�3�".Xcَ5�c®ࢫ��I*�۳��~��wRϿ��QW�ޝ�(�EJrri&ۥ^ʶ齲��Im�|[yb;�mn�m��֩ui�ܘ�q�>
E+�I��kx߄�3r3��3-5��09ϖ�9[T��z~m�r���5N�s��Wl$�o�Pu��sޛ�
^��{Z��;�����);s���ڹf�\3oٹZm���ԉ�/���'�k����8���4���{����N �O:����r���Q���IBø���8�������Bݱ����3n�֤Di�K�4�u&
�
o���fS��Ȓܩ�x<�˘|��N��0�Fչ]q���sp�"�}!� �Q��W�w@�
�t���4ӭ+�cO5%�]'*�{���eM�߲D��RO�1���y*�q�8��w++e!c
�߶��ܪ��l�Z�Wّ���M欼
��CQ��̼빶�l��X��{v�i��b/V�/
ai;x����6��~]�+z]M�W��B>�r�e-��:��lgk}պ��!�#���9?�%�܋�V-c[���z�!W?��c��7YN��m/jRr�[��HO���z�Ի
���e�f�ճ0q1�5Z�p#�r�kQQ��0�tU-�A��m����ڵ�P��/���cȕ?0c�ZY��j;��:�0�Z���M���=D6g��
��?'U�N���+�ձ[K�� ܖ��B2��'���x�q9{�|۫�N0�k�u
7��x�aj;n\� �2[V�z���������������������������������������nM�lW����i�Kb�S�k�))f
.����.)Km)&bGZ��=��>
OR���܍W:j��'rM���'���w�Y�z&����� /鶧{S�ʵb�"��v�ջq[
�I-�����Ռ���
Z���H�.���_x�*�Bag�C'T��(�Q�
�:$ͳQ�cM�C��K�y�?�3g'�ߝ�qnT��);q�s�
#ؤ�Z�}OO���I:c��f�n�c��8W�~qy��.;�^��p���Vl��]Hԓ>^�H�^�@�7-AA܃��n���mL���(�uW��ܻ�S߿����
���T�d95�Bdh4�t6*d��
Dh�!Eh���I��[i���Ũ�\L�.&N��c
ܮf^���;�$�R)�\rip�9I���|ٺ��?#R�.Z��DZ;�/]��nݻqs��\�Q��E9�M��&�Bd ����]N
�mN�*D�>tgbK�>+ˏ.��!�23�]BȔ����R1ɝ���^��j'k2�ƮqBQq�[���$��d���i�]�i����cV�/�e`B����.FIIJ�q���b�i�>Ӥ|�p���;��
�
6�$����
{)��RU���>�_e}^��dz�dfzi� � �������%�e
�k�����
R���V�US���?6'���hׂ)�5�.\+q�U�g�zE2C��˷e���cŏ^���֔ibk �s�he�s�F����W������J�#~>�� Wk��~ݨ�}�ڶ>ơǚ�)��ZƉo���~B�-ڼ�rv��o�E����:Ʃ�3ۣ
�K7+Y�
�`Wi�
�rS��)�:{�>ڛ}�:�w��Ԩ�(J_�";�����6�R��%�
[�u�&ƫ�dZ��_�\'np���|
�RJ�wN�eT�����������W�,�=�r��r����b�nkڄ���[M3ܴz� )3-
�R.?��:o�kۼ�0TU��'�w{�����6&w7�j�1�z�����3��O�N'��fGo�O�?�)S�_��bQ���_¿�R(^�ԴԴ�G��. ��
E���t�M��ڇ��&��RU�i��W
�uQj�����
�U>�
Kiu�1d��<ѥIQ'RQ�1:O�/l�ŗᏩi��ʂv&�J���c���{��D�5
T��t)���1.��n[n�۶�X��}Rj�q�n���O�ʽ�(�~��[N��s{�ސ⛌���uO�,k�go�֢�d�RNQȄ �. �'��6���W��!�P朼t�dZjFG�E�"���]K@�'i�۪�N;����sI�[{SOzk�>��`
��r���R�R�+!σj�8�&TjlvA��̷
Q?Hy��j��y�LH�Nտ���JM��jܶ��T۽������l�G�?��S�n��KN�%<���
�nq[N0�S��q[Ta(&������
�t��(|HG��O�~�
�g����v����kݻ��T�R4��&Z$��#V�iO�Y���1�r�$�6���YF?e4�U�/M�v�x�ų�:z�bU^��g�Q�Q���+NW_'
4�jf��z
^��c�'#`r����v�r�ڡ(IJ/�J��
��ݦ6�� ]�-CW� ����
�����|_��{v*_��q3�^��DZ�}���Ic
6�
��U��ڌ�8p��
�7�{��c�rZq5k�����i���`�)�m�U�6|�
-Z��5�^�i�Ez3P��=:�Cu7�DF�'���k%�}�<�
��C-���ֲ̱#\,(��f�8�8%X�-��N(���c��k��0���V�L���������R~��}
��G�"-8��ӏ/��ϰK�q�?�(���#�nrV��Tm�Z��;�z�ióM4���
m��
|U��T�'C�^�����������������������������������������������_1X�.�gX��M�{�%ʤd��
��4�\ov�N":�"�������y-��,�T)f��LQ�g�
ۢr=�/Cƹ�ǨJV�r�[���a��+!��rT��|%Y\ٱ���zs�
S��>jͱ.o���Oc�6��f�$�q�% �
� �ǒ���Go;��n�[];ߎ�j���r�k�{��~\�Vۓ�NI�G�n�:�i��q���x�o�
�|��~�t� 5���)�Rxע��r�i�{V�i&�N����UOl
_��Ѯ�MfsޕkЄa
�y� .0��P��{7�N((�B�aI�P�$�
��K���"U6�G�l�
����ݙqJ��R�u�������+q��N$���
m���#�*���p����<|{:>-�E�v�=�86�N*�M�M�긭�U*���uѾ�?/^�o7;'�u,h4��xښRM�:5.(��/
� \ի���U.{���F�^��rmF�-�J�ɷ.�>������Q�"[4xT�^�OZ�~m�K}�T0�ݛ^S�A�o9u?�l�X��(�����'��
���q�j��%=X}"^e4w�ˠ|������rܫ
6�I\��Ķ;Ӻ�w!'��ڍ��Wg{ �i��������������������������������
�U�_9�
��Av�h��ۣ��ƾ��+�:v�s��/M��K�[�ɭīe{��`��Z�g��b}r�[i'G
E2���J��7�Ne�z�5�79w�R��q�+�
Un�
�]��J.��c�J4�M:�h���箽��Wx
��x��m^�
�p�c�\wcN���%��'My
�$�$|
:$��F�q����ɏ��¾ ^�қ�P�9J6���Wxv�u}ݵP�>Z'��FFdg�"-;
���[��¢����c�mWk�ÎT�8��n����G���%��ݣ��7*\�խ��C��L�R�Y����Zͤ�i���D�&�J#'��ehbSyX�K|���y�*Ӟ���p�S�̍�R��`�[p�T�r/��E��g�)�K���+
9�2��{_�
�n3zw�z��'�oŸ�ۤ�+s��Oj �J:�����`T�>�C�f*lwd\�fY�O�P"��
R� E�̔��֢L��4��ɥ� :��;
�.b�(B�0�2�r�J蠟9>V'9��M%)Iqn��h��P<���%�,r'P/�����v�NS�wr�#w"ݨa�q��c(|{kd�=^�0jT���MR�2�U�L��N��z
�|�.<�|��^�P��f��Y��22##!�,�K�~E�
B�E�J��ۜ
&�j���RN�sHަ���ޛg\�����r,�v�.�jK�3��)[��E�J2i�i��{KEi��H�P���^&��]�������G�n8�
x�=��K�}Wx�/������K��I9-ϵwQ�%�sp�ܾ[��^�R���}�S3$� q�v���q8M[�
��o�zKxcqmJ/���ӿ��{�_}7���&��ݨ\�f���6Z S��
yQ�z����&���� 7ۉ[�8~U�N��n|n�k�i�T���B+�����4���RI8�'Nc%tn{�!��]Ȋo.�nE�m�ʱn�J��� A�+�wy#���+�i�kǒ�ڂ�;�՛�s�8�5'K�mE:Ђu��""�I�
�ģ5p=Б�b�T���Y����-�ͽ�����ڔ詻n��g�L�
�2Q}$de�#� ��f�s��^�o�{DU���Usf��w���Ӷ�;s1T,Ǥ�t��ޒ�Q�\��J�=�.t�KU,�7čJ5 �N$y3��������k�d��SMQ���U�~�����mO����[��03 �$��<�uJ2|.N*���Am�h����t.�������|�6����5WuI�F�Z��E|]��7V�=[
�NH�'�p>��z��Aڟs�F���5�^���뜞"Կ
��Q�Hm����rR�"ӳ���ηer��+Ҕ�Z�]h����E-�6��J�mt���'�ޒ�=O��[s�Q��j)6�K}?e����4��v�_���K�fZ�heޓ=BV� �[b���Y��}l�ݒTT����Ь��{�ȫv���O�_qp��RAp��Vŗ ��6ju���=*BR�)��g
"�O1yh��b=tqJ�
gt��m�\�b3RY���+J�Q^�Ō���֍���
�\յ��\>
��+�uSi���{=��x �^w;uӘ�#�ĸz�Ln�*$��an���ok߷��C��Bӷ�}��5Yqv�dž<(�
���������������������������������������������"�_�O�Wit����5:EZj�2�
B
��ρ1��̊�fi[n!HQ
�F82q��1牙nqnE�p�T�(��2��RMoM4ϳO�u
':֧�_���X��j�����s��g
�jP�^�(��ڙ�{���2%E�͖��j^}��ZU�[Q�$'U)
�<�܂%!�s"�m
R�'���G5�M�0�<�+�zM�6�q�Ym�����$��ڕ�$����3ǧ�H�]�?o2�N�<8F1�̻r���_m�y[���R�f��59��NjpzBnl7*{��.��Q�P�
3N�&^B�LJP��j�A������HCK2Q����}�$�#~��Y�Mq�8
�k�(��MFMU)8ME�q�Ty�+�Tʞ-�ar5�y�ܕ�OXw!��e;q�-Jq���ܶ䓊��Y��:L�C� �U�E{/�t�>r�"lI��9)3KJjϤA���
6���SEE�$�d߇��3��K�G*�E����n|P�\ԭ��T�n6�I-�ƍ�K�Tj<1����H_z��wG�r19wF� �N��8���ݝ���+� a�9�ɫM6�m��he�P��i�%��m��m��D�! """"""*1�b��R�KrD"��vn���rM�۫m�m����������������������������������������Ľ�m�]�ӡi�G��� ~�e�"˩��
�l��h��R��T�Mk��^�M�X[
"J�
ݱk7���_ޕ*�
�DqĒ�&�flՒ}�����`W�}~Sմ�Z���{��ĕ~�wm*�/�{��{ѹ_���-��0��ط#P��]xlڱ~Tn5�w�i*lڪ� �(Jx�i�o���Ϗ�bq�K�Y����R|!|KN�53�
OS222$�jzw�w%i��}>���N)�E��+����r���ۥ��7���c�$
�O�fl/L�N��ث�\��6�H9:
F�Y���I)fB֔�JI��_ ֣^: ����9��mY��{6���6㒢�7Uj��]�:���.-�os[��R�&�g��������MF3��˸�#�km��jq��^8�W���"�P���ΦU�R��j�ʄWa˧T!����͋ ��lW�48��JB���2�ko+
/N�w
Q�w Q�zQ� �ے���%$�ޓ�7����^��Y��L�|�
��r��7!v��%T�rܥ &������|���M8�~y���b�����rn[
R��V�
g�Sn�{����{*#2#Խ�ᢏ���Ӵ��H� a�k"
�ӌcw��Ҝw&��R��J���0��7ױ>�Ļ
�����=�^
B���Ɇ�)����v��32.�M��1=�#�6�%�̠�tҤ����n�zq��M�w��ԣ~��s�*�%�-����j|���_���������m��*��.�Yx9S��z��=���)qE4� �3p�k+,`�=���kN�R�ڥ=��B��=nŔ��NA��x�)Q�$�ԩ���ȧ��4�z 3t�#Z�2l�ҮYn��$��S�%��y-�
�J�� ����z��G�p�u|L���BV�7�ZW#
;Ww�ipܷ%(6���j�F���G��5#��{$D"�uۭ~�]�֫�Sr��D���܃��f�Ҏ���Ӿ�+��T����u>-Z�T�Q&
N
�|��$���沸�ii>����
�e���R��W�ݳu'[�����O̻�j8���J��ۻEѩ[��]vni=���� ڒ,[��_%��k��C7�I��3N��v$��4Ɏ���Ј�e��ٸoU��u:[����}Do��5�|��zN�����q�=�T�r�e%�ɧ6��&���~DȍF]ƞ��G�5�q�
��m]���/���w�/
\ʲr�8��=�oʔ�e
9U(��W"�|�S]uZ�d�#�?S��e��[�W��"����ֿh�][�-�7Nu�:�T�=)�R�}�.;ml��*5D��l�f� �$fF�(̏T���
�hiI����U�U4Sz�ɕ��
��t(
�����%��_�|���2
������~��6�eM�����;T��ƗK[f�&]L��K^C�E2[��ȏB��O�d;�M�i�|�c�x�,^��6��;s��ی�G�p����Q���\���NuJ����IFT����J�~�đ��Ar�h�*
B"$���H���쉩�eX���PRj?s���l�"ԥ)�su���]�x��������������������������������������������������������������������������������������p�Դ��Y%V�ES��H"Ћ��J�ǰ����
��������K��&���5��^Ukzׄ8kE�g���S2h��&�Se���\
Y�����l�]W��Ҷp-Z�U��vi����7�QS����:4�byq��Oo+[̺�腋[6-���_��Fo.����6����[7$p��&^�
_G�Z�
���Ը�ߍ�k
���c
�������.�qqo�I�[�9m������߸���YxOZ�Ц��1u�o��i�SH�)P9Uʄj�cq=
S����>֙��N�eR�><;+�ڌk�%_q
T���]�.�s
�rNO?�s�[���=�v��H�[�]�RZH�R�Mtᩗ������Vؾ��:
����/~���u�)�ԍdg����%�=��e�d�V�rISb{6vSu=(�ܥ)mT�v/J�}̇�
8���
S3a�d:^h�BS��f؉Oɔ�L��h���I_��1d8�,�L>�<�_��A0y��3r��X�q����"��'(۱;��m�FNII.v5�_(^q�~��X�>y�{3�צ� I�����*V�ܛv��/jW��'
���T'��N�R��'�j�%�ꔩ���:mJ3��S�B}��!-H�-��R��JBТQ�
oe�di9�t�j�E�N��enPp�ke
.%4�]�#{:>����m�kEɱ��dY��Wl\��\���\'nR��M4�&�U>?�Ќˉk÷�!������]�]����5}UqG�~�ݏ�I"��O�~����s���6������(�Ļ)��qO~����h}�uԕ�d}�Q~��G��,o�E��!&�G&�/]_�����H�-����O��=�o��{�k\�̭bk���v�.��Ô܈+;��arZ���x)m�?�M�\�3l<�L��k<��C�q�r�KnV��s�$�\V��B�gD��]w=ʑO�/�>U�$mk�-C������F�X�j�T�v��6�u�'�
��g:V��n_��*��qk:�V�C�
��A%�'�4�J�V%EY)�����#BғO��4���<���e��jQ�Q�]���y����U�r4=w�
���m���[���K�1r�%Iũ-�
�������O�}����|k�C�;/V�c�ݩ�����W
Z�)��EHdž����T��ru��]��8��hgĵ-;=>���������U��_��
I�n�v�Tm�_jBM�+Q���iF�"9�*{�DI/iuo(��=Tz���ϖm��<�ot��?[�i��7�'Q����'�?XY�m�Ү��Kf���ݸ�I24�Ihg���8�a�C�[�ޥ����{䓵mF8�✛k��˱
�RR���
N��A褨��H�z(�1��݅�ӎ
E~���O�XdžN�{u�g�(�o��O��5衴�Q:��mU~�N�F�zk���se��\��ZjfH��7^F
��QIڎ�۪h/��V3j:zT���~�b����� Q��V)7�G�'��]��W
�� 1""��ǶM�/b5~��s���v�/|͝��'K��\�RI�_q)��DJn�f�JI���%�9� *��p�fr����
-z�B���U�W�Ԕ%
�OkM�n-Q�?�CZ�f�
'
����=��
��cj�.�ioi���=9�E��O]>�P�Q��l�_�v4��z�>��T������������������������������������������������������������������������������������*�ȴ�>�YF��;ε�\t�]��������E����H��4�ꌇ[�Vr�L����z����ef�
��2T^�V>g���2��~kg����5�~N�ק;{�~Z~�W��}&����BӿS2$��J�?�~��(�Y�"˲ߩ\�O��]��:��
�����JښT����{��m��m��I�ѩn3˧)4�L�dFZ���/����zU�G��
>�U>
n<�k
�5&
�ϴ�-�KJ����i2�����o]�uKljv�K�3��$�bԔҚ�V旧i��Y�5�.ί���fi96�v��7!v���))F�JM4���{�j��G�~�J�����t�����/���lUE%�p��T���A�Fe���
������4�
����q
Qk���\ve۽/u�/I���m+�W')v{\-��E|Pm�s7
߮D������ZRr۞/����mu�*�1�ՙa�B��܆���
-��x��g��3�#6��ۥtRogʌU)������]ZҞN�nŞr���}F1����Nnޞ��;cZ�{N}���ۿ��M�i����ux�ʉ*3�qi'�9
KHQ�$����W����J����x�Xyر�Ŕe~[v5�~�/j��N����9����Q��4
o�6��rJv� Fr�d�
�x�M*�iRj�M�zUi�
��n�H�����d� ��н�7�ᾞ�S��=��S��'�7
}�
��
�̽zt7�K|_g ��J�����=L��q+/B����������� �w�_\ۧ�x\�H�JUP��zQ��<
h��qF[�V��0x����==C��s��U�7q�|^
{�)Iq3�8��$�_A(V���gcKu��0��6�Ƅ�����"%��i�~�_��ˉ��k� Q���C�ܣB���8K�u� ��/ �u(�[��w��}$F|8T
�ՠI�.E
!;R��J^��}Mɒ�D_q2�
�];���Ɖ{�5�}*�n7nEI���n��O{Mw����v�}&��q�+v���
[V���}Ĝ@��%>#d�XQ��
�$��f;ie�p.Gq�uixVt�
x6b�j͵mlKقQ[�T�]�z���s/&y�ە��nM��'W����}����!�F�����p�_d�^T��������u
��N{�ɻ���'l{���խ��2�.�sT�u{��W�^��H���&;1����s�)P���� ӛ���6�����>�$�m��ě��;��Łn�j=�
�f�L�T�)�>+���qRe�ɴ[��U��R\L�*P�/!�$�Ӊ3Q� ������������
���'�K=m��~��6��Xq��W�3��^W�����+��ųO��_[�F$rR*u"��
���T�%@O
�+�%��#
]˽!aܽz�{��ͷvQh�쩎]���h����G�ތ�5ɇ*�Dz�JD���RNLi
4��������������:�{��~�2F�m�����X���Y
�-z��zĽ^f=�]��u�ū{��/+�&c:��M���a{�ĝDp2��m܍k�Hș
/(�-�-���m_vݮK(V��{R}�.k&��y�ƴ7i^�4@�3f
s��K�3�^��Ř�˸�
B�=�]��?g�t�5����Kb�Z���B��<��e;���kQ�L��px����u�WC�}n���
���5�Ҵ��e���p�B##~�q=��
`���x]KW��
F
��{��GfŲ�}��?G�
�.�I9��pj�W�k�U]>={7��q{�����k�O�
/��^���I3==f�1ɏ%n�nʫ��/Zu_�y��X�N<�������5���7�ۍ����'v�y/"��8��넭M2e�Է&�Y�,���в33%����
Ik
��jM�r7��x�f
���n�mQ�k��X��4��踼>a�-GcI�eތw���&���U���=����-�:q�n��W)z¥j
:��� Wq���S��Z�v����Ԓ��#�j�"K���rIU������)%q�r�mR��o��DGQ~����S�Y���Rsu*�V)
�
,�/�x�
)M���F��D�6��O�#]z
���9�����6[Ui(�JR� �fw'y��$�G�e�����U�ީk�������dMF-�ݻ�98F2��d[�o{R�n0n-���x�sV��6�D��h��|�Eb�2E:�K�C�O�Ӫ�v4�S�JCr"J�!�!m,�hRL�D|
Z��Y�Fm�/X�~Χfr�����N��&�4�Ƒ�= Z�9�M��h���.M�ܵw
�/B�d���rܥniŪ8ɧ���|y%[M�=��_t�j�?F!z5�
\e��v����M:��\
�����~�F�-�s�g钬�����������OWq���ii�ȍ<�G���i%%n
2rq�ͻ�l�lƑ��)���ok�w�7�}�\����Uk�-���:�&�f�j��솘�Xe�r��V���9yZu��ʼş�dF�C��=��rmo��%�����~���Z��N�78X����(�N)��_�7.Εn1Mp���J}�����6�2�j�j�J�dI�";�R�5�&�iL�Ը�c:jm�
�q�iQj$u�j���p�\{;v��5�
���B�Xn
Ą��4���qO�E�Rj���z�N����(�G�a��٠䌡)p*�v��(J7��#Z�ۻ��Z�8O� �W
uO�N�b�+^Qipv�������9G�v��ֽƼ�ϯ���rYƖK�G�J��Q��D��N�Ph�R�Jj����ᡧC"21
��"9
ѓS�1��;R�_O��7/�WG��z)���8�fE�%F���2���ukmv�Sov/i��Z�&�/�]~�K�mI�[�:�^�~ͤ����\� k����M���i����稜�\y�w�Jt�3W7
8��Ʒ�~ݥ�eF���g�Ѽ��w"8�VVSج�\�뻆�}�ݭ/J6�����Q)d|)�zU<���HP�`����7) ��ŵ
vlA�F�}��
��svk�{.��G�rR���s��Kpr[����o
��on���u>�3>�k��\L����=����;ow֯g�N3�pK�ѫ�|wmk���
�Z$�z^2��R:E)f�>ς��
���н��d|�#׆�?�\���ǔ��p�V�{;\$�Ƶ�E%-ͪm0�S���6�[n<
���kE��[}m�vE��4����DDZ������^ �$O��Z���0�����*$�
�~�X��U�v҅B�@�����^�?��]����s��o�#��%��o��j�w�;��Y��#S��x�x��u����eBگ�y v�^��i��-��)s�)�zV�� j��C{7�G����t�.��w�3v,�ygg8����s]�a�E�_��,�*E �����t��Y5k٨���h��=����o�"m泏:�\�6�w噓��ai�L�n^�c\�75A��G��k�Я��0���Lf46َ�`egZ˓p/�k��;�̛]kq����!ݸz�p�ԭG�"�}���R9Ve�>�ˏ�HUjJ-&���7
n�����r�n���wG�*���Xv��\���˱/v�N��}O)��ʼn��&C��V͍f̵]r�\��PMB-6Du���-
#��RͰt��R�����N^)�m����T
�_���}���nSȕ�
�C*_xBuT�kJ�W[��`ɩ���`e�j�v��sn�����gP
�ڻ��.��-���WU�tܑqԹ�Qj�)t;v��N&RNũT+8�%I�
�X�Ӄ5fK��՛�-d���9�
����������]�CƑ��m|n�Z�-6=�H��z,*aE�
��m W3Vz������Ršd���Y�~��X�f�׀����X�x�"]s�;��)5
�u�*����ُ�H�B��
��BRG���S�6bݶ�ؿ�
����9j���[�1*��������jױg�a7o�X� ���C�U�I��%0�v#�~\�-�O���-���Ꙛ��u
��ɷ���쏪&5��mY��٦�
�����M`�L�J��2�qK~��HZb�r �=�N�����'�Y���ob������I�.
��(���^ ��{_
��?�O����J��`S`3������B�N���[�}�5��w6:ǵ/���iS��l�t=���4�F�*d��&��T�4�y/�� #.��
��ɵ��i���m��5U��ֲ��f
�眕6��Y�7 f�ơ=�3dϕq�뚩$�q�TM-%r!$@A�?��
��V0�c~{��[{���;��a~ڵ����
»&ڄ���v1e�k������=�
�wb�����
���������M��L�kN�AԬ��w���-���x���>��~/r=�e�7
�3V��eV�N)�K�%Sښe���"���+3u �X���u
چ�rn �ֺ�VzscJ峻�m��}
�v�b㶓n\Y�bI��UBT���%���
*�,���0nov����=;��z꣓�S/nS�XSpl##����k9��m�XGr�Z�v^G�d�e!ŷR�Ԡ�z�QyjC�]`�g���T�o��Po�v�{����j��~���KR��B�M�Y�}�i[�
߶�9K�L�����2ԉO0K#���m����>�wB��[�ٍ+n[��[b٦��D�X����
ݲpo]��
[�\�m�5�qdT(�)m��o4�Oy9Ie b][���wղ����m���M������~v�m�i�۱�~�t� �\�}$я���i���mRk��(�L�
�c�
Cvk7r�9�_��r1����
�
;�zv|���F��@��Ky���Z�[��&�jE��j�i/��"6$69��ml��#e]��9s\���{�Sc�L�}Ȣؿ0��q��/�nZ�*��t,C���L�oD���߉���Nj���
ǚy�=�P��gm�u6�^�]�
�l���-["��çU�ʖM�lʍ�p�-���"�q�m���U>۷�u�F�OJ%Ǔkx
��'g=�睋�k[�3u��,�����{�³�Wɘ�ݪF���]ՍeF��X�������"�O���y\�,cچ�=���w�/��
g�n
Ļ��������]����#2�? ��v�q���y-�gX��n
R�.�^�}�ݺ�F���s{�ŝG����]��}�e|#�0m�j���x�"ƬW���كm?rgU^�xV�����B"�:Dt>�@L�R�����b�un��~����
ݭ,�w�+��v��
⪕;
\U�<�EqNj��
}p\
�.��ˊ&�C��+i�#^��Y�z�
���|˸��������va���H��ѭ�vޮ��=�oQ�U&��C��Xq��>��(R��Ya�61�>�#�Jm���˞��Μ9��g��9��X���Ka��G��='���u8���g�f}'q�y�#���ɉ�
�w���
����J�]�We.ʲ-<��+&����q�%s���?��2��dњ�zt�Ҽn��`��cΤmm��qMdz���
O�[��-�ߩӲ&;��[t�mܝV�n�r"��>{��x���<�8�U�+�p����:I���g]��z�j����Gk�t,u�<�P��X���vvK�A��q��P�|���VbL��Y6�A��u��S.�=:�gT7MN�5�{�_
��`;���W�zǶt�Q��5��˫c�%�u߸�Z&�L�뉩<�oN/`�(+�,���`�N[غ��zؓ|[��6m�lI��Ε�i���kv�V��&�B���V����=A������o<�%�
p.9�6�,n�
��G�.��Π[�{n�^ ���h4J�5�\�^߽ku�U��r`�L8aC����܄��<�<ğ�,R*I�&ľ�n�s�7+G�;��f�p-�d�v5��&_N��Ch���m�m�����3�s��4�m5��$���
��w�:�ڽ4(�Iz��|c�dǷ-�t����g3�{���t�Y�w�h�V��obL9�N�G�TfD4:�i�$�Ǯ�����n�r֮=�\\�w�z߉��}$���<��bP�H�o�#N�$D��.ʛq�59#F��b��㚜`�2�����}���
揺l���F�wM�qVo�x�T:B�Y�/�.�]��0ك��Y5)eXn�R�ʠG��o���e�e�d����X�o3w�g��Veخ{��r�~S�Q��>�zf}�d���ؠ�o��J��a�کq�E��q �-��(:d<պ
=���e�����Ky[�˗^����%ZX�kX���[C����2߱\�I�T�TL��GzA����N��M������i<�/�o;��3ߐ��v�#���^�Q�6[?�rɱt��
p��sp�`�e�ޭ���x;�OSM����� ��m���Kҏf`��S}�A��
v�����m�_�
��Z��I�\w��a�Ď�tnޅ�����wa�`Ń�r5�q�����ҩ�K���f*�n:]63�ŁO�+6S��iD�t��9�������������������ŲtUR��I��������������G���5��`��σr�L�Π\6
ZR5O��qQXu�A;�֪
I�fM�Ȉ���
r9zoQ�9�
�N��d���W�EW��jSi9Wf��f���w�?1�����qj�U�MYƸ�r��ڃI��$�NK]t>]K�>Us�O�G�DDD�.�ZF���6��*�
҃V�� Zhz{'���x�p^�`�
��wo8��r0�h�
��Z�mJ5�"j
�b[��l=�y���Uu7-�;�7�I���T�%��:jFj�ߖm�0t�zU�'���K
)��څ�Nۧ��YJ)��4IQ�}��^�K���W�m��7k���SP�>q;��ނ��#)'n7&������r���?��óM{I��w�R�\�j2Qn[�v
��pe���#/���tA����F\�ϵ��225����q�֒�om6z}
�)6҅*�oq�D�s��M�f
CN�I���N=T��� S2t,<�e�RZ�
��D��ҙ)BcI>_�ѧ�}���k���v���e�M�F0�J\Rnnݙܹy�[r�U�c-�j{yG�tkQ�%s���]5�qB.Nw.�JN1���L�v���R�����
��Ui5J
Z�E�S�Q�ԙr)�:MJ+��g�}���χ!���2;���q([jA����u�����d]��[ljV�K�3��$ײ�SJI�=�/|�&���
����t
�l�'*�n۽f�.��f���rܥ ��jQ�O�����8>�&Z �];��.��|7T�/C}�$ڋ�UmP�2R�e��ҭ8hFF\L�� �������3~����e
v�\۫]��ݝ�Nm�r�
�nB%*]Z«�h�Kc�=��B�T��LG���
:�V�7��4$��=Ǘy�+E�X��'��4tn����(�I
:�Ѝ;�D���f�8c�,k�1�%�dJ6.�j��6ź�{N~l����6�&������*�f�œ
I7�
W��A�lGO�u��-��Ң�H,,�
�(�ǔe�����뿋쩨k�M��܍ ZſgR�vQ�' �9)?n���|�e�r˭|I|-���f��GK�.rΛ�p�8XV1��%K6�mvG�+tc�+q�E�
&��Ǹ����C��_��N�m:��l��=_��/�m5^��[dߌ��ڇ.c<��%:�)��t�Q$��Ow����~�-a��Y�;UJ����>��=F)�2[�n�k�����؆�?훐���
�M=����l6[4�(O.�]�2#-H�^�n��#->�&m�p���5~Fӛ��+�|��|�
�S�,��xa�g%�����q�k�EUz�����UgæBhߕP��(��7]����k�Fnq?֖��C��pru
�Z6*r�E�ڊ�tS|*tI�*��E�}�7R�<�,����nU�U��֫^��I7��Q�*��mS���l��y%rd�ȓ��d8����hE<9oH��h��M���f��NS�R��j��[i7�D�[R��j��݊���+kდq��{"�$�$��H?p���������������\��̅�S�?㭻;�t~�� ���R��߁������
���)^/>�Qj`y��t��[w ԛ;�����²
�~�+����ߔ_ YW��~|o]���
��
?��x^�ᯛ� `ʼn��;g����)T��@��vW�n��]���>&4�l
�p�+�$D�������̢1��l�|��ȨF�%����-����}���.�9[}w�~�
Ԡ���LM��9hС����ablf�e���&Q�oW
���!����s�?w��j��L��K�?�s7�y��O�>(���=��C��~�_n��y�ǜ�u�? v�����3vyo
�o����I��@���qV-�jeES�^�[�9W�oS�ܝh"l�2�C�1�a͔��C�iJ@�3:Pճ��w�=���/7ov����uk�+\V�;���l�D�gն�����<�[A��+r
X��~�d�;����m�!_s�8ݖ���;��;����.�0llUC���+��?�i���#�_�c�r�ʙ1~�C.\����q ��
u���l��8Hܶ�2�����m�`���ܻ�M��3���T�o�v|�B�s�
���� r�ɵ"o��L���S-
�D���w���=T�v@�f
��'�6�|YlD��͓�Y����%����-�#Ѯo%:�&�!�3o%�\J<02����;K8�7���>�^vgƓ�# ���;�ݝ�mz�^Y�6=���P�S39���U�%���~
�&f#�
�}o!m���uH�;��
ʲŇ��˷��yvP�+�&.7�e��[3'��v�R4Y�j�̗IZ�`e˽3o[W�U{�
�m[�sU�b���ۋ�ZǾ�ۆ��l�6~9�'V*�.\S2��<�Sd�*zY�[aŶ`]���C$n�.�v��^Ʌ�
�dng>ەZ�����,Mmϑ�
:�n���6�nϦez�W
qUJ�4!�
ۇ4�R�! ��=>>F������n|Q��[{p��R��O� ��1��7��ƕ�~.�_����I�
'��'��00���k=b�՛o��}Osð���c2�'o�\�3��}ݭQ�^�
�2
���.� ��R�1��yK��ȣ����t���Aݿ�-�u
ܾ�w!��`�?1Wh�n��|�g�z��U
��o�[�E��CW��w�jUIן)^h#�1�ɭ��!�/Z�����
�n�p;o�;�ΗŻkX���s."���6��E�`Z1�
עӐ���9Kl�8�q�d q�} 2�St�t;��#���j�>;խ�a��b�ONŗ=f��w�P�1j)l����6�J�̶|gV��2�`y���/0E˛��6+ԫ1�?
�6���}��KW
c\�K�oKͨ�2ۅ����F���w��s*T�ԞLיu�Dx�� .���kC�zW����X����hy�۶g�L�u|��%Tnu�pǺl�-�����S*�� �P��
RaL����n����T+���c+�*�xl.v��!�.U=���|�; ��!_L̎뱚U=4�hm:ٯ�"y)$�:�>��%�(�n�}X�'��p[�ȴ
�^���˒���4kƓm��zD��x�
\
��'N��q
a��m��P7�n�yN�݅�=������<�j�v>�j���7%��M�cS
�ڵj�%�S�T�y
��qX�y���m��vC���g�{w���/�w��=wS�W5r�̹�u
e�rծˊ�sO��m�=�D�h����E��Қ�R�b#n)�Q�Oxtվ����Q�we]�I��}��wC��a�'"[ۂ����-z}2��U�u�KP�$㜉��ԧ:��m�c���<�Ý>R���oL �?������w��u|%�ҷ&�����K��
y�_�!y�9���� ??:tq��3�(��U�U�-�l�k�
�S��'���ɸ��@��j��dz��Q�ˬR]� EV�PW1D�Jq��2n�:,
���c|ǻ̑��;���y�{X���,ۂ��.�u�.b�����˕u�.tK�B�jQ"[�S��園S�`��ٮd�Nب�e�����J&9�Ơ�
�~�0��a�(V��m٘�L+J�r*�vڑE�(�
��x���������0�+tp˕
�n';�w�m�-ޜ�MOxX>���{#�2%j�g��b��2�M�[�`���K�*\������5����@�8���l�'e=0�u+w
֘鳾�{y�܀��:R��*
Y�a�]"�<�Q+!�
�")WJ�X&�a*�z�\�8:�t�N����7�܃�m�팮�xWq��۷����p.�'"b����H��'��FD��)o#�6�u
�l�l��ۭ�y�����M�����Y�/+
a�ڍH��}:����:����":�J�&�3���Q �@>�Ӧ%kty�n�lۣ�65�,3gU�}��{GY��rb;����ge�'T��K�w
ǘ.��,�r�p�ܚ��V���]����T�r�,�!d�p� /ԺU�,x��Չ����
�>�s~W�5�o�Th��
y ���������x�?xrr�x��?)�?���il�bT��,������z$�Ԏ.U�H�٠\U�1p�U:]J��wS������r�GZ�q�8àd驐,N�67Q
���YB�Ӣ���D����㏙W�!Q25ϸo9m�s-�7���-��%�����3���Cih�����O.J�鯽��-�;M����Z���M��8k�u����-7�k���9����S���$��8���]�q��2�E(�}����b�ۏI�[�DK�OK}��3�K�
U��B�^u
%�����Y,u.-&�f#���]'܆o�$x�`Y���u�,dz�wM��;�#oKx�n;��\[d�7}Rb�+*Y�䛂�Zu�Bӱl{j�0��O�̓��}L�hK��;[a���ֶ���aGL{Cb�#��S�.T[>߃F]NK��"u^LUʐ���_ykW?�!����G�R��j��2�9��͖qa�'0[��n�����pcD�vV)q�z�9R)��PۨM�
���^aJx
W�]
r�>��];e�N3��v����xd��m��Ę�(5W�2K1�䪖�weF�{m�E�/���QP6\u�5�4x��5[hۮ-�N��ki
[�l�U�g��L]J��}5
S�:�EhiU�r���gH�l��!ŒJ$�������������������pe�=���q�^�b���͵Q������'
?�6�|��
R���\,�JA ��ڵ"T���D��ꈭ:����y�mg���`�B�5t�%M]��
�<�N_z�v2_O��rtٵ/i��/ReӮ��*��
7[qүq�EG*�� m�"��[�I:�6�e�^��p"I$�jԴ���ęh�!m)]�G�Zk��cjS�!{e�^�z��}+Cѥ��9;R|/�ֱ�ei�U������ԏCN��u2��Zhc�ٗg��$�ݭ��wv�r�
P���8*�7/Lk�~�I'Km�1��+M�W��%���B�k��|����oOm�>��-�#�qj�*��|�D�<���Dr7�w?�I�hi���CE�%2m�F��ۜܧF+j�����t���tZ�T:5>bѱ��k�n|���n��{v���#�j���Į��qNpMIU�m������(��7������L��iz;{�Ҝ�ݞ��ڝVƚ��V��Ϭ�+sO!�Os�t��G�vx�Ӊ']uӎ��4�g�_�
�1^-8ۦ�� k�!)Ύ5�O���;Y�S�B#2��Zzχ���;<.�ֵ��Ot�ge��~��.(R������C#�w�FZe
��G��Z���ٸ�6�FFJ4
�e��2�ˇ��pJ
T�$�[�wg��V)�q6��muDG���J�56��q
\�I�����!�̗
y/
I��~R�tJ�9kJ]Iy*��'�FN�� �0�s .[��l�����!��� �fw'y�(7$�œ�����
W�ƫg�y���ΙdMEU��� JQJv̋v��mr��ۖ�
.j�W�����R�_�M�֨�d�j���YgSj0^\y�'E��oE�Cjm��$�
I����Ʃ����K>��Z���2�8J2T�i�J2N��#}.��s
�cA����rl�嫶nB�.FIJ.�)۔\Zi�M>��/h��L���ĸ�=C�����1�s��[�?YMqp��|
��94�-
��鮝�����𦔽/k^�#�NT���(Y
L�S$�6���˩}��{;5 �)B۷��W���$qpN� �)qqoo�t�
��}��Z����D��V��ә;��7TiK|�6�f���3
��h�$�dԄ}�f�q�ݡ�>N��b+���Ͷ����O�]��>�ߡ_VtYf��79ڰի�F
s�q�~p�r��ս�|Q�M�)g���%l�0��oc��J���ȨHz
�V�;B��b��/����kL���A��
cf�PJ,�ԭ{ƍgp���jN�R6��V��S�I*��$��!yV足���j�ᇑ�.]�(E�ܣ�����q��M\���qJ2����eZ�T
�).<9U��B/�(��B�0j)����mt��K��Ej#����fDI-=��r���Z��ړ�j����|'Nڤ]k*��i$�5qt��"ݙ
PM�6E4�k���e^��Z8ۏh�z
$���Q(�R
����
A�y�2z�fRñn�p�������nkbk�I:=�j �
����&�ΝșW?
�d����{+�ύ�M�
��'?��?�Xq��e���e��Ľ���.������[���o���=�Ux�F�S��=��ӷ�dZw�e��n��Մ������]��_�X=�ĭV������a�*
p�K�s0ބۍ��<�jT�Z6����G�����
������G��4�ӵx��չ,�p�ᒊuMMx��STT��tl�
�Θz��4�K�d�&�k��ͦ�j�;���SԌ���ˁ��Q��zz(�M;D���yƔ�7�W��bqJ�f�J3�
�gz̚i|�wnxtj�c
¼5$�{(�1�f�� X�Q��65ȼ�b��̶����Z�k�n>%�F�����Q��MJXӡ���{TZ
�E��V�N�ᖣ�im�T�/��3���7cNJUPn�����P��҂ZO�E�~"��-R�c4�^b-
FEͧ
t f5�[�)�S!��O��Z�Iښݲ��͑���;��t��vܡ+N��
�)A�R��=��h�C�N��n;��w�L��1�6-:��特7����M������$�=Tҕ-�.��R[Hٷ�����nX��k s�n[�ҞD-�0WS�����9p�9�:-�Ϸ�-�
��jѬ��Nu{ҹfv�)[Ľvwf�g(ٷf�e+0�mY�j�8����Q1��\�ݧ�g��]�Eǎv��ڿc�!4�#j5�
�����̋��C2"����}�B��Rr�i�F�p7����=ô\T�Z�:\BL�fj#I�22װ�<;�
صZl
j
6���
:�l"��6]۸
�K'�6�R�T��ѯ�^ئO�ԓV��\��?�$�x�7��s#�r�:��O�h���{��ց�=M��m�u��H��Էd{��p�N
�/܅:�U�E�#Yy
���+(�S����gQ���(�Щ)R��H����z��w>����^�Ѿݻ��>�mK &^
�'$�J�ۻ�&w%F|x f�����z�%�˳�
L~3N?Cy�9����������
�v �w/�{��ƿ
�kz�3x�>����
s��X��v�}�v�P"�@���WyC�
�z�`�'�
�톽D�w��%-�t�t
y���V��Y���\wm�uPY�Q���A0iG��-2
�JP���,����6��/��gˢ]���u.-n��!Zw����.�N�7Q]�����Df}Q�0�� (��{�a�\@�=�i�_�X�7g��Fǘ�8^��
⻲}�G��
�M�Z��1)���W��Ef�O�1�2�G�+=-�B�@z\����`|��|���w6ċj߬�m�}�U���w��Ro��x֢I���
&c~X�GP��6Qnd��pv��ܻu��l'V7^F��J��t�^{��b^��B(
L�~s�ѣ6@߿^�x��qU!ڙ�5�|�V��p��v��ef-��u��ӥ^3�
��
��F�SDɯK�D%0��r}��F��F穛���r�7
�+o�"�V��8�t��v̖�N�QU!5�uF���d"bCr^bJ=�֤�fM������#ʳԷP��0�O-9x��������R�B��m\�=�`�r-:���;~3T��l�(n��XtXi��%2Vٛ�#v��� w�q���ƴ���`�L@���"��H����
��q��W.j,J�M���5B[)Wܺ������������U��eZF�q����c'V���˷1W7�V��̾���-�M��H�Ф�w�n����8N�;��H�P��S��d��ݷ�C�7&�2 �j.�W���\τ��G�Ŏ��'�V���b]c��.x+���R�x�1%�C��2T����
�{��my��g[q����U���|�+�m:M�:շ�8�҉yWd�)Ջ��W�S%��%�����:��iq�����l�ʹ���m�������G����wݹ
W��nNŤѩ5(9� �hT��ٵ��DdG�Ui-�)vSs�2 2��{O�nT�$�����X��ck
n:�¶��(���lA�S�L�eȔBjμ�Pp���Tb2~
��N��2���~%�^�k[����ܗ�[�J�zs0�ӓ
�H��BKq[}��Jَ�A-�$�dF�����Q�gjx�xF��v�4�r/x��*Rm�%�
�����`�4�J�(�&�i�v7�S�k��Բm�SH1�����Y���Wmx
8n.���k'������]��:�Z��˭_W
>ڃX�Щ. ����jT�q���%��A�ā��[�E��}�am�c�]�D���:�rm�H��Ri�u:�uӚ�Ӣ\p(5�����<�i�J�$�����@������������������������:�"2-{ D}�ٯn���]��Q˅n�{
4�*ڣ�q=W���s�-�K"���;ĝP(��7�
��.�0�
*Lɔ��EB+d� -�m����O���sЖ��B�״�.rP_��ۍ���#jw'7'[p�r���'���0�WS��\�}[��~�,�S᷏�rv�k"^%�V�����9�(ґ�F��3Q+�����%
۩��fF|9��
�I��nܯA��%+M4��5����q�ޟa�+Wl��ec4�qq)*pJ;ԣ%�\I����T�;8�'aji=�T�L�E�222��|��l�v
��Z��m�ʮ��
�T��QFok^��T�8�&��n��rF<�K���fssi��-IB҂W��ԙl�S�U(��%�s���Z�����r�3k\��������+7#Ɣ�N�~Ӝa(ɧ�J����I�7NyS�
�����b��#&����nV��(F��\��۽o�����[Vʛy�}�w�(jD+_,Q������-
�f\�;pZ�%�H�[��x�7
��'�Zu���ëܹ�l�dc��$�;�n3�IVv���.NӔ�R�{w���勝��wmeY�����9�gۅ�٤�s�ǽ��l�)[��GcMN
�ٝ�/�ӷ��*�T�jZ+��ݥ��/�N�7�*��22{NN�Ġ�«������������
�h�T�x����������Q/Ur�sͮ�;t�]{E��e��]�i��=]�b��;
���.�Ի�؋e�{N�m��?�[&�*�U����
�
l����&x;- ���
O�կg�}�LU�o
��|�ҧ�k�lkӹ��:q��v)��K�t���5l1�d��ז�RS���������Tt'�\)J7YJLӯ;dGΗ: � +�WQ�ۜ��k
�:�Zrp��d�>-�q��%���e)(۬ҖȽ�I�����f
��<����߽p��r��&ݫV�fY9�1q���2�ĭ��EQ�g�Y���bTGQ&,��y�L�+��N$��[q*RVۉQ �=F�u�T�ܻ�>�f�>�f㋳8N��6$�܌n)9&�»����i
ˤ�s������X��,݅�܍ȩ��v�+sR�Tp�O��}�d��?Wn��/I��np��ȸ���%O]S���t�QO|v5������\}�����7Z�wb�.��AI�V���������K^:w���
b�{[u�ݯ�c��yt��O����߶S��<{8KSR�ׁH̏��N��7�ۚ��[x��kw��Yy_������'�ZӵF�+��>�쌛Z�U�Ħ�r��eE�9�������F�[2���4�D��e�{}@��:������ExWs-\ǻ7�K-\��JN���vE�k���%
��
:s˙#κ��]��.��o�ͳ;�լ�7��w�B6n���w�u:�$���L�������; D�k��I#Wz�����.:����X�p��(�˅v$�Sq���
���,�wn\���q�I�N��-�����e<5�����O�e+v��u���YT�p��cojUI������_ާ��P8���
�����O�
7&�V�L��8z�$�_�B-H-�[u���h�]T��{�|8�
��=qVR�N����-:
���Ij:7PUtXϷ��m�������y��鉿:RI�M~�33Ӹ��S2#�׳�����G�dŲ5+/�B�x{(Wz�Ȩ�����5��Y�㞎�#|�˖�+�
�ط����.|e��<�o���/��r���ߔX�
�>���7s}V��E���.
��OV�ti���
.5���nN����J���O���"95���{�����#q�}�Ay�9�d�o�]R"M�6����z\��t�nN�S���-D��!����@3���N���_�ji�cW���sy��*�5u�ٮR���cWv/��.�,�j}
=S)�j5C��^�>
��I�e ��=�g�u9�ӛq�jtz���
����]۪��TM��o���ߧ�I!Ǧ¶m:�,�����"[L����!���{��q�A�v-o�
�3�{�"K�ʼn�
��rIkfٶ�j�2�ƙ���S`�7`�
�k�6j��z���������ޞ��[X�?e5�G&��6�u��ʷ2%ԒR�K��E��*G�\�N��p�o�m F/V
�|��C�0� �.�q_�eenƣ�<5�O���h�'����6�7��ɪn[�SĽ��{�ڔ�jǘ��z�s;���~(ۂ�����`��ܢ1��ƣ`
�_l9��V�a6�%�UQ�Wh���~�P
~\F^Z��HR@��:�ۧ�C��J����
���{ôG�eB��h;~������ۧn�U����
J�\�O�+������n�2� �RҠ)����n���
g}�K�h{���5��+����S×ܛ
�.��1Z�jG�)i�R��ȤI�N�
�4��%��{o����/e�O[����N����ffd��
ĹK?n�nԼM�qX�'܌�nZv�q<���ķ��bFn��ͪa�Q�
`�5� s��,�M_�����լ�����?�������-��@_���{��w���{���Ӻձ�J}G�F[�%�v\�5[Œ��G�k��O��w/���Μ����M9�rj
Ë�%�2���+rd~��+���������C9�U��۳r[���a�Jǭm�|˒LAʨ�SC���q[��X�Mۺou�b�fp�:��t�+Τ���Ļ���o
][��
zt���-*6�7�kv��S7��D·M�MCQ���Xm��;)�n��_h�%]�4ܙn��������R�k�!��]�ڵ�sD��UF�"�`R,
�&�#R_��*[�z*ZqF�Xɻ��
��]�7|۵� �
�w+'p������F�Dە�s=r�.�/���ᐚm3H�ש�y�
��yD"��j�H�C�r�'���:sA�6���5��نѮ^���o1V/��
f;�nF�r3�V���M)e*-��
s����
��D'H݅fӧ�\*���[k<�7u�<��-�]֍�Q�8R
���h�|�p=���W��l�W3s���%Q
%�3�l}@��U-��K��6f�-N���Ͽ��u�|ڴ���m����W�N��[��F�*m�W\���%r��!�
��C�78���:�vB��G�7ŵ.J�թԚ�2�x��)S�T!ř�n<����J��K��ׁ)�R���g����������
�o+n�I*ۊ��݁�,�nd�Ճ�1ݕ���e�E�jA�V��u֙U�=6,48��~$5E6�jo��
���r���w�]��_���-�Ở�c�
ظJ�Z�Y���p�Fޯ�1W.I�V�R���9
)6�P���T�[uo�$}�
�ߔ�}.���s�{�-"��&���D�m+�}����@�U�
~L�m)�M�As�����>�~���9
��W��:�Wp�ܢ件�{�xf��8�
�ٳ�wK��E
ҰWx�V�B�
�\�q���B
Z� 2�wM��b�[l�GS��n��yԚ~��z9Zmያv��oN�2���A��f��nݽjf�>����)�j3���
��!��;��gO��Y��ʹK"�
W�ftڎ�+b��*2ϻ�K>ۢӱe�yԪ���X�ISUm[��z+ugX%0��l������Ϗ���n��vg�!�;t��{�������Bq��P���j�>P�y�v�R�7�Cj]O%+ݲ
: q�iMj�6W�}��3vC�/R��=4�Som���]ŗ=�ю���,
T��F�6U_-\6My�skwMr�&�Q\wj�K���ܩ���yM�ϣUj0��*}R�Zܷ�SdY3
�>��
���� Z��jqj6�Tg���z�p��A�/�M���`�������/��Cm�л,������f��e�E[/�+uk��^�Vs1W$�G��(J����sW2�ٰ��u*��q��*�����Y�.�Wi:����u�r��5�T��),=0��u�R�m�h���o�.twܖ�iY�wr�WHn��t�vE�j8�q��h�f�`Ͻpf�(��R&����>��K�i�%I7$QӖm-2��
�~y�ߗQ-��앑/
�������x[�k8nw.c��㩵k��}]�F��kbJl:{�.
�(˩��n0��Hqv���αp�������7 ��귎�.G�u���p��x��[�N�� `Yq�'�+ru����U<�J|�$�ɯ>�7[��ү�+����>���!
�x�rȫ�oS��o]�OC# ������� d�^���Q]�\�>!ƛG����w^�M��x"��-+%v���dX���-:�M�2UR�%�d>��%l�
���i�oS
���u��6�ls�j�7D�
�P�>X�x�H�z�
�U�k ��(����n�^�����Q���
V�>��5�cV��
�tWj�
S�Ei����J���dzny��
e�j[��lE'
3k�uٌN���n�4��JW)�g��������������������B�
��{4����
����j�� �6��&�]'
�m-(ZM� ��E���z���8�cz>�WZ�6�#���7+��[�,�M�R�-Z�!��4ܓt�Cy�E|��u�m���j
��1ƽv��ƷV��\��;����%>Q� �:��#L�e�(�iV�z�5�����
4��ũ �ۤU�Wx�X�
�^(Ҕ���s��
�լ�B2w-�V��
^��R+�;
˂M\�z�+�Uwr�+RW��Y⺧~ Q*J�c�������YSNS���λ
Ud�8i�n=�v��
�K��낫k\�I�R�רS��Ua�CF�����mϿ5̗P|�u
ZT��ԕ}�>�����oYѲ�1s��fP�+sQ�kX8�Gb��~6r�,s��>^�\,mGL��+7�[�n-�E\�.Fq���ḕc�l���*�Jm��jb�5�
,�m��]����<��EC�H��Tjr\݈�/U1���駚�
�
'���+IC"Ҍl�1J*w�{%ˎOl�c���nZ|��t�/^�1t���
�r��9�ˍ�9V��$m��c �N7RNSi9N-�}�y��n�z�NA;�lV�պs�4�̊e2L���\�O72U�ȏQ-4mD�,e���a�ڒ�v/[� S�����Wa��d�>c�}N��X�f�e�V�l�Ǹ��������J5�
����eˡ$��4��
����%� g�~����N� ��p�4�Y*W��w���W٧
<8v�#���;��q��ԩT�ut,
��m�"#Y�
�D\5V�`\\Lȋ];Lȇ�iS����6�ϝZ���
l�>L�r��uR\��v=������ǘϔ�Dg��=�Ԉ�dFZ+M{�=��������|�,[��;�0�>�RiS�i�4�,�S5�}����y�x�w&�(�E7&���f�ݙ�4�
�U��Օ!
~'��I�d)<�r����bK5)KmD�FfkivK� �l��k��j|�w
��P����r��*J���r�y
t����m
�}
ZG�>]ǽ�u2�K��-fޭ
�\0������8��V�څ�쓬=��V�y�^^ Ih�yKR-�B��#Ըr�=�]��mܻ
Ӿ��'*U��mk��oy�
rTqT������_i�,/8Q�^���<ݤ|4ԻO�(�܄"�'5N��~��#��m.(��Ҿ���
2�i6Uev��&�I�*�
�<�������}��҄��$eN�tÛz���yWJ�ub��W��^�i�BW.܅���W��ڮ�g�]i���rO6�Ve�90�s�gv�.��+s��V�aޔ�[p�?�3q�*Fu�tUo*���e�L�\KM'EG�*ZcA�FfG5J
�5jj=MJ3�OK:k˝'�NM��B7m�3�uFҕ����\�-Ywg%�PRq�M�IyZ�GY9��|��μ�v��n���5cW�ݷ�a^��+X֥vnݘ\v��7
�m��>�Fg�zv�"-;�E�w֝}��1|R�j����N
��
�����7�g��#֟�*��G
� �Q�Q���|��#/��bo�]���p��$��>_�Un9����������г���Ub�n�9�׃E�rQ�B�U-���^v��D�����m���Vh'<R[fd��
��H
�T�]*�~���}�
3j;��nv�jc7s���-�rӳ�� Y�8����[n[1�
�pJ�x�
��kX[J��k9�M�n���!_�N�ю6�x�:���i��Z˦U��
����|߉�^Ԛ��݃�h
Y�x�k�
&���U���^
�
bwKk���.[j��E��+P(�˞=�
9���j�@���snCv��7���%����c�_7=���x
�ǁ�< ��l
�{t������'酚�+��1F��l���:���ݻI����Lr�uǶkL�-�L(K�0L<�G]}��j�v{���aL�L���՜w�g��*���1"�N
�V�pj�"��
�R��$�s��L�Gl�T�H����I�-�I��.�x�u+��Q�/�J��l�~ȇ�jvQD���r�ll��W�mR
��[�)S�!�%9�aq�Y-���x~���F��i�]�կ�7c}��yeW�R�
E�^��L��i؎���y�K����☘��ꖙ�y�
��j3 aϳӹ��
�}�z��{�m1�졳�SWچ
�ZXꕆ.�Z��_�ZW]��s��u������z���J -&�f��K���-��q <����mV��/���,���bˇ|m��~a{���wݾF���^�_7��2�c�e�Lv��]��m�#�*���ǟ
� �g�P��
������������x���E���3�W#�ۊ����
�6����ʮ�6�r�}���
VH��&Z�
+e
�W�ܨUmE�bґ:
1�m�v
4F"
�8tK���{�f������M���ǒ1^ٷ#o�-�Wjé[�[��[.�ۻݖ�T�\
d�Ȉ�2O��$Fyl�.�����ɻK�f�:��'-u�wt0�����1����PUM�?b{�T���fڮSbV#�TR�f2��9
O�����Y{^[�꩸}�bM��϶|�4��=�P�I���wxc��B��b٢7�ɭ&
J�R�����,
B�#��W7�bm㩮^�N���qf
����o`
CL��3}�����Q���.E�@��)����M�D�KK�U6��
d
���2���]r �!����s���������x�&*��� 4�|�����S��<�7��3��`e�հ�����⮣�5<��-�^{\�7�?�������㟘G�o��O+��q��t�|�?c�b��cG��q��M罪��?�u�w{um�)��`�|̴*y$���WnL��)�(���Pb�c��aJnL�\�(
Y�9;C��c� ��#����~���mt��L�P��}�s\�y\jݪ�h�-�
�s�Uit�\io=D�M[������M4%�¶�u������
�(H�mY��n�yu{�m=5�n�&$��+����!��!�
�JmdF��m��fR�oJ�����������@��-��n�#�pe����:�r�Mņ�VN�r-} �]r
%�G!q
֡
0,m��Ћ*F�g�g�^�9�i�
݅�{�;��-����F�*���ɰp�v�%�o������ʅ
%A�%�_;*&�b��'����-c_+ĘåmJ�;;iɽ��{r��4�kO�O���tI��N��+�J�=
��JC��Cj3p����F�C7
�Eù��{2bΧ��3��oò�YlF��� �*߭˹ox��b\��:�2��T�D��,��'���I���,���-��T�>�1&����>wX�
�B(p��m�;��1�f�pn��l��p�֓%S��kid��� �kt(�U
��+��x�ul����o'/�ڕ�e��N
�r=^�pZ��Z�:��Pnj�8���Hf�"48��i�jY[��
��N�[��yZٻ�+��=��������
ø:��3��
?^��ܷ^��S�r#�Y�K[UF?CuhC b
]�G��M')mڏ��s��N��rܗI�]ljq6V��B�. W,�
����UK"YX��5�{�c����
�>�Iqā> �T:n!,5l��
��2���Vz�C�l|+I[�*SrjnS�6٨�y+x��,��@>�П��.��g�����+��!��rn��9>N|�W>�O�Z�T_u�t��
����Y"���"�v�7�|�s�fި;P���cl�m�� E�ùN�,{�'��f�N�T���%U&�LfH�8�~1��v�>���I�l
}统u
��6P˗���c�(�W���V~H�^��bM�U.o*�oO�F�0N������:_���:6S��mr_.�b��+����|ݶ��YY
غ��F,���m�w����j��v�>��f*>QM�뭱 �Sd:`N�{��l�/⎱;����n�-��z~"�G��ze�
퇎
��J5S K�G9�!�Gn�
;��N��1� �ݎ
�h6��m�|S�?���ɂ�5�'�����W
��OÞ��� ��7�|� 7��^a�o @m��x�Gm�i�^jϽ>01Mf����0լ�D��������3-2T��.
�VXR"���ɥ���V�
Kl
���J
���O7|�����u��?�b��vа�;�6.��
�������
eߓ|[1b�mR�r,�e�Rz�`z
��6��-ͨ�ku��F�ː�
d��P�hY�
gZUj}n�v�X�;z=�g�V�ե��������Tv_J��� }�\��1�n�7��w2�J�?ޘ�γc�\E�
1A�ޑ��z��q�;�\��r]]
��\�Y�&[��n�s��Nei�������������������������\u������UR�
je*�Qk�2�C�S�l*��x��Jz-xٶ��l�m+����|�Uj�U��ؓ`La�d�q�iĩ�!G�d\�W��~f���z��;T�n�
�*�P��d��RM&���T���4`չSW���q5�k�훶�(N"Ӎ%�
V�]��֦�����w�b�.����n�U��O�!�u*����J�������&�Oӕ�2e|��Z=e�V��쫚΅g#+�/�R���W
:����طn�b��i*Wy�o)
p�{�:E�T�KؚR��(�R��Y���+��r�웓r��(��I�F�)
V�m�ȵN�B��:h��
Q 1�ғ�|u�8E]�{,'�$��-�TR��[����j4���9�l����*3"I��鯴z�hd�>���Q�+�\��B�kN�F���=�.�$�ZR�4�N�wհ�(I�pN���i.(�G��i33#33�e��<�R���ʴዣK
_c�OP�'/n�iQ�������+
e���j�V�nB��*���$�lWj�����FX�D��a�㶲ԛ���#�
�A�k囱��g�b�/�Z�v� �F�k�c�t�L���r�7�zVu늞5�Lk��UJ���S�%�L�Lg�Kt�\f�ݔ�{�� ��Tn
=B�p��/�[uZm,��FFj���3#ׁ�� 6�����������;f��w[쬞R��a
y����֩nY<���agJ~�<|g��ء�\�t�Wj��)�=u�[iMϷ�G|���A��)��3Dz�
�I�ԭ;51�0|�h� �%�{�����,������䮹h���Km$FXK*�Nd�Wr�u���d�[r{x�n���k$v
2ı
h�+J1�T���Q�[#JQl[tRO]L�H�K�����ٮ�� NӍnF�����֞�������E����m�'����MI��L���B"ԋ��%�dBŋ���+p����̿�_1���7��jz�T��~4��p����c �Vo\ƹ��b9R�q���-'�1j;����8ܗ)hE�%�DZ��K�S<璸�Bu��*%�*�Yw5ڻ�9��ۣ��^�z4��U;
Ñk��\�U(���o~��G�?�VU�Ď:?P?���� ����_�F_�K��ߤ���~ᓾI��
|�p��r.�����������������������������������������������������������������������������������������
Ok�\����� ��S�k��l�R�hҪ�����z{�P��
.}�SktZ�7���U�Q�4ڌIM8̈��e��a�ӊJ�Z�%FFZ�u,KZ����vl��n��廐S�N��FI�V�tuN�i�?CM�5]+P��h���,{��j����N
JS�R�����$�I�S^��t��S�U�V�r�OR��Y�u.9W��y��
�P6 ��[K�i��u ���m�! X|�]Y79���ӄ�)\ģ��)pbڳ��r�%*�&ꑶ_- H*dzk���)�1�
V3��')UA�Ϲ���ٶW���R��xe'պn۫�h7
�A�R�9
�E�A�J��e�G��L����ms!�%D|
�A
5]/Q�3e��b��̄�v�nV���n��%���z�a��\�m
���kZnv�(��[�e���m�qrI�ҕi����j|��""><����hjJ�שvvǕ��|P��ޟs�}���V�~2��&�Z���?�+2�N&Z
�4�w��@�)4���i��S���ڪ�_�>/�J�N9H�i�ۏ��
uf�8�'�I
t�[��Ȳ�R.�hZ�$ȋ_Y
�~�U�<���UU��O�*�6�b)O��vz�ڜ�j\R��̋�.$FsQ����u��Ҋj�^נ䈈��y��<��z�Z��I�uP[}���Qm��
�=����C�?���z�N(Exqu/��kn
���S�-FzK�Z�zOס
��ӽj��J\)F��3�b���!��r�5�����ٝ��|;6� ��o=�
��-3*λ�
��]�αb���\a�b��q�R����i-�w�⦪�~b�8Kp��o�)��Z�=>)�ғ"5/�GTZ���L�E��-��輵�f7ݘ۹~�+&��+���w/7G�F�I:l<�u���D�ͳ�nwԮ�;�v��de|�
��Q�����QQ��#=Ε���)ǿ��]�ff�(�S>�33�fg�.N~��۲��\2|*��c�n���er�m�����n�n����������M�����+�Fq�"�ѪIz%��j������� ��=���
���YW�8��@����~�gc��/�~��?���N�'?�)��«qȸ�����s���➟n�=���k"
���Xm֮�Vre�M�h2[�uݖ] �*�Fܖ��N��)M��Ȑ`f0 �g�,C�9�����̑o;���d��dudJ=�In��13���:ݒv��v��dMUE
JL��p�^,6t-@͐��9'{���7m{�-��3,�����>�h��nF;�Ѱ�
����M�)�->�>+Ěz!R*
:�����`�e�
�--�m�7nB��\u{ b����
U��>�[8�֪]��6��^ߤL�ʦ�\DF�N�
o�$��$�dͶl�gn�o8Or��sQ�\�l̯hRo8t�u�N�o�+��
�C��Txu��!2[�>ct����F������������������������������������������������������������������������pe����ޓ��ƻ�ֶR�"3Qr���������Q�u�Oѳgw��Qr����;S�~��)6H��
���hZw��/Gg�VT�mU�f����_�yt�7%$�];��zLW�F̰��xy2Ʉu�!MC�m�š_0[W6�j�f#��a�-KLi��+3Q7��c^q�g%s�<�1aY��IQeZ�f+}>�;S���6���L��0]Y��u����_�h��9��<���ƅ�pm��i�M$��AVv�Ś,�*�#t�2�.8���Y�����������)��-��Zh��
s���hü�97/#Oro�"���u�^/uF�g�Wɺ�,p:��������6a,^����x��%$�Yve���^�3PƗ���M���nT�P&y���S}��OJ
'��덫MH��^��:r��XԴ�Jۋ���/��r��I;�S��*�,+yz1h��v)�Q��w�^�ڍ�J2�oL�����q(��\�fD� �j:��^�T���%v��O��a��d�ɂ�������n�S�}���Z�O��)N����*λd��aȜkG_P�I��E���O�}��нa(^iQX᯦���-��7^)%�g
�'SJx�(.S�9�zV�ɴ�Z�{E� �))ۅ����i/s����7
� VIV��-��|sj0�*UBTHIqRf>�FP�$�Kq�N0� �R�̻8j\Gc��C����}I���U���z�\i�� 6����
F��)�Q��{Gҧ�3q������S��z�����Kj-A�z
V�ЛS�-z y:��8�*mNk�|D�鿓N��D2u+�0�Y��ŝ7�k���q�
m�·?8�I�b�]�����u���>�˗�^_�>(]��v
��Ӌ�zv�+�ݩ){v�ZrJ����2R�Q�몋�C���$z�
���[�,�p�p,����� �8mڊ���b�R�]�Il .f~��d����/��ݓs���㓓�mͶ�{�m��g����jQ�wn�=O�i�c�9ܚ�m4�Q�����/6ݨ[�������T�Ƨ?n�Զ���oytf���{�@�������AzT{ e{�[O�'Z�R�����������Z�����
t~�AG�D?s3���Չ�Iw� ���'|����~�U��\�����
w~�di�:Kޱ)U/sU%n jѩ�&�G�S����P�^ǝ�d).�.!�^U
�`
1wX[��aԇ�S�����x�o�FV�6����_��扐)T
�2M�fd=�ۖͭi��Z���7K��K
Bi��9%�7�@�<3�<ճ���Ի��U���,}���,a}��F�Rq�ɛr
�i�@�O��N���JvK�
K�L�N�� M, ʖv��0n��-�]Dw��lI�-�X�6ܶ$���Jʴ���h�5�O+m��O�I��+R�a瞠�\�� MG7�Bف�j��Y���o1��#�͖��0�V`��Ѱ��2M?
c��8>-C�rt��*���J�k��I�G�S:��e�#�hP��Kx[�鱼>�{��5�m�;w��c�ն��&�>�����j�-M��֥�^�َ�)������
�����6y�Ȝ����l_��������w{��-ō��̱�r> �U=�]���i�w�3��)�r�*]:�K]6��B�d���CT��Z����|���>���gf}�
��L�W��}���[��$'Y5
��&�c�
�-�j���.�z�6����R�� ���
6������7�MԷ�FM���n�Ìw�I��7�w5�E�}o��+��K
�ֵy����4���܌ȥW�"CO��<�H���?�&zp�]�o�1�@Z���������������������������������������������������������������������������hIH��DZ� n�p�(�*J\+���
59l��m��gY#R�JQkǷ����T�^�I&�.$��M�M��-����NyR\9��=
���wj\=B� 4�d�
��SQ�eU�۫?:�G��X\Z�6�S��
�>
y������R[q�5Ӱ��͙��f[v���"�_�#q{�M V6���܍�3"���u�9BK�(4��1���ӯ�qˇc$�{�ߝC�i6�I�(��O�m���θz�Ҝ5k�^:>Jzw�.�>��qV8��{vU[ڶ��E�
�m������|DžBz�]��.���K�H�j�I]��x��;��<�feN��'�iTj�M= ЈuL�.�.�u����
lG���K��KM��e����J�߾����
��]J��o)�#-[���2B���Q_��)��F?:ǖ��aݍ�YɻWE��ot��*5���
�<�br!+vuEj�Oڏ���5�*>�M�ɗ�{m�,�qZXr��忇2u^�R�O��2��Z}�Z��ێ�S[2�Je���n!*N�Dc�r�B�U��ً�4��<����Ǽ��MҲ���
s��1Z��w��5�7� �c3&Ė��ڻ�z��mP��*����FuJG1���-�����d�N:|�OU}ҵ�g�i2t~F�^^��Z.����Vx����jv�ŧ�n��N����Nh���<��:��]��^~NN��+�g�e^�����g.����SԔG�Fe߯�'[v�n'(ScJ�]�kܗ����7eJOl����
R�rfziݮ������q�̋��S"�\*��U<*�W�]��k��$�FջV���
�}?�
����������7�g��#֟�*��G
� �Q�Q���|��#/��bo�]���p��$��>_�Un9�����;��l
S
�Vv�Q�U�%O��LU{ο��m������U6����b�Z�1MTx�%�!�֙Q7�,
J�=!3
;�����Q,���ڌ;�6ͱ�݅q^��&ߔ·n
�#W�b���wӖ�X���.�Ht�G)N��&�d̵z��p�I�,�n
�cu
ޖU�j+V��X����U�p[w]�N��
�o�.J�6���Z���8�Ts�&��u���tx�ln;�~�H��P�H�S��/�xw
`�G
\��ʡ¿rj�
�Z^v�t"[L:�S��D�\����h�����0��s�U�wR
��,}�[���x^��X�,R2
�Vn<
����]�2�Y��D���r�[��S��RKs8t�X��b̷�G��?Ps
�T�v
�3��be,��z��V�����z����
D[�/I�.�K�OEQr�m'�$�
��7����|[���J��>�r
�S`5�յw���T#\�w1FT�z\Ԛ���� ��&�"ׅ�hS��H�r���D���\'����r�]����~/�>��p���;����:�P�����i��u�
u:�"9ő=t��TaS�7V�2��r�ӷk�����7m�b[�^W��m�Pp�*��[y.Þ��6f]���ci�z�JCgR���R��@�UVl�큝���.W���J�
���P�1��N�{/
�\whZ�
ػϧ�ӱ���E�7|�E�
֫Sί
�.x�-��Y���&����������������������������������������������������������������������������pi%v�
��'�'�-�x�6�r�
'�Ws*�6=���D�� ww���Uu�]�=C�?�MK��
��[�yrtܒG$�!WG�qJ*�%S�A�z���
�ED[��^)/t�ė/g��=�#���Omd����.|^
�n�/�s��l�����g��
�DZ������qem��qowݮ����RzU�ܜ��=�ڽ��-o�/�Iۖ�;q��V���ʘgPp���|m��m;6zGl�9.8pwWg�sJ2qP�b��e}}���U��p����Njٯ}7T���M�QKrؽt��Ex%�v��� w�����߾8%� |j
�;~���|}�pK����]��ơ�/��� w�����߾8%� |j
�;~���|}�pK����]��ơ�/��� w��&������~��e_�H�� 8�P���L7:������%�ʭ5�Kw�&��������U2
�v�w��R��
������������������������������������������������������������������������������������������������������_��������������+�r��m'��������}��C�7�#���� �rW��o��O����&���H�����o�G����?���������� �M������������$���U���R7{�FU�]�u� ;#���
!��W�k���`�|���W����>���潇
9�V�n)�6�)*���ҹ{��%�q�V4����q>�W1vi�#�T�"Qk��&G�wx��cJ�������������������������������������������������������������������������������������������������������B�J-
Ϸ^�����ˁ�xk�U}�������ԣ/�3�.��;]J=��<�*)�c��S��)����ROK
���9H=,r�
zX� ���@)�c��S��)����D���a�^��Խ�Q�
gxJI=��w�֣�g�f*T�R�j��������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������
- 1,431 Views
- 11 Download
- 0 Crossref
- 0 Scopus
Abstract
Purpose
In Lisfranc joint injury, the traditional treatment has been open reduction and internal fixation with a transarticular screw. Despite this, additional complications, such as damage to the articular surface and breakage of the screw, have been reported. Therefore, this study compared the clinical and radiological outcomes of dorsal bridge plating with those of transarticular screws and combination treatment in Lisfranc joint injury.
Materials and Methods
Among the 43 patients who underwent surgical treatment due to Lisfranc joint injury from June 2015 to March 2021, 40 cases followed for more than six months after surgery were analyzed, excluding three patients: one lost to follow-up, one had to amputate, and one expired. The radiological parameters were measured using the Wilppula classification in the last follow-up. The clinical outcomes were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) midfoot score.
Results
The AOFAS midfoot score, according to the surgical method, was significantly higher in the dorsal bridge plating (p=0.003). The radiological outcomes showed significantly better anatomical reduction when dorsal bridge plating was used (p=0.040). According to the Wilppula classification, the AOFAS midfoot score improved as the quality of anatomical reduction improved (p=0.018). Finally, the AOFAS midfoot score decreased as the number of column fixations increased (p=0.002). There were two complications: screw breakage in dorsal bridge plating and superficial skin necrosis in the combination treatment. Skin defects caused by necrosis improved after negative pressure wound therapy and split-thickness skin graft.
Conclusion
In treating Lisfranc joint injuries, open reduction and internal fixation by dorsal bridge plating can be an appropriate treatment option. Nevertheless, studies, such as long-term follow-up research, on complications, such as osteoarthritis, will be needed.
J Korean Fract Soc. 2023 Jan;36(1):17-24. Korean.
Published online Jan 18, 2023.
https://doi.org/10.12671/jkfs.2023.36.1.17
Published online Jan 18, 2023.
https://doi.org/10.12671/jkfs.2023.36.1.17
Copyright © 2023 The Korean Fracture Society.
Original Article
수술 방법에 따른 리스프랑 관절 손상의 결과 비교: 배부 가교 금속판, 관절 관통 나사 및 혼합 고정법

Comparison of Surgical Outcomes for Lisfranc Joint Injuries: Dorsal Bridge Plating versus Transarticular Screw versus Combination
초록
목적
리스프랑 관절 손상 시 관혈적 정복술 및 관절 관통 나사를 이용한 고정법이 흔한 방법으로 여겨졌으나, 관절면의 손상 등의 추가적인 합병증이 발생한다. 이에 본 연구는 리스프랑 관절 손상 시 배부 가교 금속판, 관절 관통 나사및 혼합 고정법에서의 임상적, 방사선학적 결과를 비교하고자 하였다.
대상 및 방법
2015년 6월부터 2021년 3월까지 본원에서 리스프랑 관절 손상으로 수술 후 6개월 이상 추시가 가능하였던 43예의 환자 중, 추시가 되지 않은 1예와 합병증으로 절단술을 시행한 1예, 사망한 1예를 제외한 40예를 대상으로 후향적으로 진행하였다. 최종 추시 시 Wilppula 분류로 정복도를 평가하였고, AOFAS midfoot score를 평가하였다.
결과
배부 가교 금속판 고정 시 AOFAS midfoot score와 정복도가 가장 높았다. 그리고 정복도가 좋을수록, 열 고정 개수가 적을수록 AOFAS midfoot score는 높았다. 합병증으로는 배부 가교 금속판을 이용한 군에서 고정 나사의 파손 1예, 혼합 고정법을 이용한 군에서 창상부 괴사로 피부 결손이 발생하였고, 음압 폐쇄 드레싱 및 피부이식술 후 호전된 1예가 있었다.
결론
리스프랑 관절 손상 환자의 수술 시 배부 가교 금속판을 이용한 고정은 리스프랑 관절 손상 시 시행할 만한 적절한 술식이다.
Abstract
Purpose
In Lisfranc joint injury, the traditional treatment has been open reduction and internal fixation with a transarticular screw. Despite this, additional complications, such as damage to the articular surface and breakage of the screw, have been reported. Therefore, this study compared the clinical and radiological outcomes of dorsal bridge plating with those of transarticular screws and combination treatment in Lisfranc joint injury.
Materials and Methods
Among the 43 patients who underwent surgical treatment due to Lisfranc joint injury from June 2015 to March 2021, 40 cases followed for more than six months after surgery were analyzed, excluding three patients: one lost to follow-up, one had to amputate, and one expired. The radiological parameters were measured using the Wilppula classification in the last follow-up. The clinical outcomes were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) midfoot score.
Results
The AOFAS midfoot score, according to the surgical method, was significantly higher in the dorsal bridge plating (p=0.003). The radiological outcomes showed significantly better anatomical reduction when dorsal bridge plating was used (p=0.040). According to the Wilppula classification, the AOFAS midfoot score improved as the quality of anatomical reduction improved (p=0.018). Finally, the AOFAS midfoot score decreased as the number of column fixations increased (p=0.002). There were two complications: screw breakage in dorsal bridge plating and superficial skin necrosis in the combination treatment. Skin defects caused by necrosis improved after negative pressure wound therapy and split-thickness skin graft.
Conclusion
In treating Lisfranc joint injuries, open reduction and internal fixation by dorsal bridge plating can be an appropriate treatment option. Nevertheless, studies, such as long-term follow-up research, on complications, such as osteoarthritis, will be needed.
Keywords
Lisfranc joint injury, Tarsometatarsal joint injury, Surgery
리스프랑 관절 손상, 족근중족관절 손상, 수술
서론
리스프랑 관절의 손상은 족근중족관절(tarsometatarsal joint)의 손상을 포함하며 관절염, 변형, 인대 불안정성 및 영구적 장해를 유발할 수 있는 심각한 부상으로 간주된다.1,2) 연간 55,000명당 약 1명의 비율로 발생하며, 전체 골절의 약 0.2%를 차지한다는 보고가 있다.3,4,5,6) 그러나 리스프랑 관절 손상에 대한 초기 진단 오진율이 1/3 이상까지 보고되고 있기 때문에 실제 발생률이 과소평가될 수 있다.7)
발생 원인으로는 저에너지 스포츠 손상에서부터 고에너지의 외상 손상까지 다양하며,6,8) 이로 인해 단순한 인대 손상부터 족근골 탈구까지 함께 나타날 수 있다. 따라서 리스프랑 관절의 손상 시 적절한 치료가 중요하며, 일반적으로 해부학적 정복과 수술을 통한 리스프랑 관절의 견고한 고정이 필요하다. 비관혈적 정복 및 고정법은 주변 연부조직의 관절면 사이를 막아 정복이 어려워 이상적인 치료로 보이지 않는다.9)
리스프랑 관절의 손상 시 성공적인 치료법으로는 관절면의 충분한 고정과 안정이 필요하다. 그렇기 때문에 관혈적 정복 및 내고정술은 리스프랑 관절 손상의 치료에서 필수적이다.10,11) 리스프랑 관절의 손상 시 관혈적 정복술 및 관절 관통 나사를 이용한 고정법이 흔한 방법으로 여겨졌으나,12) 관절면의 손상 및 고정 나사 파손 등의 추가적인 합병증이 보고되고 있다. 이러한 손상과 합병증을 피하고자 배부 가교 금속판을 이용한 연구들이 진행되고 있다.13)
본 연구에서는 리스프랑 관절 손상 시 배부 가교 금속판, 관절 관통 나사, 그리고 두 가지 방법을 혼합한 고정법에서의 임상적, 방사선학적 결과를 비교하고자 하였다.
대상 및 방법
1. 연구 대상 선정 및 분류
2015년 6월부터 2021년 3월까지 조선대학교병원에서 리스프랑 관절 손상으로 수술 받은 후 6개월 이상 추시가 가능하였던 43예의 환자 중, 추시가 되지 않은 1예와 합병증으로 절단술을 시행한 1예, 사망한 1예를 제외한 40예를 대상으로 후향적으로 진행하였다.
술 전 모든 환자들은 컴퓨터 단층촬영을 시행하였다. 리스프랑 관절 손상은 Myerson 분류14)로 분류하였고, 수술법으로는 배부 가교 금속판 고정술(16예, 40%), 관절 관통 나사 고정술(16예, 40%), 그리고 배부 가교 금속판과 관절 관통 나사 혼합 고정술(8예, 20%)을 적용하여 총 세 그룹으로 분류하였다(Fig. 1).
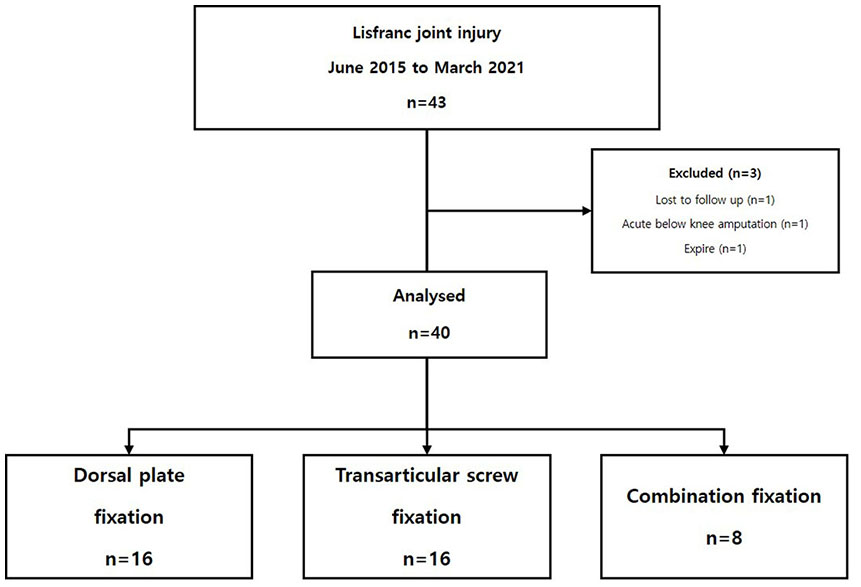
Fig. 1
Consort diagram of patients.
본 연구는 조선대학교병원의 기관생명윤리 위원회(Institutional Review Board, IRB)의 승인을 받아 시행하였으며(IRB No. 2021-03-011), 후향적 의무기록 연구로 환자 서면동의서는 IRB에 의해 면제 받았다.
2. 수술 방법 및 수술 후 관리
수술은 전 예에서 한 명의 술자에 의해 시행되었으며, 수술 방법의 선정은 무작위로 진행하였다. 리스프랑 관절 고정 시 족근중족관절을 고정하는 방법에 따라 세 그룹으로 구분하여 관절 관통 나사는 유관 나사를 사용하였으며, 배부 가교 금속판은 2.4 mm 또는 2.7 mm 잠김 압박 금속판(locking compression plate)과 2.7 mm 또는 3.5 mm 피질골 나사를 사용하였다(Fig. 2).
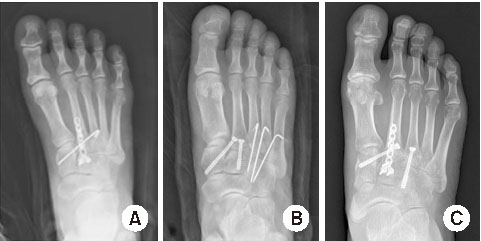
Fig. 2
Three groups according to the type of surgery performed. (A) Dorsal plate fixation. (B) Transarticular screw fixation. (C) Combination fixation.
관절 관통 나사를 이용한 수술 시 최소한의 절개를 통해 고정하였다. 배부 가교 금속판 및 두 가지 방법의 조합을 이용한 수술 시에는 가장 보편적인 중족부의 배부 접근법을 이용하였다. 이는 두 번째와 세 번째 중족지의 중간으로 절개하며, 첫 번째, 두 번째, 세 번째 열을 포함하여 중앙 및 내측 부위로 접근이 가능하다. 중족지 관절을 고정하는 몇몇 금속판은 첫 번째 열에서는 내측 설상골과 제1중족골, 두 번째 열에서는 중간 설상골과 제2중족골, 세 번째 열에서는 외측 설상골과 제3중족골을 이어준다. 외측 부위의 고정이 필요하다면, 이는 배부 외측 접근법을 통해 시행하였다. 이때 배부 신경, 혈관 구조물들의 손상을 피하기 위해 주의하였다. 해부학적 정복은 직접 골절 부위를 노출한 상태에서 시행하였고, 정복 여부를 수술 중 실시간 방사선 영상장치를 통해 확인하였다.
모든 환자는 수술 후 6주 동안 비체중부하를 시행하였으며, 6주부터 3개월까지 CAM walker를 통한 부분 체중부하, 3-6개월 동안은 족부 아치를 지지하며 전 체중부하를 허용하였다.
3. 방사선학적 평가
방사선학적 평가는 족부 전후방, 측면, 비스듬 사진을 촬영하였다. 방사선학적 지표로 Wilppula 분류15)를 이용하여 최종 추시 시에 체중부하 상태에서 족부 전후방, 측면, 비스 듬 사진을 촬영하였고, 족부 전후방 사진을 이용하여 첫 번째 및 두 번째 중족골 기저부 간의 거리를 구하여 좋음(<5 mm), 양호(5-10 mm), 나쁨(>10 mm)으로 나누어 비교하였다(Fig. 3). 방사선학적 지표의 측정은 2명의 정형외과의에 의해 측정되었고, 이후 측정자 간 신뢰도는 ICC (intraclass correlation coefficient)를 이용하여 평가하였다.
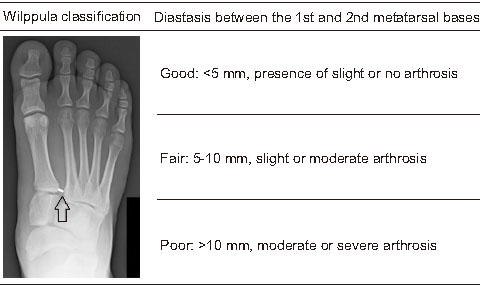
Fig. 3
Wilppula classification of anatomical reduction. Arrow: diastasis between the 1st and 2nd metatarsal base.
4. 임상적 평가
환자의 임상적 평가에 있어 최종 추시 시에 American Orthopaedic Foot and Ankle Society (AOFAS) midfoot score16)를 이용하였다. AOFAS midfoot score는 크게 3가지 항목으로 환자가 호소하는 통증, 기능적 측면 및 정렬 상태를 평가하고 있으며, 기능적 측면으로는 활동 능력, 보행 거리, 보조기 착용 여부, 걸음걸이 상태로 세부적으로 나누어 평가하고 있다.17) 총점을 합산하여 우수(90점), 양호(75-89점), 보통(50-74점), 불량(<49점)으로 비교하였다. 수술 후 연부조직 감염, 인공 삽입물 부러짐, 불유합 등의 합병증 발생 여부에 대해 확인하였다.
5. 통계 분석
환자군의 성별, 나이 등 일반적 특성과 기초 자료에 대해서는 기술통계 기법을 이용하여 요약하였다. 수술 방법에 따른 AOFAS midfoot score, 정복도 차이를 파악하기 위해 Kruskal–Wallis 비모수검정 및 χ2 검정을 실시하였다. 또한, 하위집단 분석을 위해 골절 형태, 정복도, 열 고정 개수에 따른 AOFAS midfoot score를 비교하기 위해 Kruskal–Wallis 비모수검정을 실시하였다. 모든 통계 분석은 윈도우용 IBM SPSS (ver.26.0; IBM, Armonk, NY, USA) 프로그램을 이용하였다. 통계적 유의수준은 p값이 0.05 미만인 경우로 하였다.
결과
1. 연구 대상
평균 연령은 42.5세(범위 18-69세)였고, 남자는 30예(75.0%), 여자는 10예(25.0%)였다. 평균 추시 기간은 7.5개월(범위 6-11개월)이었다(Table 1).
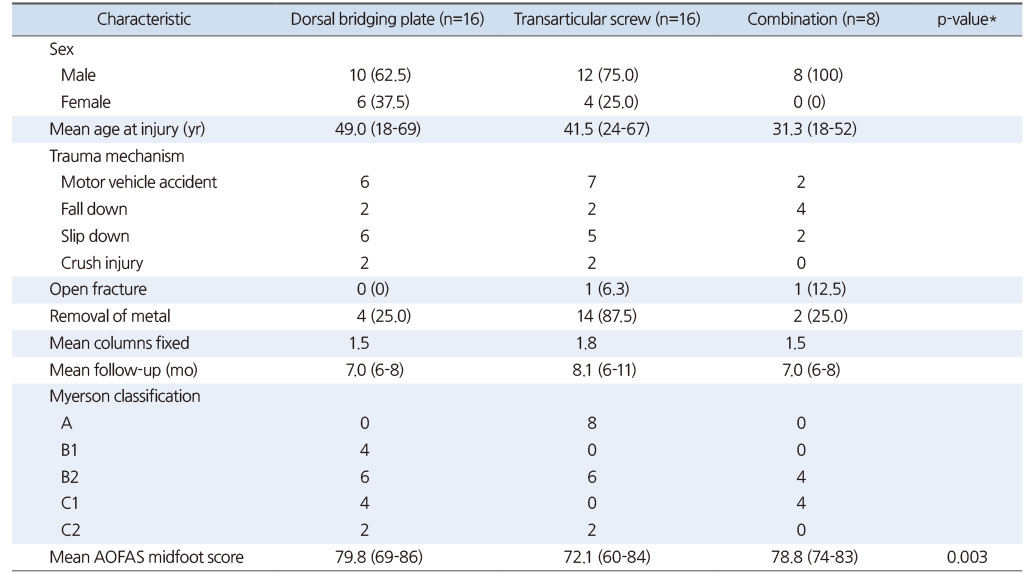
Table 1
Patient and Trauma Characteristics and Functional Outcome
2. 수상기전 및 동반 손상
수상원인으로는 미끄러짐 13예, 추락 8예, 교통사고 15예, 으깸 손상(crushing injury) 4예였으며, 이 중 개방성 골절은 2예였다(Table 1). 16예에서 동반 손상을 보였으며, 경골 및 비골 골절이 각각 8예로 가장 많았고, 안면부 골절 4예, 흉부 골절 2예, 전완부 골절 2예, 수근부 골절 2예가 있었다.
3. 골절의 분류
리스프랑 손상의 분류에 있어 B2형이 16예(40.0%)로 가장 많았고, 다음으로 A형과 C1형이 각각 8예(20.0%)로 많았다. B1형과 C2형이 각각 4예(10.0%)로 뒤를 이었다(Table 1).
4. 치료
모든 예에서 내원 후 평균 6.8일(범위 0-32일) 이내 수술적 처치를 시행하였으며, 1예(2.5%)에서 내원 당일 응급 수술로 골절에 대해 고정술을 시행하였다. 배부 가교 금속판을 이용하여 고정한 경우 평균 6.8일이 소요되었으며, 관절 관통 나사를 통해 고정한 경우 평균 7일이 소요되었다. 그리고 두 가지 방법 모두를 이용하여 고정한 경우 평균 6.5일이 소요되었다.
5. 방사선학적 결과
해부학적 정복도는 최종 추시 시 방사선 사진을 평가하여 Wilppula 분류를 적용하였다. 수술 후 첫 번째와 두 번째 중족골 기저부 간의 거리는 배부 가교 금속판만을 이용하여 고정한 경우 평균 5.61 mm, 관절 관통 나사로 고정한 경우 평균 8.04 mm, 두 가지 방법 모두를 이용하여 고정한 경우 평균 5.68 mm로 측정되었으며, 유의한 상관관계가 나왔다(p<0.001). 배부 가교 금속판만을 이용하여 고정한 경우 6명(37.5%)은 좋음(<5 mm), 10명(62.5%)은 양호(5-10 mm)한 결과가 나왔고, 관절 관통 나사를 통해 고정한 경우 1명(6.3%)은 좋음, 15명(93.8%)은 양호했으며, 마지막으로 두 가지 방법을 혼합한 고정의 경우 4명(50.0%)은 좋음, 4명(50.0%)은 양호한 결과가 나타났다(Table 2). 해부학적 정복도는 통계 분석 결과 배부 가교 금속판을 이용하여 고정한 경우 좋은 결과가 나타났다(p=0.040, Pearson χ2 검정).
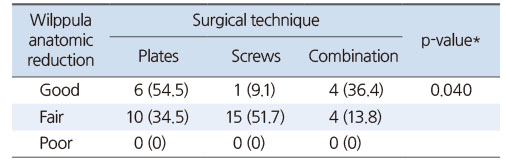
Table 2
Wilppula Anatomical Reduction Stratified by Type of Surgery
6. 임상적 결과
임상적인 평가를 위해 시행한 AOFAS midfoot score는 배부 가교 금속판 고정 시 79.8점(범위 69-86점), 관절 관통 나사 고정 시 72.1점(범위 60-84점), 두 가지 방법을 혼합하여 고정 시 78.8점(범위 74-83점)이었다. 총 28명(70.0%)에서 양호(AOFAS midfoot score 75-89점), 12명(30.0%)은 보통(AOFAS midfoot score 50-74점)으로 나타났다. 수술 방법에 따른 AOFAS midfoot score는 배부 가교 금속판만을 이용한 군에서 유의하게 가장 높았다(p=0.003) (Table 1).
Myerson 및 Wilppula 분류 그리고 열 고정 개수에 따른 AOFAS midfoot score를 평가했고, Myerson 분류 C2형에서 A형, B1형, B2형, C1형보다 AOFAS midfoot score가 가장 낮았다(p=0.003). Wilppula 분류에서는 정복도가 양호할수록 AOFAS midfoot score는 유의하게 높게 나타났다(p=0.018). 마지막으로 열 고정 개수가 많아질수록 유의하게 AOFAS midfoot score 점수는 낮았다(p=0.002) (Table 3).
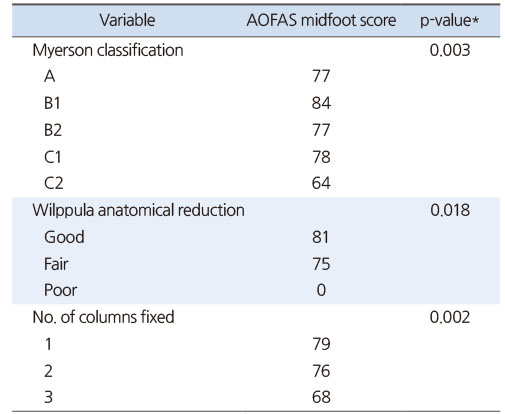
Table 3
Myerson Classification, Wilppula Anatomical Reduction, and Columns Fixed, Stratified by Functional Outcome Measures
합병증으로는 총 2예로 배부 가교 금속판을 이용한 군에서 고정 나사의 파손으로 제거한 1예, 두 가지 방법의 혼합법을 이용한 군에서 창상부 괴사로 인한 피부 결손이 발생하였고, 음압 폐쇄 드레싱(negative pressure wound therapy) 및 피부이식술 후 호전된 1예가 있었다.
고찰
현재, 리스프랑 관절 손상 시 배부 가교 금속판 또는 관절 관통 나사, 그리고 두 가지 방법을 모두 이용하여 고정 후 방사선학적 및 기능적 결과를 비교하는 연구는 거의 없으며, 이에 대한 표준치료법은 정해져 있지 않다.18) 가장 좋은 고정 방법에 대한 논쟁은 계속되고 있지만, 리스프랑 관절 손상 시 해부학적 정복은 좋은 결과를 얻기 위한 조건이라는 데에는 의견이 일치한다.19) 최근 Lau 등20)의 후향적 연구에서 골관절염은 해부학적 정복도에 달려있다고 보고하였다. 또한, Adib 등21)의 연구에서도 해부학적 정복을 시행한 환자에서 정복을 시행하지 않은 환자에 비해 골관절염 유병률이 낮게 보고되었다. 본 연구에서도 해부학적 정복도가 좋을수록 임상적 결과가 좋게 나타났다.
리스프랑 관절 손상 시 치료법으로 비수술적 치료인 석고 고정부터 관절 관통나사, suture button/tight rope를 이용한 수술적 치료까지 다양하지만 배부 가교 금속판을 이용한 고정은 최근 발달했으며,20) 내부 구조물을 고정시키면서 관절면을 보존하기 위해 사용되기 시작되었다. 게다가 더 나은 해부학적 정복을 유지하며 특히 분쇄된 골절을 고정하는 데 장점이 있었으나, 관절 관통 나사와 비교하였을 때 강도 또는 내구성이 부족하다는 약점이 있었다.13)
2014년 Hu 등9)은 60명의 리스프랑 관절 손상 환자들의 배부 가교 금속판 또는 관절 관통 나사를 이용한 고정법을 비교하였다. 단기 및 중기 추시상, AOFAS midfoot score는 배부 가교 금속판을 사용한 그룹에서 근소하게 더 좋은 결과가 나타났다. 또한 2018년 Kirzner 등18)은 108명의 리스프랑 관절 손상 환자들의 배부 가교 금속판, 관절 관통 나사, 또는 두 가지 방법을 혼합하여 고정한 방법을 비교하였고, 배부 가교 금속판을 이용하여 고정 시 더 좋은 임상적 및 방사선학적 결과가 나타났다.
본 연구에서도 배부 가교 금속판을 이용한 고정 방법이 관절 관통 나사를 이용하거나 혼합하여 고정한 방법보다 더 나은 임상적 결과가 나타났다.
2017년 Lau 등13)은 50명의 리스프랑 관절 손상 환자를 대상으로 관절 관통 나사, 배부 가교 금속판, 두 가지 방법의 혼합법을 이용한 고정 시 수술 후 임상적 결과에 대하여 평가하였고, 고정 방법보다는 해부학적 정복도가 좋을수록 임상적 결과가 좋게 나타났다. 최근 van Koperen 등22)에 의한 34명의 환자를 대상으로 한 후향적 연구에서는 관절 관통 나사 고정보다 배부 가교 금속판을 이용한 고정법 시 AOFAS midfoot score는 더 높았으며, 환자들의 만족도는 더 좋았으나 통계적으로 유의하지는 않았다. 이는 두 가지 방법을 혼합하여 고정한 군을 배부 가교 금속판 군에 포함시켰기 때문에 혼동된 결과가 나타났다. 게다가 해부학적 정복도에 대한 분석이 이루어지지 않았다.22) 본 연구에서는 수술 후 방사선 사진을 평가하여 해부학적 정복도를 평가하였고, 배부 가교 금속판을 이용한 고정 시 해부학적 정복도의 호전과 관련이 있음이 유의하게 나왔다(p=0.040).
하지만 첫 번째와 두 번째 중족골 기저부 간의 거리를 측정했을 시 두 가지 방법을 혼합하여 고정한 군에서 5.68±1.03 mm로, 배부 가교 금속판을 이용한 군(5.61±0.89 mm)과 비슷하게 측정되었다. 이것은 아마 두 가지 방법을 혼합하여 고정한 군이 8예로 증례 수가 상당히 작았고, 표준편차가 커서 두 군 간 뚜렷한 차이가 없었다고 볼 수 있다. 또한, 상대적으로 수술 후 상태가 양호한 환자들이 추시가 가능한 점도 배제할 수 없다.
또한, 골절 형태에 따른 분류 시 Myerson 분류 C2형에서 다른 type에 비해 임상적인 평가는 AOFAS midfoot score 평균 64점으로 상당히 낮게 나왔다. 이는 Kirzner 등18)의 연구에서도 동일한 결과를 보였다. 이러한 차이는 부분적 손상이 아닌 완전히 분리된 손상 시, 즉 초기 손상 정도가 심할 시 수술 방법에 관계없이 결과는 좋지 않음을 알 수 있다.
그리고 관절 관통 나사를 이용한 고정법 시 상당히 더 낮은 임상적 결과가 나타났다. 이는 초기 손상의 심각성 때문일 것이다. 열 고정 개수는 관절 관통 나사로 고정한 군(1.8개)이 배부 가교 금속판으로 고정한 군(1.5개)에 비해 평균 열 고정 개수가 더 많았다. 이에 열 고정 개수가 많아질수록 결과가 유의하게 더 나쁘다는 것을 보여준다.
본 연구는 몇 가지 한계를 가지고 있다. 후향적 연구로 인하여 환자들이 각 군으로 할당되고, 한 명의 술자에 의해 수술 방법 선정 시 무작위 방법으로 인하여 선택 편향(selection bias)이 발생하였을 가능성이 있다. 본 연구에서 관절 관통 나사를 이용하여 고정한 군에서는 대부분 Myerson 분류 A형이었다. 이 점을 제외하고 세 군은 비슷한 환자군을 가지고 있다. 그리고 평균 추시 기간은 7.5개월로 외상 후 골 관절염으로 진행 여부를 판단하기에는 충분한 기간이 되지 못하며, 관절 표면의 추가 손상을 방지함으로써 배부 가교 금속판을 이용한 고정 시 임상적 결과를 개선할 수 있음을 확인하기에는 짧은 기간이다. 마지막으로 상대적으로 적은 표본 수는 본 연구의 통계적 유의성을 나타내기에 제한적이다. 따라서 중, 장기적으로 임상적, 방사선학적 평가를 위해서는 추후 후속 연구가 필요할 것으로 생각된다.
결론
리스프랑 관절 손상의 치료에 있어 배부 가교 금속판을 이용한 고정법은 단기적으로는 방사선학적 및 임상적으로 비교적 만족스러운 결과를 보였다. 하지만 본 연구는 단기 추시 결과로, 골관절염 등의 합병증 및 기능적 결과에 대해서는 추가적인 연구가 필요할 것으로 생각된다.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Puna RA, Tomlinson MP. The role of percutaneous reduction and fixation of Lisfranc injuries. Foot Ankle Clin 2017;22:15–34.
-
-
Alberta FG, Aronow MS, Barrero M, Diaz-Doran V, Sullivan RJ, Adams DJ. Ligamentous Lisfranc joint injuries: a biomechanical comparison of dorsal plate and transarticular screw fixation. Foot Ankle Int 2005;26:462–473.
-
-
Watson TS, Shurnas PS, Denker J. Treatment of Lisfranc joint injury: current concepts. J Am Acad Orthop Surg 2010;18:718–728.
-
-
Abdelgaid SM, Salah M, Abdulsalam S, Abdulmalak F. Closed reduction & percutaneous fixation of lisfranc joints injuries: possibility, technique & results. Clin Res Foot Ankle 2013;1:109
-
-
Lee CA, Birkedal JP, Dickerson EA, Vieta PA Jr, Webb LX, Teasdall RD. Stabilization of Lisfranc joint injuries: a biomechanical study. Foot Ankle Int 2004;25:365–370.
-
-
Rajapakse B, Edwards A, Hong T. A single surgeon's experience of treatment of Lisfranc joint injuries. Injury 2006;37:914–921.
-
-
Welck MJ, Zinchenko R, Rudge B. Lisfranc injuries. Injury 2015;46:536–541.
-
-
Ahmed S, Bolt B, McBryde A. Comparison of standard screw fixation versus suture button fixation in Lisfranc ligament injuries. Foot Ankle Int 2010;31:892–896.
-
-
Hu SJ, Chang SM, Li XH, Yu GR. Outcome comparison of Lisfranc injuries treated through dorsal plate fixation versus screw fixation. Acta Ortop Bras 2014;22:315–320.
-
-
Ho NC, Sangiorgio SN, Cassinelli S, et al. Biomechanical comparison of fixation stability using a Lisfranc plate versus transarticular screws. Foot Ankle Surg 2019;25:71–78.
-
-
Stavlas P, Roberts CS, Xypnitos FN, Giannoudis PV. The role of reduction and internal fixation of Lisfranc fracture-dislocations: a systematic review of the literature. Int Orthop 2010;34:1083–1091.
-
-
Kuo RS, Tejwani NC, Digiovanni CW, et al. Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609–1618.
-
-
Lau S, Guest C, Hall M, Tacey M, Joseph S, Oppy A. Functional outcomes post Lisfranc injury-transarticular screws, dorsal bridge plating or combination treatment? J Orthop Trauma 2017;31:447–452.
-
-
Myerson MS, Fisher RT, Burgess AR, Kenzora JE. Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment. Foot Ankle 1986;6:225–242.
-
-
Wilppula E. Tarsometatarsal fracture-dislocation. Late results in 26 patients. Acta Orthop Scand 1973;44:335–345.
-
-
Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int 1994;15:349–353.
-
-
Ponkilainen VT, Uimonen M, Repo JP, Mattila VM, Haapasalo HH. Validity and internal consistency of the American Orthopaedic Foot and Ankle Society Midfoot Scale in patients with Lisfranc injury. Foot Ankle Surg 2020;26:523–529.
-
-
Kirzner N, Zotov P, Goldbloom D, Curry H, Bedi H. Dorsal bridge plating or transarticular screws for Lisfranc fracture dislocations: a retrospective study comparing functional and radiological outcomes. Bone Joint J 2018;100-B:468–474.
-
-
Perugia D, Basile A, Battaglia A, Stopponi M, De Simeonibus AU. Fracture dislocations of Lisfranc's joint treated with closed reduction and percutaneous fixation. Int Orthop 2003;27:30–35.
-
-
Lau S, Howells N, Millar M, De Villiers D, Joseph S, Oppy A. Plates, screws, or combination? Radiologic outcomes after Lisfranc fracture dislocation. J Foot Ankle Surg 2016;55:799–802.
-
-
Adib F, Medadi F, Guidi E, Alami Harandi A, Reddy C. Osteoarthritis following open reduction and internal fixation of the Lisfranc injury. Orthop Proc 2012;94-B Suppl 37:20
-
-
van Koperen PJ, de Jong VM, Luitse JS, Schepers T. Functional outcomes after temporary bridging with locking plates in Lisfranc injuries. J Foot Ankle Surg 2016;55:922–926.
-
 Cite
Cite
