 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 21(2); 2008 > Article
-
Original Article
- Classification and Treatment of Unstable Intertrochanteric Fracture according to the Existence of Posterior Fragment : Preliminary Report
- Lih Wang, M.D., Sung Keun Shon, M.D., Kyu Yeol Lee, M.D., Chul Hong Kim, M.D., Myung Jin Lee, M.D., Chul Won Lee, M.D., Sung Soo Kim, M.D.
-
Journal of the Korean Fracture Society 2008;21(2):110-116.
DOI: https://doi.org/10.12671/jkfs.2008.21.2.110
Published online: April 30, 2008
Department of Orthopaedic Surgery, College of Medicine, Dong-A University, Busan, Korea.
- Address reprint requests to: Sung Soo Kim, M.D. Department of Orthopaedic Surgery, College of Medicine, Dong-A University, 1, Dongdaesin-dong 3-ga, Seo-gu, Busan 602-715, Korea. Tel: 82-51-240-2953, Fax: 82-51-254-6757, sskim2@dau.ac.kr
Copyright © 2008 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,508 Views
- 13 Download
- 2 Crossref
Abstract
-
Purpose
- To predict the feature and stability of intertrochanteric fractures with posterior fragment using preoperative 3D computed tomography and to investigate the importance of the posterior fragment in treatment of unstable intertrochanteric fracture.
-
Materials and Methods
- 15 cases of unstable fractures with posterior fragment which were treated with nail only between October 2006 to August 2007 were classified into 2 groups: study group (5 cases with cannulated screw fixation of posterior fragment) and control group (10 cases without cannulated screw fixation). The average difference of neck-shaft angle, neck screw sliding distance and the complications in the two groups were compared retrospectively after a follow up of at least 3 months.
-
Results
- The average difference of neck-shaft angle in study and control group was 3.8 and 7.5 degree (p>0.05), respectively. The average difference of neck screw sliding distance was 1.6 and 6.6 mm (p<0.05), respectively. Complication which required reoperation was not noted in study group and complications of 3 cases about neck screw lateral protrusion, proximal migration and Z-effect phenomenon were noted in control group.
-
Conclusion
- The recognition and fixation of the posterior wall was found to be an important predictive factor in unstable intertrochanteric fracture treatment.
- 1. Bellabarba C, Herscovici D Jr, Ricci WM. Percutaneous treatment of peritrochanteric fractures using the gamma nail. Clin Orthop Relat Res, 2000;375:30-42.
- 2. Boyd HB, Griffin LL. Classification and treatment of trochanteric fractures. Arch Surg, 1949;58:853-866.
- 3. Bridle SH, Patel AD, Bircher M, Clavert PT. Fixation of intertrochanteric fractures of the femur. A randomized prospective comparison of the gamma nail and the dynamic hip screw. J Bone Joint Surg Br, 1991;73:330-334.
- 4. Briot B. Fractures per-trochanteriennes: anatomie pathologique et classification. Cahiers d'Enseignement de la S.O.F.C.O.T. n 12, Expansions Sci Franc Edit, 1980;69-76.
- 5. Butt MS, Krikler SJ, Nafie S, Ali MS. Comparison of dynamic hip screw and gamma nail: a prospective, randomized, controlled trial. Injury, 1995;26:615-618.
- 6. Cirotteau Y. Boyd H.B. and Griffin L.L. classification: a refinement proposal. Eur J Orthop Surg Traumatol, 2002;12:152-157.
- 7. Curtis MJ, Jinnah RH, Wilson V, Cunningham BW. Proximal femoral fractures: a biomechanical study to compare intramedullary and extramedullary fixation. Injury, 1994;25:99-104.
- 8. Den Hartog BD, Bartal E, Cooke F. Treatment of the unstable intertrochanteric fracture. Effect of the placement of the screw, its angle of insertion, and osteotomy. J Bone Joint Surg Am, 1991;73:726-733.
- 9. Evans EM. The treatment of trochanteric fractures of the femur. J Bone Joint Surg Br, 1949;31:190-203.
- 10. Hardy DC, Descamps PY, Krallis P, et al. Use of an intramedullary hip-screw compared with a compression hip-screw with a plate for intertrochanteric femoral fractures. A prospective, randomized study of one hundred patients. J Bone Joint Surg Am, 1998;80:618-630.
- 11. Harrington P, Nihal A, Singhania AK, Howell FR. Intramedullary hip screw versus sliding hip screw for unstable intertrochanteric femoral fractures in the elderly. Injury, 2002;33:23-28.
- 12. Haynes RC, Pöll RG, Miles AW, Weston RB. Failure of femoral head fixation: a cadaveric analysis of lag screw cut-out with the gamma locking nail and AO dynamic hip screw. Injury, 1997;28:337-341.
- 13. Jensen JS, Michaelson M. Trochanteric femoral fractures treated with McLaughlin osteosynthesis. Acta Orthop Scand, 1975;46:795-803.
- 14. Jones JB. Screw fixation of the lesser trochanteric fragment. Clin Orthop Relat Res, 1977;123:107.
- 15. Lee JM, Kim KY. Treatment of unstable trochanteric fracture using sliding hip screw with wiring of lesser trochanter. J Korean Orthop Assoc, 2000;35:861-866.
- 16. Mahomed N, Harrington I, Kellam J, Maistrelli G, Hearn T, Vroemen J. Biomechanical analysis of the gamma nail and sliding hip screw. Clin Orthop Relat Res, 1994;304:280-288.
- 17. Osnes EK, Lofthus CM, Falch JA, et al. More postoperative femoral fractures with the gamma nail than sliding screw plate in the treatment of trochanteric fractures. Acta Orthop Scand, 2001;72:252-256.
- 18. Papasimos S, Koutsojannis CM, Panagopoulos A, Mega P, Lambiris E. A randomized comparison of AMBI, TGN and PFN for treatment of unstable trochanteric fractures. Arch Orthop Trauma Surg, 2005;125:462-468.
- 19. Saudan M, Lübbeke A, Sadowski C, Riand N, Stern R, Hoffmeyer P. Pertrochanteric fractures: is there an advantage to an intramedullary nail?: a randomized, prospective study of 206 patients comparing the dynamic hip screw and proximal femoral nail. J Orthop Trauma, 2002;16:386-393.
- 20. Utrilla AL, Reig JS, Munoz FM, Tufanisco CB. Trochanteric gamma nail and compression hip screw for trochanteric fractures: a randomized, prospective, comparative study in 210 elderly patients with a new design of the gamma nail. J Orthop Trauma, 2005;19:229-233.
- 21. Watson JT, Moed BR, Cramer KE, Karges DE. Comparison of compression hip screw with the medoff sliding plate for intertrochanteric fractures. Clin Orthop Relat Res, 1998;348:79-86.
- 22. Werner-Tutschku W, Laitai G, Schmiedhuber G, Lang T, Pirkl C, Orthner E. Intra- and perioperative complications in the stabilization of per- and subtrochanteric femoral fractures by means of PEN. Unfallchirurg, 2002;105:881-885.
REFERENCES
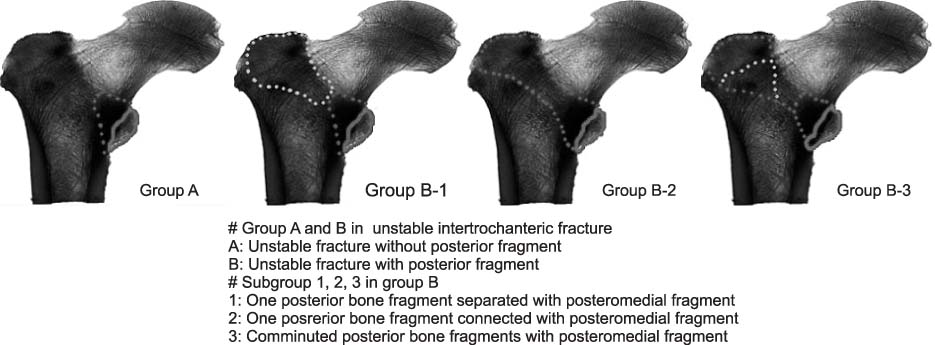
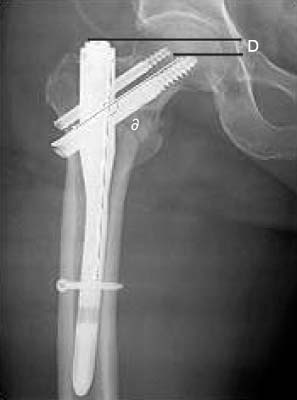
Fig. 3
(B) Fracture pattern of B1 unstable reverse oblique fracture by 3D computed tomography.
(C) Postoperative AP radiograph of Gamma nail insertion with percutaneous 2 cannulated screws fixation.
(D) AP radiograph showed satisfactory reduction at 3 months post-operation.
(A) Preoperative AP radiograph of a 86-year-old male with intertrochanteric fracture.
Fig. 4
(B) Fracture pattern of B2 unstable fracture by 3D computed tomography.
(C) Postoperative AP radiograph of Gamma nail insertion with percutaneous 2 cannulated screws fixation.
(D) AP radiograph showed 1 cannulated screw pull-out at 6 months post-operation.
(E) AP radiograph showed bone union with satisfactory reduction at 12 months post-operation.

(A) Preoperative AP radiograph of a 80-year-old male with intertrochanteric fracture.
Fig. 5
(B) Fracture pattern of B1 unstable fracture by 3D computed tomography.
(C) Postoperative AP radiograph of proximal femoral nail insertion with satisfactory reduction.
(D) AP radiograph showed neck screw back out and varus angulation at 2 months post-operation.
(E) Z-effect phenomenon was shown at 3 months postoperation.
(F) Bipolar hip arthroplasty was performed.
(A) Preoperative AP radiograph of a 80-year-old female with intertrochanteric fracture.
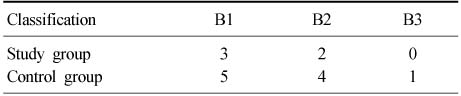
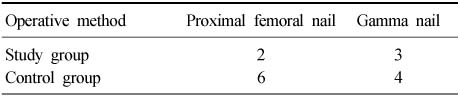
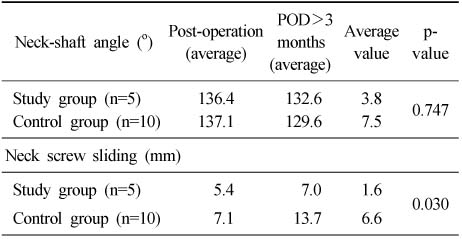
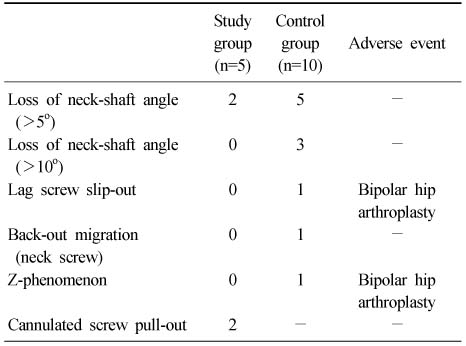
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Outcomes of dynamic hip screw augmented with trochanteric wiring for treatment of unstable type A2 intertrochanteric femur fractures
Chetan Puram, Chetan Pradhan, Atul Patil, Vivek Sodhai, Parag Sancheti, Ashok Shyam
Injury.2017; 48: S72. CrossRef - Additional Fixations for Sliding Hip Screws in Treating Unstable Pertrochanteric Femoral Fractures (AO Type 31-A2): Short-Term Clinical Results
Su Hyun Cho, Soo Ho Lee, Hyung Lae Cho, Jung Hoei Ku, Jae Hyuk Choi, Alex J Lee
Clinics in Orthopedic Surgery.2011; 3(2): 107. CrossRef
 Cite
CiteClassification and Treatment of Unstable Intertrochanteric Fracture according to the Existence of Posterior Fragment : Preliminary Report
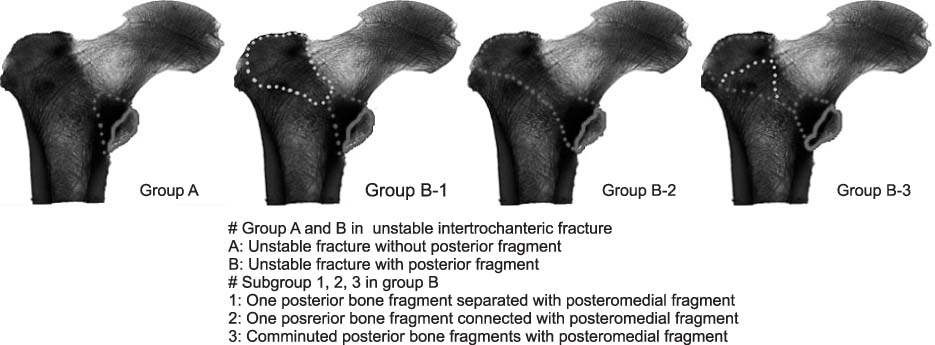
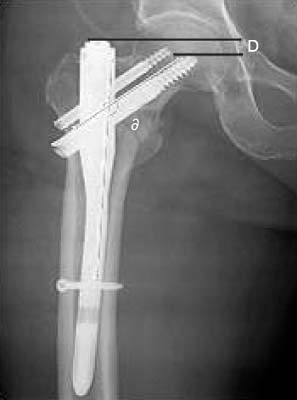
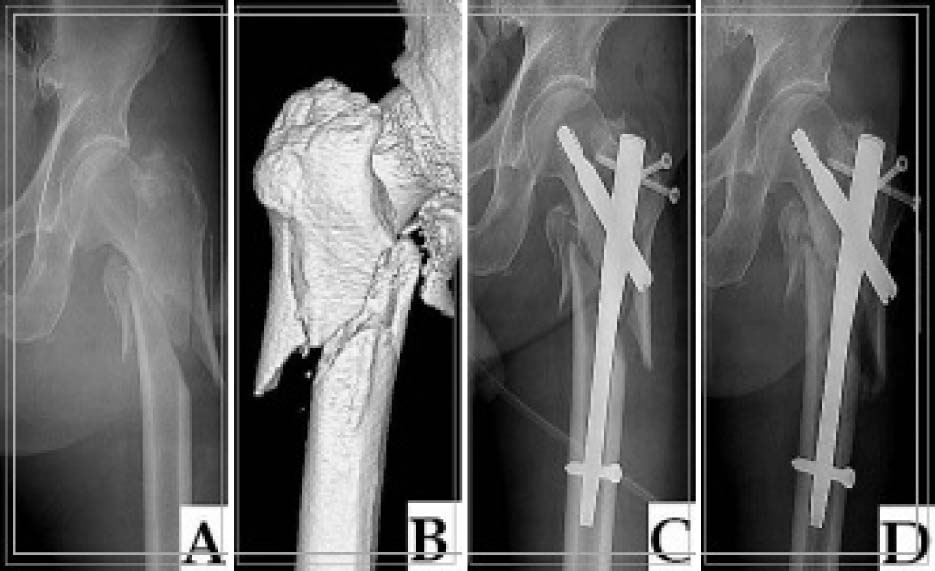

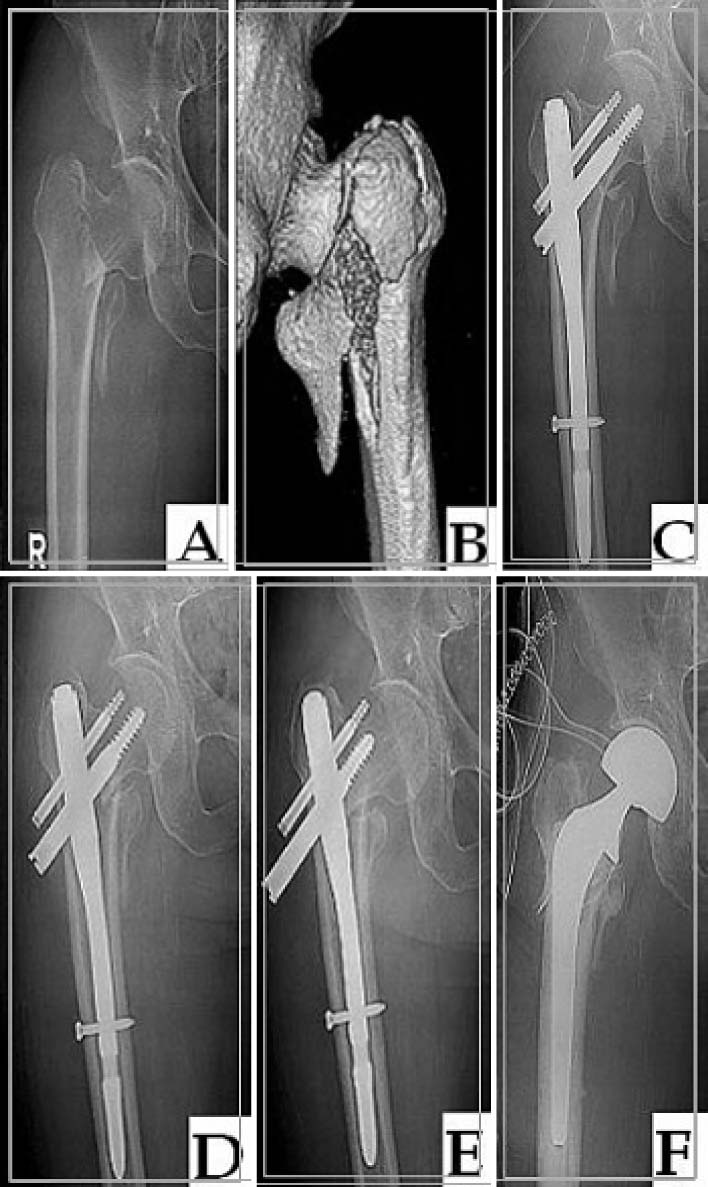
Fig. 1
Modified classification of unstable intertrochanteric fracture.
Fig. 2
Photograph shows measurements of neck-shaft angle (∂) and neck screw sliding distance (D).
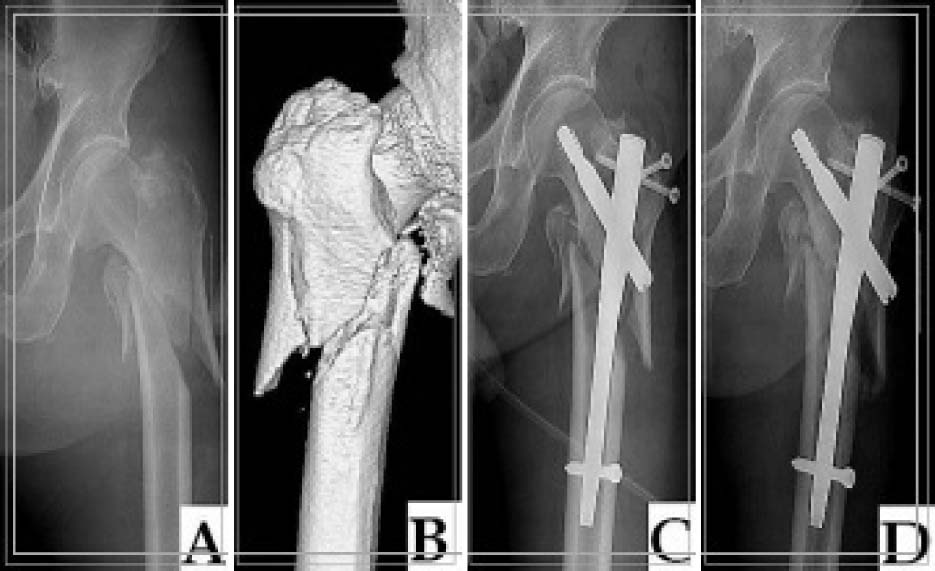
Fig. 3
(A) Preoperative AP radiograph of a 86-year-old male with intertrochanteric fracture.
(B) Fracture pattern of B1 unstable reverse oblique fracture by 3D computed tomography.
(C) Postoperative AP radiograph of Gamma nail insertion with percutaneous 2 cannulated screws fixation.
(D) AP radiograph showed satisfactory reduction at 3 months post-operation.
Fig. 4
(A) Preoperative AP radiograph of a 80-year-old male with intertrochanteric fracture.
(B) Fracture pattern of B2 unstable fracture by 3D computed tomography.
(C) Postoperative AP radiograph of Gamma nail insertion with percutaneous 2 cannulated screws fixation.
(D) AP radiograph showed 1 cannulated screw pull-out at 6 months post-operation.
(E) AP radiograph showed bone union with satisfactory reduction at 12 months post-operation.
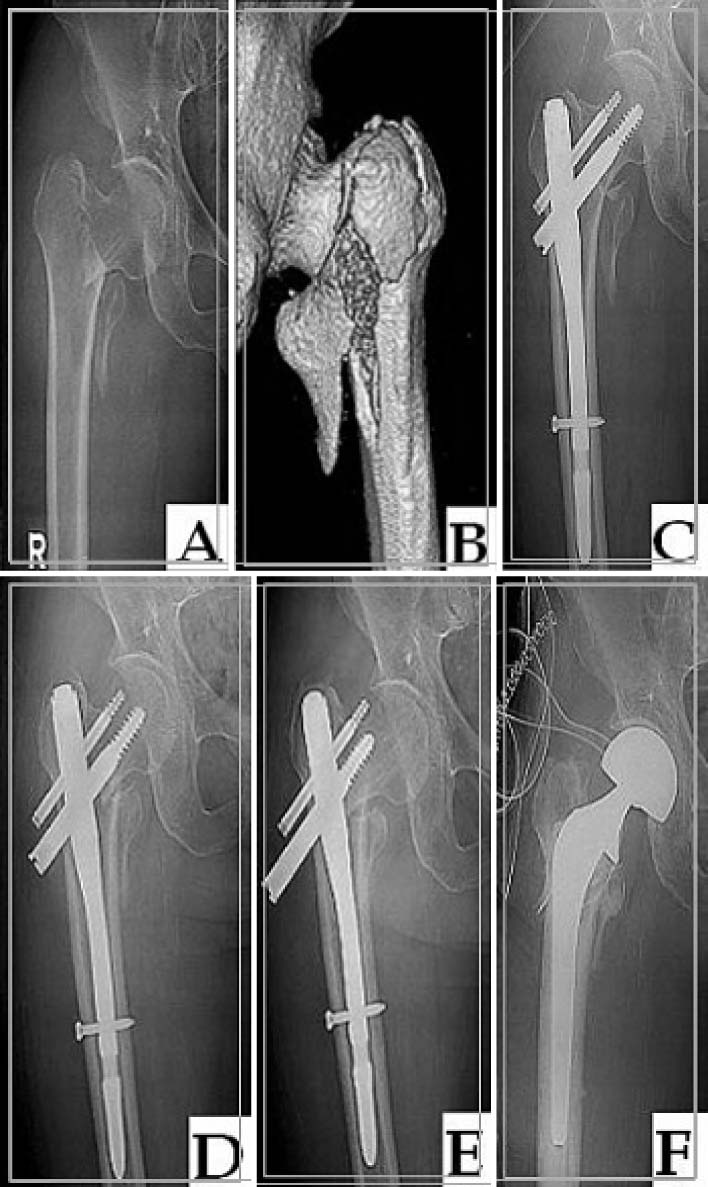
Fig. 5
(A) Preoperative AP radiograph of a 80-year-old female with intertrochanteric fracture.
(B) Fracture pattern of B1 unstable fracture by 3D computed tomography.
(C) Postoperative AP radiograph of proximal femoral nail insertion with satisfactory reduction.
(D) AP radiograph showed neck screw back out and varus angulation at 2 months post-operation.
(E) Z-effect phenomenon was shown at 3 months postoperation.
(F) Bipolar hip arthroplasty was performed.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Classification and Treatment of Unstable Intertrochanteric Fracture according to the Existence of Posterior Fragment : Preliminary Report
Distribution of modified classification between study group and control group
Data according to operative method between study group and control group
Average values of neck shaft angle between study group and control group
Summary of complications
Table 1
Distribution of modified classification between study group and control group
Table 2
Data according to operative method between study group and control group
Table 3
Average values of neck shaft angle between study group and control group
Table 4
Summary of complications

