 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 22(2); 2009 > Article
-
Original Article
- Volar Percutaneous Cannulated Screw Fixation for Subacute Scaphoid Wasit Fracture
- Jae Kwang Kim, M.D., Jong Oh Kim, M.D., Seung Yup Lee, M.D., Nam Hoon Do, M.D.
-
Journal of the Korean Fracture Society 2009;22(2):104-109.
DOI: https://doi.org/10.12671/jkfs.2009.22.2.104
Published online: April 30, 2009
Department of Orthopedic Surgery, School of Medicine, Ewha Womans University, Seoul, Korea.
- Address reprint requests to: Jae Kwang Kim, M.D. Department of Orthopedic Surgery, Ewha Womans Mokdong Hospital, 911-1, Mok-6-dong, Yangcheon-gu, Seoul 158-710, Korea. Tel: 82-2-2650-2591, Fax: 82-2-2642-0349, kimjk@ewha.ac.kr
• Received: January 18, 2009 • Revised: February 12, 2009 • Accepted: March 30, 2009
Copyright © 2009 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,079 Views
- 5 Download
- 1 Crossref
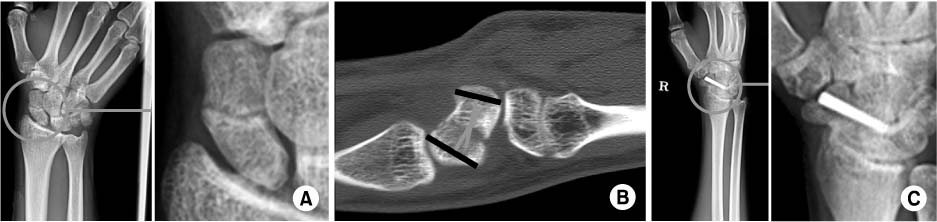
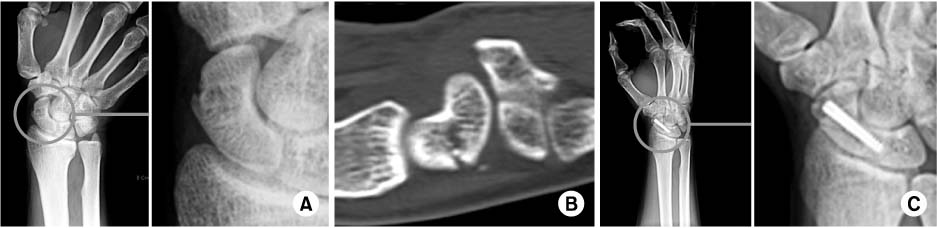
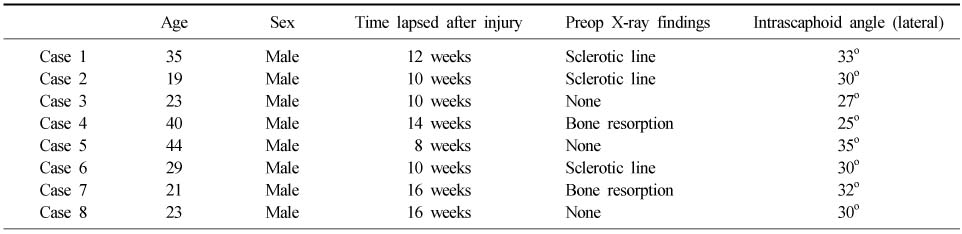
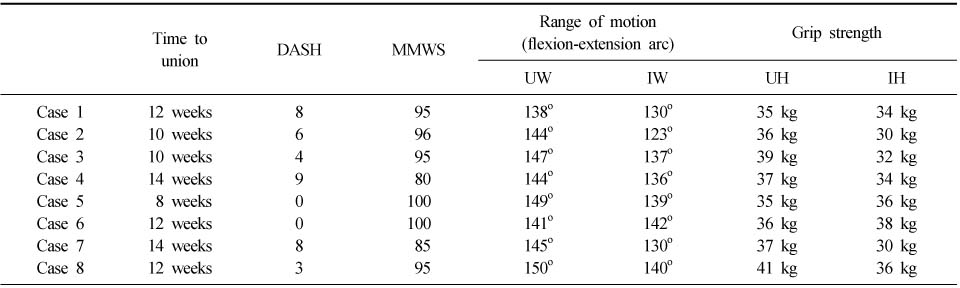
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Surgical Outcome of Stable Scaphoid Nonunion without Bone Graft
Eun Sun Moon, Myung Sun Kim, Il Kyu Kong, Min Sun Choi
Journal of the Korean Fracture Society.2010; 23(1): 69. CrossRef
 Cite
CiteVolar Percutaneous Cannulated Screw Fixation for Subacute Scaphoid Wasit Fracture
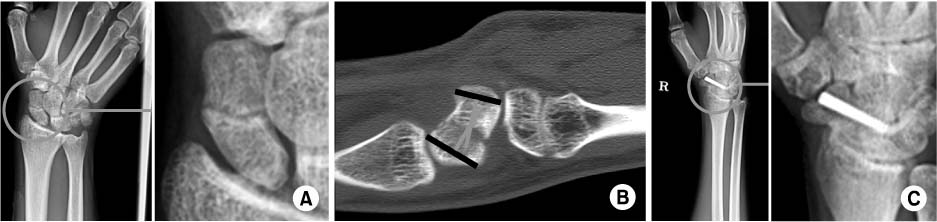
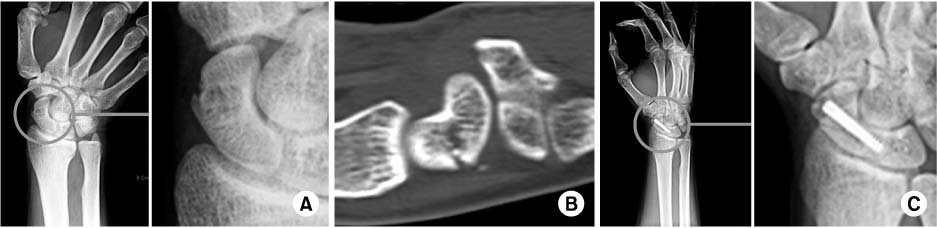
Fig. 1
Subacute scaphoid waist fracture with minimal sclerosis.
(A) Anteroposterior radiograph shows a minimal sclerotic line around the fracture.
(B) Lateral intrascaphoid angle is 28 degrees in CT.
(C) Healing was achieved 10 weeks after volar percutaenous screw insertion.
Fig. 2
Subacute scaphoid waist fracture with cyst formation.
(A) Anteroposterior radiograph shows cyst formation with bone resorption at the fracture.
(B) CT shows cyst formation with bone resorption at the waist of scaphoid.
(C) Healing was achieved 14 weeks after volar percutaenous screw insertion.
Fig. 1
Fig. 2
Volar Percutaneous Cannulated Screw Fixation for Subacute Scaphoid Wasit Fracture
Preoperative data of patients group
Data of patients group at 12 months follow up
DASH: Disabilities of the arm shoulder and hand, MMWS: Modified mayo wrist score, UW: Uninjured wrist, IW: Injured wrist, UH: Uninjured hand, IH: Injured hand.
Table 1
Preoperative data of patients group
Table 2
Data of patients group at 12 months follow up
DASH: Disabilities of the arm shoulder and hand, MMWS: Modified mayo wrist score, UW: Uninjured wrist, IW: Injured wrist, UH: Uninjured hand, IH: Injured hand.

