 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Article
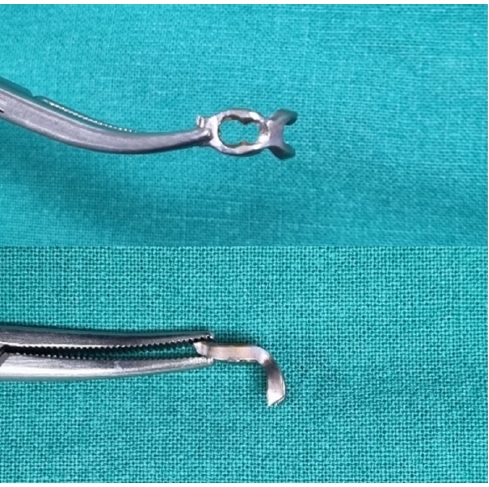
- Hook plate fixation for volar plate avulsion fractures of the middle phalanges in Korea: a case series
- Kang-San Lee, Sang-Woo Son, Hee-June Kim, Hyun-Joo Lee, Dong Hee Kim
- J Musculoskelet Trauma 2026;39(1):48-53. Published online January 25, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00339
-
 Abstract
Abstract
 PDF
PDF - Background
Volar plate avulsion fractures in phalanges are relatively common injuries. While surgical treatment can help reduce limitations in motion after injury, the small size of the fracture fragment can make the procedure challenging. In this study, we used hook plate fixation as a surgical technique for treating volar avulsion fractures in phalanges and evaluated its radiological and clinical outcomes.
Methods
The medical records of eight patients (nine digits) with volar plate avulsion fractures of the middle phalanx were retrospectively reviewed. All fractures were treated with a 1.5-mm hook plate after open reduction. Radiologic evaluations were performed using simple radiographs, and clinical outcomes were assessed through range of motion, instability, and pain.
Results
The mean follow-up period was 4.89 months (range, 1–9 months). All nine digits achieved bone union at the final follow-up. The mean union time was 2.2 months (range, 1–4 months). In all patients, the range of motion in the proximal interphalangeal joint was 85° (range, 70°–100°) before implant removal and 89.4° (range, 80°–100°) after implant removal. All patients demonstrated no joint instability and no residual pain.
Conclusion
Using a hook plate for volar plate avulsion fractures presents a promising alternative to existing fixation methods. Its biomechanical advantages and ease of fabrication make it a valuable tool in hand surgery. Level of evidence: IV.
- 1,541 View
- 41 Download

Review Article
- Fixation Options of Unstable Posterior Pelvic Ring Disruption: Ilio-Sacral Screw Fixation, S2AI Fixation, Posterior Tension Band Plate Fixation, and Spino-Pelvic Fixation
- Dong Hee Kim, Jae Hoon Jang, Myungji Shin, Gu Hee Jung
- J Korean Fract Soc 2019;32(4):240-247. Published online October 31, 2019
- DOI: https://doi.org/10.12671/jkfs.2019.32.4.240
-
Abstract
PDF
- The fixation methods that can be used for unstable posterior pelvic ring injuries have undergone many innovative changes due to the recent development of surgical and imaging techniques. After understanding the appropriate indications of first and second sacroiliac screw fixation and spinopelvic fixation, innovative methods, including the trans-sacral screw fixation, posterior tension-band plate fixation, and the S2AI screw, would be chosen and applied. Considering the anatomical complexity and proximity to the surrounding vessels and nerves in the posterior fixation, the safe zone according to the fixation options should be well understood in preoperative planning. Moreover, the functional reduction of the posterior pelvic ring through the reduction and fixation of the anterior lesion should be achieved before placing the implant to reduce the number of malposition-related complications.
-
Citations
Citations to this article as recorded by
- Clinical Research through Computational Anatomy and Virtual Fixation
Ju Yeong Kim, Dong-Geun Kang, Gu-Hee Jung
Journal of the Korean Orthopaedic Association.2023; 58(4): 299. CrossRef
- Clinical Research through Computational Anatomy and Virtual Fixation
- 1,956 View
- 19 Download
- 1 Crossref
Case Report
- Treatment of Traumatic Posterior Dislocation of the Sternoclavicular Joint: A Case Report
- Dong Hee Kim, Do Hoon Kim, Seok Kwon Kang, Eui Chul Lee
- J Korean Fract Soc 2013;26(1):56-59. Published online January 31, 2013
- DOI: https://doi.org/10.12671/jkfs.2013.26.1.56
-
Abstract
PDF
- Compared with acromioclavicular dislocation, dislocation of the clavicle at its sternal end is uncommon and accounts for 3% of all injuries to the shoulder girdle. Furthermore, the posterior dislocation of the sternoclavicular joint is relatively a rare injury compared to the other types of sternoclavicular dislocation. We report this case since we have experience with similar cases of traumatic posterior dislocation at the sternoclavicular joint, which were successfully treated with x-ray guided reduction.
-
Citations
Citations to this article as recorded by- Posterior Sternoclavicular Dislocation: A Case Report
So Hwa Yoon, Sun Ki Kim, Ki Jun Kim
Journal of the Korean Society of Radiology.2015; 72(2): 128. CrossRef
- Posterior Sternoclavicular Dislocation: A Case Report
- 1,183 View
- 3 Download
- 1 Crossref
 First
First Prev
Prev

