 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 29(2); 2016 > Article
-
Original Article
- Usefulness of the Additional K-Wire Fixation and Suture for Reinforce the Treatment of Distal Clavicle Fracture Using Modified Tension Band Wiring
- Seung-Bum Chae, M.D., Chang-Hyuk Choi, M.D., Dong-Young Kim, M.D.
-
Journal of the Korean Fracture Society 2016;29(2):107-113.
DOI: https://doi.org/10.12671/jkfs.2016.29.2.107
Published online: April 15, 2016
Department of Orthopaedic Surgery, Daegu Catholic University Medical Center, Daegu, Korea.
- Address reprint requests to: Chang-Hyuk Choi, M.D. Department of Orthopaedic Surgery, Daegu Catholic University Medical Center, 33 Duryugongwon-ro 17-gil, Nam-gu, Daegu 42472, Korea. Tel: 82-53-650-4276, Fax: 82-53-652-4272, chchoi@cu.ac.kr
• Received: March 25, 2015 • Revised: November 2, 2015 • Accepted: December 31, 2015
Copyright © 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,422 Views
- 7 Download
- 2 Crossref
Abstract
-
Purpose
- We attempted to evaluate the clinical results of modified tension band wiring (MTBW) with additional K-wire fixation and suture for distal clavicle fracture.
-
Materials and Methods
- Fifty-nine patients with a distal clavicle fracture from May 2009 to December 2013 treated with MTBW were enrolled in this study. Their fracture types were type 2, 12; and type 3, 33; type 4, 8; and type 5, 6 according to Craig classification group II; average age was 47.2 years with a mean follow-up period of 27.9 months. The operations were performed within a mean of 3.1 days a fter t rauma. The c linical results were evaluated u sing University of California at Los Angeles scores (UCLA), American Shoulder and Elbow Surgeons scores (ASES) and Korean Shoulder Society scores (KSS) at 1 year after surgery.
-
Results
- Radiographic bone union was achieved at a mean of 3.7 months after the operation. In the last observation, their range of motion was forward flexion 159.0°, external rotation 59.8°, and internal rotation 4.3 points, and there were 2 cases of nonunion. Each average functional score was UCLA 31.3 points, KSS 91.6 points, and ASES 93.0 points.
-
Conclusion
- For the surgical treatment of distal clavicle fractures, MTBW with additional K-wire fixation and suture is a useful technique allowing early range of motion exercises, minimizing soft tissue damage, and preserving the acromio-clavicular joint.
- 1. Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res, 1994;(300):127-132.Article
- 2. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am, 2004;86:1359-1365.ArticlePubMed
- 3. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg, 2002;11:452-456.ArticlePubMed
- 4. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br, 1998;80:476-484.
- 5. Stanley D, Trowbridge EA, Norris SH. The mechanism of clavicular fracture. A clinical and biomechanical analysis. J Bone Joint Surg Br, 1988;70:461-464.ArticlePubMedPDF
- 6. Allman FL Jr. Fractures and ligamentous injuries of the clavicle and its articulation. J Bone Joint Surg Am, 1967;49:774-784.Article
- 7. Kim JH, Lee SC, Cho DY, Yoon HK, Lee YS. Percutaneus cerclage wiring in distal clavicle fracture type 2a-one case report. J Korean Shoulder Elbow Soc, 2006;9:124-129.Article
- 8. Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc, 1960;172:1006-1011.ArticlePubMed
- 9. Ellman H, Hanker G, Bayer M. Repair of the rotator cuff. End-result study of factors influencing reconstruction. J Bone Joint Surg Am, 1986;68:1136-1144.ArticlePubMed
- 10. Richards RR, An KN, Bigliani LU, et al. A standardized method for the assessment of shoulder function. J Shoulder Elbow Surg, 1994;3:347-352.Article
- 11. Tae SK, Rhee YG, Park TS, et al. The development and validation of an appraisal method for rotator cuff disorders: the Korean Shoulder Scoring System. J Shoulder Elbow Surg, 2009;18:689-696.Article
- 12. Lee GJ. The shoulder & elbow. Seoul: Yeong Chang Co; 2007.
- 13. Herrmann S, Schmidmaier G, Greiner S. Stabilisation of vertical unstable distal clavicular fractures (Neer 2b) using locking T-plates and suture anchors. Injury, 2009;40:236-239.Article
- 14. Hessmann M, Kirchner R, Baumgaertel F, Gehling H, Gotzen L. Treatment of unstable distal clavicular fractures with and without lesions of the acromioclavicular joint. Injury, 1996;27:47-52.ArticlePubMed
- 15. Kashii M, Inui H, Yamamoto K. Surgical treatment of distal clavicle fractures using the clavicular hook plate. Clin Orthop Relat Res, 2006;447:158-164.ArticlePubMed
- 16. Neviaser RJ. Injuries to the clavicle and acromioclavicular joint. Orthop Clin North Am, 1987;18:433-438.Article
- 17. Kona J, Bosse MJ, Staeheli JW, Rosseau RL. Type II distal clavicle fractures: a retrospective review of surgical treatment. J Orthop Trauma, 1990;4:115-120.
- 18. Kao FC, Chao EK, Chen CH, Yu SW, Chen CY, Yen CY. Treatment of distal clavicle fracture using Kirschner wires and tension-band wires. J Trauma, 2001;51:522-525.ArticlePubMed
- 19. Ko SH, Cho SD, Park MS, Ryu SG. The use of hook plate on the management of unstable Neer II lateral end fracture of the clavicle. J Korean Shoulder Elbow Soc, 2003;6:131-137.Article
- 20. Khan LA, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg Am, 2009;91:447-460.Article
- 21. VanBeek C, Boselli KJ, Cadet ER, Ahmad CS, Levine WN. Precontoured plating of clavicle fractures: decreased hardware-related complications? Clin Orthop Relat Res, 2011;469:3337-3343.Article
- 22. Flinkkilä T, Ristiniemi J, Hyvönen P, Hämäläinen M. Surgical treatment of unstable fractures of the distal clavicle: a comparative study of Kirschner wire and clavicular hook plate fixation. Acta Orthop Scand, 2002;73:50-53.ArticlePubMed
- 23. Flinkkilä T, Ristiniemi J, Lakovaara M, Hyvönen P, Leppilahti J. Hook-plate fixation of unstable lateral clavicle fractures: a report on 63 patients. Acta Orthop, 2006;77:644-649.Article
- 24. Mizue F, Shirai Y, Ito H. Surgical treatment of comminuted fractures of the distal clavicle using Wolter clavicular plates. J Nippon Med Sch, 2000;67:32-34.Article
- 25. Kang HJ, Park KK, Yoon HK, Song HK, Hahn SB. T Plate fixation for unstable fracture of distal clavicle. J Korean Fract Soc, 2006;19:329-334.Article
- 26. Levy O. Simple, minimally invasive surgical technique for treatment of type 2 fractures of the distal clavicle. J Shoulder Elbow Surg, 2003;12:24-28.Article
- 27. Chun JM, Kim SY, Lee KW, Shin SJ, Kim EG. Modified tenson band fixation for unstable fracture of the distal clavicle. J Korean Orthop Assoc, 2002;37:416-420.ArticlePDF
REFERENCES
Fig. 1
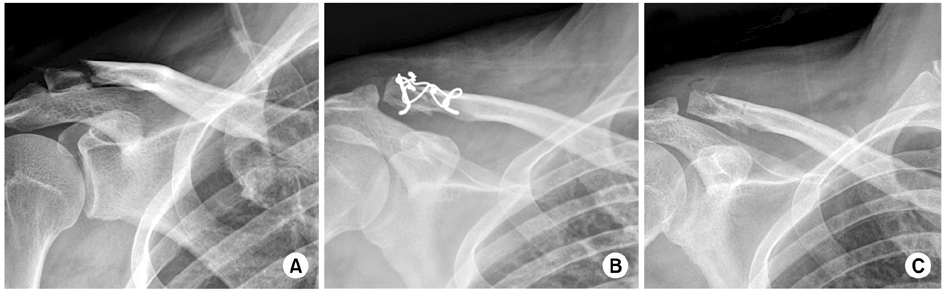
(A) A 46-year-old male sustained a Neer type IIb right distal clavicle fracture. (B) The fracture was reduced with modified tension band wiring. (C) The last follow-up (postoperative day 4 months) radiograph shows solid union.
Fig. 2

(A) A 16-year-old male sustained a Neer type IIb left distal clavicle fracture. (B) The fracture was reduced with modified tension band wiring (MTBW). Ahead of MTBW, K-wire fixation on the displaced bone fragment (arrow). (C) The last follow-up (postoperative day 5 months) radiograph shows solid union. (D) K-wire fixation on the displaced bone fragment (arrow), which affords additional stability maintaining reduction of the displaced fracture segment.
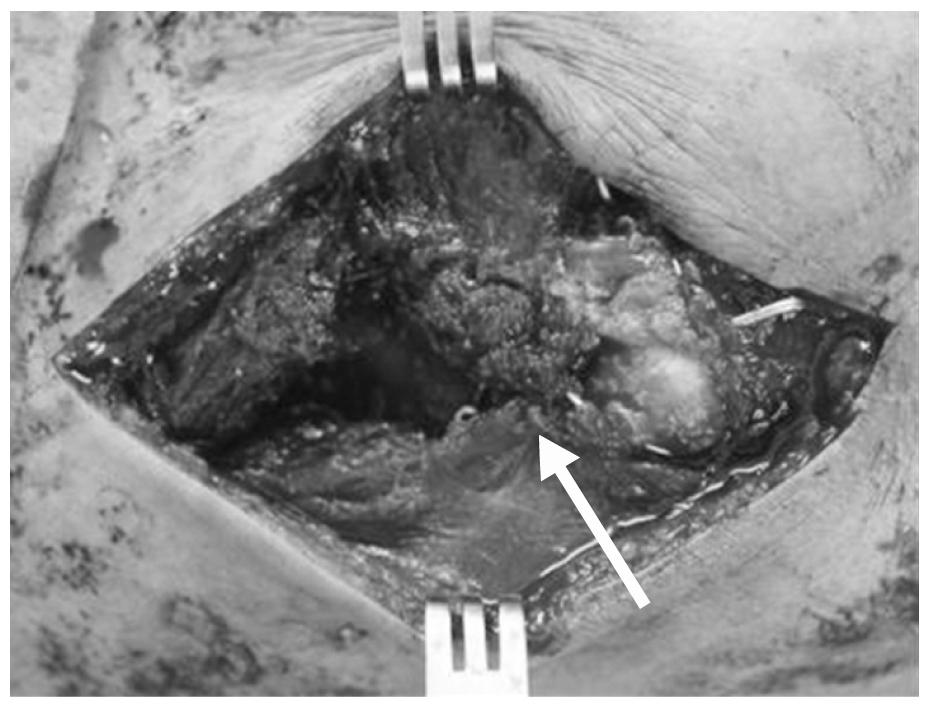
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Treatment Results for Unstable Distal Clavicle Fractures Using Hybrid Fixations with Finger Trap Wire and Plate
Jeong-Seok Yu, Bong-Seok Yang, Byeong-Mun Park, O-Sang Kwon
Journal of the Korean Orthopaedic Association.2022; 57(2): 135. CrossRef - Comparison of Locking Compression Plate Superior Anterior Clavicle Plate with Suture Augmentation and Hook Plate for Treatment of Distal Clavicle Fractures
Jun-Cheol Choi, Woo-Suk Song, Woo-Sung Kim, Jeong-Muk Kim, Chan-Woong Byun
Archives of Hand and Microsurgery.2017; 22(4): 247. CrossRef
 Cite
CiteUsefulness of the Additional K-Wire Fixation and Suture for Reinforce the Treatment of Distal Clavicle Fracture Using Modified Tension Band Wiring
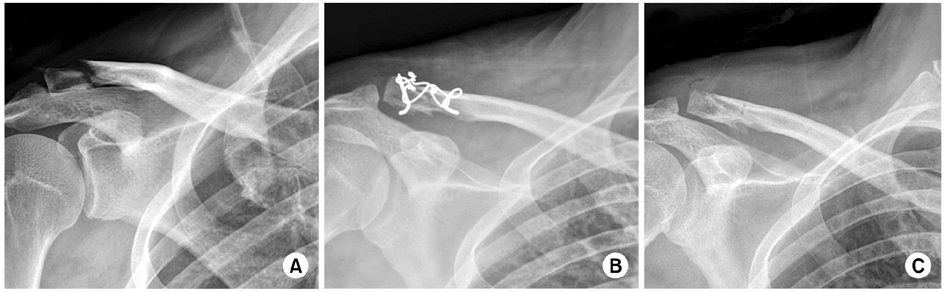

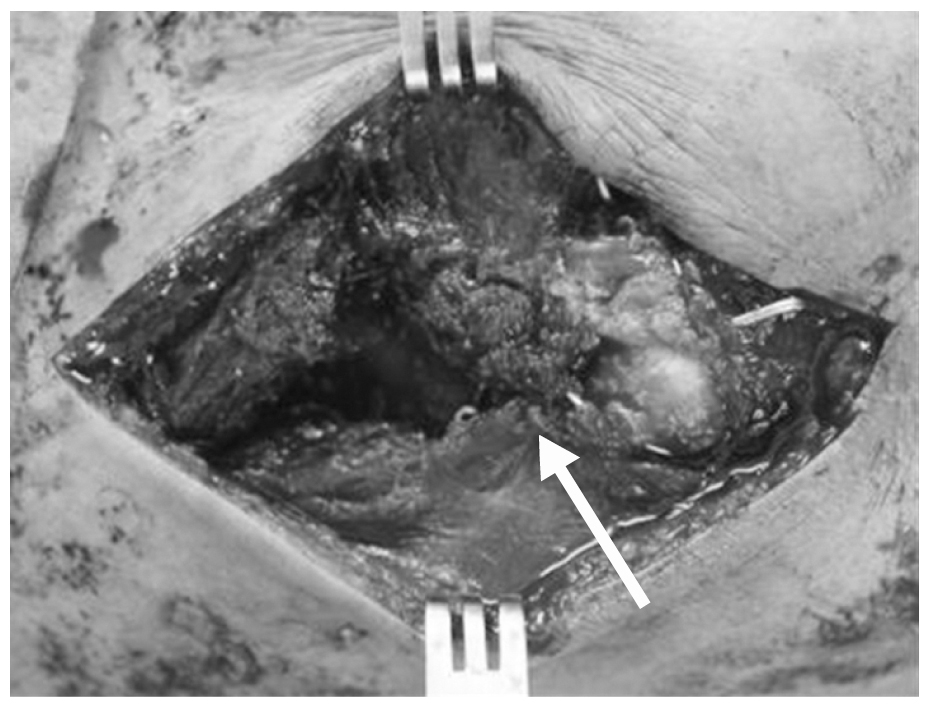
Fig. 1
(A) A 46-year-old male sustained a Neer type IIb right distal clavicle fracture. (B) The fracture was reduced with modified tension band wiring. (C) The last follow-up (postoperative day 4 months) radiograph shows solid union.
Fig. 2
(A) A 16-year-old male sustained a Neer type IIb left distal clavicle fracture. (B) The fracture was reduced with modified tension band wiring (MTBW). Ahead of MTBW, K-wire fixation on the displaced bone fragment (arrow). (C) The last follow-up (postoperative day 5 months) radiograph shows solid union. (D) K-wire fixation on the displaced bone fragment (arrow), which affords additional stability maintaining reduction of the displaced fracture segment.
Fig. 3
Small bone fragment fixation with non-absorbable suture material (arrow), which affords stability of the fracture site as well as soft tissue healing.
Fig. 1
Fig. 2
Fig. 3
Usefulness of the Additional K-Wire Fixation and Suture for Reinforce the Treatment of Distal Clavicle Fracture Using Modified Tension Band Wiring

