 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 29(3); 2016 > Article
-
Original Article
- Orthogonal Locking Compression Plate Fixation for Distal Humeral Intraarticular Fractures
- Hyoung Keun Oh, M.D., Suk Kyu Choo, M.D., Kyoung Hwan Koh, M.D., Ji Woong Yeom, M.D.
-
Journal of the Korean Fracture Society 2016;29(3):178-184.
DOI: https://doi.org/10.12671/jkfs.2016.29.3.178
Published online: July 21, 2016
Department of Orthopaedic Surgery, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea.
- Address reprint requests to: Hyoung Keun Oh, M.D. Department of Orthopaedic Surgery, Inje University Ilsan Paik Hospital, 170 Juhwa-ro, Ilsanseo-gu, Goyang 10380, Korea. Tel: 82-31-910-7968, Fax: 82-31-910-7967, osd11@paik.ac.kr
• Received: November 3, 2015 • Revised: December 2, 2015 • Accepted: May 23, 2016
Copyright © 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 730 Views
- 0 Download
Abstract
-
Purpose
- To investigate the surgical outcomes of orthogonal locking compression plate fixation for distal humeral intraarticular fractures.
-
Materials and Methods
- This study included 18 patients presenting a distal humeral intraarticular fracture who were treated with orthogonal locking compression plate fixation. According to the AO/OTA classification, there were eight C2 and ten C3 fractures. We evaluated radiologic outcomes, clinical results with range of motion, operation-related complications, and functional score by Mayo elbow performance score (MEPS).
-
Results
- The a verage u nion t ime was 3.5 months, and there was no c ase of r eduction l oss of a rticular f racture at t he last follow-up. Additional surgical procedures were needed in the three cases of C3 fractures. There was one case of heterotrophic ossification and one case of K-wire irritation. The average range of motion of elbow joint was 7° to 122°, and functional results were graded as 14 excellent, three good, and one fair by MEPS.
-
Conclusion
- Anatomical reduction and internal fixation with orthogonal locking compression plate could provide satisfactory surgical outcomes for the treatment of distal humeral intraarticular fracture.
- 1. Galano GJ, Ahmad CS, Levine WN. Current treatment strategies for bicolumnar distal humerus fractures. J Am Acad Orthop Surg, 2010;18:20-30.ArticlePubMed
- 2. Bégué T. Articular fractures of the distal humerus. Orthop Traumatol Surg Res, 2014;100:S55-S63.ArticlePubMed
- 3. Davies MB, Stanley D. A clinically applicable fracture classification for distal humeral fractures. J Shoulder Elbow Surg, 2006;15:602-608.ArticlePubMed
- 4. O'Driscoll SW. Supracondylar fractures of the elbow: open reduction, internal fixation. Hand Clin, 2004;20:465-474.Article
- 5. O'Driscoll SW. Optimizing stability in distal humeral fracture fixation. J Shoulder Elbow Surg, 2005;14:186S-194S.
- 6. Korner J, Diederichs G, Arzdorf M, et al. A biomechanical evaluation of methods of distal humerus fracture fixation using locking compression plates versus conventional reconstruction plates. J Orthop Trauma, 2004;18:286-293.Article
- 7. Wilkinson JM, Stanley D. Posterior surgical approaches to the elbow: a comparative anatomic study. J Shoulder Elbow Surg, 2001;10:380-382.ArticlePubMed
- 8. Bucholz RW, Hackman JD, Court-Brown C. Rockwood and green's fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006. p. 1059-1064.
- 9. Kaiser T, Brunner A, Hohendorff B, Ulmar B, Babst R. Treatment of supra- and intra-articular fractures of the distal humerus with the LCP Distal Humerus Plate: a 2-year follow-up. J Shoulder Elbow Surg, 2011;20:206-212.Article
- 10. Charissoux JL, Mabit C, Fourastier J, et al. Comminuted intra-articular fractures of the distal humerus in elderly patients. Rev Chir Orthop Reparatrice Appar Mot, 2008;94:S36-S62.
- 11. Pajarinen J, Björkenheim JM. Operative treatment of type C intercondylar fractures of the distal humerus: results after a mean follow-up of 2 years in a series of 18 patients. J Shoulder Elbow Surg, 2002;11:48-52.Article
- 12. Hoppenfeld S, deBoer P, Buckley R. Surgical exposures in orthopedics. The anatomic approach. Philadelphia: Wolters Kluwer Ed; 2009.
- 13. Imatani J, Morito Y, Hashizume H, Inoue H. Internal fixation for coronal shear fracture of the distal end of the humerus by the anterolateral approach. J Shoulder Elbow Surg, 2001;10:554-556.Article
- 14. Faber KJ. Coronal shear fractures of the distal humerus: the capitellum and trochlea. Hand Clin, 2004;20:455-464.Article
- 15. Sen MK, Sama N, Helfet DL. Open reduction and internal fixation of coronal fractures of the capitellum. J Hand Surg Am, 2007;32:1462-1465.Article
- 16. Vennettilli M, Athwal GS. Parallel versus orthogonal plating for distal humerus fractures. J Hand Surg Am, 2012;37:819-820.ArticlePubMed
- 17. Ruan HJ, Liu JJ, Fan CY, Jiang J, Zeng BF. Incidence, management, and prognosis of early ulnar nerve dysfunction in type C fractures of distal humerus. J Trauma, 2009;67:1397-1401.Article
- 18. Chen RC, Harris DJ, Leduc S, Borrelli JJ Jr, Tornetta P 3rd, Ricci WM. Is ulnar nerve transposition beneficial during open reduction internal fixation of distal humerus fractures? J Orthop Trauma, 2010;24:391-394.Article
REFERENCES
Fig. 1

Plain antero-posterior (AP) X-ray (A) and 3-dimensional computed tomography image (B) of an 84-year-old male show C2 distal humeral intraarticular fracture. Articular fracture was fixed with 4.0 mm partial threaded cancellous screw and orthogonal locking plate fixation was performed without olecranon osteotomy. Last follow-up AP and lateral views (C, D) show solid bony union without implant loosening.
Fig. 2

(A) A case of comminuted intraarticular distal humeral fracture of a 33-year-old male. Plain X-ray and 3-dimensional computed tomography scans show intraarticular comminuted fracture. (B) Small comminuted articular fragments were fixed with 2.0 mm screws. Orthogonal locking plate fixation was performed and intercondylar fracture was fixed with K-wires and 2.7 mm locking head screw through the lateral plate.
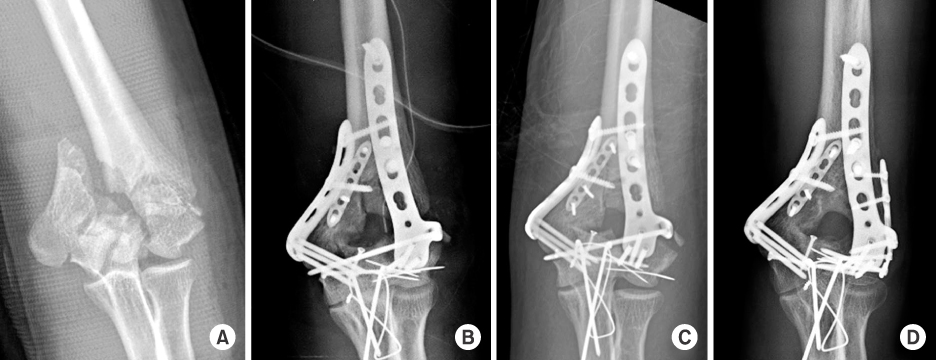
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteOrthogonal Locking Compression Plate Fixation for Distal Humeral Intraarticular Fractures
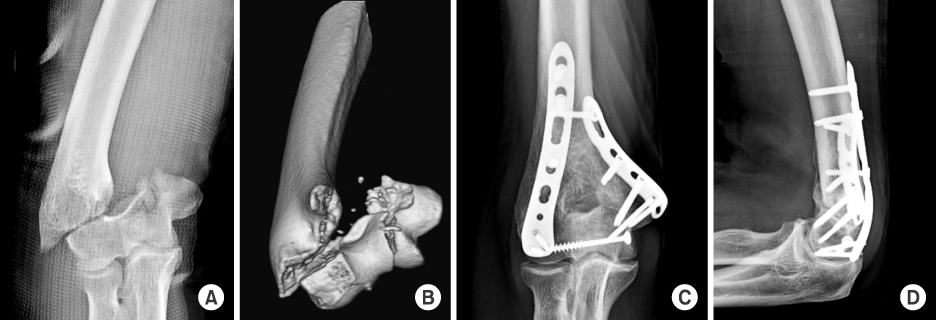

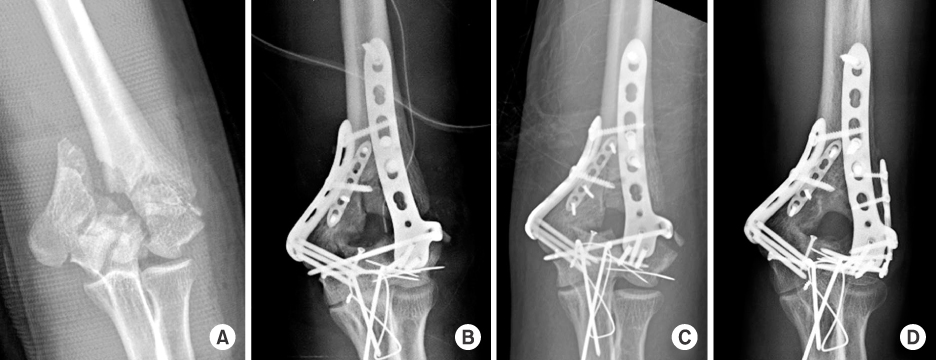
Fig. 1
Plain antero-posterior (AP) X-ray (A) and 3-dimensional computed tomography image (B) of an 84-year-old male show C2 distal humeral intraarticular fracture. Articular fracture was fixed with 4.0 mm partial threaded cancellous screw and orthogonal locking plate fixation was performed without olecranon osteotomy. Last follow-up AP and lateral views (C, D) show solid bony union without implant loosening.
Fig. 2
(A) A case of comminuted intraarticular distal humeral fracture of a 33-year-old male. Plain X-ray and 3-dimensional computed tomography scans show intraarticular comminuted fracture. (B) Small comminuted articular fragments were fixed with 2.0 mm screws. Orthogonal locking plate fixation was performed and intercondylar fracture was fixed with K-wires and 2.7 mm locking head screw through the lateral plate.
Fig. 3
(A) A 30-year-old male suffered from open comminuted distal humeral fracture. Open reduction and plate fixation was performed (B), but after range of motion exercise, fixation loss occurred on lateral plate (C). (D) After additional plate fixation, solid bony union could be obtained.
Fig. 1
Fig. 2
Fig. 3
Orthogonal Locking Compression Plate Fixation for Distal Humeral Intraarticular Fractures

