 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 34(1); 2021 > Article
- Review Article Pediatric Femoral Neck Fracture
- Joo Hyung Han, Hoon Park
-
Journal of Musculoskeletal Trauma 2021;34(1):34-43.
DOI: https://doi.org/10.12671/jkfs.2021.34.1.34
Published online: January 31, 2021
Department of Orthopaedic Surgery, Gangnam Severance Hospital, Seoul, Korea
- 2,632 Views
- 56 Download
- 0 Crossref
- 0 Scopus
Abstract
Pediatric femoral neck fracture is an uncommon injury with a high complication rate, regardless of the appropriate diagnosis and management. The bony anatomy and blood supply of the proximal femur in a skeletally immature patient differ from those in adult patients. Generally, these fractures result from high-energy trauma, but pathologic hip fractures also occur, usually from low-energy trauma. Pediatric femoral neck fractures are categorized using the Delbet classification system. This classification guides management and aids clinicians in determining the risk of avascular osteonecrosis. The ideal surgical treatment is determined by the fracture type and the age of the patient. Reduction, which is achieved using a closed or open procedure, combined with stable fixation and/or cast immobilization, is recommended for most of these fractures. Anatomical reduction within 24 hours from the injury may result in a good surgical outcome. Although the effects of capsular decompression after reduction and fixation have not been established, decompression is easy to perform and may reduce the risk of avascular necrosis. Despite appropriate management, osteonecrosis can occur after all types of pediatric femur neck fractures. Other complications include coxa vara, nonunion, and premature physeal arrest.
J Korean Fract Soc. 2021 Jan;34(1):34-43. Korean.
Published online Jan 25, 2021.
https://doi.org/10.12671/jkfs.2021.34.1.34
Published online Jan 25, 2021.
https://doi.org/10.12671/jkfs.2021.34.1.34
Copyright © 2021 The Korean Fracture Society. All rights reserved.
Review
Pediatric Femoral Neck Fracture
Joo Hyung Han , M.D.
and Hoon Park, M.D., Ph.D.
, M.D.
and Hoon Park, M.D., Ph.D.
, M.D.
and Hoon Park, M.D., Ph.D.
Abstract
Pediatric femoral neck fracture is an uncommon injury with a high complication rate, regardless of the appropriate diagnosis and management. The bony anatomy and blood supply of the proximal femur in a skeletally immature patient differ from those in adult patients. Generally, these fractures result from high-energy trauma, but pathologic hip fractures also occur, usually from low-energy trauma. Pediatric femoral neck fractures are categorized using the Delbet classification system. This classification guides management and aids clinicians in determining the risk of avascular osteonecrosis. The ideal surgical treatment is determined by the fracture type and the age of the patient. Reduction, which is achieved using a closed or open procedure, combined with stable fixation and/or cast immobilization, is recommended for most of these fractures. Anatomical reduction within 24 hours from the injury may result in a good surgical outcome. Although the effects of capsular decompression after reduction and fixation have not been established, decompression is easy to perform and may reduce the risk of avascular necrosis. Despite appropriate management, osteonecrosis can occur after all types of pediatric femur neck fractures. Other complications include coxa vara, nonunion, and premature physeal arrest.
Keywords
Femoral neck fractures, Fracture fixation, Avascular osteonecrosis
Figures
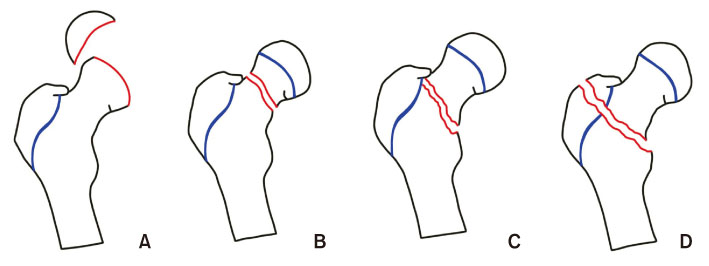
Fig. 1
Delbet classification of pediatric femur neck fractures. (A) Type I, transepiphyseal fracture. (B) Type II, transcervical fracture. (C) Type III, cervicotrochanteric fracture. (D) Type IV, intertrochanteric fracture.
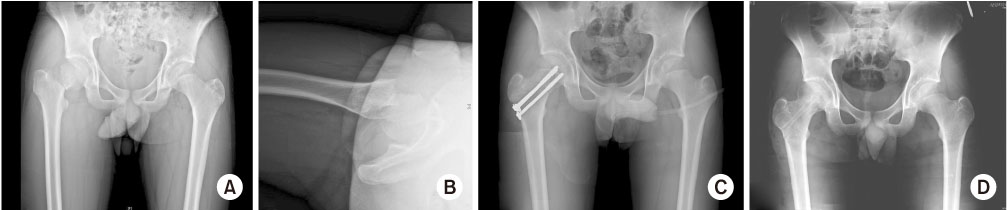
Fig. 2
(A) Anteroposterior radiograph of the 12-year-old boy who sustained a Delbet II femoral neck fracture. (B) Axial radiograph. (C) Radiograph after closed reduction and internal fixation with three cannulated screws inserted through physis. (D) Radiograph at one year after surgery showing union without complication.
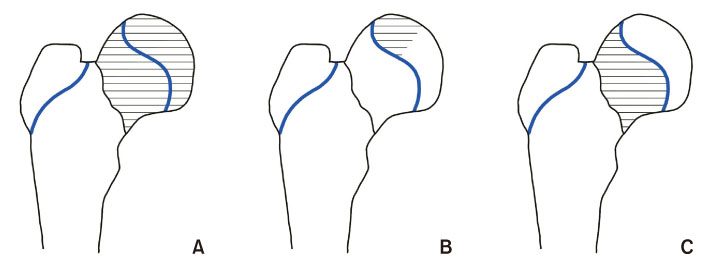
Fig. 3
Ratliff classification of avascular necrosis after femur neck fracture. (A) Type I, involvement of the whole head. (B) Type II, partial involvement of head. (C) Type III, area of necrosis in the femoral neck from fracture line to physis.
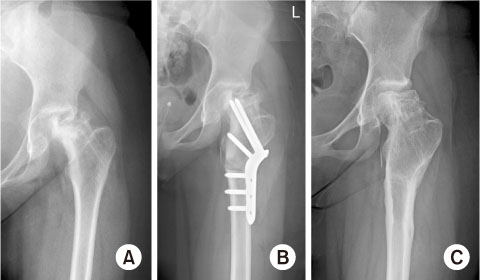
Fig. 4
(A) Anteroposterior radiograph of the 11-year-old girl who developed avascular necrosis after a femur neck fracture. (B) Vagus osteotomy and internal fixation with plate were performed. (C) Five years postoperative radiographs that demonstrate partial remodeling of the femoral head.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Ratliff AH. Fractures of the neck of the femur in children. J Bone Joint Surg Br 1962;44:528–542.
-
-
Patterson JT, Tangtiphaiboontana J, Pandya NK. Management of pediatric femoral neck fracture. J Am Acad Orthop Surg 2018;26:411–419.
-
-
Edgren W. Coxa plana. A clinical and radiological investigation with particular reference to the importance of the metaphyseal changes for the final shape of the proximal part of the femur. Acta Orthop Scand Suppl 1965;Suppl 84:1–129.
-
-
Hansman CF. Appearance and fusion of ossification centers in the human skeleton. Am J Roentgenol Radium Ther Nucl Med 1962;88:476–482.
-
-
Hughes LO, Beaty JH. Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283–292.
-
-
Trueta J. The normal vascular anatomy of the human femoral head during growth. J Bone Joint Surg Br 1957;39:358–394.
-
-
Ogden JA. Changing patterns of proximal femoral vascularity. J Bone Joint Surg Am 1974;56:941–950.
-
-
Boardman MJ, Herman MJ, Buck B, Pizzutillo PD. Hip fractures in children. J Am Acad Orthop Surg 2009;17:162–173.
-
-
Ehlinger M, Moser T, Adam P, et al. Early prediction of femoral head avascular necrosis following neck fracture. Orthop Traumatol Surg Res 2011;97:79–88.
-
-
Spence D, DiMauro JP, Miller PE, Glotzbecker MP, Hedequist DJ, Shore BJ. Osteonecrosis after femoral neck fractures in children and adolescents: analysis of risk factors. J Pediatr Orthop 2016;36:111–116.
-
-
Bali K, Sudesh P, Patel S, Kumar V, Saini U, Dhillon MS. Pediatric femoral neck fractures: our 10 years of experience. Clin Orthop Surg 2011;3:302–308.
-
-
Mirdad T. Fractures of the neck of femur in children: an experience at the Aseer Central Hospital, Abha, Saudi Arabia. Injury 2002;33:823–827.
-
-
Bagatur AE, Zorer G. Complications associated with surgically treated hip fractures in children. J Pediatr Orthop B 2002;11:219–228.
-
-
Cheng JC, Tang N. Decompression and stable internal fixation of femoral neck fractures in children can affect the outcome. J Pediatr Orthop 1999;19:338–343.
-
-
Dial BL, Lark RK. Pediatric proximal femur fractures. J Orthop 2018;15:529–535.
-
-
Iwata T, Nozawa S, Dohjima T, et al. The value of T1-weighted coronal MRI scans in diagnosing occult fracture of the hip. J Bone Joint Surg Br 2012;94:969–973.
-
-
Lam SF. Fractures of the neck of the femur in children. J Bone Joint Surg Am 1971;53:1165–1179.
-
-
Yeranosian M, Horneff JG, Baldwin K, Hosalkar HS. Factors affecting the outcome of fractures of the femoral neck in children and adolescents: a systematic review. Bone Joint J 2013;95:135–142.
-
-
Akahane T, Fujioka F, Shiozawa R. A transepiphyseal fracture of the proximal femur combined with a fracture of the mid-shaft of ipsilateral femur in a child: a case report and literature review. Arch Orthop Trauma Surg 2006;126:330–334.
-
-
Moon ES, Mehlman CT. Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta-analysis of 360 cases. J Orthop Trauma 2006;20:323–329.
-
-
Drake JK, Meyers MH. Intracapsular pressure and hemarthrosis following femoral neck fracture. Clin Orthop Relat Res 1984;(182):172–176.
-
-
Dendane MA, Amrani A, El Alami ZF, El Medhi T, Gourinda H. Displaced femoral neck fractures in children: are complications predictable? Orthop Traumatol Surg Res 2010;96:161–165.
-
-
Stone JD, Hill MK, Pan Z, Novais EN. Open reduction of pediatric femoral neck fractures reduces osteonecrosis risk. Orthopedics 2015;38:e983–e990.
-
-
Panigrahi R, Sahu B, Mahapatra AK, Palo N, Priyadarshi A, Biswal MR. Treatment analysis of paediatric femoral neck fractures: a prospective multicenter theraupetic study in Indian scenario. Int Orthop 2015;39:1121–1127.
-
-
Ng GP, Cole WG. Effect of early hip decompression on the frequency of avascular necrosis in children with fractures of the neck of the femur. Injury 1996;27:419–421.
-
-
Bukva B, Abramović D, Vrgoć G, et al. Femoral neck fractures in children and the role of early hip decompression in final outcome. Injury 2015;46 Suppl 6:S44–S47.
-
-
Eberl R, Singer G, Ferlic P, Weinberg AM, Hoellwarth ME. Post-traumatic coxa vara in children following screw fixation of the femoral neck. Acta Orthop 2010;81:442–445.
-
-
Forster NA, Ramseier LE, Exner GU. Undisplaced femoral neck fractures in children have a high risk of secondary displacement. J Pediatr Orthop B 2006;15:131–133.
-
-
Kishan S, Upasani V, Mahar A, et al. Biomechanical stability of single-screw versus two-screw fixation of an unstable slipped capital femoral epiphysis model: effect of screw position in the femoral neck. J Pediatr Orthop 2006;26:601–605.
-
-
Lark RK, Dial BL, Alman BA. Complications after pediatric hip fractures: evaluation and management. J Am Acad Orthop Surg 2020;28:10–19.
-
-
Forlin E, Guille JT, Kumar SJ, Rhee KJ. Complications associated with fracture of the neck of the femur in children. J Pediatr Orthop 1992;12:503–509.
-
-
Taylor KF, McHale KA. Percutaneous pin fixation of a femoral neck fracture complicated by deep infection in a 12-year-old boy. Am J Orthop (Belle Mead NJ) 2002;31:408–412.
-
 Cite
Cite- Related articles

