 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 34(3); 2021 > Article
- Original Article Comparison of the Results between Plating and Intramedullary Nailing for Ipsilateral Fibular Fractures in Pilon Fractures
- Yong Jin Cho, Jun Young Lee, Jae Hwan Lim, Je Hong Ryu, Jung Ho Lee
-
Journal of Musculoskeletal Trauma 2021;34(3):97-104.
DOI: https://doi.org/10.12671/jkfs.2021.34.3.97
Published online: July 31, 2021
Department of Orthopedic Surgery, School of Medicine, Chosun University, Gwangju, Korea
- 793 Views
- 3 Download
- 0 Crossref
- 0 Scopus
Abstract
Purpose
To compare the results between plating and intramedullary nailing for ipsilateral fibular fractures in pilon fractures.
Materials and Methods
Among 124 patients with pilon fractures from November 2008 to March 2019, 50 patients with a fibular fracture were studied retrospectively and divided into two groups: Group A using a plate and Group B using a Rush pin. The radiological tests confirmed the fracture pat-terns (Rüedi–Allgöwer classification, AO/OTA classification) and evaluated the degree of reduction of fibular and tibial fractures after surgery. The American Orthopaedic Foot & Ankle Society (AOFAS) was examined for a clinical evaluation, and the complications were checked.
Results
The two groups showed similar distributions in gender, age, injury mechanism, diabetes, smoking, mean follow-up period, Rüedi–Allgöwer classification, AO/OTA classification, and open fracture.
The fibular fractures were classified as simple, wedge, multiple, and segmental, showing significant differences between the two groups (p=0.03). There was no difference in the Talocrural angle, Shenton line, and Dime sign. In the reduction of pilon fractures, the appropriate reduction was obtained in 22 cases (88.0%) for both groups. The AOFAS averaged 83.24 in Group A and 80.44 points in Group B, showing no significant difference in complications (nonunion, malunion, infection, and arthritis).
Conclusion
Regardless of how the fibular fracture was fixed, the reduction of pilon fractures in both groups showed good results. Both intramedullary nail and plate fixation could be a suitable fixation method for ipsilateral fibular fractures with a low risk of shortening in pilon fractures.
J Korean Fract Soc. 2021 Jul;34(3):97-104. Korean.
Published online Jul 23, 2021.
https://doi.org/10.12671/jkfs.2021.34.3.97
Published online Jul 23, 2021.
https://doi.org/10.12671/jkfs.2021.34.3.97
Copyright © 2021 The Korean Fracture Society. All rights reserved.
Original Article
Comparison of the Results between Plating and Intramedullary Nailing for Ipsilateral Fibular Fractures in Pilon Fractures
Yong Jin Cho , M.D.,
Jun Young Lee, M.D.,
Jae Hwan Lim, M.D.,
Je Hong Ryu, M.D.
and Jung Ho Lee, M.D.
, M.D.,
Jun Young Lee, M.D.,
Jae Hwan Lim, M.D.,
Je Hong Ryu, M.D.
and Jung Ho Lee, M.D.
, M.D.,
Jun Young Lee, M.D.,
Jae Hwan Lim, M.D.,
Je Hong Ryu, M.D.
and Jung Ho Lee, M.D.
Abstract
Purpose
To compare the results between plating and intramedullary nailing for ipsilateral fibular fractures in pilon fractures.
Materials and Methods
Among 124 patients with pilon fractures from November 2008 to March 2019, 50 patients with a fibular fracture were studied retrospectively and divided into two groups: Group A using a plate and Group B using a Rush pin. The radiological tests confirmed the fracture patterns (Rüedi-Allgöwer classification, AO/OTA classification) and evaluated the degree of reduction of fibular and tibial fractures after surgery. The American Orthopaedic Foot & Ankle Society (AOFAS) was examined for a clinical evaluation, and the complications were checked.
Results
The two groups showed similar distributions in gender, age, injury mechanism, diabetes, smoking, mean follow-up period, Rüedi-Allgöwer classification, AO/OTA classification, and open fracture. The fibular fractures were classified as simple, wedge, multiple, and segmental, showing significant differences between the two groups (p=0.03). There was no difference in the Talocrural angle, Shenton line, and Dime sign. In the reduction of pilon fractures, the appropriate reduction was obtained in 22 cases (88.0%) for both groups. The AOFAS averaged 83.24 in Group A and 80.44 points in Group B, showing no significant difference in complications (nonunion, malunion, infection, and arthritis).
Conclusion
Regardless of how the fibular fracture was fixed, the reduction of pilon fractures in both groups showed good results. Both intramedullary nail and plate fixation could be a suitable fixation method for ipsilateral fibular fractures with a low risk of shortening in pilon fractures.
Keywords
Pilon fracture, Fibular fracture, Intramedullary nail
Figures
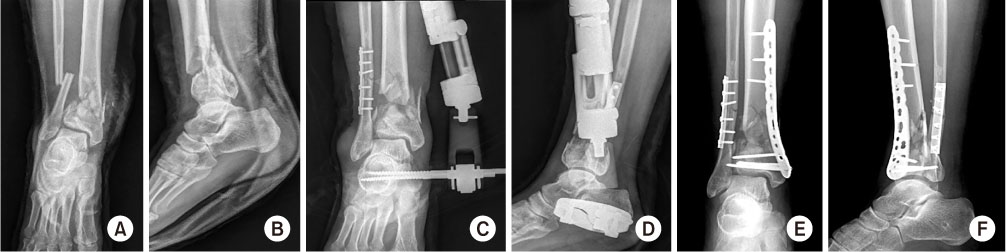
Fig. 1
A 44-year-old man in Group A, preoperative simple radiology (A: anterolateral view, B: lateral view), postoperative radiology after a primary emergency operation with external fixation for the tibia Pilon fracture and plate fixation for a fibular fracture (C: anterolateral view, D: lateral view), postoperative radiology after a secondary operation with internal fixation for a tibia pilon fracture (E: anterolateral view, F: lateral view).
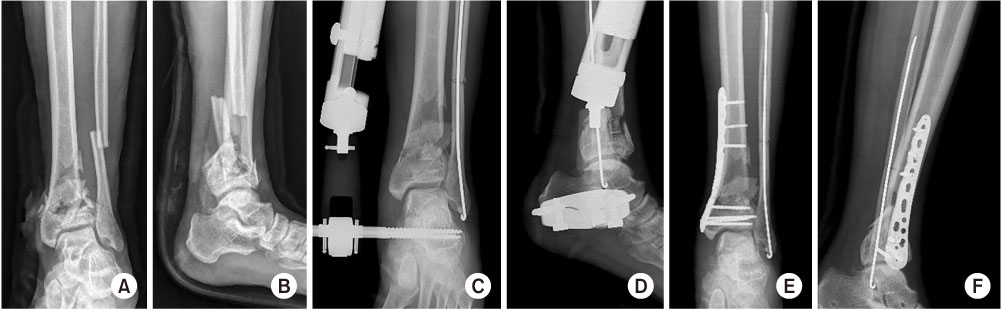
Fig. 2
A 55-year-old man in Group B, preoperative simple radiology (A: anterolateral view, B: lateral view), postoperative radiology after a primary emergency operation with external fixation for a tibia pilon fracture and Rush pin fixation for fibular fracture (C: anterolateral view, D: lateral view), postoperative radiology after a secondary operation with internal fixation for tibia pilon fracture (E: anterolateral view, F: lateral view).

Fig. 3
(A) Fibular displacement (black solid line). The distance from the tip of fibula to the fracture (black dotted line). (B) Talocrural angle (white solid line), Dime sign (white circle), Shenton line (black dotted line), Medial clear space (black solid line). (C) Fibula minus, vertical distance between the horizontal line drawn from the distal tip of the fibula and the horizontal line drawn from the apex of the lateral process of the talus. (D) Reduction of a pilon fracture, varus or valgus deformity (black solid line), joint incongruent (black dotted line).
Tables
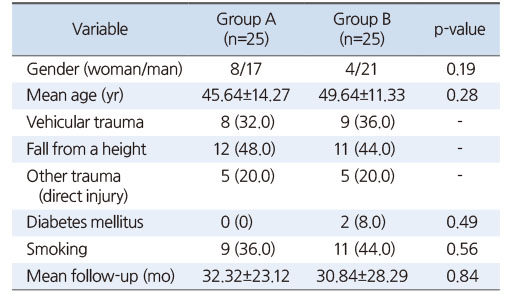
Table 1
Preoperative Demographics in the Two Groups
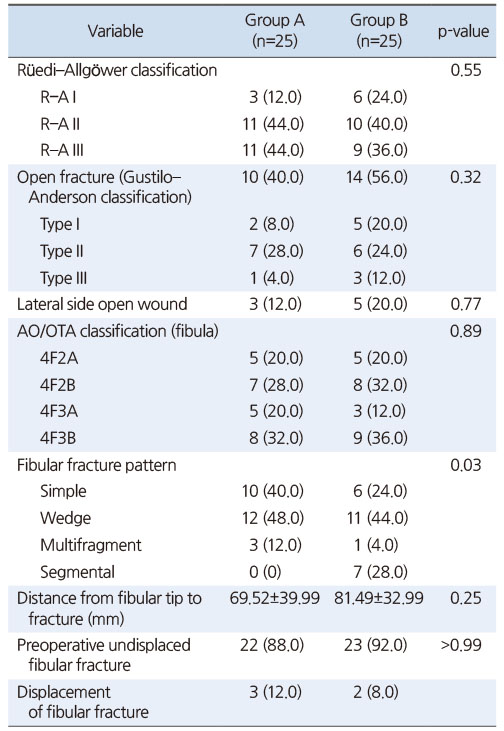
Table 2
Preoperative Radiologic Assessment in the Two Groups
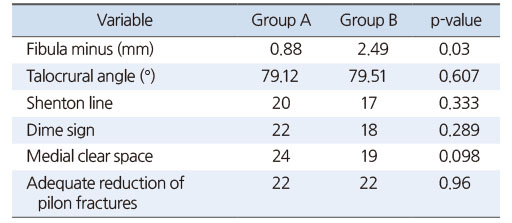
Table 3
Radiological Results in the Two Groups
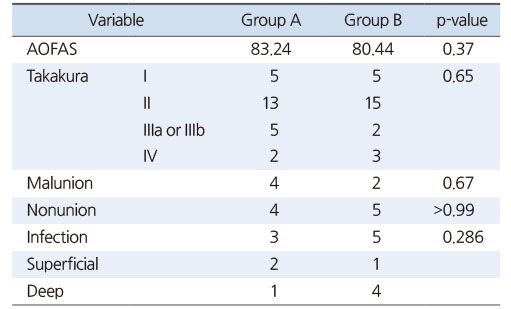
Table 4
Clinical Results and Complications in the Two Groups
References
-
Sirkin M, Sanders R, DiPasquale T, Herscovici D Jr. A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 2004;18(8 Suppl):S32–S38.
-
-
Patterson MJ, Cole JD. Two-staged delayed open reduction and internal fixation of severe pilon fractures. J Orthop Trauma 1999;13:85–91.
-
-
Leung F, Kwok HY, Pun TS, Chow SP. Limited open reduction and Ilizarov external fixation in the treatment of distal tibial fractures. Injury 2004;35:278–283.
-
-
Topliss CJ, Jackson M, Atkins RM. Anatomy of pilon fractures of the distal tibia. J Bone Joint Surg Br 2005;87:692–697.
-
-
Mandracchia VJ, Evans RD, Nelson SC, Smith KM. Pilon fractures of the distal tibia. Clin Podiatr Med Surg 1999;16:743–767.
-
-
Rüedi TP, Allgöwer M, et al. The operative treatment of intra-articular fractures of the lower end of the tibia. Clin Orthop Relat Res 1979;138:105–110.
-
-
Babis GC, Vayanos ED, Papaioannou N, Pantazopoulos T. Results of surgical treatment of tibial plafond fractures. Clin Orthop Relat Res 1997;341:99–105.
-
-
Lee YS, Chen SW, Chen SH, Chen WC, Lau MJ, Hsu TL. Stabilisation of the fractured fibula plays an important role in the treatment of pilon fractures: a retrospective comparison of fibular fixation methods. Int Orthop 2009;33:695–699.
-
-
Chen SH, Wu PH, Lee YS. Long-term results of pilon fractures. Arch Orthop Trauma Surg 2007;127:55–60.
-
-
Pollak AN, McCarthy ML, Bess RS, Agel J, Swiontkowski MF. Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893–1900.
-
-
Williams TM, Marsh JL, Nepola JV, DeCoster TA, Hurwitz SR, Bonar SB. External fixation of tibial plafond fractures: is routine plating of the fibula necessary? J Orthop Trauma 1998;12:16–20.
-
-
Asloum Y, Bedin B, Roger T, Charissoux JL, Arnaud JP, Mabit C. Internal fixation of the fibula in ankle fractures: a prospective, randomized and comparative study: plating versus nailing. Orthop Traumatol Surg Res 2014;100(4 Suppl):S255–S259.
-
-
Smith G, Mackenzie SP, Wallace RJ, Carter T, White TO. Biomechanical comparison of intramedullary fibular nail versus plate and screw fixation. Foot Ankle Int 2017;38:1394–1399.
-
-
White TO, Bugler KE, Appleton P, Will E, McQueen MM, Court-Brown CM. A prospective randomised controlled trial of the fibular nail versus standard open reduction and internal fixation for fixation of ankle fractures in elderly patients. Bone Joint J 2016;98-B:1248–1252.
-
-
Switaj PJ, Fuchs D, Alshouli M, et al. A biomechanical comparison study of a modern fibular nail and distal fibular locking plate in AO/OTA 44C2 ankle fractures. J Orthop Surg Res 2016;11:100.
-
-
Saad BN, Yingling JM, Liporace FA, Yoon RS. Pilon fractures: challenges and solutions. Orthop Res Rev 2019;11:149–157.
-
-
Sarkisian JS, Cody GW. Closed treatment of ankle fractures: a new criterion for evaluation - a review of 250 cases. J Trauma 1976;16:323–326.
-
-
Morris M, Chandler RW. Fractures of the ankle. Tech Orthop 1987;2:10–19.
-
-
Weber BG, Simpson LA. Corrective lengthening osteotomy of the fibula. Clin Orthop Relat Res 1985;199:61–67.
-
-
Panchbhavi VK, Gurbani BN, Mason CB, Fischer W. Radiographic assessment of fibular length variance: the case for “fibula minus”. J Foot Ankle Surg 2018;57:91–94.
-
-
Conroy J, Agarwal M, Giannoudis PV, Matthews SJ. Early internal fixation and soft tissue cover of severe open tibial pilon fractures. Int Orthop 2003;27:343–347.
-
-
Takakura Y. [Diagnosis and treatment of ligamentous injuries of the ankle]. Nihon Seikeigeka Gakkai Zasshi 1990;64:1111–1126.Japanese.
-
-
Teeny SM, Wiss DA. Open reduction and internal fixation of tibial plafond fractures. Variables contributing to poor results and complications. Clin Orthop Relat Res 1993;292:108–117.
-
-
McLennan JG, Ungersma JA. A new approach to the treatment of ankle fractures. The Inyo nail. Clin Orthop Relat Res 1986;213:125–136.
-
-
Lee YS, Huang HL, Lo TY, Huang CR. Lateral fixation of AO type-B2 ankle fractures in the elderly: the Knowles pin versus the plate. Int Orthop 2007;31:817–821.
-
-
Phillips WA, Schwartz HS, Keller CS, et al. A prospective, randomized study of the management of severe ankle fractures. J Bone Joint Surg Am 1985;67:67–78.
-
-
Bear J, Rollick N, Helfet D. Evolution in management of tibial pilon fractures. Curr Rev Musculoskelet Med 2018;11:537–545.
-
 Cite
Cite
