 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 32(1); 2019 > Article
- Original Article Surgical Outcomes of the Monteggia Type 2 Fracture Dislocation in Adults
- Sung Choi, Daegeun Jeong, Youngsoo Byun, Taehoe Gu, Sungsoo Ha, Dongju Shin
-
Journal of Musculoskeletal Trauma 2019;32(1):6-13.
DOI: https://doi.org/10.12671/jkfs.2019.32.1.6
Published online: January 31, 2019
1Department of Orthopaedic Surgery, Daegu Fatima Hospital, Daegu, Korea. osaabga@gmail.com
2Department of Orthopaedic Surgery, Gyeongsan Joongang Hospital, Gyeongsan, Korea.
2Department of Orthopaedic Surgery, Gyeongsan Joongang Hospital, Gyeongsan, Korea.
- 1,491 Views
- 7 Download
- 0 Crossref
- 0 Scopus
Abstract
PURPOSE
This study examined clinical outcomes of Monteggia fracture type 2, which is the most common in adults with a high rate of accompanied injuries.
MATERIALS AND METHODS
From June 2004 to November 2015, a retrospective study was performed on 12 patients diagnosed with Monteggia fracture type 2 with a follow-up period of at least 6 months after surgery. The clinical outcomes were evaluated using the Mayo elbow performance score (MEPS), and the existence of accompanied injures, radiological result, and complications were analyzed.
RESULTS
Posterior instability was confirmed in all patients and accompanied fractures were detected in 9 patients (75.0%) on the radial head, whereas 10 patients (83.3%) were found on the coronoid process. The average arc of motion was 107° (70°–130°) and the mean MEPS was 89 (45–100). Additional re-operation due to re-dislocation, radioulnar synostosis, elbow instability, ulna nonunion, and radial head nonunion were performed in 4 cases (33.3%).
CONCLUSION
The Monteggia fracture type 2 is more commonly associated with radial head fractures and coronoid process fractures rather than other types, which causes elbow instability. Because the rate of additional surgery due to complications is high, the treatment of Monteggia fracture type 2 requires careful assessments.
J Korean Fract Soc. 2019 Jan;32(1):6-13. Korean.
Published online Jan 25, 2019.
https://doi.org/10.12671/jkfs.2019.32.1.6
Published online Jan 25, 2019.
https://doi.org/10.12671/jkfs.2019.32.1.6
Copyright © 2019 The Korean Fracture Society. All rights reserved.
Original Article
Surgical Outcomes of the Monteggia Type 2 Fracture Dislocation in Adults
Sung Choi , M.D.,
Daegeun Jeong, M.D.,*
Youngsoo Byun, M.D., Ph.D.,
Taehoe Gu, M.D.,
Sungsoo Ha, M.D.
and Dongju Shin, M.D., M.S.
, M.D.,
Daegeun Jeong, M.D.,*
Youngsoo Byun, M.D., Ph.D.,
Taehoe Gu, M.D.,
Sungsoo Ha, M.D.
and Dongju Shin, M.D., M.S.
, M.D.,
Daegeun Jeong, M.D.,*
Youngsoo Byun, M.D., Ph.D.,
Taehoe Gu, M.D.,
Sungsoo Ha, M.D.
and Dongju Shin, M.D., M.S.
Abstract
Purpose
This study examined clinical outcomes of Monteggia fracture type 2, which is the most common in adults with a high rate of accompanied injuries.
Materials and Methods
From June 2004 to November 2015, a retrospective study was performed on 12 patients diagnosed with Monteggia fracture type 2 with a follow-up period of at least 6 months after surgery. The clinical outcomes were evaluated using the Mayo elbow performance score (MEPS), and the existence of accompanied injures, radiological result, and complications were analyzed.
Results
Posterior instability was confirmed in all patients and accompanied fractures were detected in 9 patients (75.0%) on the radial head, whereas 10 patients (83.3%) were found on the coronoid process. The average arc of motion was 107° (70°–130°) and the mean MEPS was 89 (45–100). Additional re-operation due to re-dislocation, radioulnar synostosis, elbow instability, ulna nonunion, and radial head nonunion were performed in 4 cases (33.3%).
Conclusion
The Monteggia fracture type 2 is more commonly associated with radial head fractures and coronoid process fractures rather than other types, which causes elbow instability. Because the rate of additional surgery due to complications is high, the treatment of Monteggia fracture type 2 requires careful assessments.
Keywords
Elbow, Ulna, Radius, Olecranon process, Monteggia's fracture, Fracture dislocation
Figures
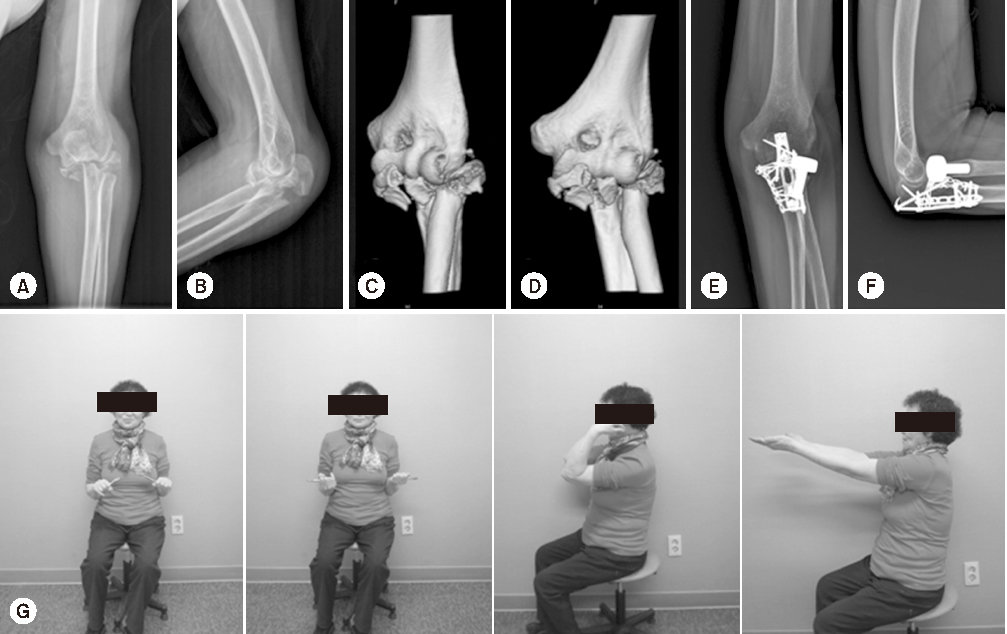
Fig. 1
A 66-year-old woman fell on the ground and injured her left elbow (Jupiter's Type 2A fracture dislocation associated with a radial head fracture and coronoid process fracture). (A) Initial anteroposterior. (B) Initial lateral view. (C, D) Three-dimensional computed tomography. (E) Anteroposterior view 32 months after the open reduction and internal fixation of ulna, replacement of the radial head and repair of medial collateral ligament & lateral collateral ligament. (F) Lateral view 32 months after surgery. (G) On the last follow-up, 32 months after surgery, range of motion=10°–125°, Mayo elbow performance score=100 (excellent).

Fig. 2
A 39-year-old woman fell from a height and injured her left elbow (Jupiter's Type 2C fracture dislocation associated with radial head fracture). (A) Initial anteroposterior & lateral views. (B) Postoperative anteroposterior & lateral views after open reduction and internal fixation & radial head excision. (C) Metal failure 3 months after surgery. (D) Postoperative anteroposterior & lateral views after 2nd surgery. On the last follow-up at 57 months after 2nd surgery, range of motion=20°–100°, Mayo elbow performance score=75 (good) with elbow instability.
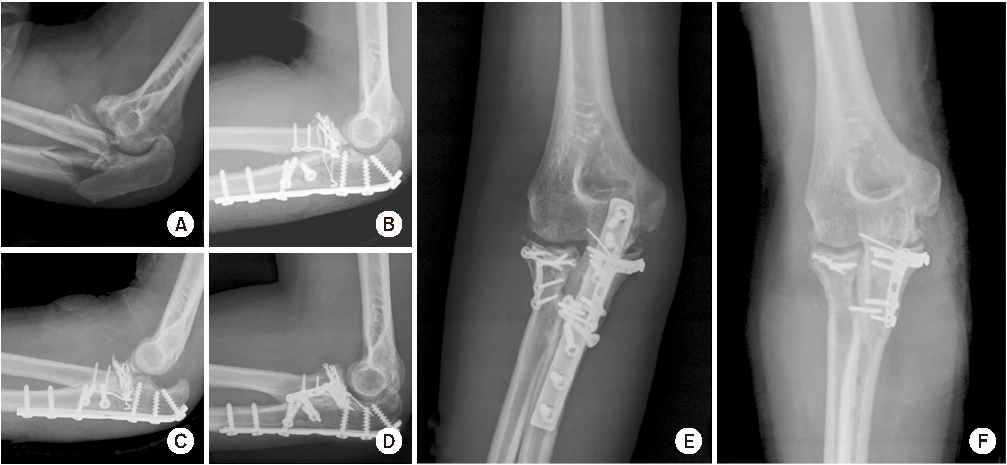
Fig. 3
A 22-year-old woman fell from a height and injured her right elbow (Jupiter's Type 2D fracture dislocation associated with the radial head fracture and coronoid process fracture). (A) Initial lateral view. (B) Postoperative lateral view. (C) Lateral view 3 weeks after surgery (instability of elbow joint). (D) Postoperative lateral view after the 2nd surgery (additional plate fixation at coronoid process). (E) Radioulnar synostosis 18 months after the 2nd surgery. (F) Postoperative anteroposterior view after the 3rd surgery (ostectomy & partial implant removal). On the last follow-up of 25 months after the first surgery and range of motion=10°–120°, Mayo elbow performance score=95 (excellent).

Fig. 4
A 40-year-old man injured by a motor cycle traffic accident and injured his right elbow (Jupiter's Type 2C fracture dislocation associated with lateral ulnar collateral ligament rupture). (A) Initial anteroposterior & lateral views. (B) Postoperative anteroposterior & lateral views after open reduction and internal fixation. (C) Elbow instability 9 days after surgery. (D) Reconstruction of the lateral ulnar collateral ligament with palmaris longus tendon & postoperative anteroposterior & lateral views after 2nd surgery. On the last follow-up 34 months after the 2nd surgery, range of motion=20°–126°, Mayo elbow performance score=100 (excellent).
Tables
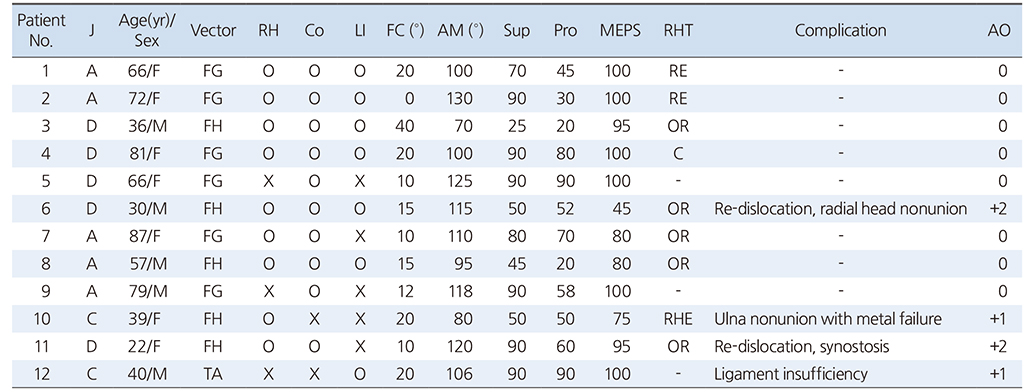
Table 1
Demographics of the Patients
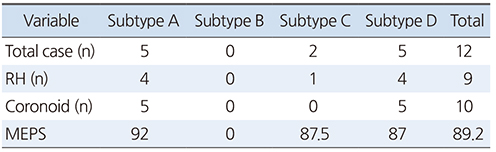
Table 2
Jupiter's Subclassification
Notes
Financial support:None.
Conflict of interests:None.
References
-
Bado JL. The Monteggia lesion. Clin Orthop Relat Res 1967;50:71–86.
-
-
Ring D, Jupiter JB, Simpson NS. Monteggia fractures in adults. J Bone Joint Surg Am 1998;80:1733–1744.
-
-
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM. The posterior Monteggia lesion. J Orthop Trauma 1991;5:395–402.
-
-
Ring D, Jupiter JB. Fracture-dislocation of the elbow. Hand Clin 2002;18:55–63.
-
-
Kamali M. Monteggia fracture. Presentation of an unusual case. J Bone Joint Surg Am 1974;56:841–843.
-
-
Wong JC, Getz CL, Abboud JA. Adult Monteggia and olecranon fracture dislocations of the elbow. Hand Clin 2015;31:565–580.
-
-
Reynders P, De Groote W, Rondia J, Govaerts K, Stoffelen D, Broos PL. Monteggia lesions in adults. A multicenter Bota study. Acta Orthop Belg 1996;62 Suppl 1:78–83.
-
-
Konrad GG, Kundel K, Kreuz PC, Oberst M, Sudkamp NP. Monteggia fractures in adults: long-term results and prognostic factors. J Bone Joint Surg Br 2007;89:354–360.
-
-
Boyd HB, Boals JC. The Monteggia lesion. A review of 159 cases. Clin Orthop Relat Res 1969;66:94–100.
-
-
Egol KA, Tejwani NC, Bazzi J, Susarla A, Koval KJ. Does a Monteggia variant lesion result in a poor functional outcome?: a retrospective study. Clin Orthop Relat Res 2005;438:233–238.
-
-
Bruce HE, Harvey JP, Wilson JC Jr. Monteggia fractures. J Bone Joint Surg Am 1974;56:1563–1576.
-
-
Givon U, Pritsch M, Levy O, Yosepovich A, Amit Y, Horoszowski H. Monteggia and equivalent lesions. A study of 41 cases. Clin Orthop Relat Res 1997;(337):208–215.
-
-
Strauss EJ, Tejwani NC, Preston CF, Egol KA. The posterior Monteggia lesion with associated ulnohumeral instability. J Bone Joint Surg Br 2006;88:84–89.
-
-
Biyani A, Olscamp AJ, Ebraheim NA. Complications in the management of complex Monteggia-equivalent fractures in adults. Am J Orthop (Belle Mead NJ) 2000;29:115–118.
-
-
Llusà Perez M, Lamas C, Martínez I, Pidemunt G, Mir X. Monteggia fractures in adults. Review of 54 cases. Chir Main 2002;21:293–297.
-
-
Karbach LE, Elfar J. Elbow instability: anatomy, biomechanics, diagnostic maneuvers, and testing. J Hand Surg Am 2017;42:118–126.
-
-
O'Driscoll SW. Classification and evaluation of recurrent instability of the elbow. Clin Orthop Relat Res 2000;(370):34–43.
-
-
Ring D, Hannouche D, Jupiter JB. Surgical treatment of persistent dislocation or subluxation of the ulnohumeral joint after fracture-dislocation of the elbow. J Hand Surg Am 2004;29:470–480.
-
-
Matar HE, Akimau PI, Stanley D, Ali AA. Surgical treatment of Monteggia variant fracture dislocations of the elbow in adults: surgical technique and clinical outcomes. Eur J Orthop Surg Traumatol 2017;27:599–605.
-
-
Regan W, Morrey B. Fractures of the coronoid process of the ulna. J Bone Joint Surg Am 1989;71:1348–1354.
-
-
Steinmann SP. Coronoid process fracture. J Am Acad Orthop Surg 2008;16:519–529.
-
 PubReader
PubReader Cite
Cite
