 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 32(1); 2019 > Article
- Case Report Pseudoaneurysm of the Anterior Tibial Artery after Reduction with Pointed Bone Reduction Forceps on a Spiral Fracture of the Distal Tibia: A Case Report
- Hyunseung Yoo, Youngho Cho, Seongmun Hwang
-
Journal of Musculoskeletal Trauma 2019;32(1):43-46.
DOI: https://doi.org/10.12671/jkfs.2019.32.1.43
Published online: January 31, 2019
Department of Orthopaedic Surgery, Daegu Fatima Hospital, Daegu, Korea. femur1973@gmail.com �����JFIF���d�d�����Ducky�����d����qhttp://ns.adobe.com/xap/1.0/� ���Adobe�d���������������������������
�����������
����! 1AQa"q�
2#w8���B3��6v�7�X�Rr�$�9��b�C��t%u&��W��s'(xy���4T�5f���H����
�!1AQaq"���2B ��Rbr#��u67�Ѳ3sTt5v8���Sc$4Ă��C�Ô�%U���Ӆ�FV����
��?����������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������_A���נ�j-
�H���>�>�,�m*>
��
���fzp"�����T������r�Kkr����^����r.�����������������������������������������������������������������������������������������������������������|_&��]�|*��v�P��uܶv�o���Q�1������m
��w�VJU�hu-�I�"=L��n���i��Aƕ8���"�۲����
�k�*ҿ[y�u:�.��v�U���Q +�)��%F� D�Hy�V���B� ��k�>�H�y8��j�ݹ
q~�9D��4�KR��m�z���Q����)�^ʔ�.J%k_tVi5NT��jg!'�k��y|5as����O��Ȼ)R��۸ߩFMԿ3L�4�j�6d��ڜ#�NIw UF��]J��q�B���/(�F�a��fJ�Rzq3�\G՛�
?
�~\�
6�)6���W��4�m[O�
�^L0�E�&r�RM�ض*���C
.��]Un�l��-1�
1�r#Rj/����&QɈ˩��s6�Rj=5Tg�.��y�.·Pӡ:�JJ�S���
:��C8��-���2u]�d�&����v���U�z;��7p�
9���
5V��nL֢����"y)��">�iי�(�IDDd|���
Yj0��;
L���R�f����S��:k����tY�K%*�N2^�m�|&dğ
th�":���e��y�)u�P���Q��Z��W)gcC3Pv&�M���M���W���d&�Ŵ�۲��mv �T��Ro�ժM0�3�*�F
3Y��d������ 6����\8�,�\h�ݻ
kߔ���i��<
k� ��NT��wS�Ԫ���mlj���j[>->�p�������������������������������������������������������������������������������������������������������tU���%�'�
L�R>&E�B��H$�
����
�MQAU�x[�$Z6���v��i&�_�a.K�IQ{�h�yƒ�
�j"J�OC���9����e�F��ҝ����f�j���;�˚Ω<[3�_m%����
��l��Q@��4���g���=5$��(J]Y���c-OMq�<����Ǎ��
wS�����z����
ڗ)k�$
��7
�V�I���P�붾ͯnV+卵*t]i�ЎD�31��~S�A��1�
é�C�2u)��ʼn���Qn-U�o�i�3�:��g��rI8���ؓWm*G
z�ܕ)Z�קJ}��
Y� Y�lGeJ6�cB2I �NS3�Q�>k���=KT�� �B�����T]����W�
�����6����+�S�������O��X�QgG�R�?
te�l�ˊ%��-R�e\hѯ2TF�"��C/�O��JΩ��6���r�[N�.0��{����S��pljjX��1�jOs�ӥ;ҭhe}�x�u`�Ք �&�.���)y��O̒
�F�ߑ.$���Qw�;�9�����I�w2o+R��V�JMS�Oj[SoҌ�Z%�;��`d$�b���l�Q{Ro{�Imڌ>3�e�gf��\O�֝U�z��x��"䢸g+mv%G��������ʆ:|V�[N��'&ס-ޝ�'��k��fE�|K���
,G&˳98�J�u�i�n���/����\\Qݿ�̋v�~�����Ǩ!r��t���WU� ��d����|�E��߫R�� 4d�}.��q���Pw*Ӭv5YE���c�n��������~��f5�c�%M�T�M�k��b-F�>�5��JT���,�}�)�
Q��H�g�%�{("Ӕ�ȸ�W�MsY�y�W��NR��rkk��J�r���0�X�ドnͫ�T������ }�r�-j�j,�Ŕʍ\�Q�2Ri>v$5�!�]"�J��B���2����WɅ�)]V�Ԝ�U��c8��i�|��.�j�e�<�X��7��T�=�r[{w�Ol���TUv*�jp��m��8�KŎ}�Xu*A��H�:&�oZ�ljQj�m�����u�C;N���w
ko�ػ@��}_@�*�>�R�O�6�^�V.�����������������������������������������������������������������������������������������������������¸���
��Q�&��#|�ܶ-*�u��O���G%�JA�t��RZR��r]F�FG��\۩���w+?'zչS����ѧ��t
jz�>
�KW&���ot�{7�P�&�2D�;&\�\�����>�Q����2J�zܗ�A�KS����fe�Nn��[��jRr��ԕ�f6,q,F1�t�R�fԗ�>vֶև���j�-�&���R
'�Z��i2=xv���~E�l��bs�vm8������=ӛ"ūB����ȩl�Wa�u[�]ٷ��B��ߨF~�J�!|���I��p���r3�R̴#Y��p)={7�:G{+:\W�}�n�|Q�#%��)7^-�h��
"Ƒ��q���:M*%J�&�$�T軨�I333�g��_�-
��u���c B
�ww������jp�[�6����i�2��5�����$̏�b��U�ٱR�v?G���\~#Iͪ��b��7�<<}��E���zt"��
����q�_��In���w��,�7-���d����������,���G�÷%T�*�
W�g��1��"��䥱�k��q/�A��.�,_���K�h����q�Œ�
x�wvo��� �u�2ۥ�����ۧ.bQ}� Xκ���A��$֣
�+K��״�ZU���NmڸI�I{.��v�{5
�z5�����Ѯ��R�m����e[m��oyƾ��������d~����c��R��ݾ���K'j.\i�&�������/�S�6�f|b�=5��:�� �p!6�i_�
4�j6�=�.s��i˧eƾ�tS�^� ��c�.�Y�^�R�����������������������������������������������������������������������������������������������������J�V��S-Vi3,esi��08�?�H$G�v���Z�gg?���gi䤟2a����dw����릿�:��"۪���l��k�S��N�>q�-4�kI��܋�ێ�e�̊�qۅ�g��DoѨ���9����;�����
#�T��. �Q���
;��7�#�~� �_U�f����s����t���b����_���'w����������~X��w1���X���k,v �cOt��._}��v}�8��"���(�4��Z��� �\��ۘg
k�?��J?��bm�����_��c�����!�g���{��HZV]��F���kk�%~��g�������E�t�)���b秴��
�v�ΰ���B��������|꽸}�m�
�p~E�6ݹ��v���;�7�P٤���v�+��r��i��*3Ԣ��|�'O14�_����~��7����n�P���{7Z�U��\Vű�[�
����+���7o#:�ǥ����Ŭ\�|3�r���%T�
JX]V7���e�z�¨Y�]��lc|O3��V!��
R��
z�b�J'PnGq��V�J"19��WV����eOF�埜E�aEJω qCN5��Z���
��g��-�9[S��<���$����s��U�K�5b|7s�n\7x
����qmv�����������##�FF\
���w�[�=-4���3$^��o�o��VSi�Xօ�v�7iB�۴y�g�>]Vf�"r�$�J3""32!�Z�h���[K������%7�G��vNL��s��+�4��n����B���/B�{vls�obJ�a�Һ���JR�:����0�g�%&�z��R\
S3���T���[�&ִ�or����*ⷳ�����c�3ʊ�O�[ioz��W�٨%�$���gn:�ܶ���WwFB����Թj�H�P���&z���
u&��F�2�\f;ip�W73��
����
[��;���
'_�̽b��;v�i��b�!oe���c�
�d��C����-tS���<���yC7K��Ƶ��۹b�W/ܻu�z���;�q�\4��R3�Mw�����~��Ga
�աn��]�U�Sv}�q�WMj<���o̺�Z�F;�Pj���(y,��� KZ�<��Ө
��ir�%�q���±��V1n�
�
�ܯY�4ݩ��T�iF�d��'��)=�oD,��S�9j:�v���]yy��bٔq��*Ź%~�C�psrn.N1�^7`�����7I���ߘ�c-5���O,}����B�O�L*u
ȧUc�ǔ�K��n$�#�B1�= �/X��Լ
Vռ}F�ܘ|�
�nܨ����j�]��2On�T�l��ye��B��r��]��4'b���
R�E�����{6�pY�nR�%��+Ce!��J������������������i�-�����/���_��H���U�g?*STKF�H�Φ�`B���C�Pj4��'�}�8����-7�������P���y��ͻn�;���0�9� [�
����N)Iʮ�K�ϗN�r?I�e�`r�&4u
�:�ܬ��.�]붡r��ާ
����B���b�U��E���Ʊ�p��pVn�Bٴ�����ܙ5'�W��ǤN�¨�[���VEU5jSl�"��#��iY����[��r���{/L�Dž����e��Jڜ�|�R�j<�m��K:Aȼ��h�M��Llb��'�����'fWa~v�]�Nӄ���5v*�
)�������������������������������������������������������������M4��m-�
{;����L�DG�C">_��_$�X�s��]�l9���&z�$�2/N��>%'�
�����[���}b�{h�/{`�{�J�i����
�YJ��B���/X%���}.|+{(�����S����:q�z���]4���_Kѵo��`���^��t�Y�_�4�����S�#*�
^��z�vݾM�r��+�T���rkQ�
g.8Ͽ�^�<��O�2���'����\\�E���w���^4��蟡z} �-dz~Q�����mkM� ����\�7�w��
���M�w�/3�/�Ǥ��^�|�W�6��lĚ�����
=��WLt��ބ� ���~�}Ve��z��֏��{���'�Q[����'�f+?��c�����b/�������I�==���d�|E�G%�����_��l�����dk�r��r?�na�u����(��O�&g�Y~�яG������,[���!iYvz�� ɭ������0M��~�b����9���3�W������Lw���:���
��������#'��;��f7m]�ɓ?]��NT���*ի-�(Ӫ��/����%�H�D���.����
̋pS����ʎ��W�u��mv������G�8~ky�����p���r�g�����I��^ń"�
�l�Hj��.o_�+��^�p����ܘ�˟Q�F�E\�0�֙�6���*�<�nT�ˮ�v�<ֿ8�G�^˙Zn=�*֓v�ƫEZO�V���y^�+~eu���V*�p���[�J���+.�t�(:UҴ1g��HN;�vE��̳Rȕs��b%��T
�[e� ݼ�R�P��\�\�yt��i>�ӈ��Ǚ��v����i��x�>�
���$o(�
�
�^��qt�*���&���t1oJ��V����u��-��q�l�5��U6��j�CЉmĻ*�"?JT���=K'��O�/�|=Vo���}l�0b}}f�?���X��[�����?
/\�J�S��Be�,�k�P��8E���T�J=��=�?.
p�5ފ��g��b�U9}���Ƕ���dNKk�����_$8�̸͓ۍ8D��i�\B���Կ-1v{FF]�|��.^��ۅ��{v��l1��2�z7-�R������7w�E?�\n�����h\�jN/Kձr_�oBw"�N
Q��M�B�Zq�
e����-m:ӨSn6�j4���%!hQ�����;sv�'�m4�kcM=���
�!8\��m�[�M4�{SMli��ۇ�%�eֽR�&N:��{2A8�)��T�HL�K3Z�j��[�jP�Bx#Bگ�Mf:�G�1\��`edcʮ�?|w�
������(�-�����̮v���X�t�,��b�������W����2�;.ι��NHRR�#��Y�wT��M�"
��<;�mk\���.f�����oI�D�j�m�lJ;v�xy7���o7i\���,�KQ�Ŋ��9d^��M�mg�c�
L�*�.T��
�6t��L�����eIuOH��3S����JQ�3=F��/�ʿ<��9�\�����JM�6��m��N6=�<{x����kP�!�F1�Q�R[�I$�6��ُim��Xu2�A�n2yԒM�U q��
���f�[��I�������B�-'��䤯jY��m�5����2���&�J�G��\���z��д�\~�v��d��g
�Qt�HG��X�w&�1���Lw+�
nD�E�dC�����1�w|YJm��vP)HZ>i��0�BP�βә?��R�:Q�O[�"��]����I_�J�ʏ��
ۍ>�Q��K�yu���^by��cB�q4lXF�~l��
[\*�N>-��J6,�G�q��(Z�r�5h�]CwY��ӤU��~ʶߑ�
����u�*
S��Iv�%���Z�f���J7�)! F����S��*s��_��\�
|I�Ÿ�Z)J
]���ܜ�i4�"��z[�����+��Z��,MOZ�)<�F�32'&����VlUlQǷi(������\�u r�ϕ"l�
�6l���.\�.)��HyKzD�,ֵ��KQ�����W�^ɽ<����E�9JRnR���)JN���m�V��K����c���j�!���J1�RJ1�IF)$�I*c��պ\Xb�h嫞�LK��2о���Ш��xf˴��ǗN7[$�o�݇(҄��D��yC�
N�œ��9�\V2�<�I5N
�r��V�nn�9Q$`�yX�OU4�as/��f��
�V�����Uv��GV�~�&��:��jݙn���.;·���ޑ
��l�$
�-���-��!JRT�i���7�)Q�n4��X��H���uc�V��cR�%o+
��7iU�*.;s^չ�U'��$�/�O��1�u�ͽR���2����²,�IJ3�Z��-�7��K�"�.D���q�6��3��jWk6��G�eK�����-j�-3`�2��Zk�B��,ȖӉQ�k�}
c����]�je���t���v��n�$�IBpjQk����y[Ѵ�`�ʚ.������j����z��pM�ܵr2��T�
���ơߍ�����?��� ��j��T����5��������
����O�������i��c+3��R�Ց��*�v-�wZ�[WX�l�w�Z�G��U�ۥ�rά\�|��JEQ�P���r�������e^{����-i|��fe�cci����W&�r�cf
����
i�Ը�K�W%(�#���_L�7����N���jy��u�?Vm�M��M�cB�7��N2MÇ<�Fۄ�/!�uU���?
�5ժ7�j��R��dXW]^C%f�ͽ.
o]�J�m
?i$��-�9r�v��ۜw��>)}�|��Ʀ���(�RUNII�I���.<��?�fӆ=�?pE�Ry���+i�a�NP�h�%(�����b�vh�9���^���?D�N�����iӦTUy]�UP��V�Ƒ5Q�6ٺ����iN�$����nq��[�
3�u]K��(cdޱKǸ��S�r�J�7D��E���
5玔kZ�:r���j��v�w7.�-�S'�ˍO~<��B��i\����?Է�2���>�˨����r�n}�M)�xx�ӕ�0��
�
eyҵ��7YMAB�]ӣ�U:/ѭ*�6��b��cwP͵
���"���+��q�ēV�j
ŹO��|G����tY�4V�
��j�[mL�V��
M
-m���>�",���B�$�
�G�D1~��j�6O�4|��L�x�nN���mqA�T�N��R�3ε��|DŽ��a����[���f��m��n���-�ڭ+F�i�K��7�P�cm�;�r�5
l�8���r{��#����-<�U��Lgd�y�|����\[F'��
ѩ�@�{�8��nR�ɕ�xi�vo5N9�'8\��$��.�����,r7/Ϭ�*�XZ=�Ў��n��ޚ�o+|(x����b�8����ۄf��d�)�F�7G���3�����G�Q�FR�R)���)��U2�|Wb@�S�D�����Yi m��II�?Q:��l.�k�X\���ó�f�ݸgeB�2n�0�cuF1�RQ�I$�I$zK��B�#�t{��=O��W'R��2�۷t�
�nݹ�bw.\��]'�nrF��h�2ruy��cb;��pW
=�njRqR��J�(��d
�mn�pc���k���N��nʹ+6�]�t�z�~E=ʕ
l ����ZZ�5�jSi3#4��7�.����Lc��fe`���9؏��v囜.��
�F\-�UZ:*�0_���<�Νu��9�Lӵm&<��qX�Ƴ�e\�F
cq[� �N*RJ\)��_�3�\�^ҹ3"���1n1v�����_|�uR�ʞͫr��'��i��ȧN�_��k�H���8���x��Xrj�=������\�М�H)�V���\�ˬ.�X�ʸ
����� oVRC�}��ySU9/��O�BY먌�5
�ٿ�w�ޞ��)��rw8Ӫ���i5*�5Z��Η�c��G�Ʊ
!Z�ۄl�mp�j�J
-�
l� <�R̵�/����J�A�պ�Zuq\������I������dUS
�� �4�8�wXJ����Jtc�g4�cI������~�aqߓ�w��ŷrm��-�v�)G�7��y��S����^���7H�^-�\��m�Ō�Aq|�"�m9�I��B�nF㏉9[N+m�m��y��/!��KK��ۉ%��n �+B�dddfFF6�FQR�N-U5�����;Sv�'�m4�kcM=������M�n���
)�\qιqUd9F���%",���6M�Gd
T%-�
�+�~
f�%+y֛^3�S���r���F>6l���c�(��֪�v�ۊ��N��;���g�.��_0��Sѧ�]
����E���T��W
�رk����Q�Kz�Ge��9��ʨs����KA"yC��
y2\��[�5
��r�ԭ�7Gk��5M���z�w���_4�s��M3��hxЊ����'���oÍ�5jsu�b�
�)�ͪ~�tR�����2�H��]�R�͍>
�̋�m�
6�=�%(˿�(��W�rr-܅�y5(�ܔ��J��Y�unW̹�븹��N��s�qK�
����]���/Q���R#�"�ZM�D�fD|4��3�Qw�|.�_ԡ�S����q���T�Z���B��g��?���?O���
���Ϥ)����/�E�_�U|i}�2
��9Z?¹ �0�:���x��'�3�,�whǣ�?��C
�y�-��A~����=d�a�������J�ј&�M?D1�_P�
��S��+���Oi�&;����a��
�@���������;�Dž�7[������ �z�Z� C"b�v:����j�jMQk�$�M
�RԸ�3u�A\��=wI����.AwC"�^�.�{��?-\����NS�iˏ"�b��}��T�/��}� �q/�
o�.
�1����
M�}R�% :�-���Z�niʒ�L$�S�g�rBW�*��,Mw�'N\�ɇ{s��\��j�]�������V�ryG��'�8f`�}���
'N�<���*/�` U숻�z�
C��wH�q�1�8���J+�vԕK�s�s�4�R�5�3/�&�����XT�t�1b�Z��Ɵ��o\�=�%��nO�)�h��$�r����B�i-�n���K
Ī������^�
���ջڜ�lwkYm��[̑+�/Q�rZo%�TQ�;�T�����Ls(�$2�C:s������.��%��+����eo�
����Ntt�q�۰��k���K�7O0m_�t�_���p������Z��1��SsS�M7"m��e�v��FZ[��w
�-F�J*T*�j�����QRg���
B� S��u|]g�:�ɵz��jq�wm�l���tL.e�3�sRM�چ
�k�Sm���jkmWœިm��++¦�'�t�IL�k*բQ
��D,�P�B��\l�I[�9{<�Y'�L��z�̶p�!�����·j�
��Jݺ�5T�ܔ�oKsG� (<�����C�B4��jyW��?zm�ӍSN����m
[�Ԓ4��=�m� |�۾��%�cZpj|ͩ�Ui�Di��<{l���/���T�=
��Q�^�hO�yH�$�sN� �R�V��:vVnN���+�q���ΰ�77F�v��;[kK*�aUlt�*���[��#���q[�˶��c^���bږ%�Gb� R�6öۍmX��-�Ma���ʉ�A�93��1cs..G<��y
� Iߵ�{'Ÿ�e��g�.|�4���C��u���jQ�տ[9
�}G��-���xwl)I�Q�z
j
��Ó�"�rq�e&��=��]꾧֎���������c)�<��kӳ+��� 0���Jr�R�R3'���T�n��X�i�^x��MF
����Bު�*t��I���L.[h"2"nK�z�Ze�'Z�V/Rr��N�Yz]�8죝���n]���Ķܩ
>��^�Ժ��]�u-7^���\m�Z�j�ܣ9+Rmn
���ߑv��?o����ꋘ?&��ƪ��y^N����4�o=3�
��-�ؔ̿��*��`��}V�݁
���ƒ���P��u���8���%�$���
ݗ]�w�t;\��y���\����>=�'O�jP�Ip/nJ��U8���{϶F����N�M��sf"�ί�Nq�ƹ(�+
ݮ��F2��K��m�
�|jܴ������Z�s%�zf*��eȫ?�]��4)I�۵�nR&F�X
��+
[jD�h��(�#�
�哑9�q9�E�ծj8n�o�Ǖ��Z�f\J�-�l���&��Z������˫}`���ӎh�yrΉ���n\ű�n�]��9p������ʌ����ӣ" ������W���t?N4��_�I��_~�5��4���#/my���1� �Xr�����*척aS#D�T��
�>����q
s��<����F#wM�F�>sΛ�W�;3o���U�aJ��S�����R�M��D��gQnt��:�Ql�,��/ ܷfR���q�iM��
�Ȼ�>����Co�b;A���>ڦ��Wق�M9X���~���/!'�M�W.�}Vrߔꔵ!�5
|���iB����(�0-����z�
F=���}�����okڢ�E$�^w���W�~n�okY�߮�\�6՜
̌
{i�-AF*�9)\t��9�I��V���
������6����۸�5�Z�UF��6�R$ŨQ�Iq砳Y�UZ]e�yv��� �>hI櫥<����w0���N
�)���&��l Ju�
l��wE1��G����D�Ou� F�N2�|
�}馥��uC�1��rޫ�V�+^�g����d�b��&W[4<^e��4�Y�W,d��|h�t�ͮ�sUM)۸�8:{3�d��{A���Ѣ��)��~
��� \#J=N�d�����Ʈ�������ꮓ��90
��|�����1���K $�����v�*?��S�
�]i��$J ���,�C,���SG�?�/�����_՜��pMSƯM��|mG���1V1�$������~�K���>C�S�
v��k����u��j=&�)
-,yLj��uFHK{c駗���.�SO��u��a;��B�r�Sq�j�-ۍZ�#��
�'Jy����s��7��[g��2z
/.u��4�+XV��2V��Q�.ޕ��)$�"�(�%�)#Z������7suZ�%j���
}�B�������Ǭݕe)J��vz�8z�Jf:�hIN�|�svO1�O#I���E�cۍj��ݽ:Sd��Ὦ��v��u^@:o���^�5���c�s>��i/�Vqm�V��m]�ؔ�ܢ���n�6�'v�ޑ��̗J��4�Wn@��O�lKb��X�
��;��n�:h��g��J�9�Ży
Ǒz8�f���܌��q&��Y�
�f��N0��N;[�69�
r�bׅ�
C2��/#�k�E
��l�&2�~�è��MR����.�*%��g�=�Ft�<��N�a��w��R�w��w\���ϊ�k]��5o4^b5�fZ�O9���]�
>.%�؝�e�8<. e�
��=Uv{���~㻏"E�ˑn���vD�ѭ�͜�����Lu��3u0��:�U֝$��[M5<����:o�i��+�V4�V9
���6nXvx��&��_� ��q�
Qq�w�3�W:uϔ����2y���b/�(�ɳ��|5zQ��i��J�#r�|H�w#�.�W�?�4a����D����Ų\ug�W����G�;��Cw��������������������������������������鐢K|x���g)��##�=O���.�d��F��˟�j�MUvW��Ļ�s�r�������.z]�kPc9"]R�)���mkf�Od��*uYf١���R s�B
�A��îh���=k]ʳ���Ur���r�Z�sq����`�d�#�r�$�/<������Yy���F0�nweM�W'��N6�T�q�F��H��y}Qr�y��m
AS�1n �S�`�T�����j�rT >�Ը�3o��^&�l�R�WȍyuW̦��Y�4�Q�DUM�J���6�5��ƒ[�������+��y�g���k
X�K���_±��k#y��:��8(�T��JOSQ�h�Jt2.D��R}�"5 �[�)�
r�)6�V�6�u����5�k:e�XZm�v𭤔!�푊Q[q��Q���}ҹL����E���-
�8�q��IZ�G�|U�M�4�j}Mܕ��[V�wm�{}
N�aqµ"Ԉ�M
��zO�p��KѰ?IA����D�����3I��r�0�'/q1�i�to�B�5{���%�w��kO
��B��n��-ۜd�uqIz�YK6�
��0{+D�ʕ��ܞ�qI����t"��;r����1��m����G����/��\�/�y�m��[�6��J�
ƫ��R�
\L������=S���=OT����@��I�x[T���M�m{>ݾտ֒ݸ�Ӊ�L����Y��Ix�>+"J��V��N�zx����||5r�I?C{�oz�8�۹e\����R-���^\A�2F
��R�+N�9� v�lT]�"ۭ ��d)t֞i ����#�E�2�jB�@=#���/���N�+�!ĕh� x�}I�!�cM��`ą�Z��*ŻɄҒ�߮Y�.�Z}�=�'/oۙ�3��Ip�W�̮�hT�7�c���T�S��uz9�>B}΄�&�h�!��>lӵ�n�~
�j�˅IvU.'�v'�CS�Z�w8��Q���K3G�>�
�,J5��9ٷ���+����HSg��䧎���hJd���zvwv
����-��c�v���x������S�5�[̊n�~ؿ�%��ַ�X?O���0�\�6���n��e�
6��kn��9.ϯ���}����
�*���h��
����8�_���Q��h��L���ݣ
����7q
+=�X����BҲ���5�?�[[�)+�F`�=4���
}B,s��Ng��==����u���*������������Nj��9k_�GJ)�+R�~GS��P�B��ȒZ���:(�����K]h���e��L=vK PӢ��wq�(N��r�G^�ث�ϣ?�#�tC?�.ͼ�[��
���ۅ�o�����؞��y�#%�Ǜ�jVy������LS�w�%T*s92
JTM%�"Y��kQ��О.q� )��gC�Ͳn8cgi�6����j1�M�����Ѿ��[{���9<���Y8�]CK��/�*q�����v�R̃�T��Od��w�����܁9O*e�y��t�0e��
jm]hs�n ��K�BQ��ЏA�y�Y�1s
~�s��76���kz�nJt{ZإJ&ҥ�`rW-��o&�<������7<;��f�UI��V�&����� ����F�T�raJ��h�^�v�Ƙ��ǚ�םidfi.^R�H�m�����g��&�rׇz:}�݃�}x�T����$��ض
k�����'5s-���狶,\��vp��bP�D�،��=�Okf�������.c#c�dz2�F����K�5T���!&�)|��n�t���D�<���+���OŹ�U������
��i��-�G�[�E��E*��FDfe��a��f�
���2�Q�Ƥ���M\�UG_��{
ǹ�m%�\y�r Gy�����:.\�4��wjP�GUJޕ�U�V�7Do\7Vy_13w;��[?�c]�H�\��$IJ,*L��]3b%�L{�y.�J�R�KG2s�q,��B��6��T���}(�#��nW��
|km+��q5]��
�r㪍b���J@y{����by�z ,�b踊3�ϻJ�,'^����xd�،���)JV��w#�.V�ټ<�S}�j�bZ�}�t+�LvAF��"�q\����r㲝
\w!�}jR�����3���ν��d�ҰT��o
�%.�*wo�����7
2m��c
�r���ӓ�
kO��
[�*w��Q⧶���JŘBM�*�o\�TW�'�)b���n�d����}C��zC�����1���)Ŧ<(U��ᰕ(�
4�m:%)$�b��Y����>c��''Ý�պ���Wtb�RؒJ�z��۠8�!�o�9IۄS���95E�9ؔ�-�e9JR{d�m�nッ<�[~�n���$�
<����nZ܈��K~�Y�6{��a$�ҧ
(A$��Qյ�c_�z������8��������s�)I��*�v#�yc��CK���z~���R�q�,ZƱM�NQ�f����&�Y=���>� ���{~�Њ$W���?&���Ր����Y_��? #a.�ߑv��?o����ꋘ?&��ơ|�y^N����4�o=3�t������=��~�7!���/�M���3>n����8�W��홎2�
M`���Qx��+
��z
qy��8�%�]7��_~�5��4���0ۦ�彷��]W��q
C���ѡw�kď���y�������F��5Du���m��_}~�P(��5���.��(�X�,�K9��vᯐ�?�le�B������9;��J����hm����#3�{��CxG��E-��S{��;���@�F�z���� ˙���]=O�'�!ɿ�]'�
r`:��7'��2b����Ж>I��y��,/�e��T�y/�V��<.���H�?�U��Y��Y�{����\�^#�ѣ��r��9������^��7��?x�o�R��Ȇ7��E�o��S�_������������&�?�?��z����������ϾM?��(~Q���-���K&�>"��~a�ߨ
�t7�E����m�s�ϛ��+�?���;f�����Cr���)f�Y�+>��z��$����tIk���j���n_�>�v�nrֳk��i��-˹l=
t;
�'EyC¥�|���/B������LwBJdgjۛ��$s S�1��|ɍV��%JI 6�Kv�əhz���IlBY
ɒ��|�0"�Sy��0F���<����H�b�����ծI}���ы������b|�y5������[��� ��G�
�������c��m��������������
�u¿��q�q�u� ��'�|?�-�:��ꯙ�����w���)`����������������������������������\�g�����K���I{�$�b�ܛ���O-$J�#J�DZ�� z��. �.��T�
[{�ܽ=��W�(ǂ7
�E�lM�k�{-fe̶&
ǗJ��t�m�z�qH�T�*LZ
�:�r���LG#-V�e!
Rz�5�~�ɺ�b��F�"����&�
q��rTj1RM�ټ�
>�>e�o5��W)�O+X˻u�';v�)�2�vV�q۳k�����ۮ������ws?U�ʑBǴYO����漪e
2MIj�PA�ک\�b��1)DD�ؚKm6Z���W�Ψg�ȕ۶yj�ڳ� �2ضN����� ��[C
[|�r�@9J�f�o<_� �e��I7��q.|���c�Ê�V߷:�i��.:$�ȋ�)1�%%�)A�DZ�CEBx�J0MJ���ۥ��y(b���N��s�K���M9��k��43�Iw����N����t.�\���%N簤�I'.��j|ƃ2�$�g���rB�E��ٌ�\}�9:v�*���!n�7��M(��ɽ�]���7c���@�XxƱԨ 37��īf�6�2cT��T��f�FK]9�� wn�����
tQ��
�Hͮ�v�ٱI/f|j��
��=�����7}�\�_V��5U^+:u�l��j�S�ȃ���� Y(X��I��.�ȱ��mo�1�甅j���ڎ�I�Z��2>�#�\����*�:g�Y|4k�\8�Zw�Sq�t�y��A�!�+];бޞ�K���ծ�Ë�¥�����e���)�#�5<�p8I/ڕ�Cc�Z�(�T[B�ʎ
fc$��T�i�
N�r_oap���.�QK�^��8��VdU{*�ѽ�L\�=qm�j�n�
B5>{����� ����Ӟ`��v±5
�����^�k�&O~O�s��hɷ��,�;6n�������O�W>u6�{�R�q�S`�)S%�jp����\ip�dE�BL�fTW���y$G�IYw����~�䲭J���.1�v�SY�5��z.V>^+Ǎvc.�I[���R�{Q�s��NR3ӎ���f�h��d>y?
UJ*}��~�[�e\�i5U^͛�����E�]�G��_F���
S�(�Iɿ]i��8���:4���zj���~շsW,ˆ�s��y�:�%��O}iu�r�]iF�5~3��M:Ӟ#N0�6�)�4 ߧgda�w�I����o�ti��z:�1r����5�YDZL���HBS�i�;NQ�c4��4���la�=��Y� ��kQI�T��*ըl<�S*p[�EZ���R��ϒP�~�W
-T�ԅ�Z�wT4mG�q�
�5�C%ߒNs��i)\s�M��ݷ�� �/,��Ҟ�˜4��r
�~
%K��oۛV�طe]��JTj�6�B�R22R�HQv(��g�n�D���i�5v��+��b�
N������w����ܔT�IxU�b��[h��5��a�pׁ�a���)�dGʒ#�
�gb�c
J�j�����%c��
^+T�J|K�P���U�m��Q��^��)M��2뵓i
<��|�䜃26H�#�\�.��Fw!�����l�+���
�r�3r�d��-�kDtM'��
^h��2�X�l8*q/i��)n��U��˿ӡ�����RQTG��
]�V�ޯ���ҒRt��RE�əcK[M?�������6:g��G�Hxj�����|?�9�_�X�Į&z�N�/�sk��h;�RU�)�uy&�WE
|%\�G�Z����B��UN9�]8~��m�qo�p�~��y~p�\St�j��O�R������^�u��
��^ �Op��zJ�J����Bo[�vu���\x�~U��%���l����~�\\�/ 1'�:ݥNg���Ӧ�j��_/�����b�+���)}���mI�C�j�{]d�*l���� 澩kܓzj5m
O�����b�x�
���.:�H֚�pVm���� ��@��6)�2
�H�A�4�ԕJ�I�>�:tq�2�(�է�9�VO�4뒳��܂�~2��r�q'��nr�V�ZŦ�[��t�7\��oլ���f����b�/�ml��p�
c.I8������콚q^1i��E�~���䰳m�i��[���d�ۧ��w֤�ICfdFe���C��sg:i|���
��6擣�*�
�96��l�u
�s���t�^�{��%��99�UN��RvaM�ܽ�����o��
�a���m���m�i$��e�m4�D�6�DD\�n����A%�$�$�#�}۷/ݕ��r�99JMն�[o����T�����E�"�KT��aP+�HG���kŴj�5��T�M5���x��Ʊ�����OS-k�����`ۛk���ٝWz�;{k�S}�F�;~q�|�~�^��_����|�e�u�wn�E'�pSu��pU�P)V��]v�E��+t�
=Z�R���aVd��G6=� *.ϼ����nj9���:Uɷ�b�ې����mF�_t���ޫ���gH��j���V�
S'
ś���Ǖ�ً��d�k��k��ѻ
�_��]��K��v?�nT>�)��^���e=�A���r�1�
�'�3ԔI�LyD�?�:�-^��i�n):{7.����\���.�:V
}#�����������뺾.3����r̸��*x�b���F�M��
��aȵ��z
�6S�Q��:ײ��j[�
8�n�n
��iFM��w
rR��"5�M���5I旘35��f�^����j�=���'j�:nNW.ʭo�cZ�
����v���Z�K�V��^��ɚJ���.c�M�1�ZI7E'6�rg����탸��5o��Z�=�[�m�
Z`\�h��b�M�UR١����Ȗ�
ĉ)��:Jin!_7��Dй��+����f̷e�KҷvͨB��PR��(V���`��y���6tw����*����MRΝ
���cB����.ڭTn�c;P�
���$8nF��v��m�4�(���D�(�R�#R-�L
-2:��FP�
lx�ZKQc6�I("Km�%�$E��,
7
8�u�X��IF�A$�RQ�I$�J�bInG�]c[ֹ�:Z������M�+�n^�')Jm���JM�JRu{e)7��jQ��Dw��~%��yQ�l}
BZujS�Sf��۩Q�Z+�Dzhd5o����%BI��c'GZ?�}:>Ɵi����vז-%����J5MqG�W��T�Vʦ�����h����������݇�ܟ���~��Օ�_�6�
�n'�{3���~����mϬj�'�������
�J1���1��O�Ȼn߃���r
�Qr����\�3������y�٘�+��� ������W���Ӎ'�W���x�E��s^��O�
3
�o~[�|���7�>]]���H��9�݇����Z�o
�m��T@�]?��������5�B�:��Z ��߂����������'`�����V�_�+/��MS��K���X߆��ޠ��k��3?�o�7�y:4R�/�7��þ]���
�iG�߬�a���������BR
��U��&�?�r�&/��} c����������Q�ߥG�����j��2�?�C�5Y�ś�e�7��h�U����=�?�+����� �x�龳���f��-�܈cz�W�^7���p�%<��Q�/��,�O�9�n�!��@ǯ_���
��
�����r���+|��i���n����.۷�� ���܇CT\��6��<�������^��j��[&V>����-��(\�D4��h��{�U�K&ӡ�n�^m��]F��ݢ��:��`δ��v�j��俜F��+�)�
�y[�{
����{
7
tu��>gv��rěOj��������'��5 ��iRg[��Ͷ�F���j�Ge
�n�~�qT$����c��i�
��ۚ0��oԹc*j�L[s�V���Wq�j�\ݻ�&��6��"W�o��K�:c���nWmr��v
)�o >6��6�(F�>=�W�^�bf�#c�
zz�ʞ��t�پ�y��%��m�ՉPël��
���e���}����J.\��Z�k���4t�tt�>�o�EM���=�q��)h�J���j�I=ͥ(���%]脼���_��8�8ф;���� �͛�g�W����G�;��Cw������������������������������������~��˘�$�4=u���W�����d�Ĝ�Tث�����N�D��kiQ���L9U*��O"4XP`0�2���,Ge�-k5$���h>
ܼ]3�v�r6�!9�RQPIVSnM(��ۓ{�>�;/Qͱ��v�{3&�-[���r�c�)�ܚI$�n�{���Sv�3�[�j00��)��-D�3������z�}�MRzV�Qпj,
T�[u����V�s�0\�����}���Sid;r��(ݝ�����J>æʺ���L�&�c[�j�P�K0�~�d��(FKÝ�W�\�m]����G���Tc���F|�Iׁ��)�I3�~���#�oX�%vҦEݑؼ5Żv���2��qAZT�E�^..�M��{ʐf���ȏ��2#�#.��R�}�*K�ʛZ�z^ӞN*���l����P�����ťL��f\��G6[�W�V�Q��q�uV�]��X�Ai��)5�J�!�,��$��i�����J�6���o$t����P��Z���c;K�
���jx�_�n3�`�qI�e�l�V��~v�L�y{���f���n匋�Ѿ�n�%��;�zV.�n����'���-ұ��dd�2߽1�b�Z�k����s����Pe
�3TI�9�)�$�
ԩ���IN�9V���ơ�\�=2���885N
�\
�p��)�/a柛�w�9g_���l���ױo8ݷ� ��i�ix�JV�&� ғ�R�i�{�N�� ^�_o��AŮE��6�Y�
���7��������I$���N��k���$�|Q)��-�*4�����Z) ���^�¸� �%����4�Qm�
[�I%�.c-OV���+C֧R#%�Ѩ��C�e���3i��;w$G���+_���dy��| Fzj�$�����D�I(��=OA
gj%�v/]�8qԯN��I��S�*֩',Q%�\44��Z��Z%D|Ǧ�ʴ�����6�����&�vֵ�I$�%8�(�Ԭ��ƾS����&�<����S�_�Z�3��>��#�Z��.
��}6z�?b/|J��l�{�ץv&�����m�p����x��4��Z$ڝ4-H%�dGK�fM:sKSRW��eJA�����n]�>�s����6应���-����W�9'H�]'�uȫ�YvgK�^�\cz
p���|M��� y���\鏩w�/ËQ�.�)��]�\Q�iS`8�u�L��뚛̸�=J"�ܻ�i\å�'��-�)�54�Ue��]�:���K�\퓡�v�K���� xw���Bqr���H�\*�֕Tn�z��C.mT�=t-H�]SČ~��Nu╏N���Å�����3�f|��͡�G��~�B��+�X��m[Q�7��U{�9"~��
�jg����K��
Zo�ʰ�7��������"�qJ,ek�S�eN�G��
�g���ϳ]
^�.�6:s}_�,%eR
�g��<���5��z{��ZP�un�
#jRІ����.6�g�
�T�.!]�x��a
�����c�#�j�N$�Zp�l̋H�
������W�Z�����u��8�������W�m� M���R�ýsĮ�?�M�co~�s��x� ��T�U���҆�Q��
�:��K�DG���4���n4��2.<3/'�^?6��/ܠ�ڒ^�����y���r�rÿr2������\D���}}��B���]�^��� E~�^T���
��c�ɛ7϶�Y[���<�֞�[7d��}2%��QP��qOLEQ�R\�C�Isj1?\��}%�t�J�0e~
*�s�k"*)&ۓ��E���i#���{�1����J8��H��rt�|'�ܝR�
�r��8)=Ɣ�N'�RVz:cf�]�F���7�b��ZyZ��UȘ4�x��8�,��#�J��G̒��?.�W���9X��n�O�]�KO��]�%]�ƻ� O�5Γ�/3�q�Ó�j�؍/���r̺�r�Ƶ 5�\��&m�6�h�.����xoeX�����[�=<������3%< l�Z�"2��h\��Z�����[��&��jW�3ejm?�k&[]�ųj+{N{66l����e�u _�+�lj�]��q*�
�
�7g*����knأY��v��=
q� �ە �d��xЬZ|���%�GUr�Q��3jL�ŒqE�T��]�1� %�
q�kX�Yū�Y�����c�� ���[�7Ś]�Q��Y\��
�jk���o�\��<���/Lc�7�+��'hMSU���c6�qX��y��ؙ~
��6��#ѯ�v��.�0��$B�Qi��5�Yy�Ihɍiy��������=�KD�!n3��V�m[V�%��W-B���%sw���
�a������97aj�ۗ�
m�+�9�~����]�f�K�q�|Dda�ˑ0
A���]_v���m�M5*
F�-
B�Y�HJ���5}�q>ʉ.6hy��Dm��p�D�'-_v5;5[��8K�[��v���iJ.3�d���R:o��Y�
�H�H�h9I7����:۽f�i+wm���^�� �[��)���o�dP�ѱ5�2C
���ZU��Ji�c�Sw\�&_s���0uBȍ
�h3�������2�dž��zQ��f��l�c�d^��m|7G���ѹ��E�!�fO�5]]���H��9�݇����Z�o
�m��T@�]?��������5�B�:��Z ��߂����������'`�����V�_�+/��MS��K���X߆��ޠ��k��3?�o�7�y:4R�/�7��þ]���
�iG�߬�a���������BR
��U��&�?�r�&/��} c����������Q�ߥG�����j��2�?�C�5Y�ś�e�7��h�U����=�?�+����� �x�龳���f��-�܈cz�W�^7���p�%<��Q�/��,�O�9�n�!��@ǯ_���
��
�����r���+|��i���n����.۷�� ���܇CT\��6��<�������^��GY
��.�}+tv-ꌻF��{+Ӡ����
C}�跒#��k�o����,�f�52�Y���
����+Wĵԭ۹υ����&ݻ�*��%u�e��&�jMLߣ��
��f_�_5ߍ�}C%�iW&�|�qQ����Idp�x�n���[�n^�k�o��R�H�����
�@�ë�k4�D�S*p D�sa�iIq��m*J���j9�N}�OL�;�=����:J��d��O�;
�j�F���y&��k+H˳;W�݊����E�p�^�E��%J��{w�{r=
e;ܕ�
ݵ�:���C�,&�!��D��<���5,��=[4{M�y��.p�Z�2/�
>5�|Y:S�J�E�\U��-(���a�_�c�ƣ��Uǽ�XX����K�
��
iȞNl����mۊڭڄR�!
*�*���ܤ��M�eȽ$�|���X5��(Ź\�rJ��~�ܮ]�>��'H�B
0�c
p��
X���Fr���_�c�?��f���?��7��<�����������������������������������u<�JM9�RO7a���K��LY5Zlmq*�}=
��p���҃�^��bwa"Dzi;m�*��ȴ�|�p%���?L(����%�[r�˄�kI����H#(�泩�
&�%�W-�C.��M�8�r��d�I%U88J*I��w����
m�՞f�s�&�a�±�t]���#;2�/��U��5(^�ej��$dfkQj�pR�M
�3�Wg���u1�ےO&�����R{k���o��w�-I���mF>�k�Sgov¥i��G��>�>䙗i ��.�+t���+����b�OjI�ܶ ��. ��i^:nm}�s}�(3>�N�Z$��2�Qg��(�[�"��.��>�i�.�ƾ���������)B�̋M8+��"-
���>��eE��6��D�����ݥ�J�nJ��ˣt����
����5��.���˅nJ�GwZD��~�!��i۶�a�,Db�
3�ZQ�3�O#��KO5��/֍o�z��uK����'GbR��i�N��V�_�ҝ��c��v�ם
Z��o�X���}F6�z 7�e��5��_e�:ۓ�j��=���A����B��+��iܔ��ER��a�d��M��B�q*ԯ
DwI/Gy*mĥiRKg�6��s
�kY�/�#�SN��4���e$��-�
�y��X�M�
�Y��L�?^ĸ�N��NӪ{$�r1���JJ��R�SL���O� �]�Aq����m>V/s[��~�i�/j+m>z}eI"Q���vp�]{�Z��Լ:{��vPA�G�2�=T������͡�@����ڐ��#�u"����E*�>�C;o$����~��C#�_d���/�HB�q^��Y��RٽzIKbO�m�\~�ż�����jFFG�diQ(�*/i*#.FF]©�����m=B�m��p�QQ���Q�S�P&Ҫ�!T�&^�>�:
y���)$ˑ�Ð�F�čI
B�ӡ�-t!��b�M�
���W�ҦŶ�'UZ=��}zvn~��oT�/\��ǒ�'nr�8��� A�JIӆ�z�<���^�uߖ4�eFC���1�i+v�!���3q ���N��yߕni�?�4�JZl�m�YF��X�F�ۼ�O��0��B�\���m[�
t�����ʄU��3���s"Sr����(NJ;SK�W72L�4�̏�BV�df^Ҹj\�]��ȱ۪���(ӷm
�?J��-��K�E�mW�ڽ^���4���<8q��u��%9pŹ��W~��877���ܾ��eVг��S(���յe^C�]���yX! �םm4�
���FG��ȋ�\��y'Z����
FX7e�)|��Gj�t�߹�#��������gb��\ŧq_�([R�8[�q��U��$�Z� ��(ʻ
e�zV������2V�!iQ,�i$�
JE�˂��٩�
�a(G�K��'O�{�v��nBvr��yR�d�-RK���4�=��q��xZJM�l���_�C���uuI��z
@�Rt㮽�!|6��8���\-l[џ8���4����-2�P��u"��
�RJ�_^�O��L>G�1�~�X�n�BŬw6�J0�*�Uvlږ�1�N
�G��1�q9���IU�m*�'�o�Wu][��&�Uy�
���YZ�b
BZ���R��ZN�fE�J��f�"+�2��
nF~E�û7n1��xv��.RU��M�$����6
l�Ax��S�Q��J�&�n5ܞ�w
l���Eó�i��"�#>�4Q�.���nEq�7Oko���[1���wg8�ZQ�w�����ZYi�q�tm��&~"�>Bo�?w�͡n�i��2峋<��X�����N��C�E��y
Ҕ���+%��ZJ�
���ʩq*fpˤl,�~��^��Mχ��k1����+�:ݕ
z�&�Y��`K�L�ӪУ�D�r�3�[*Z
:(�S�L����<�����r�8�jQ�Ȼw#r���5(-�j�����K�
e��?`����=o�Q�Dg;#z��!v�Z���q��r
MFI�$kR&Կ�p�����4�:���Ӧ ����|O��5?�<���Q� �]G��U$_n;z�v��i��
J�*�2�Y��J�M�_�:�9ɲ^�J�R(T�
��
5��k��PJ�Q� �Ț7M�f�*�3�s��O���+��ɹ�'n��^�
يN��Î���z��W��������Y�����,[��(E[�۷�.'Yˊ�9ɮ�*��b��^�5��mz��~۔��ԯFTJ�
���%�fJB��
��
8�q��4:˩J�RV�Q~n���z��wHֱ�ei���;w"� /J}�zkjti��?{�9���/]��nT�����I�ڿfn�����g ' Ÿ�.-�C���/O�9f��,I���E�Q!�<(ܒ �T�.�hWo�SF�˝5ĒJ5�ۉ<��ӓ����+�yzb����B9v�:�������;����%ñ�F�O���a��yM�.�ۊ�b���ӕcIݥ��
ӍJ6�Y��ZQ�j}���&�*lTr�Q��1e��hTj<|kB�ڌ�!��-f鸝Cn�Z�Ԡ-|� ���r��^M�2#��:�^��6�8AbZ�h�����:>&ݻ�۬V�q�s��yԭs
x|��i���I߽zZ��r���g��.:mp%���6Ԝ���v�gm�p��IU���t�;�Qb���S.Է)
ǨK�S���V,���*lڌ���|5Jt��3#NP��.�=����+OZ~/��G سI��gbꥹJn
��l_D�UM�\iM!֔�wV�ZuԺ�,yV�.Q�
>f��
v:��݇�W���iaŸN5�Ҕ[��M7S�s����rv���ǣr��MW�=�
\�8��ZW-�js�nڕ.Z���nF2qt� ً[ٻޘ��Y�۷��
Zm�"J�x����r�&�N�AfA-���t����o�9s3�59݆m�Z�+N1��-�q�S�$�D��=��1�7��
x�+%_�
��ve4�ir6�Z��$�F� ����Dڗ��n����F���t������O���r'7��'�{���9C�˨��ꤡa�Yoa
ce�{Ref�n��f�t��
�R�R"4��%ʌ�m:����Sj3)�OdInT�
O��>X�'vxV#jܮ���w9�Fo����g�����;�5.~���Y�5\�~�1�8Y��Q��ܹvj4��+�~���t�7S��
����ﬕs�
%^۵ڴ�DZ�V�6��9��R����^��Y+�rj�$ԇ�o�JK�R5
�wB9C���>��Y:���l+�EǎS���{�ʲ{T��6Wi*�
���^^9k/�y/C���s�\�g*��qڵg��n4T8mE��R�r|Ti+i��P��e;;.��i�\�EBEJ�
丬i�9ɧM�-ԼsG��D��rZ>r#��R>��~X9�y��4��b棇9J�wV۔%m�(b[�T�j���vl}۩�~���nDԺ{�Zo-Y�uK1�vx������.�nWu���O���+��jN�� ��[�ٮ0�%"����C�dT��JK�-RަH�"�$I(�*��v�e�� �&�҉Fz��B,_����Vpqp9��m�8werv�')�E�;�o&��QE��^d9�˦��j\����_�,ڵugZȻ�̧8�k +����j�K{��w���m���r@�3�ӭ��2� �wF���kzFV����qs1�؛�.���v�'�I%$��[��iT��]D�5�D����l���2
n���k7��q�Uxԫ� �L�S��+sا3/Ζ�e�ZYK�<�["%-g��/k�R�s�:�f�����3;*�E�
ت
w�J���%)5�&�+&�������rw*霣�i|�sMҴ�|;R���+���fm�䡩�.���!*��*�d�Ӷ-�6s6����,�]z��A�XM�W�jm�n�z��%SJߴm�2�UXw�7M�Q%<���!t�����K��ys#P�,��W>s;3IYw
x<+i_\\\U��6�
u��7P|���x�b��n_���k&ӓ�V��O�e䦒�
VUr������,-�㘘�"���-
�L�Z�eO�S��Ҡթ��rEv�q�8Kf��%
�5%&K"#%v
���D�/.Z���Y�Y�ŏ+p��$�nZ�
��k��v�އu����W9㓱��Z�
�G
�w�Y�����IF��y�f)?ƎU�m5 �ԉ�/���'�k����8����4���{����K��O:����r���Q���I}��X�R����u�Ԫ|*lu��)��3qZ[�m��S�m�5R�3�".Xcَ5�c®ࢫ��I*�۳��~��wRϿ��QW�ޝ�(�EJrri&ۥ^ʶ齲��Im�|[yb;�mn�m��֩ui�ܘ�q�>
E+�I��kx߄�3r3��3-5��09ϖ�9[T��z~m�r���5N�s��Wl$�o�Pu��sޛ�
^��{Z��;�����);s���ڹf�\3oٹZm���ԉ�/���'�k����8���4���{����N �O:����r���Q���IBø���8�������Bݱ����3n�֤Di�K�4�u&
�
o���fS��Ȓܩ�x<�˘|��N��0�Fչ]q���sp�"�}!� �Q��W�w@�
�t���4ӭ+�cO5%�]'*�{���eM�߲D��RO�1���y*�q�8��w++e!c
�߶��ܪ��l�Z�Wّ���M欼
��CQ��̼빶�l��X��{v�i��b/V�/
ai;x����6��~]�+z]M�W��B>�r�e-��:��lgk}պ��!�#���9?�%�܋�V-c[���z�!W?��c��7YN��m/jRr�[��HO���z�Ի
���e�f�ճ0q1�5Z�p#�r�kQQ��0�tU-�A��m����ڵ�P��/���cȕ?0c�ZY��j;��:�0�Z���M���=D6g��
��?'U�N���+�ձ[K�� ܖ��B2��'���x�q9{�|۫�N0�k�u
7��x�aj;n\� �2[V�z���������������������������������������nM�lW����i�Kb�S�k�))f
.����.)Km)&bGZ��=��>
OR���܍W:j��'rM���'���w�Y�z&����� /鶧{S�ʵb�"��v�ջq[
�I-�����Ռ���
Z���H�.���_x�*�Bag�C'T��(�Q�
�:$ͳQ�cM�C��K�y�?�3g'�ߝ�qnT��);q�s�
#ؤ�Z�}OO���I:c��f�n�c��8W�~qy��.;�^��p���Vl��]Hԓ>^�H�^�@�7-AA܃��n���mL���(�uW��ܻ�S߿����
���T�d95�Bdh4�t6*d��
Dh�!Eh���I��[i���Ũ�\L�.&N��c
ܮf^���;�$�R)�\rip�9I���|ٺ��?#R�.Z��DZ;�/]��nݻqs��\�Q��E9�M��&�Bd ����]N
�mN�*D�>tgbK�>+ˏ.��!�23�]BȔ����R1ɝ���^��j'k2�ƮqBQq�[���$��d���i�]�i����cV�/�e`B����.FIIJ�q���b�i�>Ӥ|�p���;��
�
6�$����
{)��RU���>�_e}^��dz�dfzi� � �������%�e
�k�����
R���V�US���?6'���hׂ)�5�.\+q�U�g�zE2C��˷e���cŏ^���֔ibk �s�he�s�F����W������J�#~>�� Wk��~ݨ�}�ڶ>ơǚ�)��ZƉo���~B�-ڼ�rv��o�E����:Ʃ�3ۣ
�K7+Y�
�`Wi�
�rS��)�:{�>ڛ}�:�w��Ԩ�(J_�";�����6�R��%�
[�u�&ƫ�dZ��_�\'np���|
�RJ�wN�eT�����������W�,�=�r��r����b�nkڄ���[M3ܴz� )3-
�R.?��:o�kۼ�0TU��'�w{�����6&w7�j�1�z�����3��O�N'��fGo�O�?�)S�_��bQ���_¿�R(^�ԴԴ�G��. ��
E���t�M��ڇ��&��RU�i��W
�uQj�����
�U>�
Kiu�1d��<ѥIQ'RQ�1:O�/l�ŗᏩi��ʂv&�J���c���{��D�5
T��t)���1.��n[n�۶�X��}Rj�q�n���O�ʽ�(�~��[N��s{�ސ⛌���uO�,k�go�֢�d�RNQȄ �. �'��6���W��!�P朼t�dZjFG�E�"���]K@�'i�۪�N;����sI�[{SOzk�>��`
��r���R�R�+!σj�8�&TjlvA��̷
Q?Hy��j��y�LH�Nտ���JM��jܶ��T۽������l�G�?��S�n��KN�%<���
�nq[N0�S��q[Ta(&������
�t��(|HG��O�~�
�g����v����kݻ��T�R4��&Z$��#V�iO�Y���1�r�$�6���YF?e4�U�/M�v�x�ų�:z�bU^��g�Q�Q���+NW_'
4�jf��z
^��c�'#`r����v�r�ڡ(IJ/�J��
��ݦ6�� ]�-CW� ����
�����|_��{v*_��q3�^��DZ�}���Ic
6�
��U��ڌ�8p��
�7�{��c�rZq5k�����i���`�)�m�U�6|�
-Z��5�^�i�Ez3P��=:�Cu7�DF�'���k%�}�<�
��C-���ֲ̱#\,(��f�8�8%X�-��N(���c��k��0���V�L���������R~��}
��G�"-8��ӏ/��ϰK�q�?�(���#�nrV��Tm�Z��;�z�ióM4���
m��
|U��T�'C�^�����������������������������������������������_1X�.�gX��M�{�%ʤd��
��4�\ov�N":�"�������y-��,�T)f��LQ�g�
ۢr=�/Cƹ�ǨJV�r�[���a��+!��rT��|%Y\ٱ���zs�
S��>jͱ.o���Oc�6��f�$�q�% �
� �ǒ���Go;��n�[];ߎ�j���r�k�{��~\�Vۓ�NI�G�n�:�i��q���x�o�
�|��~�t� 5���)�Rxע��r�i�{V�i&�N����UOl
_��Ѯ�MfsޕkЄa
�y� .0��P��{7�N((�B�aI�P�$�
��K���"U6�G�l�
����ݙqJ��R�u�������+q��N$���
m���#�*���p����<|{:>-�E�v�=�86�N*�M�M�긭�U*���uѾ�?/^�o7;'�u,h4��xښRM�:5.(��/
� \ի���U.{���F�^��rmF�-�J�ɷ.�>������Q�"[4xT�^�OZ�~m�K}�T0�ݛ^S�A�o9u?�l�X��(�����'��
���q�j��%=X}"^e4w�ˠ|������rܫ
6�I\��Ķ;Ӻ�w!'��ڍ��Wg{ �i��������������������������������
�U�_9�
��Av�h��ۣ��ƾ��+�:v�s��/M��K�[�ɭīe{��`��Z�g��b}r�[i'G
E2���J��7�Ne�z�5�79w�R��q�+�
Un�
�]��J.��c�J4�M:�h���箽��Wx
��x��m^�
�p�c�\wcN���%��'My
�$�$|
:$��F�q����ɏ��¾ ^�қ�P�9J6���Wxv�u}ݵP�>Z'��FFdg�"-;
���[��¢����c�mWk�ÎT�8��n����G���%��ݣ��7*\�խ��C��L�R�Y����Zͤ�i���D�&�J#'��ehbSyX�K|���y�*Ӟ���p�S�̍�R��`�[p�T�r/��E��g�)�K���+
9�2��{_�
�n3zw�z��'�oŸ�ۤ�+s��Oj �J:�����`T�>�C�f*lwd\�fY�O�P"��
R� E�̔��֢L��4��ɥ� :��;
�.b�(B�0�2�r�J蠟9>V'9��M%)Iqn��h��P<���%�,r'P/�����v�NS�wr�#w"ݨa�q��c(|{kd�=^�0jT���MR�2�U�L��N��z
�|�.<�|��^�P��f��Y��22##!�,�K�~E�
B�E�J��ۜ
&�j���RN�sHަ���ޛg\�����r,�v�.�jK�3��)[��E�J2i�i��{KEi��H�P���^&��]�������G�n8�
x�=��K�}Wx�/������K��I9-ϵwQ�%�sp�ܾ[��^�R���}�S3$� q�v���q8M[�
��o�zKxcqmJ/���ӿ��{�_}7���&��ݨ\�f���6Z S��
yQ�z����&���� 7ۉ[�8~U�N��n|n�k�i�T���B+�����4���RI8�'Nc%tn{�!��]Ȋo.�nE�m�ʱn�J��� A�+�wy#���+�i�kǒ�ڂ�;�՛�s�8�5'K�mE:Ђu��""�I�
�ģ5p=Б�b�T���Y����-�ͽ�����ڔ詻n��g�L�
�2Q}$de�#� ��f�s��^�o�{DU���Usf��w���Ӷ�;s1T,Ǥ�t��ޒ�Q�\��J�=�.t�KU,�7čJ5 �N$y3��������k�d��SMQ���U�~�����mO����[��03 �$��<�uJ2|.N*���Am�h����t.�������|�6����5WuI�F�Z��E|]��7V�=[
�NH�'�p>��z��Aڟs�F���5�^���뜞"Կ
��Q�Hm����rR�"ӳ���ηer��+Ҕ�Z�]h����E-�6��J�mt���'�ޒ�=O��[s�Q��j)6�K}?e����4��v�_���K�fZ�heޓ=BV� �[b���Y��}l�ݒTT����Ь��{�ȫv���O�_qp��RAp��Vŗ ��6ju���=*BR�)��g
"�O1yh��b=tqJ�
gt��m�\�b3RY���+J�Q^�Ō���֍���
�\յ��\>
��+�uSi���{=��x �^w;uӘ�#�ĸz�Ln�*$��an���ok߷��C��Bӷ�}��5Yqv�dž<(�
���������������������������������������������"�_�O�Wit����5:EZj�2�
B
��ρ1��̊�fi[n!HQ
�F82q��1牙nqnE�p�T�(��2��RMoM4ϳO�u
':֧�_���X��j�����s��g
�jP�^�(��ڙ�{���2%E�͖��j^}��ZU�[Q�$'U)
�<�܂%!�s"�m
R�'���G5�M�0�<�+�zM�6�q�Ym�����$��ڕ�$����3ǧ�H�]�?o2�N�<8F1�̻r���_m�y[���R�f��59��NjpzBnl7*{��.��Q�P�
3N�&^B�LJP��j�A������HCK2Q����}�$�#~��Y�Mq�8
�k�(��MFMU)8ME�q�Ty�+�Tʞ-�ar5�y�ܕ�OXw!��e;q�-Jq���ܶ䓊��Y��:L�C� �U�E{/�t�>r�"lI��9)3KJjϤA���
6���SEE�$�d߇��3��K�G*�E����n|P�\ԭ��T�n6�I-�ƍ�K�Tj<1����H_z��wG�r19wF� �N��8���ݝ���+� a�9�ɫM6�m��he�P��i�%��m��m��D�! """"""*1�b��R�KrD"��vn���rM�۫m�m����������������������������������������Ľ�m�]�ӡi�G��� ~�e�"˩��
�l��h��R��T�Mk��^�M�X[
"J�
ݱk7���_ޕ*�
�DqĒ�&�flՒ}�����`W�}~Sմ�Z���{��ĕ~�wm*�/�{��{ѹ_���-��0��ط#P��]xlڱ~Tn5�w�i*lڪ� �(Jx�i�o���Ϗ�bq�K�Y����R|!|KN�53�
OS222$�jzw�w%i��}>���N)�E��+����r���ۥ��7���c�$
�O�fl/L�N��ث�\��6�H9:
F�Y���I)fB֔�JI��_ ֣^: ����9��mY��{6���6㒢�7Uj��]�:���.-�os[��R�&�g��������MF3��˸�#�km��jq��^8�W���"�P���ΦU�R��j�ʄWa˧T!����͋ ��lW�48��JB���2�ko+
/N�w
Q�w Q�zQ� �ے���%$�ޓ�7����^��Y��L�|�
��r��7!v��%T�rܥ &������|���M8�~y���b�����rn[
R��V�
g�Sn�{����{*#2#Խ�ᢏ���Ӵ��H� a�k"
�ӌcw��Ҝw&��R��J���0��7ױ>�Ļ
�����=�^
B���Ɇ�)����v��32.�M��1=�#�6�%�̠�tҤ����n�zq��M�w��ԣ~��s�*�%�-����j|���_���������m��*��.�Yx9S��z��=���)qE4� �3p�k+,`�=���kN�R�ڥ=��B��=nŔ��NA��x�)Q�$�ԩ���ȧ��4�z 3t�#Z�2l�ҮYn��$��S�%��y-�
�J�� ����z��G�p�u|L���BV�7�ZW#
;Ww�ipܷ%(6���j�F���G��5#��{$D"�uۭ~�]�֫�Sr��D���܃��f�Ҏ���Ӿ�+��T����u>-Z�T�Q&
N
�|��$���沸�ii>����
�e���R��W�ݳu'[�����O̻�j8���J��ۻEѩ[��]vni=���� ڒ,[��_%��k��C7�I��3N��v$��4Ɏ���Ј�e��ٸoU��u:[����}Do��5�|��zN�����q�=�T�r�e%�ɧ6��&���~DȍF]ƞ��G�5�q�
��m]���/���w�/
\ʲr�8��=�oʔ�e
9U(��W"�|�S]uZ�d�#�?S��e��[�W��"����ֿh�][�-�7Nu�:�T�=)�R�}�.;ml��*5D��l�f� �$fF�(̏T���
�hiI����U�U4Sz�ɕ��
��t(
�����%��_�|���2
������~��6�eM�����;T��ƗK[f�&]L��K^C�E2[��ȏB��O�d;�M�i�|�c�x�,^��6��;s��ی�G�p����Q���\���NuJ����IFT����J�~�đ��Ar�h�*
B"$���H���쉩�eX���PRj?s���l�"ԥ)�su���]�x��������������������������������������������������������������������������������������p�Դ��Y%V�ES��H"Ћ��J�ǰ����
��������K��&���5��^Ukzׄ8kE�g���S2h��&�Se���\
Y�����l�]W��Ҷp-Z�U��vi����7�QS����:4�byq��Oo+[̺�腋[6-���_��Fo.����6����[7$p��&^�
_G�Z�
���Ը�ߍ�k
���c
�������.�qqo�I�[�9m������߸���YxOZ�Ц��1u�o��i�SH�)P9Uʄj�cq=
S����>֙��N�eR�><;+�ڌk�%_q
T���]�.�s
�rNO?�s�[���=�v��H�[�]�RZH�R�Mtᩗ������Vؾ��:
����/~���u�)�ԍdg����%�=��e�d�V�rISb{6vSu=(�ܥ)mT�v/J�}̇�
8���
S3a�d:^h�BS��f؉Oɔ�L��h���I_��1d8�,�L>�<�_��A0y��3r��X�q����"��'(۱;��m�FNII.v5�_(^q�~��X�>y�{3�צ� I�����*V�ܛv��/jW��'
���T'��N�R��'�j�%�ꔩ���:mJ3��S�B}��!-H�-��R��JBТQ�
oe�di9�t�j�E�N��enPp�ke
.%4�]�#{:>����m�kEɱ��dY��Wl\��\���\'nR��M4�&�U>?�Ќˉk÷�!������]�]����5}UqG�~�ݏ�I"��O�~����s���6������(�Ļ)��qO~����h}�uԕ�d}�Q~��G��,o�E��!&�G&�/]_�����H�-����O��=�o��{�k\�̭bk���v�.��Ô܈+;��arZ���x)m�?�M�\�3l<�L��k<��C�q�r�KnV��s�$�\V��B�gD��]w=ʑO�/�>U�$mk�-C������F�X�j�T�v��6�u�'�
��g:V��n_��*��qk:�V�C�
��A%�'�4�J�V%EY)�����#BғO��4���<���e��jQ�Q�]���y����U�r4=w�
���m���[���K�1r�%Iũ-�
�������O�}����|k�C�;/V�c�ݩ�����W
Z�)��EHdž����T��ru��]��8��hgĵ-;=>���������U��_��
I�n�v�Tm�_jBM�+Q���iF�"9�*{�DI/iuo(��=Tz���ϖm��<�ot��?[�i��7�'Q����'�?XY�m�Ү��Kf���ݸ�I24�Ihg���8�a�C�[�ޥ����{䓵mF8�✛k��˱
�RR���
N��A褨��H�z(�1��݅�ӎ
E~���O�XdžN�{u�g�(�o��O��5衴�Q:��mU~�N�F�zk���se��\��ZjfH��7^F
��QIڎ�۪h/��V3j:zT���~�b����� Q��V)7�G�'��]��W
�� 1""��ǶM�/b5~��s���v�/|͝��'K��\�RI�_q)��DJn�f�JI���%�9� *��p�fr����
-z�B���U�W�Ԕ%
�OkM�n-Q�?�CZ�f�
'
����=��
��cj�.�ioi���=9�E��O]>�P�Q��l�_�v4��z�>��T������������������������������������������������������������������������������������*�ȴ�>�YF��;ε�\t�]��������E����H��4�ꌇ[�Vr�L����z����ef�
��2T^�V>g���2��~kg����5�~N�ק;{�~Z~�W��}&����BӿS2$��J�?�~��(�Y�"˲ߩ\�O��]��:��
�����JښT����{��m��m��I�ѩn3˧)4�L�dFZ���/����zU�G��
>�U>
n<�k
�5&
�ϴ�-�KJ����i2�����o]�uKljv�K�3��$�bԔҚ�V旧i��Y�5�.ί���fi96�v��7!v���))F�JM4���{�j��G�~�J�����t�����/���lUE%�p��T���A�Fe���
������4�
����q
Qk���\ve۽/u�/I���m+�W')v{\-��E|Pm�s7
߮D������ZRr۞/����mu�*�1�ՙa�B��܆���
-��x��g��3�#6��ۥtRogʌU)������]ZҞN�nŞr���}F1����Nnޞ��;cZ�{N}���ۿ��M�i����ux�ʉ*3�qi'�9
KHQ�$����W����J����x�Xyر�Ŕe~[v5�~�/j��N����9����Q��4
o�6��rJv� Fr�d�
�x�M*�iRj�M�zUi�
��n�H�����d� ��н�7�ᾞ�S��=��S��'�7
}�
��
�̽zt7�K|_g ��J�����=L��q+/B����������� �w�_\ۧ�x\�H�JUP��zQ��<
h��qF[�V��0x����==C��s��U�7q�|^
{�)Iq3�8��$�_A(V���gcKu��0��6�Ƅ�����"%��i�~�_��ˉ��k� Q���C�ܣB���8K�u� ��/ �u(�[��w��}$F|8T
�ՠI�.E
!;R��J^��}Mɒ�D_q2�
�];���Ɖ{�5�}*�n7nEI���n��O{Mw����v�}&��q�+v���
[V���}Ĝ@��%>#d�XQ��
�$��f;ie�p.Gq�uixVt�
x6b�j͵mlKقQ[�T�]�z���s/&y�ە��nM��'W����}����!�F�����p�_d�^T��������u
��N{�ɻ���'l{���խ��2�.�sT�u{��W�^��H���&;1����s�)P���� ӛ���6�����>�$�m��ě��;��Łn�j=�
�f�L�T�)�>+���qRe�ɴ[��U��R\L�*P�/!�$�Ӊ3Q� ������������
���'�K=m��~��6��Xq��W�3��^W�����+��ųO��_[�F$rR*u"��
���T�%@O
�+�%��#
]˽!aܽz�{��ͷvQh�쩎]���h����G�ތ�5ɇ*�Dz�JD���RNLi
4��������������:�{��~�2F�m�����X���Y
�-z��zĽ^f=�]��u�ū{��/+�&c:��M���a{�ĝDp2��m܍k�Hș
/(�-�-���m_vݮK(V��{R}�.k&��y�ƴ7i^�4@�3f
s��K�3�^��Ř�˸�
B�=�]��?g�t�5����Kb�Z���B��<��e;���kQ�L��px����u�WC�}n���
���5�Ҵ��e���p�B##~�q=��
`���x]KW��
F
��{��GfŲ�}��?G�
�.�I9��pj�W�k�U]>={7��q{�����k�O�
/��^���I3==f�1ɏ%n�nʫ��/Zu_�y��X�N<�������5���7�ۍ����'v�y/"��8��넭M2e�Է&�Y�,���в33%����
Ik
��jM�r7��x�f
���n�mQ�k��X��4��踼>a�-GcI�eތw���&���U���=����-�:q�n��W)z¥j
:��� Wq���S��Z�v����Ԓ��#�j�"K���rIU������)%q�r�mR��o��DGQ~����S�Y���Rsu*�V)
�
,�/�x�
)M���F��D�6��O�#]z
���9�����6[Ui(�JR� �fw'y��$�G�e�����U�ީk�������dMF-�ݻ�98F2��d[�o{R�n0n-���x�sV��6�D��h��|�Eb�2E:�K�C�O�Ӫ�v4�S�JCr"J�!�!m,�hRL�D|
Z��Y�Fm�/X�~Χfr�����N��&�4�Ƒ�= Z�9�M��h���.M�ܵw
�/B�d���rܥniŪ8ɧ���|y%[M�=��_t�j�?F!z5�
\e��v����M:��\
�����~�F�-�s�g钬�����������OWq���ii�ȍ<�G���i%%n
2rq�ͻ�l�lƑ��)���ok�w�7�}�\����Uk�-���:�&�f�j��솘�Xe�r��V���9yZu��ʼş�dF�C��=��rmo��%�����~���Z��N�78X����(�N)��_�7.Εn1Mp���J}�����6�2�j�j�J�dI�";�R�5�&�iL�Ը�c:jm�
�q�iQj$u�j���p�\{;v��5�
���B�Xn
Ą��4���qO�E�Rj���z�N����(�G�a��٠䌡)p*�v��(J7��#Z�ۻ��Z�8O� �W
uO�N�b�+^Qipv�������9G�v��ֽƼ�ϯ���rYƖK�G�J��Q��D��N�Ph�R�Jj����ᡧC"21
��"9
ѓS�1��;R�_O��7/�WG��z)���8�fE�%F���2���ukmv�Sov/i��Z�&�/�]~�K�mI�[�:�^�~ͤ����\� k����M���i����稜�\y�w�Jt�3W7
8��Ʒ�~ݥ�eF���g�Ѽ��w"8�VVSج�\�뻆�}�ݭ/J6�����Q)d|)�zU<���HP�`����7) ��ŵ
vlA�F�}��
��svk�{.��G�rR���s��Kpr[����o
��on���u>�3>�k��\L����=����;ow֯g�N3�pK�ѫ�|wmk���
�Z$�z^2��R:E)f�>ς��
���н��d|�#׆�?�\���ǔ��p�V�{;\$�Ƶ�E%-ͪm0�S���6�[n<
���kE��[}m�vE��4����DDZ������^ �$O��Z���0�����*$�
�~�X��U�v҅B�@�����^�?��]����s��o�#��%��o��j�w�;��Y��#S��x�x��u����eBگ�y v�^��i��-��)s�)�zV�� j��C{7�G����t�.��w�3v,�ygg8����s]�a�E�_��,�*E �����t��Y5k٨���h��=����o�"m泏:�\�6�w噓��ai�L�n^�c\�75A��G��k�Я��0���Lf46َ�`egZ˓p/�k��;�̛]kq����!ݸz�p�ԭG�"�}���R9Ve�>�ˏ�HUjJ-&���7
n�����r�n���wG�*���Xv��\���˱/v�N��}O)��ʼn��&C��V͍f̵]r�\��PMB-6Du���-
#��RͰt��R�����N^)�m����T
�_���}���nSȕ�
�C*_xBuT�kJ�W[��`ɩ���`e�j�v��sn�����gP
�ڻ��.��-���WU�tܑqԹ�Qj�)t;v��N&RNũT+8�%I�
�X�Ӄ5fK��՛�-d���9�
����������]�CƑ��m|n�Z�-6=�H��z,*aE�
��m W3Vz������Ršd���Y�~��X�f�׀����X�x�"]s�;��)5
�u�*����ُ�H�B��
��BRG���S�6bݶ�ؿ�
����9j���[�1*��������jױg�a7o�X� ���C�U�I��%0�v#�~\�-�O���-���Ꙛ��u
��ɷ���쏪&5��mY��٦�
�����M`�L�J��2�qK~��HZb�r �=�N�����'�Y���ob������I�.
��(���^ ��{_
��?�O����J��`S`3������B�N���[�}�5��w6:ǵ/���iS��l�t=���4�F�*d��&��T�4�y/�� #.��
��ɵ��i���m��5U��ֲ��f
�眕6��Y�7 f�ơ=�3dϕq�뚩$�q�TM-%r!$@A�?��
��V0�c~{��[{���;��a~ڵ����
»&ڄ���v1e�k������=�
�wb�����
���������M��L�kN�AԬ��w���-���x���>��~/r=�e�7
�3V��eV�N)�K�%Sښe���"���+3u �X���u
چ�rn �ֺ�VzscJ峻�m��}
�v�b㶓n\Y�bI��UBT���%���
*�,���0nov����=;��z꣓�S/nS�XSpl##����k9��m�XGr�Z�v^G�d�e!ŷR�Ԡ�z�QyjC�]`�g���T�o��Po�v�{����j��~���KR��B�M�Y�}�i[�
߶�9K�L�����2ԉO0K#���m����>�wB��[�ٍ+n[��[b٦��D�X����
ݲpo]��
[�\�m�5�qdT(�)m��o4�Oy9Ie b][���wղ����m���M������~v�m�i�۱�~�t� �\�}$я���i���mRk��(�L�
�c�
Cvk7r�9�_��r1����
�
;�zv|���F��@��Ky���Z�[��&�jE��j�i/��"6$69��ml��#e]��9s\���{�Sc�L�}Ȣؿ0��q��/�nZ�*��t,C���L�oD���߉���Nj���
ǚy�=�P��gm�u6�^�]�
�l���-["��çU�ʖM�lʍ�p�-���"�q�m���U>۷�u�F�OJ%Ǔkx
��'g=�睋�k[�3u��,�����{�³�Wɘ�ݪF���]ՍeF��X�������"�O���y\�,cچ�=���w�/��
g�n
Ļ��������]����#2�? ��v�q���y-�gX��n
R�.�^�}�ݺ�F���s{�ŝG����]��}�e|#�0m�j���x�"ƬW���كm?rgU^�xV�����B"�:Dt>�@L�R�����b�un��~����
ݭ,�w�+��v��
⪕;
\U�<�EqNj��
}p\
�.��ˊ&�C��+i�#^��Y�z�
���|˸��������va���H��ѭ�vޮ��=�oQ�U&��C��Xq��>��(R��Ya�61�>�#�Jm���˞��Μ9��g��9��X���Ka��G��='���u8���g�f}'q�y�#���ɉ�
�w���
����J�]�We.ʲ-<��+&����q�%s���?��2��dњ�zt�Ҽn��`��cΤmm��qMdz���
O�[��-�ߩӲ&;��[t�mܝV�n�r"��>{��x���<�8�U�+�p����:I���g]��z�j����Gk�t,u�<�P��X���vvK�A��q��P�|���VbL��Y6�A��u��S.�=:�gT7MN�5�{�_
��`;���W�zǶt�Q��5��˫c�%�u߸�Z&�L�뉩<�oN/`�(+�,���`�N[غ��zؓ|[��6m�lI��Ε�i���kv�V��&�B���V����=A������o<�%�
p.9�6�,n�
��G�.��Π[�{n�^ ���h4J�5�\�^߽ku�U��r`�L8aC����܄��<�<ğ�,R*I�&ľ�n�s�7+G�;��f�p-�d�v5��&_N��Ch���m�m�����3�s��4�m5��$���
��w�:�ڽ4(�Iz��|c�dǷ-�t����g3�{���t�Y�w�h�V��obL9�N�G�TfD4:�i�$�Ǯ�����n�r֮=�\\�w�z߉��}$���<��bP�H�o�#N�$D��.ʛq�59#F��b��㚜`�2�����}���
揺l���F�wM�qVo�x�T:B�Y�/�.�]��0ك��Y5)eXn�R�ʠG��o���e�e�d����X�o3w�g��Veخ{��r�~S�Q��>�zf}�d���ؠ�o��J��a�کq�E��q �-��(:d<պ
=���e�����Ky[�˗^����%ZX�kX���[C����2߱\�I�T�TL��GzA����N��M������i<�/�o;��3ߐ��v�#���^�Q�6[?�rɱt��
p��sp�`�e�ޭ���x;�OSM����� ��m���Kҏf`��S}�A��
v�����m�_�
��Z��I�\w��a�Ď�tnޅ�����wa�`Ń�r5�q�����ҩ�K���f*�n:]63�ŁO�+6S��iD�t��9�������������������ŲtUR��I��������������G���5��`��σr�L�Π\6
ZR5O��qQXu�A;�֪
I�fM�Ȉ���
r9zoQ�9�
�N��d���W�EW��jSi9Wf��f���w�?1�����qj�U�MYƸ�r��ڃI��$�NK]t>]K�>Us�O�G�DDD�.�ZF���6��*�
҃V�� Zhz{'���x�p^�`�
��wo8��r0�h�
��Z�mJ5�"j
�b[��l=�y���Uu7-�;�7�I���T�%��:jFj�ߖm�0t�zU�'���K
)��څ�Nۧ��YJ)��4IQ�}��^�K���W�m��7k���SP�>q;��ނ��#)'n7&������r���?��óM{I��w�R�\�j2Qn[�v
��pe���#/���tA����F\�ϵ��225����q�֒�om6z}
�)6҅*�oq�D�s��M�f
CN�I���N=T��� S2t,<�e�RZ�
��D��ҙ)BcI>_�ѧ�}���k���v���e�M�F0�J\Rnnݙܹy�[r�U�c-�j{yG�tkQ�%s���]5�qB.Nw.�JN1���L�v���R�����
��Ui5J
Z�E�S�Q�ԙr)�:MJ+��g�}���χ!���2;���q([jA����u�����d]��[ljV�K�3��$ײ�SJI�=�/|�&���
����t
�l�'*�n۽f�.��f���rܥ ��jQ�O�����8>�&Z �];��.��|7T�/C}�$ڋ�UmP�2R�e��ҭ8hFF\L�� �������3~����e
v�\۫]��ݝ�Nm�r�
�nB%*]Z«�h�Kc�=��B�T��LG���
:�V�7��4$��=Ǘy�+E�X��'��4tn����(�I
:�Ѝ;�D���f�8c�,k�1�%�dJ6.�j��6ź�{N~l����6�&������*�f�œ
I7�
W��A�lGO�u��-��Ң�H,,�
�(�ǔe�����뿋쩨k�M��܍ ZſgR�vQ�' �9)?n���|�e�r˭|I|-���f��GK�.rΛ�p�8XV1��%K6�mvG�+tc�+q�E�
&��Ǹ����C��_��N�m:��l��=_��/�m5^��[dߌ��ڇ.c<��%:�)��t�Q$��Ow����~�-a��Y�;UJ����>��=F)�2[�n�k�����؆�?훐���
�M=����l6[4�(O.�]�2#-H�^�n��#->�&m�p���5~Fӛ��+�|��|�
�S�,��xa�g%�����q�k�EUz�����UgæBhߕP��(��7]����k�Fnq?֖��C��pru
�Z6*r�E�ڊ�tS|*tI�*��E�}�7R�<�,����nU�U��֫^��I7��Q�*��mS���l��y%rd�ȓ��d8����hE<9oH��h��M���f��NS�R��j��[i7�D�[R��j��݊���+kდq��{"�$�$��H?p���������������\��̅�S�?㭻;�t~�� ���R��߁������
���)^/>�Qj`y��t��[w ԛ;�����²
�~�+����ߔ_ YW��~|o]���
��
?��x^�ᯛ� `ʼn��;g����)T��@��vW�n��]���>&4�l
�p�+�$D�������̢1��l�|��ȨF�%����-����}���.�9[}w�~�
Ԡ���LM��9hС����ablf�e���&Q�oW
���!����s�?w��j��L��K�?�s7�y��O�>(���=��C��~�_n��y�ǜ�u�? v�����3vyo
�o����I��@���qV-�jeES�^�[�9W�oS�ܝh"l�2�C�1�a͔��C�iJ@�3:Pճ��w�=���/7ov����uk�+\V�;���l�D�gն�����<�[A��+r
X��~�d�;����m�!_s�8ݖ���;��;����.�0llUC���+��?�i���#�_�c�r�ʙ1~�C.\����q ��
u���l��8Hܶ�2�����m�`���ܻ�M��3���T�o�v|�B�s�
���� r�ɵ"o��L���S-
�D���w���=T�v@�f
��'�6�|YlD��͓�Y����%����-�#Ѯo%:�&�!�3o%�\J<02����;K8�7���>�^vgƓ�# ���;�ݝ�mz�^Y�6=���P�S39���U�%���~
�&f#�
�}o!m���uH�;��
ʲŇ��˷��yvP�+�&.7�e��[3'��v�R4Y�j�̗IZ�`e˽3o[W�U{�
�m[�sU�b���ۋ�ZǾ�ۆ��l�6~9�'V*�.\S2��<�Sd�*zY�[aŶ`]���C$n�.�v��^Ʌ�
�dng>ەZ�����,Mmϑ�
:�n���6�nϦez�W
qUJ�4!�
ۇ4�R�! ��=>>F������n|Q��[{p��R��O� ��1��7��ƕ�~.�_����I�
'��'��00���k=b�՛o��}Osð���c2�'o�\�3��}ݭQ�^�
�2
���.� ��R�1��yK��ȣ����t���Aݿ�-�u
ܾ�w!��`�?1Wh�n��|�g�z��U
��o�[�E��CW��w�jUIן)^h#�1�ɭ��!�/Z�����
�n�p;o�;�ΗŻkX���s."���6��E�`Z1�
עӐ���9Kl�8�q�d q�} 2�St�t;��#���j�>;խ�a��b�ONŗ=f��w�P�1j)l����6�J�̶|gV��2�`y���/0E˛��6+ԫ1�?
�6���}��KW
c\�K�oKͨ�2ۅ����F���w��s*T�ԞLיu�Dx�� .���kC�zW����X����hy�۶g�L�u|��%Tnu�pǺl�-�����S*�� �P��
RaL����n����T+���c+�*�xl.v��!�.U=���|�; ��!_L̎뱚U=4�hm:ٯ�"y)$�:�>��%�(�n�}X�'��p[�ȴ
�^���˒���4kƓm��zD��x�
\
��'N��q
a��m��P7�n�yN�݅�=������<�j�v>�j���7%��M�cS
�ڵj�%�S�T�y
��qX�y���m��vC���g�{w���/�w��=wS�W5r�̹�u
e�rծˊ�sO��m�=�D�h����E��Қ�R�b#n)�Q�Oxtվ����Q�we]�I��}��wC��a�'"[ۂ����-z}2��U�u�KP�$㜉��ԧ:��m�c���<�Ý>R���oL �?������w��u|%�ҷ&�����K��
y�_�!y�9���� ??:tq��3�(��U�U�-�l�k�
�S��'���ɸ��@��j��dz��Q�ˬR]� EV�PW1D�Jq��2n�:,
���c|ǻ̑��;���y�{X���,ۂ��.�u�.b�����˕u�.tK�B�jQ"[�S��園S�`��ٮd�Nب�e�����J&9�Ơ�
�~�0��a�(V��m٘�L+J�r*�vڑE�(�
��x���������0�+tp˕
�n';�w�m�-ޜ�MOxX>���{#�2%j�g��b��2�M�[�`���K�*\������5����@�8���l�'e=0�u+w
֘鳾�{y�܀��:R��*
Y�a�]"�<�Q+!�
�")WJ�X&�a*�z�\�8:�t�N����7�܃�m�팮�xWq��۷����p.�'"b����H��'��FD��)o#�6�u
�l�l��ۭ�y�����M�����Y�/+
a�ڍH��}:����:����":�J�&�3���Q �@>�Ӧ%kty�n�lۣ�65�,3gU�}��{GY��rb;����ge�'T��K�w
ǘ.��,�r�p�ܚ��V���]����T�r�,�!d�p� /ԺU�,x��Չ����
�>�s~W�5�o�Th��
y ���������x�?xrr�x��?)�?���il�bT��,������z$�Ԏ.U�H�٠\U�1p�U:]J��wS������r�GZ�q�8àd驐,N�67Q
���YB�Ӣ���D����㏙W�!Q25ϸo9m�s-�7���-��%�����3���Cih�����O.J�鯽��-�;M����Z���M��8k�u����-7�k���9����S���$��8���]�q��2�E(�}����b�ۏI�[�DK�OK}��3�K�
U��B�^u
%�����Y,u.-&�f#���]'܆o�$x�`Y���u�,dz�wM��;�#oKx�n;��\[d�7}Rb�+*Y�䛂�Zu�Bӱl{j�0��O�̓��}L�hK��;[a���ֶ���aGL{Cb�#��S�.T[>߃F]NK��"u^LUʐ���_ykW?�!����G�R��j��2�9��͖qa�'0[��n�����pcD�vV)q�z�9R)��PۨM�
���^aJx
W�]
r�>��];e�N3��v����xd��m��Ę�(5W�2K1�䪖�weF�{m�E�/���QP6\u�5�4x��5[hۮ-�N��ki
[�l�U�g��L]J��}5
S�:�EhiU�r���gH�l��!ŒJ$�������������������pe�=���q�^�b���͵Q������'
?�6�|��
R���\,�JA ��ڵ"T���D��ꈭ:����y�mg���`�B�5t�%M]��
�<�N_z�v2_O��rtٵ/i��/ReӮ��*��
7[qүq�EG*�� m�"��[�I:�6�e�^��p"I$�jԴ���ęh�!m)]�G�Zk��cjS�!{e�^�z��}+Cѥ��9;R|/�ֱ�ei�U������ԏCN��u2��Zhc�ٗg��$�ݭ��wv�r�
P���8*�7/Lk�~�I'Km�1��+M�W��%���B�k��|����oOm�>��-�#�qj�*��|�D�<���Dr7�w?�I�hi���CE�%2m�F��ۜܧF+j�����t���tZ�T:5>bѱ��k�n|���n��{v���#�j���Į��qNpMIU�m������(��7������L��iz;{�Ҝ�ݞ��ڝVƚ��V��Ϭ�+sO!�Os�t��G�vx�Ӊ']uӎ��4�g�_�
�1^-8ۦ�� k�!)Ύ5�O���;Y�S�B#2��Zzχ���;<.�ֵ��Ot�ge��~��.(R������C#�w�FZe
��G��Z���ٸ�6�FFJ4
�e��2�ˇ��pJ
T�$�[�wg��V)�q6��muDG���J�56��q
\�I�����!�̗
y/
I��~R�tJ�9kJ]Iy*��'�FN�� �0�s .[��l�����!��� �fw'y�(7$�œ�����
W�ƫg�y���ΙdMEU��� JQJv̋v��mr��ۖ�
.j�W�����R�_�M�֨�d�j���YgSj0^\y�'E��oE�Cjm��$�
I����Ʃ����K>��Z���2�8J2T�i�J2N��#}.��s
�cA����rl�嫶nB�.FIJ.�)۔\Zi�M>��/h��L���ĸ�=C�����1�s��[�?YMqp��|
��94�-
��鮝�����𦔽/k^�#�NT���(Y
L�S$�6���˩}��{;5 �)B۷��W���$qpN� �)qqoo�t�
��}��Z����D��V��ә;��7TiK|�6�f���3
��h�$�dԄ}�f�q�ݡ�>N��b+���Ͷ����O�]��>�ߡ_VtYf��79ڰի�F
s�q�~p�r��ս�|Q�M�)g���%l�0��oc��J���ȨHz
�V�;B��b��/����kL���A��
cf�PJ,�ԭ{ƍgp���jN�R6��V��S�I*��$��!yV足���j�ᇑ�.]�(E�ܣ�����q��M\���qJ2����eZ�T
�).<9U��B/�(��B�0j)����mt��K��Ej#����fDI-=��r���Z��ړ�j����|'Nڤ]k*��i$�5qt��"ݙ
PM�6E4�k���e^��Z8ۏh�z
$���Q(�R
����
A�y�2z�fRñn�p�������nkbk�I:=�j �
����&�ΝșW?
�d����{+�ύ�M�
��'?��?�Xq��e���e��Ľ���.������[���o���=�Ux�F�S��=��ӷ�dZw�e��n��Մ������]��_�X=�ĭV������a�*
p�K�s0ބۍ��<�jT�Z6����G�����
������G��4�ӵx��չ,�p�ᒊuMMx��STT��tl�
�Θz��4�K�d�&�k��ͦ�j�;���SԌ���ˁ��Q��zz(�M;D���yƔ�7�W��bqJ�f�J3�
�gz̚i|�wnxtj�c
¼5$�{(�1�f�� X�Q��65ȼ�b��̶����Z�k�n>%�F�����Q��MJXӡ���{TZ
�E��V�N�ᖣ�im�T�/��3���7cNJUPn�����P��҂ZO�E�~"��-R�c4�^b-
FEͧ
t f5�[�)�S!��O��Z�Iښݲ��͑���;��t��vܡ+N��
�)A�R��=��h�C�N��n;��w�L��1�6-:��特7����M������$�=Tҕ-�.��R[Hٷ�����nX��k s�n[�ҞD-�0WS�����9p�9�:-�Ϸ�-�
��jѬ��Nu{ҹfv�)[Ľvwf�g(ٷf�e+0�mY�j�8����Q1��\�ݧ�g��]�Eǎv��ڿc�!4�#j5�
�����̋��C2"����}�B��Rr�i�F�p7����=ô\T�Z�:\BL�fj#I�22װ�<;�
صZl
j
6���
:�l"��6]۸
�K'�6�R�T��ѯ�^ئO�ԓV��\��?�$�x�7��s#�r�:��O�h���{��ց�=M��m�u��H��Էd{��p�N
�/܅:�U�E�#Yy
���+(�S����gQ���(�Щ)R��H����z��w>����^�Ѿݻ��>�mK &^
�'$�J�ۻ�&w%F|x f�����z�%�˳�
L~3N?Cy�9����������
�v �w/�{��ƿ
�kz�3x�>����
s��X��v�}�v�P"�@���WyC�
�z�`�'�
�톽D�w��%-�t�t
y���V��Y���\wm�uPY�Q���A0iG��-2
�JP���,����6��/��gˢ]���u.-n��!Zw����.�N�7Q]�����Df}Q�0�� (��{�a�\@�=�i�_�X�7g��Fǘ�8^��
⻲}�G��
�M�Z��1)���W��Ef�O�1�2�G�+=-�B�@z\����`|��|���w6ċj߬�m�}�U���w��Ro��x֢I���
&c~X�GP��6Qnd��pv��ܻu��l'V7^F��J��t�^{��b^��B(
L�~s�ѣ6@߿^�x��qU!ڙ�5�|�V��p��v��ef-��u��ӥ^3�
��
��F�SDɯK�D%0��r}��F��F穛���r�7
�+o�"�V��8�t��v̖�N�QU!5�uF���d"bCr^bJ=�֤�fM������#ʳԷP��0�O-9x��������R�B��m\�=�`�r-:���;~3T��l�(n��XtXi��%2Vٛ�#v��� w�q���ƴ���`�L@���"��H����
��q��W.j,J�M���5B[)Wܺ������������U��eZF�q����c'V���˷1W7�V��̾���-�M��H�Ф�w�n����8N�;��H�P��S��d��ݷ�C�7&�2 �j.�W���\τ��G�Ŏ��'�V���b]c��.x+���R�x�1%�C��2T����
�{��my��g[q����U���|�+�m:M�:շ�8�҉yWd�)Ջ��W�S%��%�����:��iq�����l�ʹ���m�������G����wݹ
W��nNŤѩ5(9� �hT��ٵ��DdG�Ui-�)vSs�2 2��{O�nT�$�����X��ck
n:�¶��(���lA�S�L�eȔBjμ�Pp���Tb2~
��N��2���~%�^�k[����ܗ�[�J�zs0�ӓ
�H��BKq[}��Jَ�A-�$�dF�����Q�gjx�xF��v�4�r/x��*Rm�%�
�����`�4�J�(�&�i�v7�S�k��Բm�SH1�����Y���Wmx
8n.���k'������]��:�Z��˭_W
>ڃX�Щ. ����jT�q���%��A�ā��[�E��}�am�c�]�D���:�rm�H��Ri�u:�uӚ�Ӣ\p(5�����<�i�J�$�����@������������������������:�"2-{ D}�ٯn���]��Q˅n�{
4�*ڣ�q=W���s�-�K"���;ĝP(��7�
��.�0�
*Lɔ��EB+d� -�m����O���sЖ��B�״�.rP_��ۍ���#jw'7'[p�r���'���0�WS��\�}[��~�,�S᷏�rv�k"^%�V�����9�(ґ�F��3Q+�����%
۩��fF|9��
�I��nܯA��%+M4��5����q�ޟa�+Wl��ec4�qq)*pJ;ԣ%�\I����T�;8�'aji=�T�L�E�222��|��l�v
��Z��m�ʮ��
�T��QFok^��T�8�&��n��rF<�K���fssi��-IB҂W��ԙl�S�U(��%�s���Z�����r�3k\��������+7#Ɣ�N�~Ӝa(ɧ�J����I�7NyS�
�����b��#&����nV��(F��\��۽o�����[Vʛy�}�w�(jD+_,Q������-
�f\�;pZ�%�H�[��x�7
��'�Zu���ëܹ�l�dc��$�;�n3�IVv���.NӔ�R�{w���勝��wmeY�����9�gۅ�٤�s�ǽ��l�)[��GcMN
�ٝ�/�ӷ��*�T�jZ+��ݥ��/�N�7�*��22{NN�Ġ�«������������
�h�T�x����������Q/Ur�sͮ�;t�]{E��e��]�i��=]�b��;
���.�Ի�؋e�{N�m��?�[&�*�U����
�
l����&x;- ���
O�կg�}�LU�o
��|�ҧ�k�lkӹ��:q��v)��K�t���5l1�d��ז�RS���������Tt'�\)J7YJLӯ;dGΗ: � +�WQ�ۜ��k
�:�Zrp��d�>-�q��%���e)(۬ҖȽ�I�����f
��<����߽p��r��&ݫV�fY9�1q���2�ĭ��EQ�g�Y���bTGQ&,��y�L�+��N$��[q*RVۉQ �=F�u�T�ܻ�>�f�>�f㋳8N��6$�܌n)9&�»����i
ˤ�s������X��,݅�܍ȩ��v�+sR�Tp�O��}�d��?Wn��/I��np��ȸ���%O]S���t�QO|v5������\}�����7Z�wb�.��AI�V���������K^:w���
b�{[u�ݯ�c��yt��O����߶S��<{8KSR�ׁH̏��N��7�ۚ��[x��kw��Yy_������'�ZӵF�+��>�쌛Z�U�Ħ�r��eE�9�������F�[2���4�D��e�{}@��:������ExWs-\ǻ7�K-\��JN���vE�k���%
��
:s˙#κ��]��.��o�ͳ;�լ�7��w�B6n���w�u:�$���L�������; D�k��I#Wz�����.:����X�p��(�˅v$�Sq���
���,�wn\���q�I�N��-�����e<5�����O�e+v��u���YT�p��cojUI������_ާ��P8���
�����O�
7&�V�L��8z�$�_�B-H-�[u���h�]T��{�|8�
��=qVR�N����-:
���Ij:7PUtXϷ��m�������y��鉿:RI�M~�33Ӹ��S2#�׳�����G�dŲ5+/�B�x{(Wz�Ȩ�����5��Y�㞎�#|�˖�+�
�ط����.|e��<�o���/��r���ߔX�
�>���7s}V��E���.
��OV�ti���
.5���nN����J���O���"95���{�����#q�}�Ay�9�d�o�]R"M�6����z\��t�nN�S���-D��!����@3���N���_�ji�cW���sy��*�5u�ٮR���cWv/��.�,�j}
=S)�j5C��^�>
��I�e ��=�g�u9�ӛq�jtz���
����]۪��TM��o���ߧ�I!Ǧ¶m:�,�����"[L����!���{��q�A�v-o�
�3�{�"K�ʼn�
��rIkfٶ�j�2�ƙ���S`�7`�
�k�6j��z���������ޞ��[X�?e5�G&��6�u��ʷ2%ԒR�K��E��*G�\�N��p�o�m F/V
�|��C�0� �.�q_�eenƣ�<5�O���h�'����6�7��ɪn[�SĽ��{�ڔ�jǘ��z�s;���~(ۂ�����`��ܢ1��ƣ`
�_l9��V�a6�%�UQ�Wh���~�P
~\F^Z��HR@��:�ۧ�C��J����
���{ôG�eB��h;~������ۧn�U����
J�\�O�+������n�2� �RҠ)����n���
g}�K�h{���5��+����S×ܛ
�.��1Z�jG�)i�R��ȤI�N�
�4��%��{o����/e�O[����N����ffd��
ĹK?n�nԼM�qX�'܌�nZv�q<���ķ��bFn��ͪa�Q�
`�5� s��,�M_�����լ�����?�������-��@_���{��w���{���Ӻձ�J}G�F[�%�v\�5[Œ��G�k��O��w/���Μ����M9�rj
Ë�%�2���+rd~��+���������C9�U��۳r[���a�Jǭm�|˒LAʨ�SC���q[��X�Mۺou�b�fp�:��t�+Τ���Ļ���o
][��
zt���-*6�7�kv��S7��D·M�MCQ���Xm��;)�n��_h�%]�4ܙn��������R�k�!��]�ڵ�sD��UF�"�`R,
�&�#R_��*[�z*ZqF�Xɻ��
��]�7|۵� �
�w+'p������F�Dە�s=r�.�/���ᐚm3H�ש�y�
��yD"��j�H�C�r�'���:sA�6���5��نѮ^���o1V/��
f;�nF�r3�V���M)e*-��
s����
��D'H݅fӧ�\*���[k<�7u�<��-�]֍�Q�8R
���h�|�p=���W��l�W3s���%Q
%�3�l}@��U-��K��6f�-N���Ͽ��u�|ڴ���m����W�N��[��F�*m�W\���%r��!�
��C�78���:�vB��G�7ŵ.J�թԚ�2�x��)S�T!ř�n<����J��K��ׁ)�R���g����������
�o+n�I*ۊ��݁�,�nd�Ճ�1ݕ���e�E�jA�V��u֙U�=6,48��~$5E6�jo��
���r���w�]��_���-�Ở�c�
ظJ�Z�Y���p�Fޯ�1W.I�V�R���9
)6�P���T�[uo�$}�
�ߔ�}.���s�{�-"��&���D�m+�}����@�U�
~L�m)�M�As�����>�~���9
��W��:�Wp�ܢ件�{�xf��8�
�ٳ�wK��E
ҰWx�V�B�
�\�q���B
Z� 2�wM��b�[l�GS��n��yԚ~��z9Zmያv��oN�2���A��f��nݽjf�>����)�j3���
��!��;��gO��Y��ʹK"�
W�ftڎ�+b��*2ϻ�K>ۢӱe�yԪ���X�ISUm[��z+ugX%0��l������Ϗ���n��vg�!�;t��{�������Bq��P���j�>P�y�v�R�7�Cj]O%+ݲ
: q�iMj�6W�}��3vC�/R��=4�Som���]ŗ=�ю���,
T��F�6U_-\6My�skwMr�&�Q\wj�K���ܩ���yM�ϣUj0��*}R�Zܷ�SdY3
�>��
���� Z��jqj6�Tg���z�p��A�/�M���`�������/��Cm�л,������f��e�E[/�+uk��^�Vs1W$�G��(J����sW2�ٰ��u*��q��*�����Y�.�Wi:����u�r��5�T��),=0��u�R�m�h���o�.twܖ�iY�wr�WHn��t�vE�j8�q��h�f�`Ͻpf�(��R&����>��K�i�%I7$QӖm-2��
�~y�ߗQ-��앑/
�������x[�k8nw.c��㩵k��}]�F��kbJl:{�.
�(˩��n0��Hqv���αp�������7 ��귎�.G�u���p��x��[�N�� `Yq�'�+ru����U<�J|�$�ɯ>�7[��ү�+����>���!
�x�rȫ�oS��o]�OC# ������� d�^���Q]�\�>!ƛG����w^�M��x"��-+%v���dX���-:�M�2UR�%�d>��%l�
���i�oS
���u��6�ls�j�7D�
�P�>X�x�H�z�
�U�k ��(����n�^�����Q���
V�>��5�cV��
�tWj�
S�Ei����J���dzny��
e�j[��lE'
3k�uٌN���n�4��JW)�g��������������������B�
��{4����
����j�� �6��&�]'
�m-(ZM� ��E���z���8�cz>�WZ�6�#���7+��[�,�M�R�-Z�!��4ܓt�Cy�E|��u�m���j
��1ƽv��ƷV��\��;����%>Q� �:��#L�e�(�iV�z�5�����
4��ũ �ۤU�Wx�X�
�^(Ҕ���s��
�լ�B2w-�V��
^��R+�;
˂M\�z�+�Uwr�+RW��Y⺧~ Q*J�c�������YSNS���λ
Ud�8i�n=�v��
�K��낫k\�I�R�רS��Ua�CF�����mϿ5̗P|�u
ZT��ԕ}�>�����oYѲ�1s��fP�+sQ�kX8�Gb��~6r�,s��>^�\,mGL��+7�[�n-�E\�.Fq���ḕc�l���*�Jm��jb�5�
,�m��]����<��EC�H��Tjr\݈�/U1���駚�
�
'���+IC"Ҍl�1J*w�{%ˎOl�c���nZ|��t�/^�1t���
�r��9�ˍ�9V��$m��c �N7RNSi9N-�}�y��n�z�NA;�lV�պs�4�̊e2L���\�O72U�ȏQ-4mD�,e���a�ڒ�v/[� S�����Wa��d�>c�}N��X�f�e�V�l�Ǹ��������J5�
����eˡ$��4��
����%� g�~����N� ��p�4�Y*W��w���W٧
<8v�#���;��q��ԩT�ut,
��m�"#Y�
�D\5V�`\\Lȋ];Lȇ�iS����6�ϝZ���
l�>L�r��uR\��v=������ǘϔ�Dg��=�Ԉ�dFZ+M{�=��������|�,[��;�0�>�RiS�i�4�,�S5�}����y�x�w&�(�E7&���f�ݙ�4�
�U��Օ!
~'��I�d)<�r����bK5)KmD�FfkivK� �l��k��j|�w
��P����r��*J���r�y
t����m
�}
ZG�>]ǽ�u2�K��-fޭ
�\0������8��V�څ�쓬=��V�y�^^ Ih�yKR-�B��#Ըr�=�]��mܻ
Ӿ��'*U��mk��oy�
rTqT������_i�,/8Q�^���<ݤ|4ԻO�(�܄"�'5N��~��#��m.(��Ҿ���
2�i6Uev��&�I�*�
�<�������}��҄��$eN�tÛz���yWJ�ub��W��^�i�BW.܅���W��ڮ�g�]i���rO6�Ve�90�s�gv�.��+s��V�aޔ�[p�?�3q�*Fu�tUo*���e�L�\KM'EG�*ZcA�FfG5J
�5jj=MJ3�OK:k˝'�NM��B7m�3�uFҕ����\�-Ywg%�PRq�M�IyZ�GY9��|��μ�v��n���5cW�ݷ�a^��+X֥vnݘ\v��7
�m��>�Fg�zv�"-;�E�w֝}��1|R�j����N
��
�����7�g��#֟�*��G
� �Q�Q���|��#/��bo�]���p��$��>_�Un9����������г���Ub�n�9�׃E�rQ�B�U-���^v��D�����m���Vh'<R[fd��
��H
�T�]*�~���}�
3j;��nv�jc7s���-�rӳ�� Y�8����[n[1�
�pJ�x�
��kX[J��k9�M�n���!_�N�ю6�x�:���i��Z˦U��
����|߉�^Ԛ��݃�h
Y�x�k�
&���U���^
�
bwKk���.[j��E��+P(�˞=�
9���j�@���snCv��7���%����c�_7=���x
�ǁ�< ��l
�{t������'酚�+��1F��l���:���ݻI����Lr�uǶkL�-�L(K�0L<�G]}��j�v{���aL�L���՜w�g��*���1"�N
�V�pj�"��
�R��$�s��L�Gl�T�H����I�-�I��.�x�u+��Q�/�J��l�~ȇ�jvQD���r�ll��W�mR
��[�)S�!�%9�aq�Y-���x~���F��i�]�կ�7c}��yeW�R�
E�^��L��i؎���y�K����☘��ꖙ�y�
��j3 aϳӹ��
�}�z��{�m1�졳�SWچ
�ZXꕆ.�Z��_�ZW]��s��u������z���J -&�f��K���-��q <����mV��/���,���bˇ|m��~a{���wݾF���^�_7��2�c�e�Lv��]��m�#�*���ǟ
� �g�P��
������������x���E���3�W#�ۊ����
�6����ʮ�6�r�}���
VH��&Z�
+e
�W�ܨUmE�bґ:
1�m�v
4F"
�8tK���{�f������M���ǒ1^ٷ#o�-�Wjé[�[��[.�ۻݖ�T�\
d�Ȉ�2O��$Fyl�.�����ɻK�f�:��'-u�wt0�����1����PUM�?b{�T���fڮSbV#�TR�f2��9
O�����Y{^[�꩸}�bM��϶|�4��=�P�I���wxc��B��b٢7�ɭ&
J�R�����,
B�#��W7�bm㩮^�N���qf
����o`
CL��3}�����Q���.E�@��)����M�D�KK�U6��
d
���2���]r �!����s���������x�&*��� 4�|�����S��<�7��3��`e�հ�����⮣�5<��-�^{\�7�?�������㟘G�o��O+��q��t�|�?c�b��cG��q��M罪��?�u�w{um�)��`�|̴*y$���WnL��)�(���Pb�c��aJnL�\�(
Y�9;C��c� ��#����~���mt��L�P��}�s\�y\jݪ�h�-�
�s�Uit�\io=D�M[������M4%�¶�u������
�(H�mY��n�yu{�m=5�n�&$��+����!��!�
�JmdF��m��fR�oJ�����������@��-��n�#�pe����:�r�Mņ�VN�r-} �]r
%�G!q
֡
0,m��Ћ*F�g�g�^�9�i�
݅�{�;��-����F�*���ɰp�v�%�o������ʅ
%A�%�_;*&�b��'����-c_+ĘåmJ�;;iɽ��{r��4�kO�O���tI��N��+�J�=
��JC��Cj3p����F�C7
�Eù��{2bΧ��3��oò�YlF��� �*߭˹ox��b\��:�2��T�D��,��'���I���,���-��T�>�1&����>wX�
�B(p��m�;��1�f�pn��l��p�֓%S��kid��� �kt(�U
��+��x�ul����o'/�ڕ�e��N
�r=^�pZ��Z�:��Pnj�8���Hf�"48��i�jY[��
��N�[��yZٻ�+��=��������
ø:��3��
?^��ܷ^��S�r#�Y�K[UF?CuhC b
]�G��M')mڏ��s��N��rܗI�]ljq6V��B�. W,�
����UK"YX��5�{�c����
�>�Iqā> �T:n!,5l��
��2���Vz�C�l|+I[�*SrjnS�6٨�y+x��,��@>�П��.��g�����+��!��rn��9>N|�W>�O�Z�T_u�t��
����Y"���"�v�7�|�s�fި;P���cl�m�� E�ùN�,{�'��f�N�T���%U&�LfH�8�~1��v�>���I�l
}统u
��6P˗���c�(�W���V~H�^��bM�U.o*�oO�F�0N������:_���:6S��mr_.�b��+����|ݶ��YY
غ��F,���m�w����j��v�>��f*>QM�뭱 �Sd:`N�{��l�/⎱;����n�-��z~"�G��ze�
퇎
��J5S K�G9�!�Gn�
;��N��1� �ݎ
�h6��m�|S�?���ɂ�5�'�����W
��OÞ��� ��7�|� 7��^a�o @m��x�Gm�i�^jϽ>01Mf����0լ�D��������3-2T��.
�VXR"���ɥ���V�
Kl
���J
���O7|�����u��?�b��vа�;�6.��
�������
eߓ|[1b�mR�r,�e�Rz�`z
��6��-ͨ�ku��F�ː�
d��P�hY�
gZUj}n�v�X�;z=�g�V�ե��������Tv_J��� }�\��1�n�7��w2�J�?ޘ�γc�\E�
1A�ޑ��z��q�;�\��r]]
��\�Y�&[��n�s��Nei�������������������������\u������UR�
je*�Qk�2�C�S�l*��x��Jz-xٶ��l�m+����|�Uj�U��ؓ`La�d�q�iĩ�!G�d\�W��~f���z��;T�n�
�*�P��d��RM&���T���4`չSW���q5�k�훶�(N"Ӎ%�
V�]��֦�����w�b�.����n�U��O�!�u*����J�������&�Oӕ�2e|��Z=e�V��쫚΅g#+�/�R���W
:����طn�b��i*Wy�o)
p�{�:E�T�KؚR��(�R��Y���+��r�웓r��(��I�F�)
V�m�ȵN�B��:h��
Q 1�ғ�|u�8E]�{,'�$��-�TR��[����j4���9�l����*3"I��鯴z�hd�>���Q�+�\��B�kN�F���=�.�$�ZR�4�N�wհ�(I�pN���i.(�G��i33#33�e��<�R���ʴዣK
_c�OP�'/n�iQ�������+
e���j�V�nB��*���$�lWj�����FX�D��a�㶲ԛ���#�
�A�k囱��g�b�/�Z�v� �F�k�c�t�L���r�7�zVu늞5�Lk��UJ���S�%�L�Lg�Kt�\f�ݔ�{�� ��Tn
=B�p��/�[uZm,��FFj���3#ׁ�� 6�����������;f��w[쬞R��a
y����֩nY<���agJ~�<|g��ء�\�t�Wj��)�=u�[iMϷ�G|���A��)��3Dz�
�I�ԭ;51�0|�h� �%�{�����,������䮹h���Km$FXK*�Nd�Wr�u���d�[r{x�n���k$v
2ı
h�+J1�T���Q�[#JQl[tRO]L�H�K�����ٮ�� NӍnF�����֞�������E����m�'����MI��L���B"ԋ��%�dBŋ���+p����̿�_1���7��jz�T��~4��p����c �Vo\ƹ��b9R�q���-'�1j;����8ܗ)hE�%�DZ��K�S<璸�Bu��*%�*�Yw5ڻ�9��ۣ��^�z4��U;
Ñk��\�U(���o~��G�?�VU�Ď:?P?���� ����_�F_�K��ߤ���~ᓾI��
|�p��r.�����������������������������������������������������������������������������������������
Ok�\����� ��S�k��l�R�hҪ�����z{�P��
.}�SktZ�7���U�Q�4ڌIM8̈��e��a�ӊJ�Z�%FFZ�u,KZ����vl��n��廐S�N��FI�V�tuN�i�?CM�5]+P��h���,{��j����N
JS�R�����$�I�S^��t��S�U�V�r�OR��Y�u.9W��y��
�P6 ��[K�i��u ���m�! X|�]Y79���ӄ�)\ģ��)pbڳ��r�%*�&ꑶ_- H*dzk���)�1�
V3��')UA�Ϲ���ٶW���R��xe'պn۫�h7
�A�R�9
�E�A�J��e�G��L����ms!�%D|
�A
5]/Q�3e��b��̄�v�nV���n��%���z�a��\�m
���kZnv�(��[�e���m�qrI�ҕi����j|��""><����hjJ�שvvǕ��|P��ޟs�}���V�~2��&�Z���?�+2�N&Z
�4�w��@�)4���i��S���ڪ�_�>/�J�N9H�i�ۏ��
uf�8�'�I
t�[��Ȳ�R.�hZ�$ȋ_Y
�~�U�<���UU��O�*�6�b)O��vz�ڜ�j\R��̋�.$FsQ����u��Ҋj�^נ䈈��y��<��z�Z��I�uP[}���Qm��
�=����C�?���z�N(Exqu/��kn
���S�-FzK�Z�zOס
��ӽj��J\)F��3�b���!��r�5�����ٝ��|;6� ��o=�
��-3*λ�
��]�αb���\a�b��q�R����i-�w�⦪�~b�8Kp��o�)��Z�=>)�ғ"5/�GTZ���L�E��-��輵�f7ݘ۹~�+&��+���w/7G�F�I:l<�u���D�ͳ�nwԮ�;�v��de|�
��Q�����QQ��#=Ε���)ǿ��]�ff�(�S>�33�fg�.N~��۲��\2|*��c�n���er�m�����n�n����������M�����+�Fq�"�ѪIz%��j������� ��=���
���YW�8��@����~�gc��/�~��?���N�'?�)��«qȸ�����s���➟n�=���k"
���Xm֮�Vre�M�h2[�uݖ] �*�Fܖ��N��)M��Ȑ`f0 �g�,C�9�����̑o;���d��dudJ=�In��13���:ݒv��v��dMUE
JL��p�^,6t-@͐��9'{���7m{�-��3,�����>�h��nF;�Ѱ�
����M�)�->�>+Ěz!R*
:�����`�e�
�--�m�7nB��\u{ b����
U��>�[8�֪]��6��^ߤL�ʦ�\DF�N�
o�$��$�dͶl�gn�o8Or��sQ�\�l̯hRo8t�u�N�o�+��
�C��Txu��!2[�>ct����F������������������������������������������������������������������������pe����ޓ��ƻ�ֶR�"3Qr���������Q�u�Oѳgw��Qr����;S�~��)6H��
���hZw��/Gg�VT�mU�f����_�yt�7%$�];��zLW�F̰��xy2Ʉu�!MC�m�š_0[W6�j�f#��a�-KLi��+3Q7��c^q�g%s�<�1aY��IQeZ�f+}>�;S���6���L��0]Y��u����_�h��9��<���ƅ�pm��i�M$��AVv�Ś,�*�#t�2�.8���Y�����������)��-��Zh��
s���hü�97/#Oro�"���u�^/uF�g�Wɺ�,p:��������6a,^����x��%$�Yve���^�3PƗ���M���nT�P&y���S}��OJ
'��덫MH��^��:r��XԴ�Jۋ���/��r��I;�S��*�,+yz1h��v)�Q��w�^�ڍ�J2�oL�����q(��\�fD� �j:��^�T���%v��O��a��d�ɂ�������n�S�}���Z�O��)N����*λd��aȜkG_P�I��E���O�}��нa(^iQX᯦���-��7^)%�g
�'SJx�(.S�9�zV�ɴ�Z�{E� �))ۅ����i/s����7
� VIV��-��|sj0�*UBTHIqRf>�FP�$�Kq�N0� �R�̻8j\Gc��C����}I���U���z�\i�� 6����
F��)�Q��{Gҧ�3q������S��z�����Kj-A�z
V�ЛS�-z y:��8�*mNk�|D�鿓N��D2u+�0�Y��ŝ7�k���q�
m�·?8�I�b�]�����u���>�˗�^_�>(]��v
��Ӌ�zv�+�ݩ){v�ZrJ����2R�Q�몋�C���$z�
���[�,�p�p,����� �8mڊ���b�R�]�Il .f~��d����/��ݓs���㓓�mͶ�{�m��g����jQ�wn�=O�i�c�9ܚ�m4�Q�����/6ݨ[�������T�Ƨ?n�Զ���oytf���{�@�������AzT{ e{�[O�'Z�R�����������Z�����
t~�AG�D?s3���Չ�Iw� ���'|����~�U��\�����
w~�di�:Kޱ)U/sU%n jѩ�&�G�S����P�^ǝ�d).�.!�^U
�`
1wX[��aԇ�S�����x�o�FV�6����_��扐)T
�2M�fd=�ۖͭi��Z���7K��K
Bi��9%�7�@�<3�<ճ���Ի��U���,}���,a}��F�Rq�ɛr
�i�@�O��N���JvK�
K�L�N�� M, ʖv��0n��-�]Dw��lI�-�X�6ܶ$���Jʴ���h�5�O+m��O�I��+R�a瞠�\�� MG7�Bف�j��Y���o1��#�͖��0�V`��Ѱ��2M?
c��8>-C�rt��*���J�k��I�G�S:��e�#�hP��Kx[�鱼>�{��5�m�;w��c�ն��&�>�����j�-M��֥�^�َ�)������
�����6y�Ȝ����l_��������w{��-ō��̱�r> �U=�]���i�w�3��)�r�*]:�K]6��B�d���CT��Z����|���>���gf}�
��L�W��}���[��$'Y5
��&�c�
�-�j���.�z�6����R�� ���
6������7�MԷ�FM���n�Ìw�I��7�w5�E�}o��+��K
�ֵy����4���܌ȥW�"CO��<�H���?�&zp�]�o�1�@Z���������������������������������������������������������������������������hIH��DZ� n�p�(�*J\+���
59l��m��gY#R�JQkǷ����T�^�I&�.$��M�M��-����NyR\9��=
���wj\=B� 4�d�
��SQ�eU�۫?:�G��X\Z�6�S��
�>
y������R[q�5Ӱ��͙��f[v���"�_�#q{�M V6���܍�3"���u�9BK�(4��1���ӯ�qˇc$�{�ߝC�i6�I�(��O�m���θz�Ҝ5k�^:>Jzw�.�>��qV8��{vU[ڶ��E�
�m������|DžBz�]��.���K�H�j�I]��x��;��<�feN��'�iTj�M= ЈuL�.�.�u����
lG���K��KM��e����J�߾����
��]J��o)�#-[���2B���Q_��)��F?:ǖ��aݍ�YɻWE��ot��*5���
�<�br!+vuEj�Oڏ���5�*>�M�ɗ�{m�,�qZXr��忇2u^�R�O��2��Z}�Z��ێ�S[2�Je���n!*N�Dc�r�B�U��ً�4��<����Ǽ��MҲ���
s��1Z��w��5�7� �c3&Ė��ڻ�z��mP��*����FuJG1���-�����d�N:|�OU}ҵ�g�i2t~F�^^��Z.����Vx����jv�ŧ�n��N����Nh���<��:��]��^~NN��+�g�e^�����g.����SԔG�Fe߯�'[v�n'(ScJ�]�kܗ����7eJOl����
R�rfziݮ������q�̋��S"�\*��U<*�W�]��k��$�FջV���
�}?�
����������7�g��#֟�*��G
� �Q�Q���|��#/��bo�]���p��$��>_�Un9�����;��l
S
�Vv�Q�U�%O��LU{ο��m������U6����b�Z�1MTx�%�!�֙Q7�,
J�=!3
;�����Q,���ڌ;�6ͱ�݅q^��&ߔ·n
�#W�b���wӖ�X���.�Ht�G)N��&�d̵z��p�I�,�n
�cu
ޖU�j+V��X����U�p[w]�N��
�o�.J�6���Z���8�Ts�&��u���tx�ln;�~�H��P�H�S��/�xw
`�G
\��ʡ¿rj�
�Z^v�t"[L:�S��D�\����h�����0��s�U�wR
��,}�[���x^��X�,R2
�Vn<
����]�2�Y��D���r�[��S��RKs8t�X��b̷�G��?Ps
�T�v
�3��be,��z��V�����z����
D[�/I�.�K�OEQr�m'�$�
��7����|[���J��>�r
�S`5�յw���T#\�w1FT�z\Ԛ���� ��&�"ׅ�hS��H�r���D���\'����r�]����~/�>��p���;����:�P�����i��u�
u:�"9ő=t��TaS�7V�2��r�ӷk�����7m�b[�^W��m�Pp�*��[y.Þ��6f]���ci�z�JCgR���R��@�UVl�큝���.W���J�
���P�1��N�{/
�\whZ�
ػϧ�ӱ���E�7|�E�
֫Sί
�.x�-��Y���&����������������������������������������������������������������������������pi%v�
��'�'�-�x�6�r�
'�Ws*�6=���D�� ww���Uu�]�=C�?�MK��
��[�yrtܒG$�!WG�qJ*�%S�A�z���
�ED[��^)/t�ė/g��=�#���Omd����.|^
�n�/�s��l�����g��
�DZ������qem��qowݮ����RzU�ܜ��=�ڽ��-o�/�Iۖ�;q��V���ʘgPp���|m��m;6zGl�9.8pwWg�sJ2qP�b��e}}���U��p����Njٯ}7T���M�QKrؽt��Ex%�v��� w�����߾8%� |j
�;~���|}�pK����]��ơ�/��� w�����߾8%� |j
�;~���|}�pK����]��ơ�/��� w��&������~��e_�H�� 8�P���L7:������%�ʭ5�Kw�&��������U2
�v�w��R��
������������������������������������������������������������������������������������������������������_��������������+�r��m'��������}��C�7�#���� �rW��o��O����&���H�����o�G����?���������� �M������������$���U���R7{�FU�]�u� ;#���
!��W�k���`�|���W����>���潇
9�V�n)�6�)*���ҹ{��%�q�V4����q>�W1vi�#�T�"Qk��&G�wx��cJ�������������������������������������������������������������������������������������������������������B�J-
Ϸ^�����ˁ�xk�U}�������ԣ/�3�.��;]J=��<�*)�c��S��)����ROK
���9H=,r�
zX� ���@)�c��S��)����D���a�^��Խ�Q�
gxJI=��w�֣�g�f*T�R�j��������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������
- 1,007 Views
- 1 Download
- 0 Crossref
- 0 Scopus
Abstract
This paper reports a pseudoaneurysm of the anterior tibial artery after reduction with pointed bone reduction forceps on a spiral fracture of the distal tibia. Most reported injuries occurred at the proximal part of anterior tibial artery during drilling of the proximal tibia. To the best of the authors' knowledge, injury of the distal part of anterior tibial artery has never been reported. This paper describes a 54-year-old woman with a pseudoaneurysm of the anterior tibial artery clinically detected 11 weeks after the index surgery. This report highlights the need for surgeons to be aware of and careful about this complication during and after surgical intervention.
J Korean Fract Soc. 2019 Jan;32(1):43-46. English.
Published online Jan 25, 2019.
https://doi.org/10.12671/jkfs.2019.32.1.43
Published online Jan 25, 2019.
https://doi.org/10.12671/jkfs.2019.32.1.43
Copyright © 2019 The Korean Fracture Society. All rights reserved.
Case Report
Pseudoaneurysm of the Anterior Tibial Artery after Reduction with Pointed Bone Reduction Forceps on a Spiral Fracture of the Distal Tibia: A Case Report

Abstract
This paper reports a pseudoaneurysm of the anterior tibial artery after reduction with pointed bone reduction forceps on a spiral fracture of the distal tibia. Most reported injuries occurred at the proximal part of anterior tibial artery during drilling of the proximal tibia. To the best of the authors' knowledge, injury of the distal part of anterior tibial artery has never been reported. This paper describes a 54-year-old woman with a pseudoaneurysm of the anterior tibial artery clinically detected 11 weeks after the index surgery. This report highlights the need for surgeons to be aware of and careful about this complication during and after surgical intervention.
Keywords
Distal tibia, Spiral fracture, Pseudoaneurysm
Several reports exist regarding vascular injuries resulting from fixation of tibia shaft fracture.1,2,3,4,5) Most injuries reported are occurred proximal part of anterior tibial artery during drilling of proximal tibia.1,2,3,5) There was a report on pseudoaneurysm that developed after emergent blind AO pelvic C-clamp application for stabilizing the diastasis of symphysis pubis.6) However psuedoaneurysm of the anterior tibial artery due to reduction by pointed reduction forceps has never been previously reported. We present a case of psuedoaneurysm of the anterior tibial artery as the result of closed reduction with pointed reduction forceps on spiral fracture of distal tibia.
Case Report
A 54-year-old woman visited the emergency department with pain and false motion in her left lower leg after slipping down. On physical examination, there was no neurovascular abnormality and external wound. A swelling was mild. A simple X-ray was taken and showed the fracture of distal tibia, lateral malleolus and posterior lip of articular surface of distal tibia (Fig. 1). A main fracture of distal tibia was spiral with large wedge fragment at posterior aspect and combined with hairline fracture extension to distal fragment. Displacement of the tibia fracture was not so much but need to be operated. A fracture of lateral malleolus was trans-syndesmotic and had some comminution. A fracture of posterior malleolus was showed about 25% of articular surface involvement. She had a couple of medical problems, such as hypertension, diabetes mellitus, and colon cancer. She has taken some pills for these chronic diseases. However, she didn't take an antiplatelet agent. The fracture was protected with temporary splint. An injured leg was kept up to prevent further swelling. A surgical intervention was performed 3 days after the injury and as follow.

Fig. 1
Anteroposterior (A) and lateral (B) plain radiographs of the right tibia and fibula show a spiral fracture with a wedge fragment.
Under the general anesthesia, patient position was supine on the radiolucent table. Whole leg was draped usual manner and tourniquet was applied. A closed reduction with gentle traction and rotation was tried but the acceptable alignment couldn't be achieved. In this situation, open or percutaneous reduction is options. We chose a percutaneous reduction with the use of pointed bone reduction forceps (Fig. 2). After having achieved acceptable reduction, skin incision was made on the medial aspect of the ankle to insert anatomically pre-shaped 12 holes metaphyseal locking compression plate. A plate was introduced through the incision site and pushed up to the proximal tibia. Adequate positioning of the plate was confirmed under the fluoroscopic guidance. Screws were inserted on proximal and distal fragment in consideration of proper working length to get stable and flexible fixation for secondary bone healing. Fracture of lateral malleolus and posterior lip of distal tibia articular surface were reduced and fixed via single posterolateral approach of the ankle joint. Immediate postoperative X-ray shows acceptable reduction and fixation of all fractures (Fig. 3).
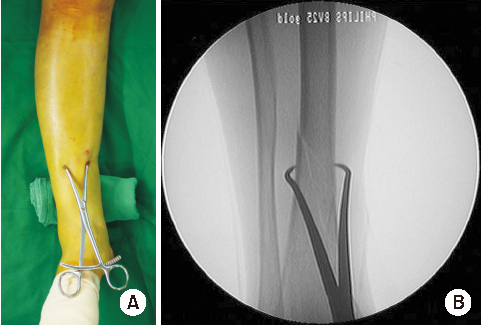
Fig. 2
Intraoperative photograph (A) and fluoroscopic image (B) applied pointed bone reduction forceps.

Fig. 3
Immediate postoperative anteroposterior (A) and lateral (B) radiographs showed acceptable reduction of both the tibia and fibula.
On postoperative physical examination, neurovascular status was intact. Postoperative rehabilitation program was applied as usual manner. After hospital discharge, she visited outpatient clinic regularly. Eleven weeks after the surgery, she complained a pulsatile mass on her injured leg. We couldn't see the beating but feel the pulse on the mass. It's located in anterolateral aspect of distal leg just under the skin. We found a small scar on top of the mass related with the insertion of pointed bone reduction forceps during the operation (Fig. 4).
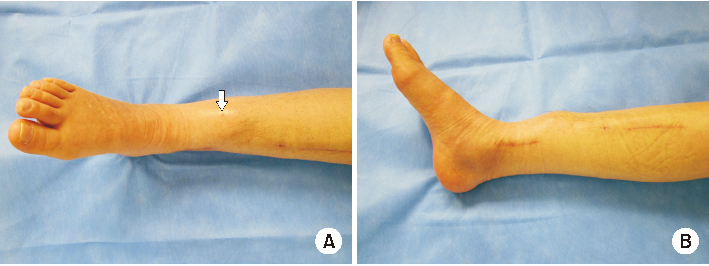
Fig. 4
Frontal (A) and sagittal (B) photographs show a pulsating mass in the anterior aspect of the fracture site of the right lower leg. On top of the mass, there is a small scar indicating the insertion point of the pointed bone reduction forceps (arrow).
For this pulsating mass, we performed a conventional angiography. On this examination, extravasation of contrast media from the anterior tibial artery adjacent to the fracture site was shown, indicating pseudoaneurysm (Fig. 5). The mass was more proximal than the uppermost screw inserted in distal fragment of the fracture which indicate pseudoaneurysm isn't related with drilling or screw tip.
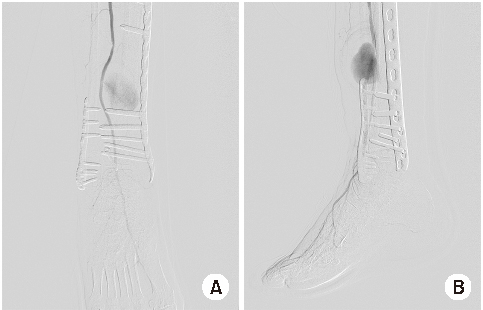
Fig. 5
Anteroposterior (A) and lateral (B) arteriograms of the right leg show extravasation of the contrast media indicating pseudoaneurysm of the anterior tibial artery adjacent to the fracture site.
A surgery was determined as a result of vascular consultation. On surgical exploration, the sac of the pseudoaneurysm was observed. An adhesion around the pseudoaneurysm due to fracture callus and scar tissue after initial injury made it difficult to dissect the mass from adjacent tissue and intact artery. So, the pseudoaneurysm was removed. Six months after the injury, we could get a fracture healing and no sign of vascular abnormality was noticed.
Discussion
Unlike a true aneurysm that is bounded by the vessel walls, a pseudoaneurysm is bounded by surrounding fibrous tissue. Any kind of vascular damage caused by trauma, infection, iatrogenic injury can make a pseudoaneurysm.
An anterior tibial artery is a branch of the popliteal artery that arises at the distal border of the popliteus muscle.7) It passes anteriorly and lies on the interosseous membrane, which in turn is attached to the posterolateral border of the tibia. The artery is relatively fixed here, as it just enters the anterior compartment after hooking across the proximal border of the intraosseous membrane. While running downward vertically on the anterior surface of the interosseous membrane, it descends adjacent to the fibula, and then to the tibia. In the upper part of its course, anterior tibial artery lies deeply along the lateral border of the tibialis anterior muscle with distance kept from the tibia.6) However, it directly adheres to the tibia at the lower part of its course.
Pseudoaneurysm of the proximal part of anterior tibial artery during the orthopaedic procedure was reported.1,3,5) Drilling for proximal interlocking screw is a common cause of pseudoaneurysm of anterior tibial artery. As mentioned previously, an anterior tibial artery at the proximal leg is relatively far from the lateral surface of the tibia.
Theoretically, distal part of anterior tibial artery, because of close proximity to lateral cortex of tibia, is more vulnerable to injury. However, surprisingly there is no report about this injury.
Minimally invasive osteosynthesis (MIO) is popular procedure because preservation of blood supply around fracture site has several advantages like rapid and sound fracture healing, lesser infection and needs for bone graft. Percutaneous reduction is essential step of MIO. A pointed bone reduction forceps is one of useful reduction tools. Surgeon should keep in mind that distal anterior tibial artery is very close to lateral surface of tibia. During the procedure, a pointed bone reduction forceps can be safely inserted through small incision identifying the lateral cortex of distal tibia to prevent arterial injury.
Since pseudoanuerysm tends to progress gradually, it may take several weeks or even months to be noticed.3) Gradual growing nature of pseudoanuerysm is also seen in our case as it was clinically detected 11 weeks after index surgery. In addition, regular follow-up examinations over several months and careful observation of wound are necessary.
Anatomically, deep peroneal nerve runs together with anterior tibial artery at the distal one third of lower leg. Therefore, one should think about the nerve injury when the patient has an arterial injury in this region and vice versa.
This report can be useful for surgeons in being aware of and careful about this complication during and after surgical intervention. Surgeons who suddenly encounter this complication can also benefit from our report in making appropriate diagnosis and management of the complication. Suspicion for the possibility of pseudoaneurysm, in addition to peroneal palsy, hypesthesia, should be always considered when patients complain of pulsatile mass near the fracture site and wound.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Gahlot N, Kanojia RK. Anterior tibial artery pseudoaneurysm due to interlocking bolt of tibial nail: a case report and review. Acta Orthop Traumatol Turc 2017;51:77–83.
-
-
Dreyfus U, Fishman J. False aneurysm of the posterior tibial artery complicating fracture of the tibia and fibula. J Trauma 1980;20:186–187.
-
-
Han KJ, Won YY, Khang SY. Pseudoaneurysm after tibial nailing. Clin Orthop Relat Res 2004;(418):209–212.
-
-
Sundararajan SR, Rajagopalakrishnan R, Rajasekaran S. Ruptured pseudoaneurysm of the lateral plantar artery after tibiotalocalcaneal fusion with retrograde nail-a rare complication. J Foot Ankle Surg 2018;57:393–395.
-
-
Hussain W, Balach T, Leland JM. Vascular injury involving proximal medial-to-lateral oblique locking screw insertion in tibial intramedullary nailing. Acta Orthop Belg 2011;77:414–418.
-
-
Kim WY, Lee SW, Kim KS, Lee JY. Superior gluteal artery pseudoaneurysm caused by pelvic C-clamp blind application. Hip Pelvis 2017;29:145–149.
-
-
Mróz I, Kielczewski S, Pawlicki D, et al. Blood vessels of the shin - anterior tibial artery - anatomy and embryology - own studies and review of the literature. Folia Med Cracov 2016;56:33–47.
-
 PubReader
PubReader Cite
Cite
